Article Text

Abstract
Objectives To investigate the presence, nature and relationship to age, sex, ethnicity and body mass index (BMI) of adverse reactions following routine cycloplegic eye drops in children.
Design Prospective observational cohort study.
Setting Ophthalmology outpatient clinic Dutch metropolitan hospital; February, March and April 2009.
Participants Children aged 3–14-year-old children receiving two drops of cyclopentolate 1% (C+C) or one drop of cyclopentolate 1% and one drop of tropicamide 1% (C+T). Patients were categorised by age (3–6, 7–10 and 11–14 years), sex, ethnicity and body mass index (BMI) (low, normal or high).
Outcome measures Rate and nature of adverse reactions reported at 45 min following treatment. Crude and adjusted ORs for reporting an adverse reaction using stepwise regression analysis with BMI, age, ethnicity and sex.
Results 912 of 915 eligible patients participated (99.7%). Adverse reactions were reported for C+C in 10.3% and in C+T in 4.8% (42/408 and 24/504, p=0.002), respectively. Central effects were present in 95% in C+C and in 92% in C+T. Compared to C+T, an increased risk was present in C+C (crude OR 2.3 (1.4 to 3.9), p=0.002). Forward adjustment showed BMI to be an influencing factor in treatment (OR 3.1 (1.7 to 5.6), p<0.001). In a multivariate model, a dose of cyclopentolate remained associated with adverse reactions. Analysis per BMI and regime and age category and regime, indicated associations with low BMI (OR C+C 21.4 (6.7 to 67.96), p<0.001, respectively, C+T 5.2 (2.1 to 12.8), p<0.001) and young age (OR C+C 8.1 (2.7 to 24.8), p<0.001).
Conclusions Adverse reactions were common and almost exclusively involved the central nervous system. Both presence and severity were associated with repeated instillation of cyclopentolate 1%, low BMI and young age. In specific paediatric populations, a single dose of cyclopentolate must be considered. Vital function monitoring facilities are advisable. Adjustment of guidelines is recommended.
- CLINICAL PHARMACOLOGY
This is an Open Access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/
Statistics from Altmetric.com
Strengths and limitations of this study
This study investigated the presence and nature of adverse reactions in commonly used cycloplegic regimes and determined risk factors.
Evidence for a dose–response mechanism is provided.
Observer bias could not be ruled out completely.
Some subgroups comprised a limited number of participants.
This study warrants a critical approach to the use of cyclopentolate 1% in specific paediatric populations and adjustment of guidelines and product documentation.
Introduction
In children, refractive errors can cause decreased visual acuity and problems in binocularity such as strabismus.
Owing to strong accommodative reflexes and the inability to respond reliably to subjective refraction, objective refraction in children is required to assess their refractive state. Objective refraction can only be obtained with cycloplegia through anticholinergic eye drops. Cyclopentolate 1% and tropicamide 1% are both commonly used anticholinergic eye drops for objective refraction in the paediatric population. Depending on ocular alignment, the (expected) refractive error and iris colour, cyclopentolate will be applied once, twice or three times.1 In subjects with darker irises, a combination with tropicamide is often required.1 The use of anticholinergic eye drops in children is generally considered to be safe.1 ,2 Severe adverse reactions following administration are very rare.2 With regard to tropicamide, the literature agrees that it rarely provokes adverse reactions.1 ,3–5 Adverse reactions following the application of cyclopentolate are more common and could be dose related.6 Young children are most at risk.1 The adverse reactions occur between 15 and 60 min following an administration, often impacting on the central nervous system (CNS), but subsiding within 2–6 h with no permanent sequelae.7–9 Anticholinergic CNS adverse reactions include: psychotic reactions and behavioural disturbances, ataxia, incoherent speech, restlessness, hallucinations, hyperactivity or drowsiness, seizures, disorientations as to time and place and failure to recognise people.1 Peripheral anticholinergic adverse reactions include: urinary retention, diminished gastrointestinal motility, tachycardia, hyperpyrexia, vasodilation, skin rash, decreased secretion in salivary and sweat glands, pharynx, bronchi and nasal passages.1
For reports on the rates and nature of the milder adverse reactions, one can only refer to the rates encountered during surveys or efficacy studies. For rates on adverse reactions, we searched in larger sample sized studies since the rates of small sample sized studies cannot be extrapolated to the general population.10 With regard to tropicamide, several very large surveys report an absence of adverse reactions.3–5 A study of Bagheri et al6 involving 96 6 to 20-year-old participants reports an adverse reaction rate of 5%, 11% and 24% after one dose, a double dose and a triple dose of cyclopentolate 1%. In contrast, a smaller study of Mohan and Sharma11 observed the absence of ocular or systemic side effects in a similar population receiving the same treatment regimes. Although Bagheri et al6 report adverse reaction rates, they do not specify the nature of these adverse reactions. A study of Egashira et al12 involving 20 participants aged 6–12 years reports one participant with drowsiness and two participants with hyperactivity, of whom one also suffered from visual hallucinations, following one dose of cyclopentolate 1%.
