Article Text

Abstract
Objectives The aim of this study was to investigate the surgical revision rate in patients with chronic rhinosinusitis (CRS) in the UK CRS Epidemiology Study (CRES). Previous evidence from National Sinonasal Audit showed that 1459 patients with CRS demonstrated a surgical revision rate 19.1% at 5 years, with highest rates seen in those with polyps (20.6%).
Setting Thirty secondary care centres around the UK.
Participants A total of 221 controls and 1249 patients with CRS were recruited to the study including those with polyps (CRSwNPs), without polyps (CRSsNPs) and with allergic fungal rhinosinusitis (AFRS).
Interventions Self-administered questionnaire.
Primary outcome measure The need for previous sinonasal surgery.
Results A total of 651 patients with CRSwNPs, 553 with CRSsNPs and 45 with AFRS were included. A total of 396 (57%) patients with CRSwNPs/AFRS reported having undergone previous endoscopic nasal polypectomy (ENP), of which 182 of the 396 (46%) reported having received more than one operation. The mean number of previous surgeries per patient in the revision group was 3.3 (range 2–30) and a mean duration of time of 10 years since the last procedure. The average length of time since their first operation up to inclusion in the study was 15.5 years (range 0–74). Only 27.9% of all patients reporting a prior ENP had received concurrent endoscopic sinus surgery (ESS; n=102). For comparison, surgical rates in patients with CRSsNPs were significantly lower; 13% of cases specifically reported ESS, and of those only 30% reported multiple procedures (χ2 p<0.001).
Conclusions This study demonstrated that there is a high burden of both primary and revision surgery in patients with CRS, worst in those with AFRS and least in those with CRSsNPs. The burden of revision surgery appears unchanged in the decade since the Sinonasal Audit.
This is an Open Access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/
Statistics from Altmetric.com
Strengths and limitations of this study
Large cohort of patients from secondary and tertiary care centres around the UK.
Chronic rhinosinusitis is a common disease and sinonasal surgery is frequently undertaken.
The data are derived from self-reported questionnaire responses by patients.
There is selection bias as only symptomatic patients returning to secondary care are included in the study.
Introduction
Rhinosinusitis is one of the most common chronic adult health problems in the Western world with a recent European study estimating the prevalence of chronic rhinosinusitis (CRS) at 11%,1 although in studies with physician-led diagnosis of CRS, a prevalence of 6–7% has been observed.2 ,3 Sinonasal surgery for patients with CRS is commonly performed by otorhinolaryngologists around the UK. Hospital Episode Statistics (HES) data for 2012–2013 suggest that approximately 40 000 nose or sinus operations are performed each year in England and Wales; this is in addition to an estimated 75 000 outpatient consultations.3 Patients selected for surgical intervention should have failed to improve symptomatically on medical treatment, but there is a greater than fivefold variation in intervention rates across the UK.4 This variation may reflect a number of factors including both underutilisation and overutilisation of surgery, a lack of guidelines and a lack of evidence in well-constructed randomised controlled trials (RCTs) to support surgery;5 a 2005 Health Technology Assessment commissioned systematic review of sinus surgery identified the need for good quality studies comparing surgery with medical treatment for CRS with nasal polyps (CRSwNPs).6 Furthermore, the duration of uncontrolled symptoms before surgery varies considerably between 1 and 10 years.7 This uncertainty regarding the role of surgery is highlighted by its inclusion in the National Institute for Health and Care Excellence (NICE) Database of Uncertainties about the effects of treatment (DUETs).8 Although level 1 evidence is lacking, recent studies evaluating the symptomatic and economic benefits of surgical intervention in CRS outside of the UK National Health Service (NHS) setting favour surgical intervention over ongoing medical therapy.9–12
In 2000–2001, a total of 3128 consecutive patients undergoing surgery for CRS at 87 NHS hospitals were enrolled as part of the UK Sinonasal Audit coordinated through the Clinical Effectiveness Unit at the Royal College of Surgeons of England.13 All of the 156 NHS Trusts in England and Wales performing sinonasal surgery were invited to take part in the Audit; those who failed to participate largely cited financial constraints as the reason for refusal. All patients aged 16 years or more and who had elected to undergo surgical procedures to treat nasal polyposis and/or CRS were eligible for inclusion. Although this study concluded that sinonasal surgery is generally safe and effective and that patient selection for surgery could be improved, the subsequent long-term follow-up of audit patients also demonstrated the limitations of sinus surgery in current practice.14 From the 1459 patients who responded to 5-year follow-up, revision surgery rates increased at each time point such that 19.1% had undergone further sinonasal surgery during the 5 years since their original operation. In CRSwNPs, 20.6% had undergone revision compared with 15.5% of patients with CRS without nasal polyposis (CRSsNPs). Looking at cases where a simple polypectomy was performed, 21.2% had undergone revision surgery compared with 20.0% of patients who had also received additional sinus surgery with an adjusted OR of 0.66 (p=0.04) for the risk of the latter group needing further surgery.
