Article Text

Abstract
Objective The goal of this present study was to determine the proportion of CCR5-tropic and CXCR4-tropic viruses and impact of tropism test on clinical presentation, CD4 cell counts, viral load and genotypic drug resistance from drug-naïve, voluntary counselling and testing (VCT) clients in southern Taiwan.
Design This was a cross-sectional study. Plasma samples were collected from HIV-1-infected patients from January 2013 to December 2013; subjects were recruited from free VCT centres in southern Taiwan.
Setting Taiwan.
Participants Plasma samples from 108 HIV-1-infected, treatment-naïve, VCT clients were analysed. HIV-1 strains were sequenced, genotype resistance was determined by a commercial kit (Viro-seq) and co-receptor tropism (CRT) was predicted by an internet tool geno2pheno[coreceptor], with a 10% false-positive rate as the cut-off. Differences in progression markers, patient characteristics, VCT questionnaires and HIV subtype distribution were evaluated statistically.
Results All the 108 VCT clients were male with 90% between the ages of 20 and 40 years. Eighty-eight per cent of the patients were men who have sex with men (MSM). The median (IQR) CD4 cell count was 342 cells/µL (221–454) and the viral load was 4.6 log (4.0–5.0). HIV-transmitted drug resistance was found in 9.3% (10/108) of the patients. CRT predictions indicated that 74% of the patients had only R5-tropic strains. CRT was not associated with CD4 cell counts, patient characteristics, VCT questionnaire and transmitted drug resistance. There was a significant difference with regard to viral load at the time of presentation, showing that patients with R5 more often had a higher viral load as compared with those with X4/DM strains (4.6±0.6 log vs 4.33±0.7 log, p=0.036).
Conclusions We found that 74% of the VCT clients were infected with R5-tropic virus strains. HIV-transmitted drug resistance was not associated with CRT predictions. Higher viral load at presentation was predictive of R5 co-receptor usage.
This is an Open Access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/
Statistics from Altmetric.com
Strengths and limitations of the study
This study uses a genotypic prediction system, which may result in a misclassification of the R5 virus as X4. The geno2pheno design is to predict unknown variants or variants with a poor sequence rather X4 instead of R5 and thus may result in an overcalling of X4.
Different co-receptor tropism prediction methods might yield different results.
Rescreening by Enhanced Sensitivity Trofile assay (ESTA) and population-based sequencing predicted similar virological response in the MERIT trial.
Study population consisted of young, mostly men who have sex with men, patients with HIV subtype B infection, and the results might not be generalisable to other subtypes and populations.
Introduction
HIV entry into host cells requires coordinated interactions of the envelope glycoprotein gp120 with the CD4 receptor and with one of the chemokine receptors, CCR5 or CXCR4.1–6 Pure CCR5-tropic and pure CXCR4-tropic virus can use only the CCR5 and CXCR4 co-receptors to enter target cells, while dual-tropic virus can use both co-receptors.1–6 The study of HIV-1 co-receptor usage has clinical significance due to its strong correlation with the rate of disease progression in HIV-1-infected individuals.7–9 Determining HIV-1 co-receptor usage is also important since the CCR5 co-receptor has become the target of a new class of anti-HIV-1 drugs that specifically inhibit the entry of CCR5-tropic HIV-1 strains into the target cells. Maraviroc was the first approved CCR5 antagonist and was used in clinical practice starting in 2007. Assessment of HIV-1 co-receptor usage is mandatory for the clinical use of this drug.10–14
Currently, the most widely used co-receptor tropism tests are the recombinant phenotypic Trofile assay (Monogram Biosciences) and its newer version, the Enhanced Sensitivity Trofile assay (ESTA).15 ,16 Despite their widespread use, there are some practical limitations to these assays, including a long turnaround time, restricted geographic access and the large sample volume they require. Genotypic tropism testing is an alternative method that is possible because the sequence of the third variable (V3) loop of gp120 is the principal determinant of tropism, allowing tropism inference using bioinformatic algorithms, such as PSSMx4/R5 and geno2pheno[coreceptor] (g2p).17–21 The use of maraviroc is recommended for the treatment of antiretroviral-resistant patients failing prior regimens and also antiretroviral-naïve patients.12 A previous study in Mainland China showed that patients with HIV subtype B strains were more sensitive to maraviroc compared to patients with HIV subtype CRF07_BC.22 Therefore, it is necessary to understand the HIV subtype distribution and tropism diversity in our community before using this drug.