In young children, about 5–9% need objective refraction because of failure in vision screening programmes due to either strabismus or decreased visual acuity.13 ,14 With older children and children in puberty, visual acuity symptoms increase up to 14%.15–19 A relatively large part of this group requires objective refraction to assess their refraction. Depending on the healthcare arrangements of individual countries, the objective measurement of refraction is performed in hospitals or healthcare centres, as well as in local optometric practices. The latter usually do not have facilities to monitor vital functions. In our Dutch metropolitan hospital ophthalmology outpatient clinic with an ethnically diverse population, we routinely use either a double dose of cyclopentolate 1% (C+C) or one dose of cyclopentolate 1% followed by one dose of tropicamide 1% (C+T). Adverse reactions following both regimes are seen, but a larger number of adverse reactions were encountered using C+C. Besides an apparent association with regime, our observations also suggested a possible correlation with younger age and/or lower body mass index (BMI). The available literature does not provide sufficient evidence to show the presence and nature of adverse reactions and relating factors. This survey does not address the reason for the choice or effectiveness of the departmental routinely used regimes. However, both regimes are commonly used worldwide.1 The purpose of this study was to gain more insight into the presence and nature of adverse reactions following the administration of C+C and C+T for objective refraction assessment in children. A secondary aim was to investigate whether the frequency of adverse reactions was associated with age and/or BMI.
Methods
This study was designed as a prospective, single-centre, cross-sectional and observational cohort study. The study group investigators were research assistants and four orthoptists. The study population included all patients between 3 and 14 years who required an objective refraction at our ophthalmology department during February, March and April 2009. The study period of 3 months was chosen because of the high return rate of our participants after this 3-month period. The lower limit of 3-years was chosen because of cooperation problems associated with length and weight measurements below this 3-year age limit. Furthermore, possible adverse reactions might not be distinguishable from common sleepiness or behavioural problems due to normal wake/sleep patterns seen in children below this age. The upper limit of 14 years was chosen because there are a limited number of patients requiring an objective refraction beyond this age. Treatment was given in accordance with standard departmental protocol. The orthoptists were not restricted in their choice of medication and used their normal individual regime to assess objective refraction with either C+C or C+T.
Ethical considerations
The study was conducted according to the principles of the Declaration of Helsinki (V.59th WMA General Assembly, Seoul, Republic of Korea, October 2008), the Dutch Agreement on Medical Treatment Act (WBGO) and the Dutch Personal Data Protection Act. The Medical Research Involving Human Subjects Act (WMO) did not apply to this study according to the Dutch Central Committee on Research Involving Human Subjects (CCMO, The Hague), and therefore a written waiver of the CCMO was provided. All parents and children were asked if they would participate in an observational survey where length and weight measurements would be recorded to establish if there was a need to develop new departmental guidelines for the eye examination of children. Information on the aims of the survey, ie investigation of the presence and nature of adverse reactions and related factors, was given. Subsequently, oral consent to participate in this observational survey was asked of both parents and children. The parents and children were free to refuse to participate in the survey. Both oral explanation as well as length and weight measurements were conducted on arrival at our department.