Given these interventions occurred 13–14 years ago during which time there have been advances in instrumentation and visualisation for sinonasal surgery, the CRS Epidemiology Study (CRES) provided an opportunity to revisit this scenario using recent data. CRES prospectively collected a national cohort of self-reported patient data in the UK (excluding Northern Ireland). The overarching aim of the CRES was to identify any difference in socioeconomic variables between patients with CRS and healthy controls using a study-specific questionnaire which included demographic and socioeconomic questions as well as disease-specific and generic quality of life tools. The study included a qualitative arm exploring patient experiences in detail. The CRES questionnaire also allowed collection of information about previous surgical interventions, allowing us to investigate surgical revisions and allow comparison of management between subgroups of CRS. Revision surgery is herein defined as any further surgical intervention for CRS (ie, repeated nasal polypectomy or repeated endoscopic sinus surgery (ESS).
Materials and methods
The CRES was sponsored by the University of East Anglia (UEA). Any patients presenting to secondary care outpatient clinics and diagnosed by an otorhinolaryngologist with CRS as defined by the criteria laid out in the European Position Paper on Rhinosinusitis and Nasal Polyps (EPOS) were invited to participate in the study regardless of symptom or disease severity or duration and regardless of any prior interventions. The study initially started recruitment in the East Anglia region of the UK but following elevation to the National Institute of Health Research Clinical Research Network Portfolio, a total of 30 sites from around the UK (including the devolved nations of Wales and Scotland) joined the study which ran between 2007 and 2013. The study-specific questionnaire was anonymous, and therefore no consent was taken but implied through their participation. Patients were classified by subgroup of CRS (CRSsNPs, CRSwNPs or allergic fungal rhinosinusitis (AFRS) by a clinician prior to completion of the questionnaire using the EPOS definitions for with or without polyps (using endoscopic and/or radiological confirmation) and the Bent and Kuhn criteria for AFRS. Questionnaires were either completed before leaving the clinic or taken home and returned by post in freepost envelopes. The returned questionnaires were then scanned into a database electronically but checked by two members of the research team for accurate correlation with the paper questionnaire and for missing data. The study questionnaire includes study-specific questions relating to socioeconomic, environmental and medical comorbid variables as well as the validated Short Form 36 (SF-36)15 quality of life measure and the Sino-Nasal Outcome (SNOT-22)16 questionnaire. A pilot study demonstrated incomplete responses to the question “Have you ever had any nasal surgery?” due to some participants excluding sinus surgery from their responses. The questionnaire therefore stated “Have you had any previous surgery—yes/no?; If yes, please specify what and when”, followed by a free field text box. This captured all forms of sinonasal surgery; the frequency of surgery and any other type of surgery undergone by participants and the dates provided by participants varied from exact dates to just the year of surgery. The self-reported questionnaire was the only means of data capture in relation to surgery. These surgery-specific data were collated and subcategorised where data were available (see flow chart). If participants did not complete the surgery text box, they were assumed not to have undergone any previous surgery and as such there were no missing data in this respect. The duration of time since the most recent surgical intervention provided and completion of the questionnaire is described as ‘recurrence time’. The study was powered based on the ability to detect differences in quality of life between cases and controls since this was the primary purpose of the study. The percentage of respondents with previous surgeries were compared across the three subgroups (CRSsNPs, CRSwNPs and AFRS) using a χ2 test. The mean SNOT-22, surgical impact and time to recurrence were compared between the three subgroups using analysis of variance (ANOVA).