In Taiwan, the impact of HIV epidemiological data, transmitted drug resistance, risk factor for HIV acquisition and co-receptor usage in HIV-infected treatment naïve individuals, are unknown. Our objectives were to establish the prevalence of co-receptor use among the voluntary counselling and testing (VCT) clients with HIV infection, and to establish the clinical and viral characteristics, and transmitted drug resistance associated with and predictive of the presence of CCR-5 using the virus.
Material and methods
Ethical statements
This study was approved by the institutional review board of the Kaohsiung Veterans General Hospital, Taiwan. The study complied with all ethical considerations involving human subjects. All information was obtained following standard clinical guidelines and all study participants understood the study procedure and provided signed informed consent.
Study population
Plasma samples collected from a consecutive group of individuals recruited from our free VCT centres at the Kaohsiung Veterans General Hospital from January 2013 to December 2013 (n=108) were analysed in this study. In Taiwan, 17 years ago, facilities offering VCT at no cost at the point of delivery were established and sponsored continuously by Taiwan Center for Diseases Control (CDC) as a key strategy to promote the early diagnosis and prevention of HIV, and others sexually transmitted diseases (STDs), and to stimulate referral to treatment. Taiwanese citizens can be tested for HIV infection for free, keeping anonymity, with easy access and in the context of a welcoming environment. For the study, the VCT procedure included a 30 min session of integrated pretesting and post-testing counselling; the clients then provided 5–10 mL of blood specimens for serological testing for HIV infection and syphilis. The VCT questionnaires recorded information including sociodemographics (age, sex, sexual orientation, occupation and education levels), sexual activity (numbers and timing of last anal/oral/vaginal intercourse partners, history of STD), history of substance abuse, participants’ attitudes towards the fear of acquiring or transmitting HIV/AIDS, frequency of condom use and reasons for access to VCT services.
Once the clients had received their reactive HIV ELISA or positive rapid test results, they were referred for clinical evaluation, western blot examination and treatment. HIV is a reportable disease in Taiwan and the government has been providing highly active antiretroviral therapy free of charge since its introduction in April 1997. The following laboratory exams were performed when the clients returned to the clinics, including the CD4 cell counts (FACS Flow, Becton Dickinson and Company, Franklin Lakes, New Jersey, USA), plasma viral load (Cobas Amplicor HIV-1 monitor test, V.1.5. Roche Diagnostics Corporation, Indianapolis, Indiana, USA), serological markers for syphilis, hepatitis A, B and C, Cryptococcus, toxoplasmosis, cytomegalovirus and amoebiasis, as well as cortisol level and liver, renal and thyroid function. The diagnosis of primary HIV-1 infection was based on any of the following: (1) patients who had recent high-risk behaviour, relatively high viral loads and normal CD4 counts, and compatible retroviral symptoms 3 months before serological positivity; (2) a positive enzyme immunoassay test for HIV-1 with indeterminate western blot results and one positive results for reverse transcriptase-PCR; or (3) negative serological tests 6 months prior to symptoms compatible with primary HIV-1 infection, with positive HIV ELISA and western blot results.23
Genotypic drug resistance testing
Resistance testing was performed on plasma samples using the ViroSeq HIV-1 Genotyping System version V.2.0, according to the manufacturer's instructions (Celera, Alameda, California, USA). Antiretroviral resistance mutations were interpreted with the HIVdb programme of the Stanford University HIV Drug Resistance Database. The patients classified as low-level resistance, intermediate resistance and high-level resistance were defined as having drug resistance.
