Article Text

Abstract
Objective To understand the prevalence of healthcare students’ witnessing or participating in something that they think unethical (professionalism dilemmas) during workplace learning and examine whether differences exist in moral distress intensity resulting from these experiences according to gender and the frequency of occurrence.
Design Two cross-sectional online questionnaires of UK medical (study 1) and nursing, dentistry, physiotherapy and pharmacy students (study 2) concerning professionalism dilemmas and subsequent distress for (1) Patient dignity and safety breaches; (2) Valid consent for students’ learning on patients; and (3) Negative workplace behaviours (eg, student abuse).
Participants and setting 2397 medical (67.4% female) and 1399 other healthcare students (81.1% female) responded.
Main results The most commonly encountered professionalism dilemmas were: student abuse and patient dignity and safety dilemmas. Multinomial and logistic regression identified significant effects for gender and frequency of occurrence. In both studies, men were more likely to classify themselves as experiencing no distress; women were more likely to classify themselves as distressed. Two distinct patterns concerning frequency were apparent: (1) Habituation (study 1): less distress with increased exposure to dilemmas ‘justified’ for learning; (2) Disturbance (studies 1 and 2): more distress with increased exposure to dilemmas that could not be justified.
Conclusions Tomorrow's healthcare practitioners learn within a workplace in which they frequently encounter dilemmas resulting in distress. Gender differences could be respondents acting according to gendered expectations (eg, males downplaying distress because they are expected to appear tough). Habituation to dilemmas suggests students might balance patient autonomy and right to dignity with their own needs to learn for future patient benefit. Disturbance contests the ‘accepted’ notion that students become less empathic over time. Future research might examine the strategies that students use to manage their distress, to understand how this impacts of issues such as burnout and/or leaving the profession.
- EDUCATION & TRAINING (see Medical Education & Training)
- ETHICS (see Medical Ethics)
- STATISTICS & RESEARCH METHODS
This is an Open Access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/
Statistics from Altmetric.com
- EDUCATION & TRAINING (see Medical Education & Training)
- ETHICS (see Medical Ethics)
- STATISTICS & RESEARCH METHODS
Strengths and limitations of this study
Two online questionnaires developed from previous published qualitative studies were administered to medical, dental, nursing, pharmacy and physiotherapy students across the UK, enabling us to measure professionalism dilemmas as defined by healthcare students, replicating findings across studies and student groups.
The use of specific questions relating to respondents’ own experiences enabled us to measure, for the first time, healthcare students’ moral distress intensity and frequency of occurrence of professionalism dilemmas across a range of specific dilemmas (thus enabling us to delineate the effects across different dilemma-types).
Multinomial and logistic regression analyses enabled us to examine the influence of gender and frequency of occurrence on moral distress intensity.
Despite some students reporting experiencing no dilemmas, there is a risk that students experiencing such dilemmas were more motivated to participate in this research.
Introduction
Society places demands on all healthcare students to act professionally with a strong moral compass: learning to work in partnership with patients and the public, respecting dignity and safety (both for patients and also for healthcare professionals) and acting with integrity.1–6 Sometimes students encounter situations during their workplace learning that run counter to this. Such professionalism dilemmas have been defined as ethically problematic day-to-day events for learners in which they witness or participate in something that they think is improper, wrong or unethical.7
In terms of healthcare practitioners, there is growing literature examining how their experiences of value-conflicts at work (akin to professionalism dilemmas in students), such as witnessing the mistreatment of others, can cause them to experience moral distress.8 Moral distress has been defined as knowing the ethically correct thing to do but feeling unable to act.9 Indeed, research suggests that acting against one's conscience at work can have a number of serious consequences for individuals and organisations. Consequences include: (1) compassion fatigue and burnout in healthcare personnel; (2) decrease in an individual's empathy, avoiding or withdrawing from patients; (3) decreased service quality in terms of patient safety, patient experience and effectiveness of care; and (4) decreases in general staff health and well-being with high-staff turnover rates and staff shortages.8 ,10–17 As physician empathy has been widely demonstrated to positively affect diagnostic accuracy and patient outcomes,18–20 this is of concern for the education of our future healthcare workforce within such an organisational culture. Indeed, a systematic review of 18 studies examining empathy decline in medical students and trainee doctors pointed to problems in the clinical phase of training, and the distress produced by value-conflict situations as the catalyst for this decline.8
Against this backdrop of personal, professional and cultural challenges resulting from healthcare practitioners’ moral distress following value-conflicts, it is important to understand healthcare students’ experiences. In doing so, this will enable us to consider such issues explicitly within their learning environment and attempt to mitigate these long-term effects. Therefore, we present our findings from two large-scale questionnaires with the aim of understanding medical, dental, nursing, physiotherapy and pharmacy students’ reported experiences of moral distress following professionalism dilemmas (a type of value-conflict) during workplace learning.