Results
A total of 1470 completed questionnaires were returned by participants including 1249 patients with CRS, reflecting a response rate across all sites of 66%. The age range of all participants was 18–102 years, mean 52.6 years, with 709 men and 606 women (155 did not identify their gender; see figure 1 flow chart). Patients with CRS diagnosed by their ENT surgeon included 651 with CRSwNPs, 553 with CRSsNPs and 45 with AFRS. From the total of 1249 CRS participants, 556 (45%) had undergone some form of sinonasal surgery (defined as one or more of polypectomy, ESS, septoplasty, turbinate surgery, rhinoplasty) including 325 (26%) who had received at least one nasal polypectomy and 169 (14%) who had undergone at least one instance of ESS (figure 2).

Flow chart for inclusion of surgical data from CRES (CRS, chronic rhinosinusitis; CRES, CRS Epidemiology Study).

Frequency of sinonasal surgery (AFRS, allergic fungal rhinosinusitis; CRSsNPs, chronic rhinosinusitis without nasal polyps; CRSwNPs, chronic rhinosinusitis with nasal polyps).
Combining data for the subgroups of CRSwNPs and AFRS (n=696), 396 (57% of those with CRSwNPs or AFRS) reported previous ‘sinonasal surgery’ of which 99/696 (14%) reported having undergone ESS and 315/696 (45%) nasal polypectomy. Looking specifically at patients with CRSwNPs who underwent a polypectomy (n=281), only 30% (n=85) reported concurrent ESS. In cases of CRSsNPs (n=553), only 160 (29%) patients reported sinonasal surgery in whom 70 (13%) specifically reported ESS (see table 1 for summary data). A χ2 test showed that the difference between the subgroups was highly significant (p<0.001). Other nasal procedures specifically reported included septoplasty and turbinate surgery.
