Article Text

Abstract
Objective To examine the population-wide overdose risk emerging from the prescription of methadone and buprenorphine for opioid substitution treatment in England and Wales.
Design Retrospective administrative data study.
Setting National databases for England and Wales.
Participants/cases Drug-related mortality data were drawn from the Office for National Statistics, and prescription data for methadone and buprenorphine were obtained from the National Health Service for the years 2007–2012. During this 6-year period, a total of 2366 methadone-related deaths and 52 buprenorphine-related deaths were registered, corresponding to 17 333 163 methadone and 2 602 374 buprenorphine prescriptions issued. The analysis encompassed poisoning deaths among members of the wider population of England and Wales who consumed, but were not prescribed these medications, in addition to patients prescribed methadone or buprenorphine.
Main outcome measures Mortality risk: substance-specific overdose rate per 1000 prescriptions issued; relative risk ratio of methadone in relation to buprenorphine.
Results During the years 2007–2012, the pooled overdose death rate was 0.137/1000 prescriptions of methadone, compared to 0.022/1000 prescriptions of buprenorphine (including buprenorphine-naloxone). The analysis generated a relative risk ratio of 6.23 (95% CI 4.79 to 8.10) of methadone in relation to buprenorphine. UK Borders Agency data were taken into consideration and revealed that only negligible amounts of methadone and buprenorphine were seized on entering UK territory between 2007 and 2012, suggesting domestic diversion.
Conclusions Our analysis of the relative safety of buprenorphine and methadone for opioid substitution treatment reveals that buprenorphine is six times safer than methadone with regard to overdose risk among the general population. Clinicians should be aware of the increased risk of prescribing methadone, and tighter regulations are needed to prevent its diversion.
- fatal overdose
- methadone
- buprenorphine
- relative risk
This is an Open Access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/
Statistics from Altmetric.com
Strengths and limitations of this study
Study is the first relative risk study of methadone versus buprenorphine in England and Wales, and the second only national study globally.
Study draws on a very large source of data, comprising more than 19 million prescriptions across 6 years.
Study presents an evaluation of risk across a full drug-using culture.
Data do not allow the identification of differences in severity of drug dependence between patients prescribed methadone and those prescribed buprenorphine.
The data used are based on the number of prescription items issued rather than number of identified patients.
Introduction
Opioid use constitutes a global public health problem, as heroin users experience significantly elevated mortality rates.1 In the UK, heroin and other opioids are the main contributor to drug-related deaths,2 despite a much lower prevalence of use relative to other illicit drugs (eg, cocaine).3
The UK National Health Service (NHS) provides opioid-dependent users with access to methadone and buprenorphine as substitution therapy.4 Methadone is a synthetic opioid receptor agonist, while buprenorphine is a mixed agonist-antagonist which is prescribed as either a single-ingredient tablet or in combined formulation with naloxone, a potent opioid antagonist that is added to deter patients from injection use.5
Opioid substitution treatment is the most effective intervention for opioid dependence.6 ,7 It has been found to reduce the risk of drug-related death8–11 as well as the incidence of criminal offending12 and is associated with the relatively low HIV rate among injection drug users in England and Wales.13
While many randomised controlled trials have compared methadone and buprenorphine with regard to their effectiveness at retaining people in treatment, suppressing craving, and reducing illicit opioid use, less is known about their relative safety. In a meta-analysis of 31 trials, only two studies tested the safety of methadone and buprenorphine, finding no significant difference in the rate of adverse events between the treatment samples.7
Similarly, the question of the relative safety of methadone and buprenorphine in the wider community, that is, among individuals not in receipt of a prescription and consuming diverted drugs, has received fairly little attention. This is surprising for at least two reasons: first, misuse of either drug can cause fatal overdose, particular when consumed in combination with other central nervous system depressants;14–18 second, the diversion of buprenorphine and particularly methadone to the illicit market for sale or exchange is a known problem in the UK and abroad.19 ,20
Recent attempts to address the problem of diversion in the UK, by the introduction of supervised consumption of buprenorphine and methadone at the dispensing pharmacy,21 have led to a significant reduction in the rate of methadone deaths in relation to number of patients treated.22 Nonetheless, it appears that the substantial majority of methadone overdoses occur in the general population. The risk represented by black-market methadone is illustrated by a UK-wide analysis of methadone-related deaths between 2009 and 2012.23–26 Of the reported 1117 deaths that involved methadone alone or in combination with other drugs, only 36% occurred among individuals who were known to be receiving methadone treatment. This finding is consistent with previous reports from New South Wales (Australia) and Germany,27 ,28 where at least half of methadone overdose deaths were the result of diversion. Over a 9-month period, the New South Wales study28 also compared total overdose mortality rates (ie, in-treatment and diversion) related to buprenorphine and methadone, and found that methadone was associated with a fourfold risk of overdose.