Professionalism dilemmas, moral judgment and emotion
Workplace learning represents a major component of healthcare students’ learning within which professional dilemmas are experienced.21–32 For example, breaches of patient safety and dignity by healthcare workers with healthcare students even committing similar breaches themselves, often through coercion from their educational supervisors, comprises common professionalism dilemmas identified by medical, nursing, dental, pharmacy and physiotherapy students.26 ,28 ,29 ,31 Furthermore, breaches of student safety and dignity through educational supervisors’ and patients’ negative behaviours, including verbal and physical abuse directed toward the student and students witnessing the abuse of colleagues, have also been identified.24 ,26 ,29 ,31 ,32
Among other things, witnessing and participating in professionalism dilemmas means that students have to make certain moral judgments. For example, should they report the dubious actions of others towards patients and themselves and risk the consequences? How do they resist against participating in such acts when requested to do so by their seniors? Such moral judgments ‘ooze with sentiment’33 as students balance the empathy they feel for the recipient of abuse (eg, the patient) with the consequences of their actions. Indeed, analyses of healthcare students’ oral and written narratives of professionalism dilemmas, and their actions during and following the events, across four studies have consistently identified a number of significant findings relating to negative emotional talk: revealing an empathic connection with the recipient of abuse.26 ,28 ,29 ,31 Using the software program Linguistic Inquiry and Word Count,34 oral narratives of medical students’ professionalism dilemmas in their clinical years contained significantly more negative emotional talk than preclinical students’ narratives.26 Furthermore, linguistic analyses of oral and written narratives of medical, nursing, dental, pharmacy and physiotherapy students revealed: (1) significantly more negative emotion (including anger) talk in patient dignity and safety breaches committed by students’ clinical teachers than those committed by themselves; (2) student abuse narratives containing significantly more sadness or anger words; (3) consent narratives containing significantly more anxiety words; and (4) female students narrating professionalism dilemmas with more emotion talk than males.26 ,28 ,29 ,31 ,32
These findings around breaches of patient safety and dignity resonate with other research examining nursing students’ reactions to seeing patients receive uncaring treatment: so-called empathic distress.35 Empathic distress suggests that, should a student witness a patient in pain, they imagine how the patient might feel.36 This produces sadness in the student. However, in the face of professionalism dilemmas, such as observing healthcare practitioners breaching patient safety or dignity or causing the patient pain, the student can then feel anger towards the perpetrator, irrespective of whether the patient themselves feels angry. While empathic distress can trigger helping behaviours,36 when students feel unable to act due to personal or situational circumstances (eg, they have no confidence to speak out due to unequal power hierarchies) anxiety can ensue. In such a situation their self-focused distress (eg, anxiety) might overshadow their other-focused distress (eg, anger). This failure to act can result in increased distress for the student and possibly guilt. Such increased distress comprises a type of moral distress that can impact on individuals in the short (so-called mild distress), medium (moderate distress) and long-term (severe distress).9 Indeed, in-depth narrative analyses of professionalism dilemmas found healthcare students narrating moral distress following traumatic events, despite these events sometimes occurring over a year prior to their participation in the studies: a few students openly wept while describing the events, while others used laughter to cope with their retelling of the events.26 ,27 ,29
Moral distress of healthcare workers
Over the past decade there has been developing interest in researching healthcare practitioners’ experiences of moral distress.11 ,15 ,37–59 However, the majority of work has focused on nurses: often acute care nurses in inpatient settings.60 ,61 In terms of nurses, research clearly demonstrates that some of the associated factors relating to the organisational context can trigger moral distress, including: lack of resources (including time) for appropriate patient care, job type (eg, hospital nurses and psychiatric nurses report more distress than community nurses), job load, lack of autonomy and the ethical climate of organisations (ie, how they perceive the organisation views and deals with ethical issues). In terms of personal factors, data are mixed, but typically gender and ethnicity have been found to be unrelated to moral distress. Although age is sometimes found to have a positive relationship with reported moral distress, it has also sometimes been shown to have a negative or no relationship.11 ,57–59
While there has been considerable research examining the moral distress of nurses, there are only a handful of studies examining moral distress in other healthcare practitioners. Freedom of speech and working outside the hospital environment are associated with lower moral distress for doctors and pharmacists.45 ,62 Women doctors have been found to report more moral distress than male doctors.63 Younger pharmacists (aged 18–30) report more moral distress than older ones (≥56).62 And when considering the differences between healthcare groups, one study found nurses reporting higher moral distress than doctors,47 although others have found the reverse.48 While the issue of moral distress has been considered within physical therapy settings,39 to date, we have found no studies that have examined moral distress in dentists.
Healthcare students’ moral distress
While there is developing research examining healthcare practitioners’ experiences of moral distress, little work has explored this with healthcare students. For example, Wiggleton et al64 administered a questionnaire to examine common professionalism dilemmas experienced by 64 medical students along with differences in moral distress intensity for gender and frequency of occurrence. The most commonly experienced dilemmas were around team members ‘bad-mouthing’ other services or making disparaging comments about obese patients. While females reported witnessing distressing situations significantly more often than males, there was a (non-significant) trend for males to report greater distress the more situations they encountered. Another example, a descriptive review of 192 third-year medical students’ case reflections submitted as part of their course, found that a number of subject themes related to higher moral distress: team problems, resource allocation, lack of patient access to care, negative role models and inaction at the time of the dilemma.65
However, existing research examining professionalism dilemmas and moral distress intensity in students have a number of major flaws. What work has been carried out comprises very small-scale surveys with data collected at single sites and with single healthcare student groups,65 making generalisability problematic. The Wiggleton et al survey was developed by researchers without a thorough exploration of students’ personal reports of ethical/moral dilemmas, so items are not necessarily grounded in students’ lived experiences. Furthermore, students’ written reflections of difficult situations submitted as part of their coursework assignments,65 rather than for research purposes, are likely to have been ‘crafted’ to fit within the nature of the assignment.
Aims and research questions
We aim to address current deficiencies in the literature by reporting two studies exploring common types of UK medical students’ (study 1) and nursing, dentistry, physiotherapy and pharmacy students’ (study 2) professionalism dilemmas and whether gender or frequency of occurrence (as explored by Wiggleton et al64) is related to self-reported moral distress intensity, specifically addressing the following research questions:
What are the most common types of professionalism dilemmas?