Summary data (percentages expressed with total in each subgroup as the denominator)
Considering multiple procedures, 157 of 315 patients with CRS who reported having undergone a nasal polypectomy previously (50%) had received more than one operation with a mean number of 3.3 polypectomies (range 2–30; figure 3). In contrast, in the CRSsNPs subgroup, 21 of 160 (13%) participants reported repeated sinonasal surgery. A χ2 test showed that the difference between the subgroups was again highly significant (p<0.001).
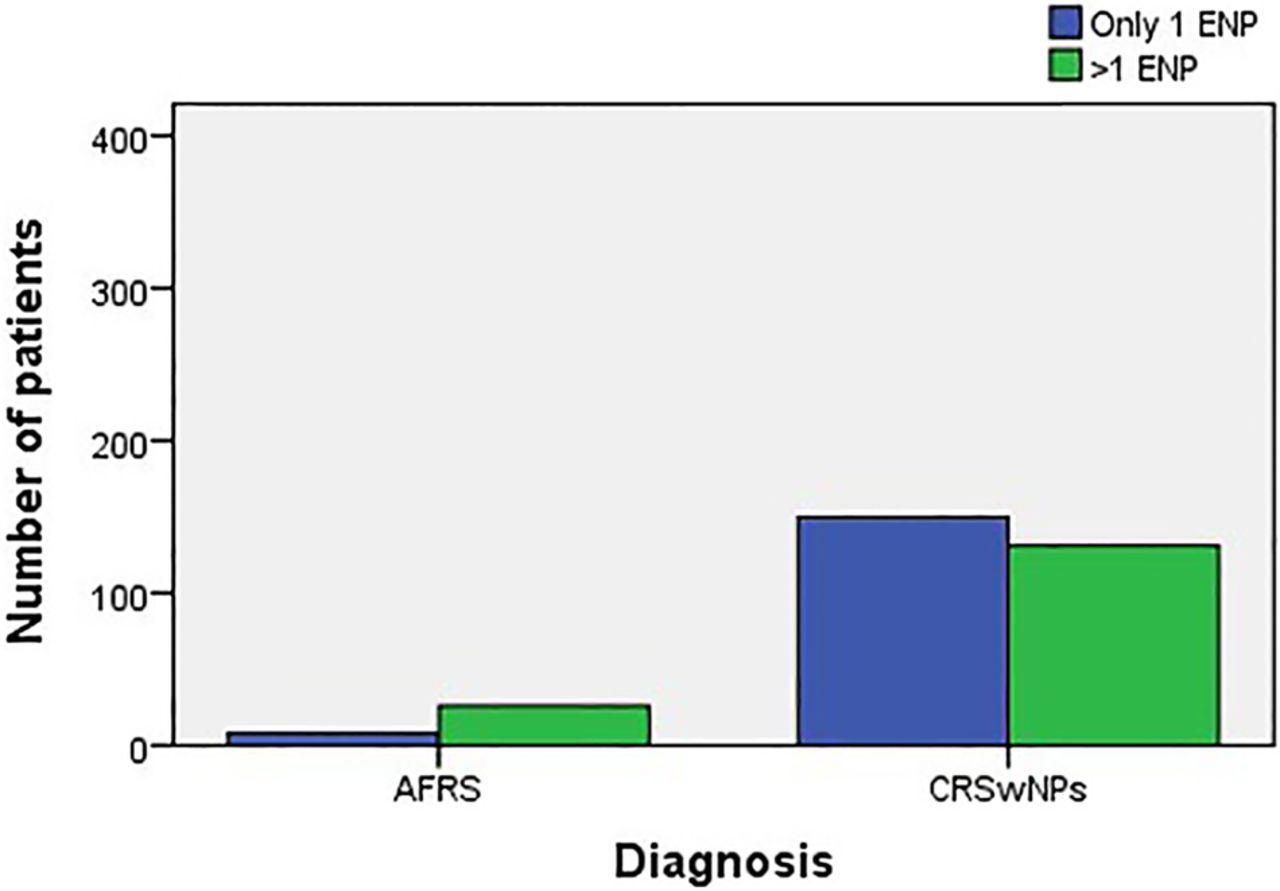
Frequency of multiple ENPs being performed in patients who have previously undergone surgery. AFRS, allergic fungal rhinosinusitis; CRSwNPs, chronic rhinosinusitis with nasal polyps; ENP, endoscopic nasal polypectomy.
Looking at the timeline for participants who underwent sinonasal surgery, 318 reported dates for surgery, with the average duration from first reported surgery to inclusion in the study being 15.5 years (range 0–74; table 2 and figure 4). Although patients may have become asymptomatic for periods between interventions, these data give a perspective on the chronicity of the disease (from first intervention), especially as many patients will have been symptomatic for months to years before the first referral to secondary care. The duration of time since the most recent surgical intervention to completion of questionnaire (most current consultation) is called ‘recurrence time’ and ranged from 0 to 70 years with a mean of 10 years for all CRS but notably a mean of 3.68 in patients with AFRS, being significantly shorter than CRSwNPs (p=0.005; table 3 and figure 5). The median interval for revision surgery in patients with AFRS was 2 years.