To date, there has been only one published evaluation of the relative safety of buprenorphine and methadone in a national treatment setting. In a review of drug-related deaths in France between 1994 and 1998, Auriacombe et al29 found that in relation to the number of patients receiving opioid substitution treatment, methadone was at least three times more lethal than buprenorphine in terms of overdose deaths among the French population as a whole (ie, among patients and the general public). In a follow-up study, Auriacombe et al30 noted that opiate overdose deaths had declined substantially following the introduction of buprenorphine treatment, but due to the correlational nature of the data, causality cannot be inferred.
To the best of our knowledge, this study constitutes the first effort to assess the relative safety of buprenorphine and methadone in Britain. Using Office for National Statistics mortality data and National Health Service prescription data for England and Wales from the years 2007 to 2012, the current study aimed to examine the population-wide overdose risk emerging from the prescription of methadone and buprenorphine for opioid substitution treatment.
Methodology
Ethics committee approval
Following National Research Ethics Service guidance, ethics committee approval was not sought for this study as all analyses encompassed non-confidential, non-attributable, de-identified data available via public databases.
Identification of individual number of prescriptions
Total quantities of buprenorphine, buprenorphine-naloxone and methadone dispensed in England and Wales from 2007 to 2012 were drawn from two sources: the National Health Service (England), and National Health Service (Wales) Prescription Cost Analysis data reports. To exclude prescriptions for either detoxification or pain management, sublingual formulations of less than 2.0 mg of buprenorphine, and buprenorphine patches were not counted. Methadone linctus, a preparation prescribed for coughs, was also excluded. As they are prescribed almost exclusively for the treatment of severe pain rather than substance dependence, methadone tablets were also disregarded. The use of methadone to manage pain is far less common than for treatment drug dependence. For instance, in Wales, in the years 2010/2011, methadone tablets comprised <1% of all methadone prescriptions. This accords with a separate UK finding that 99.5% of methadone dispensed in Scotland in 2008/2009 was against prescriptions for the treatment of substance dependence.22
Buprenorphine and buprenorphine-naloxone prescriptions are often dispensed as a composite of two or more individual items. For example, a 10 mg prescription comprises one box of 8 mg tablets, and one box of 2 mg tablets. Each of these boxes is recorded on the database as an individual dispensed prescription, leading to double counting. As a remedial means to determining the actual number of patients treated with buprenorphine or buprenorphine-naloxone, a survey was conducted of the 29 principal NHS treatment services in England and Wales to establish mean daily doses prescribed to patients. Fourteen services responded (48%). Accumulated returns from the survey produced mean average doses of 10.6 mg per day for buprenorphine substitution treatment (dose range from 6.14 mg to 11.9 mg), and 9.3 mg per day for buprenorphine-naloxone substitution treatment (dose range from 6.0 mg to 10.55 mg). Across all the 6 years studied, the mean average dose for all buprenorphine prescriptions was 10.43 mg per day.
The average dose of methadone across the 6 years was 46.6 mg per day. The total quantities of each drug dispensed per annum were subdivided by these doses to yield the total numbers of individual prescriptions written each year. As it is the standard duration of a substitution treatment prescription form raised in England and Wales (FP10 MDA), all prescriptions of buprenorphine, buprenorphine-naloxone and methadone were presumed to be of 14 days’ duration.
Identification of number of buprenorphine and/or methadone related deaths
Mortality data were drawn from the Office for National Statistics ‘Deaths Related to Drug Poisoning in England and Wales’ 2012 data set.31 In calculating deaths related to methadone or buprenorphine, the cause of death was defined using the WHO International Classification of Diseases, Tenth Revision (ICD-10) codes. Deaths were included when the underlying cause was drug poisoning, with buprenorphine and/or methadone mentioned on the death certificate.
When both drugs were referenced on a death certificate, the death was included in the breakdown of both drugs. Deaths in England and Wales include non-residents. Figures were based on deaths registered in each calendar year.
Identification of imported quantities of methadone and buprenorphine
To control for a potential confounding influence of illegally imported quantities of these drugs, the study incorporated UK Borders Agency data of Class A and Class C drugs seized while entering UK territory between 2006 and 2012.