Genotypic tropism testing
Viral RNA extraction, cDNA synthesis and nested PCR
RNA was extracted from 500 μL of blood plasma by QIAamp Viral RNA Mini kit (Qiagen, Hilden, Germany). The plasma underwent one hour centrifugation at 28 000×g at 4°C to concentrate the virus prior to extraction. The extracted viral RNA was eluted into a 60 μL aliquot and stored at −20°C or reverse transcriptase-PCR was initiated immediately after extracting. RNA was reverse transcribed with primer V3F1 (5′-GAGCCAATTCCCATACATTATTGT-3′) and V3R1 (5′-GCCCATAGTGCTTCCTGCTGCTCCCAAGAACC-3′). The RT-PCR reaction mixture contained 7 μL of RNA extract, ×2 Reaction Mix (a buffer containing 0.4 mM of each dNTP, 2.4 nM MgSO4), 5 mM magnesium sulfate, 1 μL SuperScript III One-Step RT-PCR System with Platinum Taq DNA Polymerase (Invitrogen) and 0.2 μM primer V3F1 and V3R1. The amplification profile for cDNA synthesis and first PCR was: 30 min at 60°C (cDNA synthesis), 2 min at 94°C, 40 cycles of (30 s at 94°C, 30 s at 55°C and 4 min at 68°C) and 7 min at 68°C. Then, the cDNA was amplified by a nested PCR protocol using primer V3F2 (5′-TGTGCCCCAGCTGG TTTTGCGAT-3′) and V3R2 in (5′-TATAATTCACTTCTC CAATTGTCC-3′). The cycling profile was 2 min at 95°C, 35 cycles of (30 s at 95°C, 30 s at 55°C and 3 min at 72°C) and 7 min at 72°C. After amplification, the product (5 μL) was detected by ethidium bromide staining on 1.5% agarose gels and the remaining volume (45 μL) was used for sequencing.13
Sequencing and prediction of CRT
The PCR product (45 mL) was purified using a QIAquick PCR Purification Kit (Qiagen, Heiden, Germany). The purified DNA was sequenced using a BigDye Terminator V.3.1 Cycle Sequencing Kit (ABI, USA), the mixture contained 3 μL of purified template, 2 μL of 3.1 big dye and 4 μL of the respective primer SQV3F (5′-AATGTCAGYACAGTACAATGTACAC-3′) and SQV3R (5′-GAAAAATTCCCTTCCACAATTAAA-3′). The cycle sequencing profile was 2 min of 96°C, 25 cycles of (96°C for 10 s, 50°C for 5 s and 60°C for 4 min) followed by incubation at 4°C. The sequencing fragments were purified using 75% 2-propanol.
Sequencing was performed on an ABI Prism 3130 Genetic Analyser. Using ReCall, a base calling software, automatic base for single primer coverage was performed and a ‘Fasta’ file was loaded. The CRT of all samples was predicted by using the geno2pheno[coreceptor] service at the following web site URL:http://coreceptor.bioinf.mpi-inf.mpg.de/index.php.
All of the samples were run in triplicate and the sequence prediction results above a false-positive rate of 10% were considered as CCR5 tropic. Those at or below a false-positive rate of 10% were considered CXCR4 or D/M tropic.
Statistics
Mann-Whitney U test were used to compare the median values of continuous variables between the two groups (R5 and X4), respectively, and Fisher's exact test was used to compare categorical variables between the two groups as appropriate. Logistic regression analysis was used to determine the factors associated with R5-tropic genotype. Variables with a p value of <0.2 from univariate analysis were included in the logistic regression model. The OR and its 95% CI were estimated. A two-sided p value <0.05 was considered to be statistically significant. Statistical calculations were performed using SPSS program V.12.0 (SPSS Inc, Chicago, Illinois, USA).
Results
From January 2013 to December 2013, a total of 4000 clients anonymously received VCT at our site with 120 clients (3%) being diagnosed as having HIV-1 infection. Among them, 108 patients returned for outpatient visits and none had had a history of exposure to antiretroviral drugs before. Primary HIV infection was identified in 21 patients. The median time (IQR) from VCT to first evaluation for CD4, viral load, CRT and resistance testing was 13 (8–21.7) days.