What (if any) association exists between gender and reported levels of moral distress intensity following professionalism dilemmas?
What (if any) association exists between how often a person experiences the same dilemma (frequency of occurrence) and reported levels of moral distress intensity?
Methods
Study design
Two cross-sectional online questionnaires of medical students from 31 UK medical schools (study 1); and 40 UK healthcare schools (study 2).
Sampling and recruitment
Students were typically recruited using various methods dependent on school-specific agreements: email, virtual learning environments, student noticeboards, social networking sites (eg, Facebook, Twitter) and snowballing via student organisations. The questionnaires were live between 1 January and 1 March 2011 (study 1) and December 2011–March 2012 (study 2).
Study questionnaires
The questionnaires were based on themes inductively developed from earlier published qualitative research with (study 1) medical,26 and (study 2) nursing, physiotherapy, pharmacy and dental students29 and also influenced by the literature.66 In the two questionnaire studies presented here, students were asked about situations that they had instigated and similar situations that a supervising clinician had instigated that they felt were unprofessional. Seventy-nine (study 1) and 105 (study 2) questions of specific events were developed across three main ‘themes’: (1) patient dignity and safety breaches (study 2 had additional items to study one as identified from the qualitative data: eg, “You have compromised patient safety by making a clinical mistake and covering it up/covering up others’ mistakes”); (2) valid consent for students to examine/undertake a procedure on a patient (pharmacy students did not answer these items as they were not relevant to them); and (3) negative workplace behaviours such as student abuse (study 2 had more of these specific items, being more prevalent in the qualitative data). All themes were defined by drawing on specific policy documents (eg, Royal College of Nursing definition of dignity67) and moral distress was also defined up-front.
Each themed set of questions began by asking respondents to examine a group of related questions around dilemma events and to indicate whether they had experienced any of the situations during the past 12 months. ‘Yes’ responders then indicated which specific situations they had experienced by providing two responses: (1) how often they had experienced the scenario; and (2) how distressed they felt about it, using the following Likert scale:
Frequency of occurrence: (1) Never; (2) 1–2 times; (3) 3–5 times; (4) 6–10 times; and (5) >10 times.
Moral distress: Using the moral distress scale:64
No distress (although it happened);
Mild distress (slightly uncomfortable during the event, but not much thought afterwards);
Moderate distress (disturbed and distressed during the event, feel helpless to do anything and think about it for a while afterwards, but does not bother me much now);
Severe distress (disturbed and distressed during the event, feel helpless to do anything and still bothers me).
A qualitative ‘your story’ section28 ,31 and questions on whistleblowing and challenging behaviours were included in the questionnaires but are not reported here.
Data analysis
For both questionnaires we present the number and percentages of respondents to address the first research question (common dilemmas experienced). Associations between gender, frequency of occurrence and moral distress intensity (research questions 2 and 3) were then modelled using categorical multinomial regression and logistic regression (where the moral distress outcome variable was simplified into a binary no distress/distress variable by pooling all levels which involved some distress). The categorical model ensures that no implicit weight is assigned to distress categories and provides estimates for the probability of respondents classifying themselves as being mild, moderately or severely distressed compared to the baseline of no distress. In our earlier exploration of the data we looked for relationships in terms of age, religiosity, ethnicity and clinical/preclinical students. There appeared to be no consistent patterns with these variables, so we did not include any other demographic variables in the regression analyses.
Respondents
For study 1, 2397 UK medical students responded: 68.2% female (n=1634), 78.6% white (n=1884), 67% (n=1606) clinical students in year 3 or above and 88.6% (n=2124) between the ages of 17 and 25. Owing to the recruitment process varying dramatically by school (eg, many schools advertised the study on a virtual noticeboard and others emailed information only to students undertaking clinical placements) it was impossible to calculate an exact response rate. Instead, we provide a lower-bound to the response rate by school based on actual student numbers at each of the 31 participating schools at the time of the study and the number of respondents from each of the 31 schools: overall response rate was 5.87% (range=0.10–27.11%; SD=5.82). As the main data analysis concerns associations between gender, how often a person experienced a situation (frequency of occurrence) and self-reported moral distress, a better understanding of the generalisability of our findings is the extent to which our study sample represents the target population. We therefore also calculated the difference between all UK medical students in the academic year 2010–2011 (target population)69 and the study population by gender (female, n=24 804 (56.6%); male, n=18 997) and ethnicity (white, n=25 489 (58.2%); non-white, n=18 313). While our study sample and the target population comprised more female and white individuals, our study sample included disproportionately greater numbers of females and white participants: gender, X2=108.045, df=1, p<001; ethnicity, X2=391.982, df=1, p<0.0001.
For study 2, 1399 healthcare students responded to the questionnaire comprising 756 nursing, 268 pharmacy, 201 physiotherapy and 174 dentistry students: 82.1% of the total sample were female (n=1148), 85.3% white (n=1194), 46.4% (n=621) in year 3 or above and 80.2% (n=1122) between the ages of 17 and 30. Again, due to the varying recruitment process it was impossible to calculate exact response rates. The lower bound of the response rate by school was therefore calculated, based on actual student numbers at the 40 schools at the time of the study: overall response rate was 7.75% (range=0.75–29.12%; SD=7.16). We also calculated the difference between all UK undergraduate ‘subjects allied to Medicine’ in the academic year 2011–2012 (target population statistics from https://www.hesa.ac.uk) and the study population by gender (female, n=197 255 (81.2%); male, n=45 600) and ethnicity (white, n=172 765 (77.1%); non-white, n=18 313). There was no significant difference between our study sample and the general study population in terms of gender, X2=0.636, df=1, p<0.223; but there was a significant difference for ethnicity, X2=32.693, df=1, p<0.0001.