Surgical impact data
Time to recurrence data
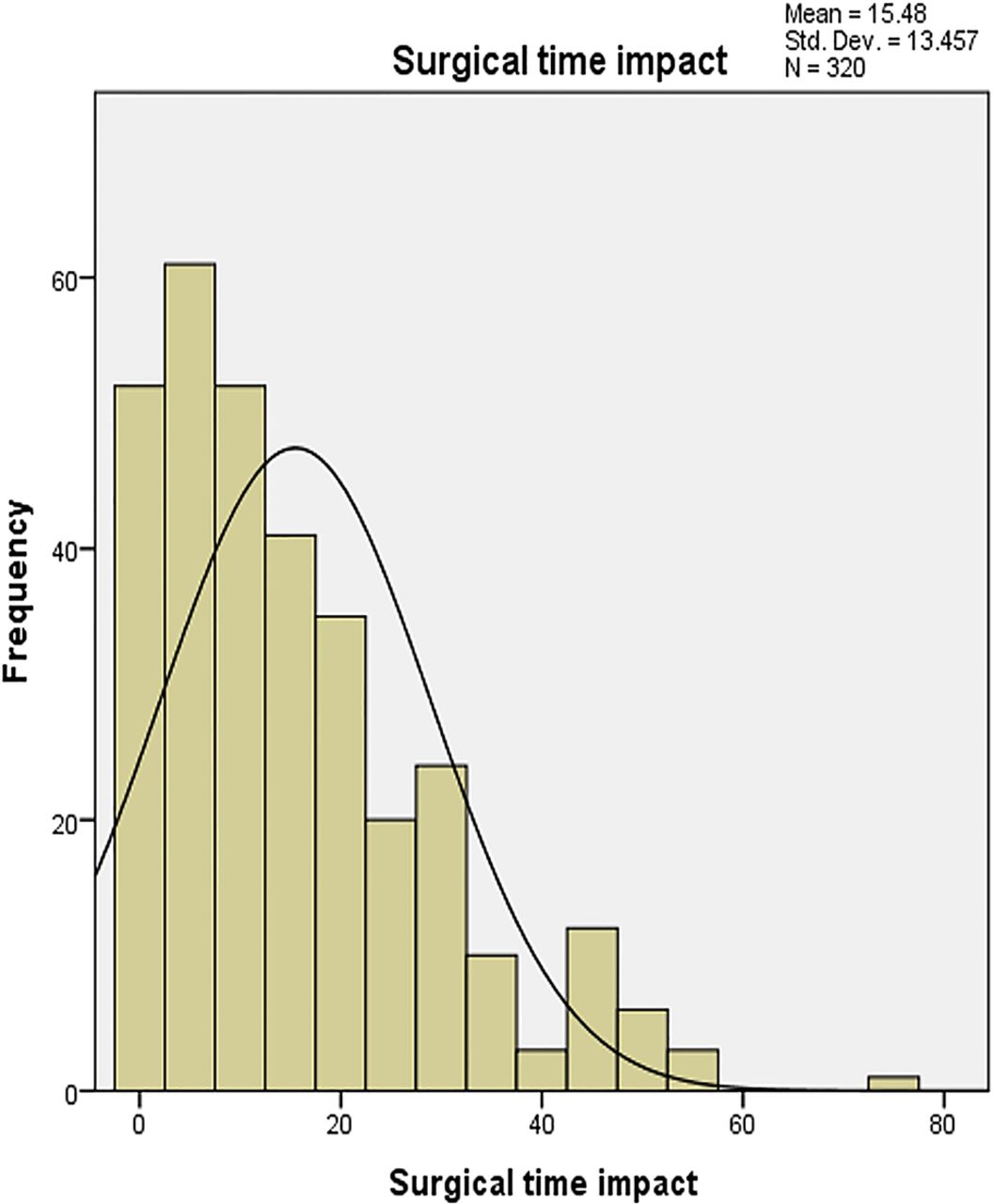
Duration of time since first sinonasal surgery for patients with chronic rhinosinusitis with nasal polyps (surgical time impact).

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Duration of time since most recent surgery in patients with chronic rhinosinusitis with nasal polyps (recurrence needing secondary care input).
Asthma and aspirin-exacerbated respiratory disease were significantly more likely to be present in patients who had had multiple surgeries (60% asthma, 35% AERD) than those who had not (43% and 11%; χ2 p>0.001). Finally a comparison in SNOT-22 scores between patients with CRSwNPs/AFRS who have had multiple endoscopic nasal polypectomies (ENPs) and those who reported no surgery shows a significantly higher mean score in the multiple surgery group (45.6 vs 37.9; p=0.001); a mean SNOT-22 score of 42.1 in those patients reporting only one ENP was not significantly different. ANOVA for SNOT-22 scores regardless of surgery showed only a significant difference between CRSwNPs and AFRS subgroups (p=0.043). A more detailed analysis of factors influencing disease in CRS will be reported elsewhere.