All 108 patients were male with 90% between the ages of 20–39 years. Eighty-eight per cent of the clients were men who had sex with men (MSM). Six per cent of the patients had self-reported having a history of STD. Sixteen per cent of the patients had ever used illicit drugs. Twenty-eight per cent of the patients had more than six sexual partners and most had experienced anal (84%) or oral sex (91%). More than 65% of the patients had unprotected sexual intercourse 3 months before presentation, and 55% of the clients never or seldom used a condom. The seroprevalence rate for hepatitis A, B and C were 9.3%, 13% and 4.7%, respectively. The prevalence rate for syphilis, amoebiasis (defined as indirect haemagglutination ≥1:32) and Toxoplasma gondii were 44.4%, 8% and 4.5%, respectively. One patient with CXCR4 virus had a higher (26 µg/dL) serum cortisol level (normal range 3.1–22.4 µg/dL) and two patients with CCR-5 tropic virus had lower serum cortisol levels (0.8 µg/dL and 1 µg/dL, respectively; table 1). The medium CD4 cell counts (IQR) were 342 (221–454) cells/µL, viral load (IQR) 4.6 log (4.0–5.0). All of the 107 patients were HIV subtype B, only one patient had subtype C. This patient was a sailor and he got HIV infection in India. Nine per cent (10/108) of the clients harboured transmitted drug resistance to antiretroviral drugs (table 1). One patient had a M184V mutation and all of the 10 subjects were resistant to non-nucleoside reverse-transcriptase inhibitors (NNRTI). No subject was resistant to protease inhibitors. The most common drug resistance associated mutations were V179D (n=4), K013N (n=2), G190A (n=1), M230L (n=1), Y188C (n=1) and V179E (n=1). CRT predictions indicated that 74% (80/108) of the patients had only R5-tropic strains. There was no difference in the frequency of X4 viruses in single analysis or triplicate testing. The distribution