Results
Most common professionalism dilemmas: higher-order themes and events
Our first question relates to the issue of how common specific dilemmas are in terms of them being experienced by a wide range of respondents. A total of 69.9% of female and 59.9% of male medical student respondents, and 47.5% of female and 36.2% of male other healthcare student respondents indicated that they had witnessed clinicians breaching patient dignity or safety during the past year. A total of 47.1% of female and 48.8% of male medical student respondents and 28.8% of female and 27.5% of male other healthcare student respondents reported instigating similar breaches themselves. A total of 61.3% of female and 56.6% of male medical student respondents and 17.3% female and 13.6% of male other healthcare respondents (excluding pharmacy students) reported undertaking an examination/procedure on a patient without valid consent following the request of a clinical teacher for the sake of their learning. A total of 31.5% of female and 38.2% of male medical student and 19.1% of female and 12.4% of male other healthcare student respondents reported instigating this themselves. A total of 80.4% of female and 71.5% of male medical students and 83.3% of female and 71.3% of male other healthcare students reported being victims of abuse. A total of 57.2% of female and 47.8% of male medical students and 49.6% of female and 37.8% of male other healthcare students reported witnessing the abuse of workplace colleagues. Twelve per cent of medical student and 8% of other healthcare student respondents reported experiencing no dilemmas.
Tables 1 and 2 set out the 10 most common types of professionalism dilemmas as reported by medical and other healthcare student respondents (ie, those being reported as occurring at least once during the previous year). For medical students, half of these refer to patient safety and dignity breaches, with the other half referring to student abuse. For other healthcare student respondents, the majority were student abuse dilemmas with only one concerning patient safety and dignity. In addition to the most commonly reported situations, we also report the top three patient-focused and student-focused dilemmas for medical and healthcare students in terms of frequency of occurrence (focusing on the percentage individual respondents reporting them occurring six or more times during the past year). The top three patient-focused dilemmas for medical students were clinicians verbally coercing patient consent for student learning (14.7%), or through misrepresenting students’ identities (9.1%) and clinicians compromising patient safety through poor hygiene (12%). In terms of student-focused dilemmas, the most frequent were students feeling ignored by their clinical teachers (24.1%), being asked questions by clinical teachers in an intimidating manner (17.2%) and asking questions that are unrealistic and beyond their level of training (16.6%). The only item not featuring in the 10 most common dilemmas was students feeling ignored. For healthcare students, clinicians talking about (7%) or to (4.8%) patients inappropriately and compromising patient safety through poor hygiene (5.9%) were the most frequently occurring patient-focused dilemmas. Students being given menial tasks (16.1%), feeling ignored (8.9%) and excluded from learning opportunities (7.6%) by clinical teachers being the most frequently occurring student-focused dilemmas. Of these, only clinicians’ poor hygiene and talking inappropriately to patients did not feature in the 10 most common dilemmas.
Medical students’ 10 most common professionalism dilemmas reported at least once during the past 12 months
Nursing, physiotherapy, pharmacy and dental students’ 10 most common professionalism dilemmas reported at least once during the past 12 months
In terms of gender, various relationships were found between gender and frequency of occurrence: males reported (1) compromising patient safety through poor hygiene more frequently than females (X2 (3)=7.822, p<0.05); (2) being called a derogatory name more frequently than females (X2 (3)=8.932, p<0.05); and (3) receiving verbal threats to make their life difficult more frequently than females (X2 (3)=7.725, p<0.05). While unwanted sexual talk from patients was more common for females than males, the frequency with which students experienced such sexual talk (when it did happen) did not differ between genders.
Moral distress intensity: influence of gender
Given that not all respondents experienced all situations, we used the recommended sample size n≥90 for a specific question to detect a medium effect.68 In study 1, 62/79 questions for medical students had sufficient responses to examine the influence of gender and frequency of occurrence on moral distress intensity using multinomial regression (MNR) analyses. Significant differences were found for 51/62 situations (over 80% of cases: mean number of responses for questions with a significant difference was n=579 vs n=272 for those with a non-significant difference). Where gender differed (42/51 professionalism dilemma items: 15 patient safety and dignity, 4 consent, 19 student abuse, 4 witnessing ‘other’ abuse) we found an identical pattern: men were more likely to classify themselves as experiencing no distress and women were more likely to classify themselves as experiencing distress. Aggregated across all 42 situations (totalling 22 540 responses; figure 1) the mean absolute probability of ‘no distress’ for men=0.40 (95% CI 0.17 to 0.42), and for women=0.24 (0.23 to 0.25). Women were significantly more likely to classify themselves as being distressed: mild distress for women=0.51 (0.49 to 0.52), men=0.45 (0.44 to 0.47); moderate distress for women=0.21 (0.12 to 0.22), men=0.13 (0.12 to 0.14); severe distress for women=0.05 (0.04 to 0.06), men=0.02 (0.02 to 0.02).

Overall pattern of medical students’ moral distress responses by gender represented as absolute probabilities. Note: the pattern for healthcare students is the same so is not repeated here.