Procedures
The participating individuals were numbered consecutively. Length and weight were determined. BMI was calculated according to the formula: BMI=Weight/height. Participants were divided into three categories: low BMI, normal BMI or high BMI, according to the international cut-off values for underweight and overweight by sex between 2 and 18 years.20 ,21 For South Asian participants, cut-off values according to the guidelines of de Wilde et al22 were used. Participants were allocated to the following ethnic main groups: Dutch, Turkish, Moroccan, Indian subcontinental (including Indian, Pakistani and Surinam-Hindoestani) or West-African (including African of the African Gold Coast, African-Caribbean participants from both the Dutch Antilles and Surinam). The remaining participants were assigned to the category ‘Other’. Participants were also subdivided into three age categories: 3–6, 7–10 or 11–14 years. A case record form with the designated number of each participant was added to the outpatient chart. The examining orthoptist noted either no drops, C+C or C+T on this form. For children receiving eye drops, the examining orthoptist made enquiries approximately 45 min following the first eye drop. The parents and children were asked “Did you notice anything different following the eye drops?” Any responses relating to blurred vision and/or photophobia were excluded. All other responses were noted. Adverse reactions were classified as severe to moderate drowsiness, mild drowsiness or apathy, excitation and hyperactivity and/or behavioural problems, dizziness, red face and/or cheeks and/or nose bleeding. A further classification was recorded as being either a ‘central (CNS)’ or ‘peripheral’ adverse reaction in accordance with the list provided in the first paragraph of the introduction of this manuscript. Parents were instructed to contact us if adverse reactions did not disappear within 4 h.
Bias
To avoid treatment bias, the examining orthoptist was kept unaware of the BMI status of the participants. To avoid response bias from parents and/or children, two procedures were followed. First, the length and weight measurements were introduced as being part of a departmental paediatric population survey and this was carried out to establish if there was a requirement for the development of new departmental guidelines for the eye examination of children. Second, the enquiries about the adverse reactions were made with an open question technique.
Data analysis
Data were analysed in SPSS 22 for Windows. Differences were considered statistically significant if p<0.05; two-sided. A difference of >2% in reported adverse reactions was considered clinically significant. Variables were compared between C+C and C+T using the independent samples t test or the χ2 test, as appropriate. Univariate stratified and multivariate logistic regression analyses were performed to assess the impact of variables on the likelihood that a participant would report an adverse reaction. ORs for treatment were calculated without and with adjustment for BMI, age, ethnicity and sex in a forward model. We computed ORs for BMI and treatment, with normal BMI participants receiving C+C as the reference group, both unadjusted as well as adjusted for age, sex and ethnicity in a multivariate model. We also computed ORs for age and treatment, with 6-10 year old participants receiving C+C as the reference group, also unadjusted and adjusted for BMI, sex and ethnicity in a similar model.
Results
A total of 912 of 915 eligible patients participated (99.7%; figure 1). A total of 408 received C+C and 504 received C+T (figure 1).