Discussion
The data from the CRES depict a story of the burden of CRS on the NHS with more than half the cases of CRSwNPs and AFRS reporting previous surgical intervention and nearly half of those with surgical intervention having had more than one procedure. As these patients were all at varying points in their journey as sufferers of CRS with some having undergone prior intervention in secondary care and others having previously received only treatment in primary care (having been recruited at their first appointment in secondary care), we believe the study population includes a wide range of CRS sufferers, rather than a specific surgical cohort, and the SNOT-22 scores reflect a range of severity (0–108) with overall recruitment across all sites being 66% of those approached for participation.
Limitations of this study data are that they are self-reported and patients may not accurately recollect the details of the procedures. There are no data on non-responders, given the anonymous nature of the study. Although there were large numbers of non-surgical cases reported, there is a potential bias towards those who had received surgical intervention, given the secondary care setting of the study and that GPs will often refer patients when they believe medical treatment has been exhausted. The study did however aim to recruit all patients seen with CRS, including those only receiving medical intervention in the outpatient setting. There is a selection bias in terms of location as only patients undergoing treatment in ENT departments were recruited—there may be many patients who have had successful previous surgery who will be missed as they are no longer requiring active care or are only receiving treatment in primary care; capturing this wider picture of patient journeys across primary and secondary care may become more of a reality now, with the advent of health informatics such as the Clinical Practice Research Datalink (CPRD).17 The study was designed to review patients with CRS at one given point of time for each participant, and since reported duration of disease for each participant varied considerably, it is difficult to accurately establish the size of the population at all time frames. Strengths of the study include the spread of data from across the UK, representing both smaller district general hospitals and larger tertiary centres as well as different urban and rural populations.
Comparison with the UK Audit data
The UK Sinonasal Audit found that 46.1% of patients had undergone sinonasal surgery before participating in the study, with 52.5% of those with CRSwNPs reporting previous surgery, compared with 35.0% of CRSsNPs. In comparison, CRES has found slightly lower rates of patients with CRS overall reporting previous surgery, 43% of all patients with CRS, but 57% of CRSwNPs and 29% of CRSsNPs. This may reflect the point of recruitment being different; Audit patients were recruited at the time of surgery, while CRES patients were recruited at the time of outpatient treatment, recruiting just those eligible for surgery in the Audit is likely to recruit more severely affected patients than a cohort being treated in outpatients; however, the mean SNOT-22 scores were very similar with a mean preoperative score of 42 in the Audit and a mean of 43.9 in CRES. The median time to previous operation in the UK Audit and in CRES was 6 years.
Our study found the highest rate of revision surgery to be among those with CRSwNPs and AFRS, with rates of previous surgery almost twice that of those without nasal polyps which is supported by the UK Sinonasal Audit. There is a growing acceptance that patients with and without polyps have distinct differences. This is reflected in the current iteration of EPOS, with different treatment algorithms for the two main phenotypes. The role of surgery in patients with CRSwNPs is likely to be no more than achieving topical access to intranasal therapies, and it may not change the underlying pathophysiological process. The need for recurrent treatment is therefore not unexpected. A recent study18 found that ostiomeatal obstruction is not a feature of CRSwNPs, and surgery, which primarily alleviates obstruction, is unlikely to be curative. In contrast, ostiomeatal obstruction is much more common in CRSsNPs, and therefore ESS which addresses this may well achieve long-term benefits. This contrasts to one previous study19 which found no difference in recurrence rates between those with and without polyps. It is not clear at this time whether the high revision rates seen in CRSwNPs simply reflect the chronic nature of the condition and the limitations of current medical management, or whether there are operative variables that may be improved in order to reduce the ongoing burden of revision surgery. CRSwNPs patients are likely to reflect a diverse group, with differing individual patient factors (endotypes) that are yet to be fully understood and characterised. The presence of asthma appears to represent a higher risk factor for recurrence.20 Similarly, a previous study has also shown higher rates for repeat surgery among those with aspirin-exacerbated respiratory disease21 (risk-OR of 2.7). One additional patient factor which may influence rates and times to revision surgery is smoking status, Wu et al showed that smokers had a shorter time to revision surgery,22 but with only 11 smokers in those with multiple ENPs in CRES, this trend was difficult to quantify.
