Article Text

Abstract
Introduction Low back pain is the highest ranked condition contributing to years lived with disability, and is a significant economic and societal burden. Evidence-based clinical practice guidelines are designed to improve quality of care and reduce practice variation by providing graded recommendations based on the best available evidence. Studies of low back pain guideline implementation have shown no or modest effects at changing clinical practice.
Objectives To identify enablers and barriers to adherence to clinical practice guidelines for the management of low back pain.
Methods and analysis A systematic review and meta-synthesis of qualitative studies that will be conducted and reported using the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) Statement guidelines. Eight databases will be searched using a priori inclusion/exclusion criteria. Two independent reviewers will conduct a structured review and meta-synthesis, and a third reviewer will arbitrate where there is disagreement. This protocol has been registered on PROSPERO 2014.
Ethics and dissemination Ethical approval is not required. The systematic review will be published in a peer-reviewed journal. The review will also be disseminated electronically, in print and at conferences. Updates of the review will be conducted to inform and guide healthcare translation into practice.
Trial registration number PROSPERO 2014:CRD42014012961. Available from http://www.crd.york.ac.uk/PROSPERO/display_record.asp?ID=CRD42014012961
- PRIMARY CARE
- QUALITATIVE RESEARCH
This is an Open Access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/
Statistics from Altmetric.com
Strengths and limitations of this study
We will systematically identify and critically appraise the available evidence and grey literature on this important question, and identify research findings.
We have endeavoured to reduce bias by using a priori inclusion/exclusion criteria, data extraction and method quality assessments ensuring a range of supporting quotes from across the included studies.
The study screening, data extraction and assessment of risk of bias will be conducted independently by two authors, and a third will arbitrate on any disagreements.
The first limitation is that the process decontextualises data, removing it from the context in which it was originally presented or reported. Our access to this original context will be limited to the primary research report, which could omit contextual factors.
The second limitation is that a meta-synthesis of this nature does not analyse original data; the synthesis relies on the sample of data reported by the primary researchers.
The inclusion of only English language publications, due to a lack of translation resources, means there is some potential for cultural and publication bias in the findings.
Introduction
Low back pain (LBP) is the highest ranked condition contributing to years lived with disability, according to the most recent Global Burden of Disease study.1 ,2 It is a significant source of long-term disability and absence from work, and a substantial economic and societal burden. Non-specific LBP, a term that underscores that a precise pathoanatomical diagnosis usually cannot be reached,3 accounts for approximately 85% of all LBP instances in primary care, and is most commonly characterised by periodic recurrences and remissions.4–7 It is managed in highly diverse and modestly effective ways in primary care.8
Over the past decade, clinical practice guidelines for the management of LBP have been developed and published in many parts of the world.9–13 Evidence-based clinical practice guidelines are designed to improve quality of care and reduce practice variation by providing graded recommendations based on the best available evidence. However, uptake of guideline recommendations is often incomplete and slow, and there continues to be a mismatch between routine clinical practice and the content of evidence-based clinical practice guidelines both in general,14–18 and in LBP in particular.19 Although many primary care clinicians approve of the content of the LBP guidelines, evidence suggests that they do not routinely adhere to the guidelines in their actual clinical practice.19–22
Studies of LBP guideline implementation have shown no or modest effects at changing clinical practice.23–25 The lack of clarity about how to effectively implement guidelines in ways that do change practice is generic across healthcare and not restricted only to LBP.25 Studies of guideline adherence that use quantitative methods can determine how commonly clinicians adhere to recommended practice, and studies that use qualitative methods are better suited to identifying the enablers and barriers to greater adherence. Identification of these factors provides insight into current clinical practice, and may inform the design of better guidelines and better implementation strategies.
The fact that many different primary and secondary care clinicians, including general and specialist medical practitioners, physiotherapists, osteopaths and chiropractors, who manage LBP, hold a range of attitudes and beliefs about the condition and its management, poses considerable challenges and frustrations, for patients as well as for practitioners.26 ,27 The factors that have been identified as effect modifiers to adherence with guidelines among medical and allied health professionals, include the experience and beliefs of the health professional, whether the implementation strategy focuses on changing simple or complex behaviours, the perceived advantage of using the guideline, and compatibility between current practice and recommendations.20 ,28–30
Aims
We will conduct a systematic review of qualitative empirical studies that explore what primary care clinicians perceive and believe about clinical practice guidelines for the management of LBP, and that may act as enablers and barriers to guideline adherence.
Methods and design
This protocol has been registered on PROSPERO 2014 (registration number: CRD42014012961), is available at http://www.crd.york.ac.uk/PROSPERO and is reported according to the PRISMA-P checklist.31 This structured review process was adapted from the Cochrane Collaboration Guidelines, and will be conducted and reported using the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) Statement guidelines, and the COnsolidated criteria for REporting Qualitative research (COREQ) checklist.32–34
Inclusion and exclusion criteria
Studies will be included if they are qualitative studies that include primary care clinicians (eg, general medical practitioners, physical therapists, chiropractors, etc) who manage LBP; use qualitative methods for both data collection (eg, focus groups, interviews) and analysis; and if the analysis describes the barriers and enablers to adherence with LBP guidelines. Mixed method studies will be eligible if the qualitative data are analysed separately to the quantitative data. Papers will be excluded if not published in English (due to a lack of translation resources) or if quantitative methods only are used.