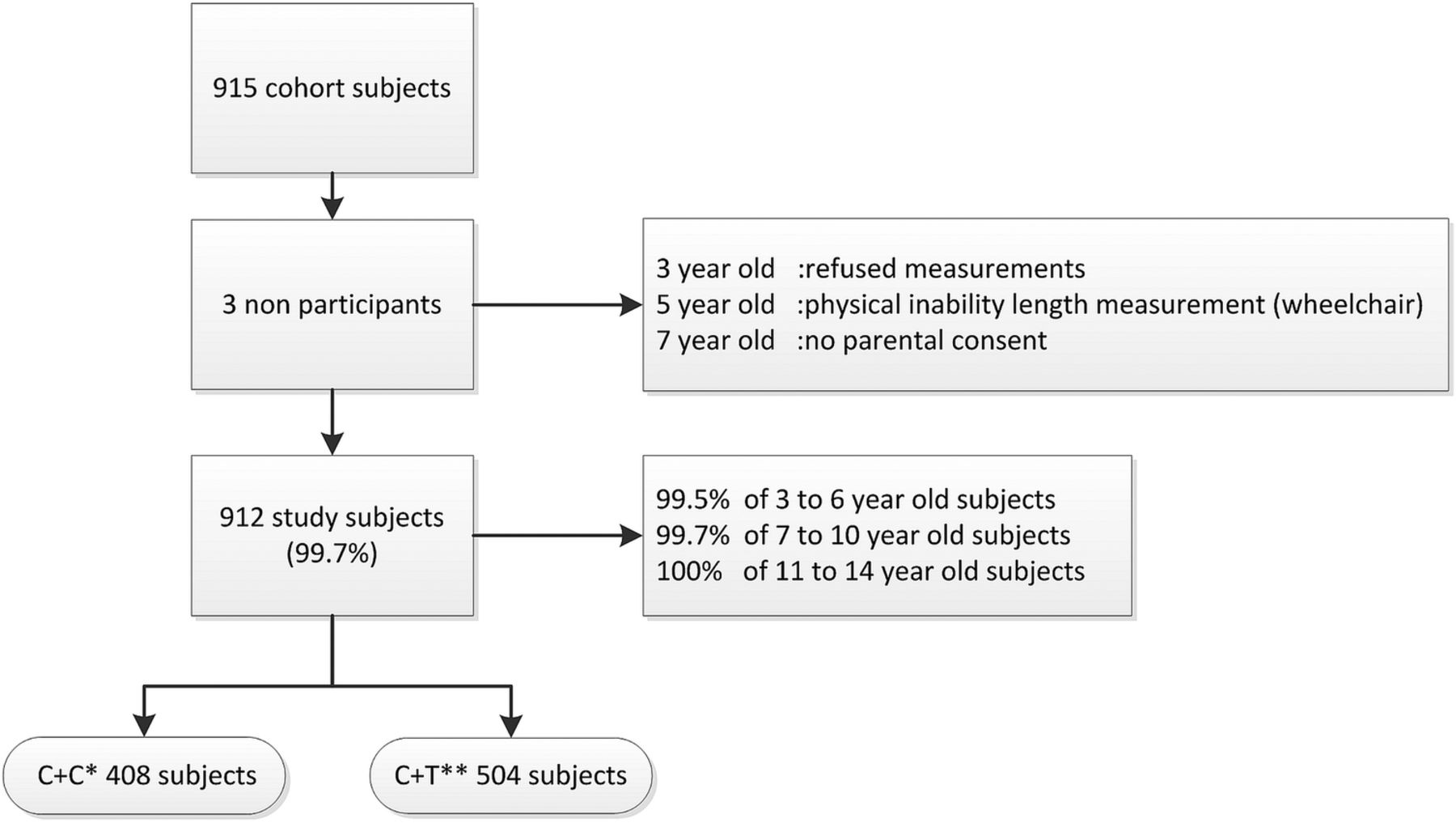{kind=link}
Flow chart diagram showing number of participants in the cohort and number of participants participating in the study. *C+C: Two drops of cyclopentolate 1%. **C+T: One drop of cyclopentolate 1% followed by one drop of tropicamide 1%.
Table 1 reflects the baseline group characteristics stratified by regimes C+C and C+T.