Analysis
Causes of death and prescriptions issued to the user were tabulated separately. These numbers were aggregated to produce an estimate of the total fatalities and prescriptions issued during the study period. A summary measure ‘Buprenorphine-All’ was created for combined prescriptions of buprenorphine and buprenorphine-naloxone, as UK Office for National Statistics mortality records did not differentiate between these two formulations.
To compare the risk of fatal overdose represented by the two drugs, the total number of prescriptions for buprenorphine (including buprenorphine-naloxone) and methadone were divided by the number of fatal poisonings attributed to either drug to calculate the comparative risk of fatal poisoning for the whole population from use of either drug, expressed as a death rate per 1000 prescriptions.
Risk ratios and CI were calculated by means of standard formula using the open-source effect size calculator by Wilson.32
Results
There were 2366 deaths related to methadone poisoning and 57 deaths related to buprenorphine in England and Wales between 2007 and 2012 (see table 1).
Number of deaths related to drug poisoning where buprenorphine and/or methadone were mentioned on the death certificate by cause, England and Wales, 2007–2012
Almost seven times more prescriptions were issued for methadone than for buprenorphine between 2007 and 2012: 17.3 million prescriptions for methadone compared to only 2.6 million for buprenorphine (including buprenorphine-naloxone; see table 2). Over that time, the proportion of buprenorphine (all) to methadone prescriptions increased from 14% in 2007 to 18% in 2012, with methadone prescriptions gradually decreasing, following a peak of 3.1 million prescriptions in 2010. By contrast, buprenorphine-naloxone and buprenorphine prescriptions continued to increase throughout, with buprenorphine-naloxone increasing from 0.4% of total prescriptions in 2007 to 2.6% in 2012 (figure 1).
Prescriptions issued in England and Wales for opioid substitution treatment

Total prescriptions issued in England and Wales for opioid substitution treatment.
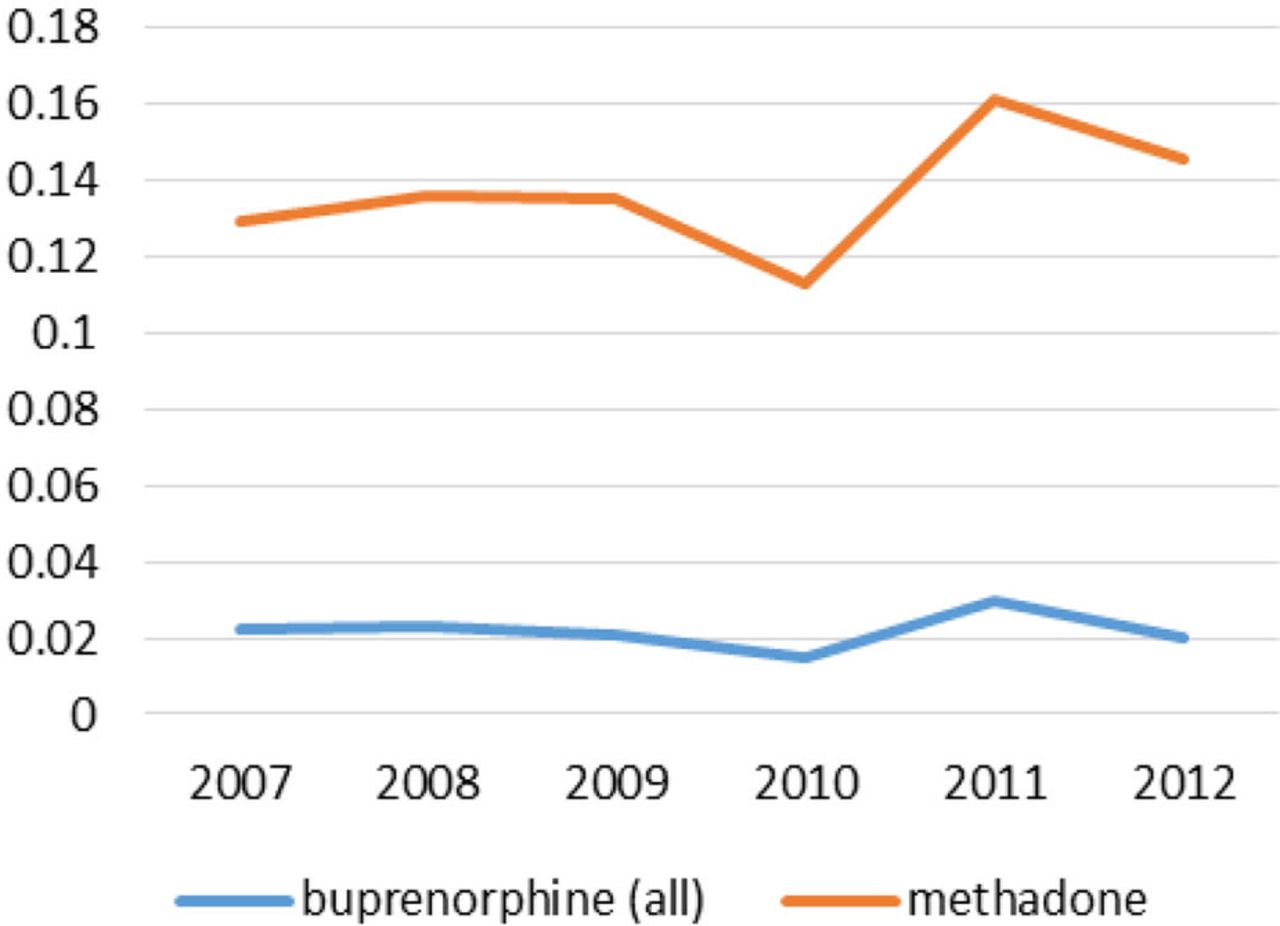
Among the whole population of England and Wales, there were 0.137 methadone-related deaths per 1000 prescriptions of methadone and 0.022 buprenorphine-related deaths per 1000 prescriptions of buprenorphine-based drugs for the substitution treatment of opioid dependence (see table 3).
Methadone and buprenorphine-related death rate per 1000 prescriptions issued
In terms of a fatality among the population of England and Wales as a whole, methadone represented a risk six times that of buprenorphine (RR 6.23; 95% CI (4.79 to 8.10)) (figure 2).
{kind=link}
{kind=link}
Methadone and buprenorphine-related death rate per 1000 prescriptions.
Could the methadone or buprenorphine involved in these deaths have come from other countries?