Identification and selection of included papers
We will use a comprehensive set of search strategies recommended for identifying qualitative reports.35–39 We will search eight electronic databases including MEDLINE (see online supplementary appendix 1), EMBASE, The Cochrane Central Register of Controlled Trials, AMED, PsychInfo and Sport Discus, perform a manual search of reference lists and Citation Tracking of relevant studies to identify additional papers, and consult content experts. The search will be conducted without date limits up to July 2014, using explosions and combinations of key search terms including, for example, qualitative research, back pain, guidelines, clinical practice, quality assurance, decision rules, clinical reasoning, behaviour, attitudes, perceptions, adherence, compliance, barriers. Study selection will be documented and summarised in a PRISMA compliant flow chart (figure 1).

Flow diagram of the selection process.
The search results will be downloaded to a reference database and, after deletion of duplicates, one reviewer (PK) will perform initial screening of titles by applying the a priori inclusion/exclusion criteria. Two independent researchers (PK and SCS) will then screen titles and abstracts of remaining references, and perform full-text review as necessary to identify those studies that fulfil selection criteria. Disagreements will be resolved through discussion with a third reviewer (RB) if consensus cannot be reached.
Method quality assessment
We will use the example of Slade et al (2013) for the method quality appraisal process.40–43 Pairs of independent reviewers will appraise the identified studies using the Critical Appraisal Skills Programme (CASP) checklist for qualitative studies because it provides decision rules and detailed instructions on how to interpret criteria.44 This checklist consists of a series of questions that help the reviewer to assess the rigour, credibility and relevance of the study. Rigour applies to whether the approach to the study is thorough and appropriate; credibility indicates whether the findings are well presented and meaningful, and relevance represents the usefulness of the study's findings to the review.43 Disagreements will be resolved by consensus or by discussion with a third reviewer if necessary.
Data extraction
The following data will be systematically extracted, by independent pairs of reviewers, under the following main headings: methods, population, data collection, data synthesis (themes and supporting quotations), results, discussion, conclusions and recommendations. The completed data extraction forms will be examined for consistency and merged for the data synthesis phase. Themes and subthemes will be extracted from each published report, independently confirmed by the pairs of reviewers and transferred to an Excel spreadsheet (Microsoft Corp, Redmond, Washington, USA). The items will be assembled into common groups and duplicates deleted to remove ambiguity.
Data analysis/synthesis
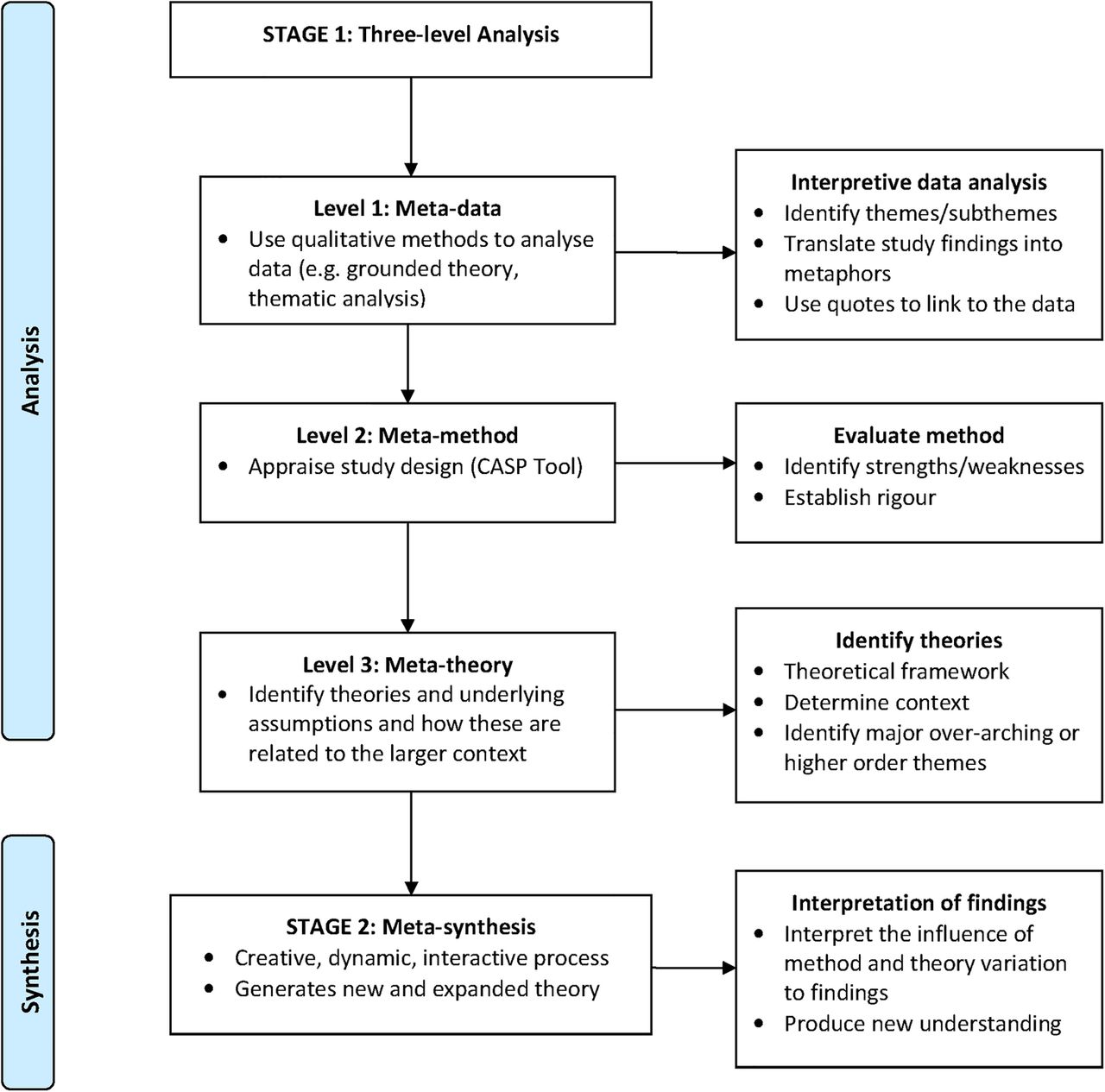
Two independent reviewers (SCS and SP) will conduct data analysis and the primary studies will be combined, compared and contrasted to generate meaning that extends beyond any individual study using thematic analysis in a Grounded Theory framework.45 During data extraction, the author-stated themes and subthemes from each paper will be extracted, and a thematic framework developed for the entire data set. This involves reading all of the included papers in depth, noting the major themes reported in all of the papers and then developing a thematic framework which encompasses all of the themes identified in the papers. This framework will then be applied to the extracted data and used to develop analytical charts to manage the data.46–48 The data analysis methods will be documented in a meta-synthesis flow chart (figure 2).