Baseline characteristics of children who underwent objective refraction assessment stratified by cycloplegic eye drop treatment
Adverse reactions: presence and nature
Adverse reactions were reported in 10.3% (42/408) of children following C+C administration and in 4.8% (24/504) of participants following C+T administration (p=0.002). Central effects were present in 95.2% (C+C; 40/42) and 91.7% (C+T; 22/24, table 2). Severe to moderate drowsiness was the most frequently reported adverse reaction (5.4%) following C+C administration. It was most often present in children aged 3–6 years and predominantly present in children with low BMI (table 2). Reports of severe to moderate drowsiness and excitation, hyperactivity and/or behavioural problems were significantly less often present following C+T administration. Excitation, hyperactivity and/or behavioural disorder were the only adverse reactions expressed in high BMI and only reported in the youngest age category following either treatment (table 2). None of the parents contacted us after leaving the outpatient clinic.
Number and calculated percentages of clustered adverse reactions stratified by cycloplegic eye drop treatment and their distribution across age and BMI categories
Relation of adverse reactions with sex, BMI, ethnicity and age
Neither sex nor ethnicity was related to adverse reactions (table 3). In both interventions, low BMI participants had a statistically highly significantly increased risk for adverse reactions; however, the OR for adverse reactions was significantly higher in C+C compared to C+T (table 3). In both treatment groups, the frequency of adverse reactions was highest in the youngest age group. Only in C+C was younger age associated with a statistically highly significantly increased risk for adverse reactions (table 3). A borderline significance, p=0.06 instead of p<0.05, however, was present in C+T. Furthermore, in both interventions for all age categories, adverse reactions were more frequently reported in children with low BMI compared to those with normal BMI (table 3).
Frequencies, percentages and crude ORs of adverse reactions with respect to sex, BMI, ethnicity and age category stratified by cycloplegic eye drop treatment
Relation of adverse reactions with dose of cyclopentolate, BMI and age
For children receiving C+C, there was a significantly increased overall risk for adverse reactions compared to those receiving C+T (OR 2.3 (1.4 to 3.9); table 4). In a forward model, we explored the influence of the variables BMI, age, ethnicity and sex on the OR for treatment. Only BMI was found to have a significant influence (table 4).
OR for reporting adverse reactions for treatment, and stepwise adjustment of this OR with BMI, age, ethnicity and sex
Our analysis indicated that the dosage of cyclopentolate saw the most adverse reactions when administered to young children with low BMI. These relations were explored in more detail. Table 5 shows the unadjusted, crude ORs for reporting adverse reactions per BMI category and regime, with normal BMI participants receiving C+C as the reference group in a multivariate model. Following adjustment for gender, ethnicity and age, the dose of cyclopentolate remained highly significantly associated with adverse reactions. We also explored age category and regime (table 5). Following adjustment for gender, ethnicity and BMI, the dose of cyclopentolate was associated with adverse reactions in the youngest participants.
ORs for reporting adverse reactions per BMI category respectively age category and regime, with normal BMI respectively 7–10-year-old children receiving C+C* as reference group; backwards analysis
Discussion
This study showed that adverse reactions following cycloplegic eye drops are common in children. Adverse reactions were highest following the administration of a double dose of cyclopentolate to young children with a low BMI. Adverse reactions were virtually absent in participants with high BMI. Our data suggest a dose–response mechanism.
Interpretation of findings
One objective of this study was to gain more insight into the nature of the adverse reactions. All adverse reactions reported were expected adverse reactions; they were observed and documented previously. Drowsiness was the most frequently reported adverse reaction. According to the international guidelines of the Council of International Organizations of Medical Sciences, the rate of both severe and mild drowsiness can be classified as ‘commonly present’ (≥1% and <10%).23 For a double dose of cyclopentolate 1%, the severe to moderate drowsiness rate as reported in the youngest age category can even be classified as ‘very commonly’ present (≥10%).23 Furthermore, regardless of the amount of cyclopentolate, severe to moderate drowsiness was very commonly present in low BMI participants of all age categories. Worldwide, only a limited number of companies produce cyclopentolate 1% and tropicamide 1%. In general, manufacturers provide a summary of product characteristics for the individual countries.24–37 The summaries of product characteristics give a wide variety of possible central effects. CNS involvement in children is mentioned as being uncommon24 ,25 or rare;24 meaning present in >0.1% but <1%.23 Drowsiness is mentioned in a few summaries of product characteristics, but without any further reference to the frequency.27 ,28 An increased risk of adverse reactions is identified for infants and young children, but no statements are made about the risks for low weight participants in the documents we studied.