In study 2, 47/105 questions for other healthcare students had sufficient data for us to detect a medium effect for the influence of gender and frequency of occurrence on moral distress intensity. MNR analyses found significant effects for 38 situations (over 80% of cases: 34 of which were also significant in study 1). We found no effect of discipline on gender or frequency for moral distress, so we aggregated the data across all healthcare student respondents. An effect of gender for moral distress intensity was found (15/38 professionalism dilemma items: 3 patient safety and dignity, 1 consent, 11 student abuse), with a pattern identical to that found in study 1. For all items, men were more likely to classify themselves as experiencing no distress, with women being more likely to classify themselves as experiencing distress. Aggregated across all 15 situations (totalling 4449 responses) the mean absolute probability of ‘no distress’ for men=0.46 (95% CI 0.42 to 0.50), women=0.28 (0.27 to 0.30). Women were significantly more likely to classify themselves as being distressed: mild distress for women=0.43 (0.42 to 0.45), men=0.34 (0.31 to 0.38); moderate distress for women=0.22 (0.21 to 0.24), men=0.16 (0.13 to 0.19); severe distress for women=0.06 (0.05 to 0.07), men=0.04 (0.03 to 0.05).
Moral distress intensity: influence of frequency of occurrence
In study 1, MNR analyses found a significant effect of frequency of occurrence on moral distress intensity for 31/51 situations for medical students (over 60% of cases: 9 patient safety and dignity, 2 consent, 18 student abuse, 2 ‘other’ abuse). We analysed the data using logistic regression (LR) to examine ‘no distress’ versus ‘distress’ for males and females. Here, two distinct patterns were apparent: we call these habituation and disturbance.
Habituation
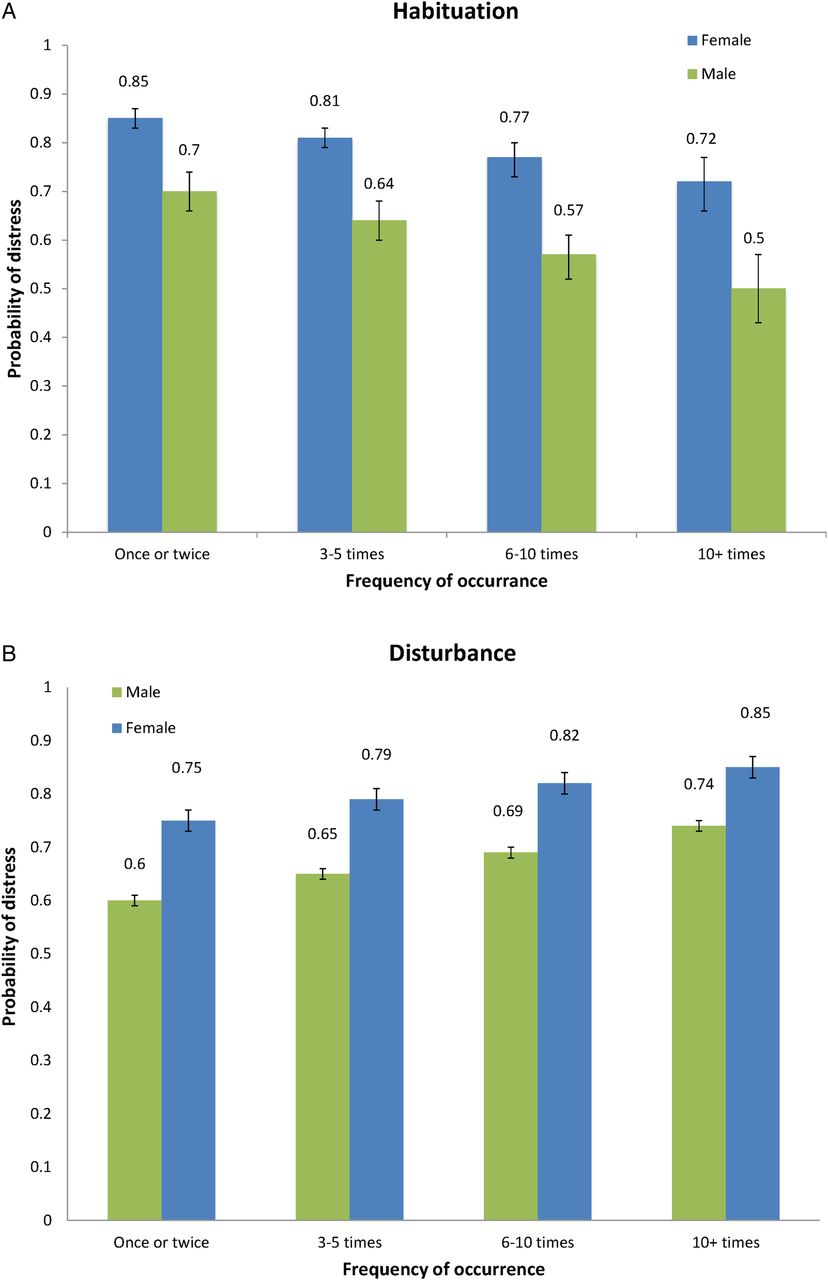
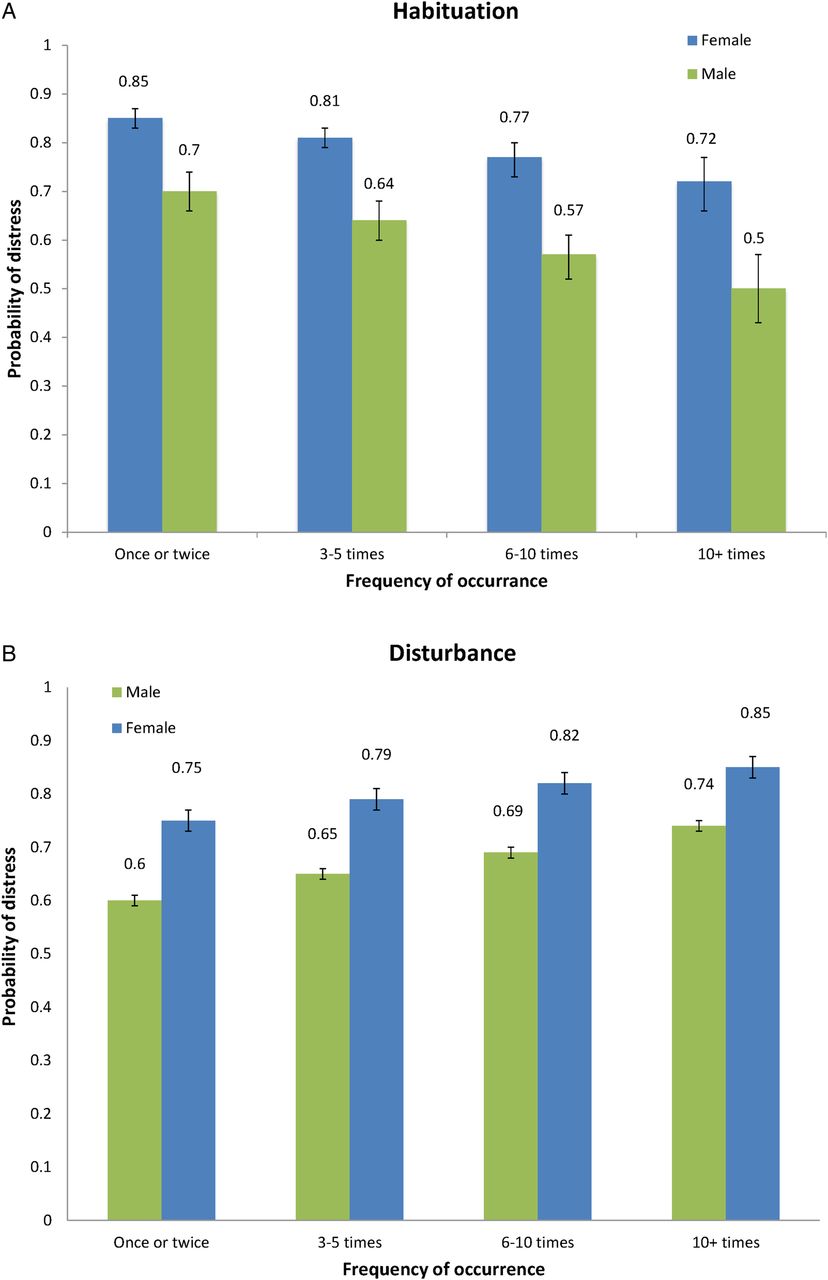
Three of 31 situations where students, or clinical teachers and students, had compromised patient care for the justifiable purpose of student learning showed significant habituation effects: (1) Clinician asking student to instigate unnecessary patient discomfort for own learning needs; (2) Student instigated unnecessary patient discomfort for own learning needs; and (3) Clinician instigated examination for student benefit despite patient being unable to consent due to personal factors. For these, respondents reported less distress as a function of frequency of