of FPR (%) among the 108 patients is shown in figure 1. There was no association between CD4 cell counts, risk factor for HIV acquisition by VCT questionnaires, HIV subtype, opportunistic infection markers and transmitted drugs resistance with presence of R5-tropic virus. The factor associated with presence of R5-tropic virus in single variance analysis was plasma viral load (4.6±0.6 vs 4.33±0.7), p=0.036, 95% CI 1.05 to 4.33 (tables 2⇓–4 and figures 2 and 3). After we excluded 21 patients with primary HIV infection who were thought to have a higher viral load, the statistics were still found to be significant (p=0.037). Age, anti-HCV antibody positive and plasma viral load that had a p value of <0.2 were put into a logistic regression model, and we found that those patients with a higher viral load were still at a statistically significantly higher risk of being infected with R5-tropic viruses, with an adjusted OR of 2.07 (95% CI 1.024 to 4.193; p=0.043).
Demographic data and HIV drug resistance among 108 HIV-1-infected treatment naïve VCT clients
The sociodemographic and sexual history in VCT questionnaires among 108 attendees in southern Taiwan
Correlation of clinical manifestations, laboratory data and chemokines co-receptor tropism usage among 108 VCT attendees in southern Taiwan
Correlation of VCT questionnaires and chemokines co-receptor tropism usage among 108 VCT attendees in southern Taiwan
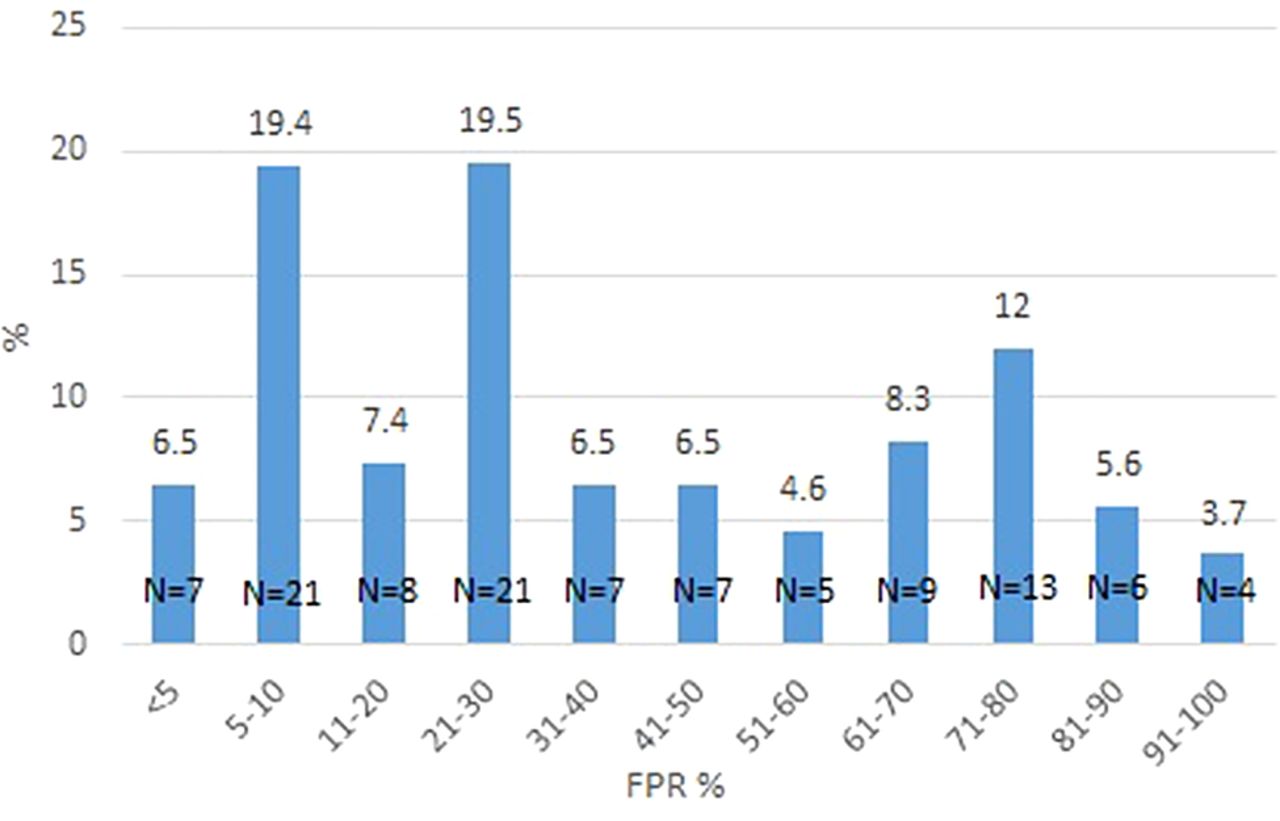
The distributions of false-positive rate (FPR) % for CRT among 108 patients are shown in figure 3. A total of 74% of the patients had only R5-tropic strains (FPR 10%).
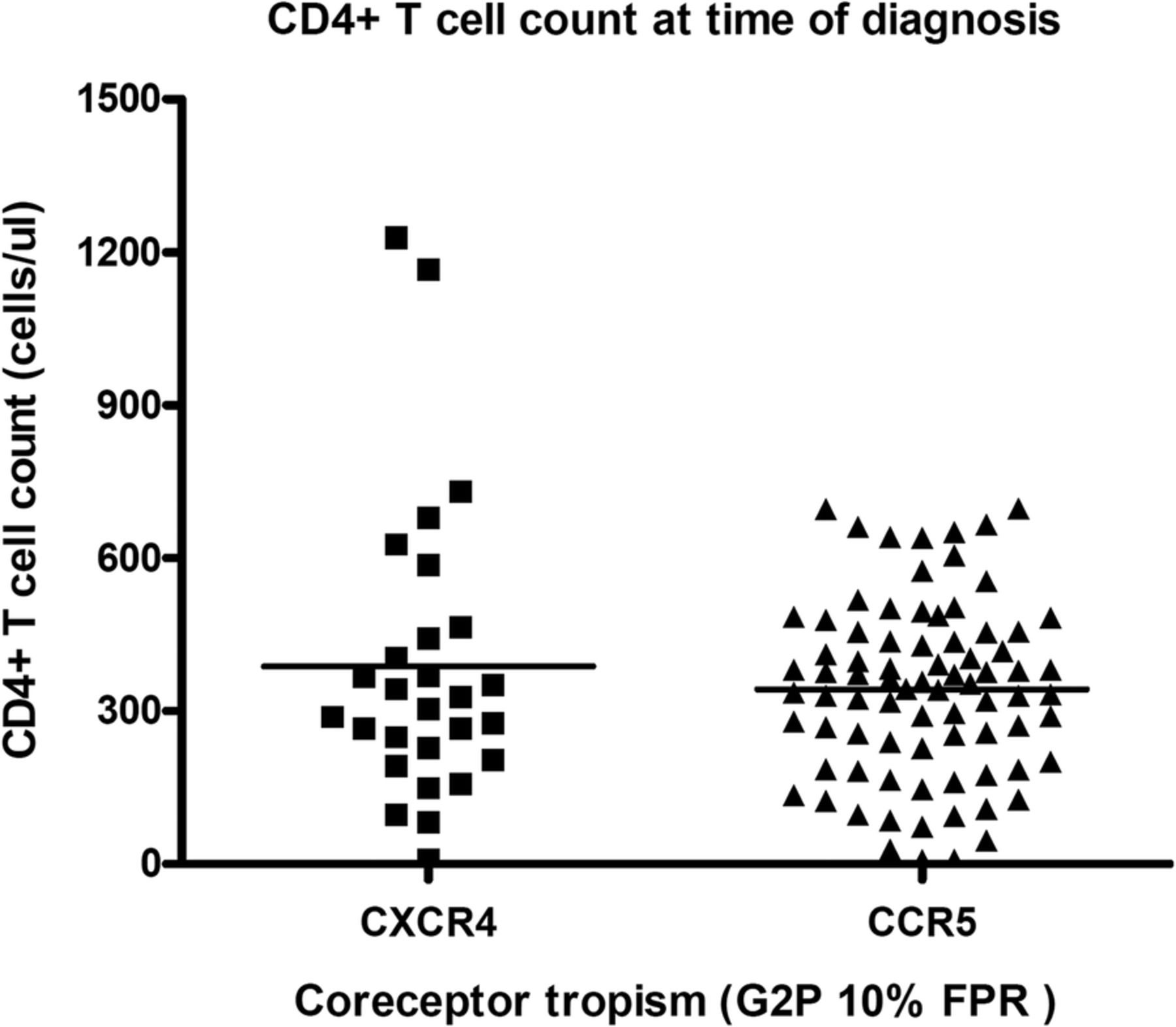
The CD4T cell counts were not statistically different among 108 patients with CCR-5 tropic and CXCR4 tropic virus.

{kind=link}
{kind=link}
{kind=link}