In addition to classification by frequency, adverse reactions can also be classified by severity. The Common Terminology Criteria for Adverse Events grade adverse reactions according to a System Organ Class.38 This system has five levels of grading; where grade 1 represents mild symptoms, grade 2 represents moderate symptoms up to grade 5, representing death related to the adverse reaction. The adverse reactions reported in our survey mainly belong to the ‘nervous system disorders’. Dizziness, hyperactivity and/or behavioural problems, and mild drowsiness or apathy are classified as grade 1 adverse reactions. Severe or moderate drowsiness is classified as a grade 2 adverse reaction. The peripheral adverse reactions reported are all grade 1 adverse reactions. A significant difference between the interventions was present. A double dose of cyclopentolate had 52.4% grade 2 adverse reactions while one dose of cyclopentolate had 33.3% grade 2 adverse reactions.
The present study showed that adverse reactions were present in 4.8% and 10.3% of children receiving one dose versus two doses of cyclopentolate 1%. Both rates and the 2.2-fold difference in rate are in concordance with the report of Bagheri et al.6 Our findings support their statement that the incidence of adverse reactions increases with repeated instillation of cyclopentolate. The reported adverse reactions in our study almost exclusively involved the CNS. This is not in line with a report of Pi et al.39 Although not reporting actual rates, they mention eye irritation and conjunctival hyperaemia as the most common adverse reactions in a large cohort of participants aged 6–15 years receiving three drops of cyclopentolate 1%. In our study, we focused on all unwanted reactions without influencing patients and/or parents beforehand by providing a specified list. This might have given an underestimation of minor unwanted effects. The symptoms reported by Pi et al39 were expected effects immediately following eye drop application. They generally subside quite quickly and might have been forgotten at the time of our enquiry.
Worldwide, tropicamide and cyclopentolate have been used for decades. The lack of adverse reactions following tropicamide is acknowledged and well described. Although an effect of tropicamide on adverse reactions cannot be ruled out, we believe that the adverse reactions can only be attributed to cyclopentolate. The frequent involvement of the CNS following instillation of cyclopentolate is in line with the literature.7–9 Drowsiness was the most frequently reported adverse reaction, followed by excitation and hyperactivity and/or behavioural changes. The 3.4 times more frequently reported severe to moderate drowsiness and the 2.5 time more frequently reported excitation, hyperactivity and/or behavioural problems in a double dose of cyclopentolate compared to a single dose of cyclopentolate are more evidence for the impact of cyclopentolate.
Our study shows that adverse reactions occurred most frequently in young and low BMI participants. In general, one can state that young children have an increased risk of drug-related adverse events. The dose relative to blood volume and body weight is in children larger compared to adults.8 ,40–42 Children have a higher cutaneous blood flow and tissues are less dense; thus, absorption may be more profound and rapid.41 ,42 Children have a limited serum protein binding capacity.41 ,42 The smaller the protein binding capacity, the greater the availability of the drug in the blood plasma. Metabolic systems and organs are immature and clearing is slower, resulting in a prolonged half-life.41 ,42 The dose relative to blood volume and body weight is higher in participants with low BMI compared to participants with normal and high BMI.
Children have a large brain mass in relation to body volume and a higher blood–brain barrier permeability than adults, thereby facilitating CNS adverse reactions.42 ,43 The thalamus plays an important role in regulating states of sleep, wakefulness, attention and alertness. The hippocampus is involved in memory, spatial navigation and inhibition. Hippocampal dysfunction is associated with poor impulse control, hyperactivity, behavioural changes and disorientation.44 It seems likely that these areas play a role in the central effects of cyclopentolate. The high incidence of reported adverse reactions, especially in the youngest children of our study, supports the hypothesis that immaturity of the CNS plays a key role in cyclopentolate's potency for adverse reactions.