occurrence (see figure 2A for this pattern modelled with LR (some distress vs no distress) using aggregated data, totalling 1884 responses): the mean absolute probability of ‘distress’ when experiencing an event 1–2 times for men=0.70 (95% CI 0.66 to 0.74), women=0.85 (0.83 to 0.87), 3–5 times for men=0.64 (0.60 to 0.68), women=0.81 (0.79 to 0.83), 6–10 times for men=0.57 (0.52 to 0.61), women=0.77 (0.73 to 0.80) and over 10 times for men=0.50 (0.43 to 0.57), women=0.72 (0.66 to 0.77).
{kind=link}
{kind=link}
(A) Habituation pattern for moral distress responses in medical students by frequency of occurrence represented as absolute probabilities (vertical bars showing 95% CIs derived from regression modelling). (B) Disturbance pattern for moral distress responses in medical students by frequency of occurrence represented as absolute probabilities (vertical bars showing 95% CIs derived from regression modelling). Note: the pattern for healthcare students is the same so is not repeated here.
Disturbance
The remaining 28 questions showed a disturbance effect where reported distress increased with exposure to the scenario and related to situations where no perceived benefit might be found (unjustifiable, figure 2B; aggregated data as above, totalling n=17 440 responses): the mean absolute probability of ‘distress’ when experiencing an event 1–2 times for men=0.60 (95% CI 0.58 to 0.62), women=0.75 (0.74 to 0.76), 3–5 times for men=0.65 (0.63 to 0.67), women=0.79 (0.78 to 0.80), 6–10 times for men=0.69 (0.67 to 0.71), women=0.82 (0.81 to 0.83) and over 10 times for men=0.74 (0.72 to 0.76), women=0.85 (0.84 to 0.86).
In study 2, significant effects of moral distress intensity and frequency were found for 29/38 situations for other healthcare students (76% of cases: 8 patient safety and dignity, 18 student abuse, 3 ‘other’ abuse). Of these, none of the dilemmas contributing to the habituation pattern found in the medical student data were significant. Only one pattern was found: disturbance, where reported distress increased with exposure to the scenario: (aggregated data as above, totalling n=14 478 responses) the mean absolute probability of ‘distress’ when experiencing an event 1–2 times for men=0.49 (95% CI 0.45 to 0.53), women=0.68 (0.66 to 0.70), 3–5 times for men=0.58 (0.54 to 0.62), women=0.75 (0.73 to 0.76), 6–10 times for men=0.66 (0.61 to 0.70), women=0.82 (0.80 to 0.84) and over 10 times for men=0.74 (0.69 to 0.79), women=0.86 (0.83 to 0.88).