The plasma viral load was higher in patients with CCR-5 tropic virus as compared to CXCR4 tropic virus (4.6±0.6 vs 4.33±0.7, p=0.036).
Discussion
We observed a significant association among HIV-1 RNA load and chemokine co-receptor use. Patients with R5-tropic virus had higher plasma viral load compared to patients harbouring X4/DM strains. Associations between HIV-1 RNA load and CD4 cell count, and co-receptor usage, have been reported elsewhere.7–9 Co-receptor use has been considered as a determinant of disease progression, and those individuals with virus using the CCR5 co-receptor generally have a slower rate of progression and lower viral load than those with virus using CXCR4. The treatment of HIV-infected individuals by using CCR5 antagonists represents a new therapeutic advance that may require a reliable determination of co-receptor use status.10–12
Previous studies in Western countries, where HIV-1 subtype B predominates, reported that 80–90% of untreated HIV-1-infected patients24 harboured R5 strains. In a study from Spain, the researchers showed that 13.4% of the 67 HIV-1 seroconverters harboured CXCR4 viruses.25 A French study also showed that 15.9% of 390 primary HIV subtype B infection contained X4 viruses.26 In a sexually infected HIV and treatment naive cohort from China, researchers found that the CRF01_AE subtype was predominant (46%), especially in the MSM group. The study revealed that the proportion of X4 tropism was higher in the CRF01_AE subtype (45.5%) than in others (C/CRF07_BC/CRF08_BC, 4.3%; B, 6.1%; p<0.001). CRF01_AE subtype was associated with faster progression to AIDS.27 Another study from Hong Kong by To et al,28 showed that the prevalence of Dual/Mixed-virus or X4-tropic virus in antiretroviral-naive subtype CRF01_AE was 24% (21/87), which was significantly higher than subtype B 14% (15/104) if using geno2pheno[coreceptor] with a 10% false-positive rate as the cut-off.