{kind=link}
{kind=link}
Flow diagram of the process into the review meta-analysis methods (CASP, Critical Appraisal Skills Programme).
Data management will begin with familiarisation with the data and noting of recurrent themes across the studies, constructing an index and labelling the data with the index. The data will then be sorted by theme and summarised in a series of matrix-based charts, retaining the context and language used by the individual authors. Charting the data will enable us to compare how the same theme was explained and interpreted within different studies, and whether there are recurring themes. The descriptive analysis will identify dimensions within the data, categorise these and group them into sets of categories. The explanatory analysis will identify links between sections of, and subgroups within, the data to explore why such associations and subgroups exist.
The independent researchers will conduct thematic analysis;45 consult at stages during the process and identify major over-arching or higher order themes. We will summarise the themes and subthemes from each paper, and summarise how the authors of each paper explain and interpret common understandings. Relevant text citations and quotes that substantiate the themes will be tabulated, and linked to the papers by title and page number. The reviewers will collapse the author-derived themes into over-arching themes for all the included studies. We will consider some common domains that are known to influence adherence, such as clinician knowledge and professional background, cultural, environmental and patient-driven factors and categories of LBP guideline recommendations such as imaging, activity and medication. The relative importance of the enablers and barriers, contrasts in beliefs and perceptions between types of clinicians, and the possible impact on clinical practice, may be analysed and reported if there are adequate reported data. Comparisons between the type of study and the emergent data will be made where possible or where data are provided.
In summary, the general framework for the synthesis comprises four main elements: (1) developing a theory; (2) developing a preliminary synthesis of findings of included studies; (3) exploring relationships in the data and (4) assessing the robustness of the synthesis. The synthesis will be further evaluated by the entire team to identify contextual and methodological factors that have influenced the published results.
Results
The results will be presented textually, with flow charts, summary tables, key emergent themes and supporting quotations linked to the text.
Discussion
We have presented the rationale and design of a systematic review of qualitative studies that investigate primary care clinician beliefs or perceptions about what are barriers and enablers of their adherence to clinical practice guidelines for the management of LBP. It is anticipated that the review will identify barriers and drivers to practice change. The results will inform research into improved uptake of clinical practice guidelines and future interventions for effective guideline implementation.
References
Supplementary materials
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
Files in this Data Supplement:
- Data supplement 1 - Online appendix1
Footnotes
Twitter Follow Tracey Bucknall at @TraceyBucknall@nursedecisions
Contributors RB conceived the idea for the study. RB, SCS, PK, EM, TB and SP were responsible for the study design and protocol. SCS drafted the protocol manuscript with input from RB, PK, TB, EM and SP. SCS, RB, PK, TB, EM and SP have read and approved the final manuscript. The corresponding author guarantees that the authorship statement is correct.
Competing interests None declared.
Provenance and peer review Not commissioned; externally peer reviewed.