Discussion
We administered two questionnaires to understand the impact of professionalism dilemmas experienced by UK healthcare students on self-reports of moral distress intensity. A total of 3796 students from across England, Northern Ireland, Scotland and Wales responded across both questionnaires. Although around 10% of respondents reported experiencing no professionalism dilemmas over the past year, the remainder reported witnessing or participating in breaches of patient dignity or safety and the majority reported being victims of workplace abuse or witnessing the abuse of other healthcare workers. The findings around patient care dilemmas resonate with recent government inquiries into patient safety and dignity breaches in the UK.6 Findings around workplace abuse concur with previous research suggesting that student abuse and witnessing the abuse of others occurs as soon as students enter the clinical environment.69
As response rates were on the low side, suggesting that we may have an issue with non-response bias, we urge caution in generalising our findings about frequencies of dilemmas to all healthcare students in the UK (so-called probabilistic generalisation). However, due to the extremely high number of respondents across two questionnaires there is sufficient data for us to examine relationships between gender, frequency of occurrence across a range of dilemma events and moral distress intensity. In other words, using our data from two questionnaires, we are able to establish robustness through empirical generalisation (because we report two studies which demonstrate replication) and through theoretical generalisation (because our questionnaire is rooted in the existing theory of moral distress). The important point here is that we are studying relationships, rather than individual variables. As Blaire and Zinkhan point out: “given these three paths to generalization (theoretical, probabilistic, empirical), along with the fact that relational results are resistant to sample bias, we can afford to be lenient about sample quality in academic research. In a sense, we bracket sample quality front and back. We pre-empt it through theory, and we remediate it through replication” (ref., 70 p.6).
Multinomial and logistic regression modelled the probability of reported moral distress intensity according to gender and the frequency of occurrence of dilemmas. For both studies, and across a range of dilemma events (eg, patient safety and dignity, consent, student abuse and, from medical students, witnessing ‘other’ abuse) females were consistently more likely to classify themselves as mildly, moderately and/or severely distressed. The question now is whether this finding reflects a genuine sex difference (ie, males experience less distress) or whether, despite the anonymity of respondents, healthcare students simply answered the questionnaires in a way consistent with gendered expectations (eg, males downplaying their distress because they are socially expected to appear tough),71 and thereby: ‘making oneself look good in terms of prevailing cultural norms when answering to specific survey questions’ (p. 2028). We do not think acting consistent with gendered expectations is a conscious attempt to deceive but results from unconscious needs to conform to social norms, such as men being expected to be strong and rational and women weak and emotional.72 Accordingly, we cannot be sure that women experienced more distress than men. Thus, when classifying themselves as being morally distressed (or not), respondents were likely to do so in accordance with their particular gendered identities.73 Indeed, this is reflected in the ‘most memorable’ narratives recorded in both questionnaires, where women's narratives contained significantly more anger and anxiety talk.28 ,31 Importantly, if males are downplaying their levels of distress then they are potentially at risk of negative emotional well-being and leaving the organisation.74
In terms of the relationship between moral distress intensity and frequency of specific events, we found two distinct and opposite patterns across the two studies. Habituation: medical students reported becoming emotionally desensitised to situations that could be justified for their learning (with no significant difference for other healthcare students). Disturbance: in both studies respondents reported becoming more distressed with repeated occurrences of situations that could not be justified for their learning. These events included breaches of both patient and student safety and dignity.
The effect of habituation appears to resonate with many studies reporting a reduction in healthcare students’ empathy over time.8 ,75–79 However, the pattern of habituation was found only for medical students and with a few items in the current study: situations where patients were harmed for students’ learning needs and a breach of patient consent for student learning. Interestingly, none of the items that displayed this pattern in medical students had significant effects for frequency of occurrence on the other healthcare student data (so do not contribute to the effect of disturbance either). This is unsurprising when we consider the percentage of respondents reporting these items within this healthcare group: only 5–9% reported experiencing these situations, compared with 14% (for the consent situation) and 28–37% for unnecessary harming a patient for medical student needs (student and physician instigated, respectively). It appears therefore that these events rarely occurred within the other healthcare group, possibly due to the different roles they play in relation to patients. The absence of significant relationships for the healthcare student group could therefore be due to a lack of power. In terms of the medical student group, rather than suggesting an erosion of empathy, this pattern of habituation with these specific items could perhaps be better understood through a utilitarian lens that explains the morality of an action in terms of its consequences.80 This explanation suggests that through workplace learning, medical students appear to learn how to balance the principle of individual patient autonomy and dignity with their own needs to learn for the benefit of future patients: a patient-oriented utilitarianism. Thus any empathic distress they initially feel for the patient in front of them reduces over time (for the greater good of future patients).