Our study showed that only 74% of treatment naïve patients had R5-tropic virus. The results in our study were similar to the study of Meini et al,29 which showed that 26.2% of HIV infected treatment-naïve patients in Italy had non-CCR5-tropic viruses. This discrepancy in prevalence of co-receptor use in different studies might be due to the different patient populations, stage of HIV infection (primary vs chronic infection) and methodology of co-receptor use tropism. Studies, such as ours, based on genotypic methods, generally reported a higher CXCR4 prevalence.
We also did not find a strong association between a low CD4 count at baseline and the detection of X4 virus. Otherwise, the R5-tropic virus had a higher viral load as compared to the X4 strain. The statistics were still significant even though we excluded 21 patients with primary HIV infection who supposedly had an initially high baseline viral load. This discrepancy may be explained by the relatively small case numbers in our series, and different patient populations. Our patients were inducted from those VCT attendees with higher CD4 cell counts and were infected relatively recently. This could explain why they possessed relatively higher viral loads in contrast to other studies showing that patients harbouring the X4 strain had a higher viral load. Further study is clearly needed to confirm this hypothesis.
HIV-transmitted drug resistance was 9.3% (10/108) in our VCT clients. In Southeast Asia, HIV-transmitted drug resistance rate was around 4–12%, including 3.8% in China,30 7.7% in Japan,31 12% in South Korea,32 4.9% in Thailand33 and 8% in northern Taiwan.34 Resistance rates varied according to the different populations enrolled. However, there are no data on the prevalence of HIV drug resistance in southern Taiwan, especially in those MSM receiving VCT. The samples from the 10 patients displayed NNRTI-related resistance mutations. Since NNRTIs are the backbone of first-line antiretroviral therapy in Taiwan, further large-scale studies conducted on the transmission patterns or trends in drug resistance were would be welcome.
Our study had a number of limitations that should be highlighted. First, we used a population genotypic prediction system, which may result in a misclassification of the R5 virus as X4. More sensitive ultradeep pyrosequencing (UDS) can provide multiple orders of magnitude greater than conventional sequencing and can detect minority CXCR-4 using variants, but clinical superiority has not been validated so far.35 UDS and the phenotype were concordant for determining HIV-1 co-receptor usage during primary HIV infection.36 Second, different co-receptor tropism prediction methods (such as Web PSSM and Wet Cat) might yield different results. Furthermore, our study population consisted of young patients with MSM with HIV subtype B infection, and the results might not generalised to other subtypes and populations. Finally, the V3 loop was not the only determinant of tropism and, therefore, tropism predictions based on V3 loop sequences might not be accurate.
In summary, our study revealed a high (9.3%) transmitted drug resistance rate among VCT clients. This finding reminds us of the urgent need for the improvement and implementation of a comprehensive public health strategy for HIV-1-transmitted drug resistance prevention. Chemokine co-receptor tropism of HIV is associated with HIV-1 RNA levels, and not associated with CD4 cell counts, viral subtype and clinical risk factors. The clinical impact of high viral load on patients’ initiation of treatment with chemokine co-receptor antagonists remains to be determined.
References
Footnotes
Contributors THC, WSR and LSJ participated in the study design and preparation of the manuscript. THC, CPY and CYS participated in the laboratory experimental work and in interpretation of the data. All authors read and approved the final manuscript.
Funding This study was funded by Veterans General Hospitals and University System of Taiwan Joint Research Programme grant. VGHUST102-G3-1-1
Competing interests None declared.
Ethics approval This study was approved by the institutional review board of the Kaohsiung Veterans General Hospital, Taiwan.
Provenance and peer review Not commissioned; externally peer reviewed.
Data sharing statement The data cannot be shared without IRB approval. NO additional unpublished data can be shared.