A crucial factor in the success or failure of surgical intervention will be patient compliance with ongoing medical management postoperatively. Although information on medical treatment was recorded, this cannot be specifically aligned with the postoperative period in these patients and is not considered further in this analysis. Anecdotal evidence from the qualitative arm of the CRES suggests that compliance with topical treatments is a problem and that patient education at the outset of treatment is crucial with a need for regular reinforcement.23 This may currently be counteracted by differing advice from primary and secondary care practitioners and emphasises the need for greater awareness of guidelines, but there is also a need for further clinical trials in terms of medical treatment to underpin this.
We acknowledge that recurrence of disease reflecting its chronic nature is a more common occurrence than revision due to ‘failed’ surgery in its truest sense. While we accept the term ‘revision’ suggests failure of the primary surgery and that recent evidence shows early postoperative benefits from sinus surgery,24 for the reasons cited above (extent of surgery and grade of surgeon) we feel consideration needs to be given to the longer term perspective on surgical management in CRS. As such there is a need for trials that address these factors, so that we can better understand whether these repeated surgical interventions reflect a disease-specific burden or are a product of current surgical strategies.
Cost burden
Within the NHS, consideration of the cost of repeated surgeries is very important. Based on annual HES data for 2012/2013 on admissions for sinus surgery for CRSwNPs,25 and considering NHS reference costs of approximately £1500 per case for each surgical admission,4 the total cost to the NHS is likely to be over £30 million per year. Although the exact proportion of revision surgeries across the NHS is not precisely known, if 50% of surgical cases are revision cases, then £15 million is spent each year on revision sinus surgery or polypectomies. As well as the financial burden to the NHS, there is a risk we may be subjecting patients to surgery and its attendant complications without good evidence of effectiveness from level 1 evidence. However, the benefit in terms of reduced healthcare costs as seen in an American model suggests that surgery may prove more cost-effective than continued medical therapy alone. This recent study showed that patients with CRS have healthcare utilisation levels at the time of surgery that are eight times greater than baseline, but also reach baseline levels within 13 weeks postoperatively.26 However, given the costs of surgery, good evidence on the cost-effectiveness of repeated interventions is needed and must be weighed up against both the direct and indirect costs of the condition.
Conclusions
Data from the CRES show that 13 years after the Sinonasal Audit, there is still a high burden of revision surgery in CRS to both patients and healthcare providers. It is therefore essential, now more than ever, that carefully designed clinical trials are undertaken that build on the existing evidence to support surgery in CRS and assess the effectiveness of surgery before making such decisions. A possible trial design might consider comparing early surgical intervention alongside continued medical therapy versus delayed surgical intervention on continued medical therapy to show benefit from surgery per se and also to investigate whether or not surgery is cost-effective. Further trials are then needed to examine the benefits of extended sinus surgery over minimal surgical intervention (eg, ENP). This study emphasises the need for ongoing research to improve the care of patients with CRS in order to minimise the need for repeated specialist care and operative intervention.
Acknowledgments
Thanks to the research nurses who aided recruitment, especially Jane Woods who also made a significant contribution to checking the data after the study ended. Thanks to Veronica Bion at UEA for processing all the questionnaires through the scanner. Thanks also to Professor Anne Schilder and the ENT Specialty Group for support in getting the study elevated to the NIHR portfolio and with recruitment.
References
Footnotes
Contributors CP was the chief investigator and devised the study. He recruited patients at various sites in East Anglia. He wrote the first draft of the paper. AC was responsible for data analysis and was involved in the study design. SM was responsible for providing a health economic perspective to the revised version of the paper. SE, CP, AC and CH were responsible for undertaking the second revision of the paper. Remaining authors were responsible as local principal investigators for recruitment and have all contributed to the final content of the paper: NK, AR, AF, SAh, SAn, RC, HK, PJ, SC, NK, PP, RA, NM, SS, MS, JR, JP, JH.
Funding The study was funded by the Anthony Long Trust and Bernice Bibby Trust.
Competing interests None declared.
Ethics approval Oxford C Research Ethics Committee.
Provenance and peer review Not commissioned; externally peer reviewed.
Data sharing statement Additional data can be accessed via the Dryad data repository at http://datadryad.org/ with the doi:10.5061/dryad.kt32c.