We believe that the larger effect of disturbance also goes against the view that students’ empathy diminishes: items that produced this effect included consent issues such as misrepresenting students’ identities and breaches of patients’ and students’ dignity and safety (eg, clinicians compromising patient safety through poor hygiene and talking to or about patients inappropriately). Thus, we see these specific items, along with associated moral distress responses, as being a measure of ‘empathic arousal’.81 ,82 Rushton et al82 point out that empathic arousal comprises four interrelated dimensions: (1) empathy (emotional attunement); (2) perspective taking (cognitive attunement); (3) memory (personal experience); and (4) moral sensitivity (ethical attunement). In the case of a distressing event when all four are aligned, compassionate care and resilience may be fostered. However, during distressing professionalism dilemma events in which value-conflicts arise (ethical disarray, rather than attunement) moral distress might ensue. That respondents demonstrate the same pattern of self-reported moral distress when students are the victims of abuse, as they do when patients are the victims, suggests to us that these four processes are at play: thus the effect of disturbance (greater moral distress in the face of ethical disarray) suggests that respondents are able to place themselves in the position of the patient (perspective taking) as they too are victims of dignity and safety breaches (memory). Although there are other possible explanations to our findings (eg, we asked different questions which resulted in different responses), our interpretation is triangulated by our previous analyses of respondents’ most memorable dilemmas taken from the same questionnaire (eg, medical students using significantly more anger talk when narrating patient safety and dignity dilemmas by healthcare professionals).26 ,28 ,32
This finding leads us to ask why we have found an increase in empathy with greater, rather than decreased, exposure to professionalism dilemmas. The majority of studies examining empathy decline have measured it using the 20-item Jefferson Scale for Physician Empathy–Student Version (JSPE-S).83 This includes items such as: “I believe that emotion has no place in the treatment of medical illness”; “A physician's sense of humour contributes to a better clinical outcome”; and “Patients feel better when their physicians understand their feelings”. Such statements are general cognitive (belief) statements about the therapeutic benefits of empathy, far removed from any specific student–patient interactions involving professionalism dilemmas. How much these types of statements reflect actual empathic responses in healthcare students within their interactions with patients is debatable, and has been contested elsewhere.84 Instead, by asking students to tell us whether they have experienced certain professionalism dilemmas over the past year, and to report their frequency of occurrence and intensity of moral distress they felt, we believe that we have ‘measured’ students’ empathic arousal for specific events.81 We think that this paints a more accurate picture of healthcare students’ compassionate and empathic values than is possible with scales such as the JSPE-S.
However, our study has some methodological challenges that must be taken into consideration when interpreting these results. Although our study is (to our knowledge) the largest of its kind across multiple countries and healthcare student groups, our medical and healthcare student samples differed from the overall target populations in terms of gender (more females in the medical student sample) and ethnicity (more white respondents in both samples). Furthermore, it was impossible to calculate the exact response rate for both studies (so we present estimates for the lower bound of responses). As such, we believe that this could influence our findings for our first research question (common dilemmas experienced). For example, that our medical student sample was more likely to be female than the target population could mean that we may have found higher rates of sexual harassment and gender discrimination than is reflective of the target population. And due to our estimated low response rates, we might have attracted only the most motivated students to participate (ie, those who had something they wished to report), thereby over-estimating the rates of professionalism dilemmas compared with the overall target populations. That both study samples were more likely to be white than the target population means that we may have found lower rates of racial harassment and discrimination than is reflective of the target population. However, as we have already highlighted, these differences should not affect our associations in relation to gender, frequency of occurrence and moral distress (research questions two and three). What might have affected these associations, however, is the issue of social desirability bias. Indeed, we draw on this very issue above in our interpretation of the finding that males report experiencing lower distress than females.
Despite these challenges, our findings have implications for what we, as healthcare professional educators, do about students’ emotional residue (ie, emotions that continue many months after the event itself, the moderate and severe levels of moral distress). To tackle this issue, we draw on the emotion regulation literature. Emotion regulation is the process of influencing which emotions we experience, when and how we experience them and how we express them.85 Successful emotional regulation has been shown to contribute to healthcare workers’ performance and well-being: influencing time spent in listening to patients, reducing burnout and increasing pleasurable emotions.86 The strategies we tend to use to regulate our emotions include choosing whether or not to engage in specific activities or thinking of ways to modify it; selecting what to attend to during the event and (possibly) reappraising the situation; and following the event, de-briefing or suppressing emotions. While some strategies have been shown to have serious negative health effects (eg, suppression), others have been shown to be beneficial (eg, positive thinking, problem-solving, seeking social support and relaxation).84 ,87 Future research therefore might examine the strategies that students use to manage their distress to understand how this might impact issues such as burnout and/or leaving the profession. As many respondents in our study experienced emotional distress for months and sometimes up to a year after the actual event, we suggest that healthcare students and professionals are taught the knowledge, skills and attitudes of effective emotion regulation. Without developing the capabilities for emotion regulation at the level of individuals, teams and the healthcare organisation itself, it will be impossible for healthcare professions to collectively set the moral compass in the ‘right’ direction.
Acknowledgments
The authors would like to thank Dr Daniel Joyce for his assistance with the statistical analysis and Dr Hannah Linford for her assistance in the development and delivery of the medical student questionnaire. The authors would also like to thank Wendy Lowe and Elaine Plenderleith for their help in securing ethics approvals for the 40 healthcare schools.
References
Footnotes
Twitter Follow Lynn Monrouxe at @LynnMonrouxe and Charlotte Rees at @charlreessidhu
Contributors LVM and CER designed the studies, participated in the acquisition, analysis and interpretation of data (LVM was the Principal Investigator for study 1, CER was the Principal Investigator for study 2). LVM drafted the first version of the manuscript. ID advised on the analysis and interpretation of the data. SEW obtained ethical and institutional approval for the research, led on the data collection (supported by LVM and CER). LVM, CER, ID and SEW reviewed (and revised where appropriate) the manuscript and all authors approved the final version.
Funding This work was supported by grants from the Association for the Study of Medical Education (study 1) and the Higher Education Academy (study 2).
Competing interests None declared.
Ethics approval Institutional permission and ethical approval was obtained from all participating schools and Research Ethics Committees for both studies (30 medical, 15 nursing, 11 physiotherapy, 9 pharmacy and 5 dental).
Provenance and peer review Not commissioned; externally peer reviewed.
Data sharing statement No additional data are available.