Changes in the way in which seizures are recorded by the UK's customs authority (the UK Borders Agency) implies that no methadone data are available for years 2010/2011 and 2011/2012 (methadone seizures were incorporated within the ‘Other class A’ return and cannot be identified individually, see table 4). Reporting in preceding years (2006/2007–2009/2010) indicates a very low quantity of methadone entering into UK territory.
Number of UK customs drug seizures by class, drug type and year (class A and C only)
According to UK Borders Agency reports, no buprenorphine was seized by UK customs in either 2006/2007 or 2007/2008.33 Buprenorphine was incorporated within the ‘Other class C’ returns from year 2008/2009; therefore, no seizure data were available for the remaining period of this study. In the 4 years that span 2006/2007 and 2009/2010 there were a total of 19 seizures of methadone by UK customs. In none of these years did the total quantity of methadone seized by the UK Border Agency amount to 1000 doses. The total number of doses of methadone seized, therefore, amounted to less than 4000, while the average annual number of methadone and buprenorphine doses prescribed in England and Wales, over the same 4 year period (2006–2007 to 2009–2010), exceeded 38 million and 3.8 million doses, respectively. There have been no reports of detection of any illegal manufacture of methadone or buprenorphine in the UK throughout the period of this study.33
Discussion
Statement of principal findings
Dose for dose, methadone was found to present a significantly greater risk of fatal overdose to the wider population than buprenorphine. Our finding is based on national administrative data collected in England and Wales between 2007 and 2012, and is consistent with the only published national study of this type.29 Further, our finding is supported by a study from New South Wales28 which reported a fourfold risk of overdose associated with methadone relative to buprenorphine.
During the 6-year period analysed in the present study, a very minor amount of imported methadone or buprenorphine was seized by UK customs, representing only a small fraction of prescriptions: per every dose seized by UK customs, roughly 10 000 prescriptions for methadone or buprenorphine were issued. Based on this ratio, the authors assume that illicitly imported methadone or buprenorphine were most likely not involved in the overdose deaths studied.
Strengths and weaknesses of the study
The high number of people enrolled in opioid substitute treatment in England and Wales during the 6-year study period (approximately 766 000 patients) is considerably larger than the sample of 140 140 cases analysed in the French investigation by Auriacombe et al.29 This allowed for a greater degree of confidence in calculating the relative risk (RR) of fatal overdose emerging from methadone and buprenorphine use.
Moreover, customs data were taken into consideration to control for illegal import of buprenorphine and methadone into the UK.
The collation of data at the prescription item level (rather than numbers of patients treated) meant that the number of buprenorphine prescriptions had to be calculated on the basis of mean doses. However, the mean buprenorphine dose identified in this study (10.43 mg per day) is broadly consistent with the pooled average dose of 11.96 mg per day, as generated by seven published flexible-dose trials of buprenorphine with doses ranging from 8.9 mg to 12.7 mg.34–40
Meaning of the study: possible explanations and implications for clinicians and policymakers
The inclusion of UK customs data revealed that only negligible amounts of methadone and buprenorphine were seized during the study period, implying that illicitly imported methadone or buprenorphine are unlikely to be risk factors for overdose in England and Wales.
This finding points to domestic diversion as the probable source of black-market methadone and buprenorphine implicated in the overdose deaths of individuals not in treatment.
Like other areas of medical research, the evaluation of opioid substitution therapy has traditionally focused on assessing the impact of treatment on clinical outcomes within treatment cohorts. However, our findings suggest that the degree of diversion of prescribed opioid substitutes19 ,25 ,26 ,41 and associated overdose risk in the wider population should also be taken into consideration.
Neither methadone nor buprenorphine are free from risk, not lastly because of potentially hazardous interactions when taken together with other central nervous system depressants (eg, benzodiazepines, alcohol),18 but our results demonstrate that for the years 2007–2012 buprenorphine was significantly safer for the population of England and Wales.
In appraising the cost-effectiveness of the methadone and buprenorphine, the National Institute for Health & Care Excellence4 recommends that “[t]he decision about which drug to use should be made on a case by case basis, taking into account a number of factors, including the person's history of opioid dependence, their commitment to a particular long-term management strategy, and an estimate of the risks and benefits of each treatment made by the responsible clinician in consultation with the person. If both drugs are equally suitable, methadone should be prescribed as the first choice”.
While taking full account of the limitations identified in the preceding section, this study identifies a substantial RR differential between methadone and buprenorphine. Our finding, together with previous UK25 ,26 and international reports27 ,28 ,30 of overdose fatalities linked to methadone diversion, suggests that the treatment sector may need to reappraise its relationship with methadone.
Generally, opioid substitution treatment in the UK begins under a regime of supervised consumption in a community pharmacy, but weekend and bank holiday closures mean that from the outset many patients are trusted to take home up to 2 or 3 days’ prescription. UK clinical guidelines42 suggest that supervised consumption can be relaxed and take-home doses prescribed when a doctor has good reason to believe that a patient will be able to maintain compliance with his or her methadone treatment.
The risk of methadone diversion into the black market makes it apparent that this can be an extremely difficult judgement for a clinician to make regarding the potential safety implications for persons other than the individual patient.
To conclude, for clinicians and policymakers alike, both risk of diversion and the significant RR differential between methadone and buprenorphine, as identified in this study, should form part of individual treatment decisions as well as treatment guidelines.
Unanswered questions and future research
Buprenorphine-naloxone shows early promise of increased safety over single-ingredient buprenorphine,43 but there are also indications that its self-injection can represent a comparable risk of death to the single-agent formulation.44 The short half-life of naloxone relative to buprenorphine may mean that the intoxicating effect of the buprenorphine is sometimes merely delayed rather than eliminated following injected use.44 There are insufficient data within this evaluation to draw any conclusion on the question of the comparative safety of buprenorphine-naloxone versus single-ingredient buprenorphine; this should be addressed by future studies.
An Australian study36 reported an indication of increased risk of mortality among patients following the cessation of buprenorphine treatment. Measurement of mortality following the cessation of treatment by either buprenorphine or methadone is beyond the scope of this study and would be a valuable subject for future research.
The study could not establish if there were differences in severity of dependence between the two patients groups (ie, those prescribed methadone and those prescribed buprenorphine). The feasibility of increasing the use of buprenorphine over methadone in the prescribed management of opioid dependence is, therefore, beyond the scope of this study.
References
Footnotes
Twitter Follow Dave Marteau at @dmarto
Contributors DM and KP conceived the study. DM carried out the database analyses and wrote the initial elements of the article, which KP helped edit. RM wrote further elements of the article, calculated each of the risk ratios and added text to complete the work.
Funding This research received no specific grant from any funding agency in the public, commercial or not-for-profit sectors.
Competing interests None declared.
Provenance and peer review Not commissioned; externally peer reviewed.
Data sharing statement Technical appendix and the data set are available from the corresponding author at d.m.marteau@sa.uel.ac.uk