In this study, adverse reactions were mostly present in the youngest children. However, in the children in puberty, a considerable amount of adverse reactions were still reported. Although no longer immature, the hormonal changes, rapid restructuring of the brain and the increased physical growth might explain the relatively high susceptibility to cyclopentolate in puberty.39–41
Oral consent was obtained from all children and parents. The procedure of consent was carefully considered. The Dutch Agreement on the Medical Treatment Act justified oral consent since the additional length and weight measurements can be considered to cause an insignificant burden and no risk. Also, the Dutch Central Committee on Research Involving Human Subjects agreed that no written consent was required. Furthermore, a written informed consent procedure would have interfered with the observational character of the study and have biased the results regarding adverse reactions following the standard cycloplegic treatment.
Study limitations
Our observational study has several potential limitations. (1) We realise that an actual dose–response relationship could only be determined with plasma concentrations using intravenous measurements of the dose. However, this is not feasible in an observational design and, more importantly, too invasive for children. If a regime with one dose and three doses of cyclopentolate were added to this observational study, we might have established a dose–response relationship in the more true sense. These regimes, however, are infrequently used by our staff. Despite the limitations, we feel we have found enough evidence to state that there is an indication of ‘a dose–response mechanism’. (2) Despite the apparent lack of adverse reactions with regard to tropicamide in the literature, a tropicamide effect could only have been ruled out if a regime using one drop of tropicamide 1% was admitted in this survey. Again, such a regime is infrequently used. (3) The design of this study did not allow for determination of the exact time of onset of the adverse reaction, but an onset of approximately 15–30 min after leaving the examining room was reported in both regimes. We did not gather information on the duration of the reported adverse reactions. However, all effects were still present on departure of the participant from our department, indicating that the adverse reactions lasted for at least 45–60 min after onset. None of the parents contacted us after leaving the outpatient clinic. This could be considered an indication that all adverse reactions had disappeared after this time period. (4) Although the examiner was unaware of the BMI status of the participants, clinical observations might unconsciously have influenced their enquiries, which might have resulted in an observer bias. However, the open question technique should have eliminated such an effect. (5) Besides age and BMI, there are more variables influencing the amount of active compound that a participant might receive, such as firmly squeezing the eyelids or crying of the participant, thereby reducing the amount of active compound one receives. We did not take these variables into account. (6) Treatment with either a single or double dose of cyclopentolate was not randomised. However, the individual orthoptists in this study had their fixed preference for one of the two regimes, and participants were planned for examination several weeks prior by administration staff who were unaware of the treatment regimes administered. As such, this can be considered as pseudorandomisation.45 (7) Finally, some subgroups comprised a limited number of participants. This could have influenced outcomes, both in rates and subsequent analyses.10 The questioning technique used ensured prevention of provoked adverse reaction reports. Furthermore, the results of the 95% CI limits enable generalisation to the population.
Conclusions and implications for healthcare professionals and policymakers
Although cyclopentolate 1% generally can be considered to be a safe cycloplegic, the high incidence of adverse events following cyclopentolate in young, low BMI children poses the question whether it is acceptable to use cyclopentolate in a setting without facilities to monitor vital functions. This study provides evidence for a dose–response mechanism with the occurrence of adverse reactions. Both the presence and severity of adverse reactions are increased in low BMI, young age and in repeated instillation of cyclopentolate 1%. The results of this survey can be generalised to the population. As a result of this survey, we changed our departmental guidelines for use of cyclopentolate 1%. In young, low BMI participants, the increased risk of drowsiness should be taken into account. In this category of children, assessment should be performed with use of a single dose of cyclopentolate and, if necessary, combined with tropicamide 1%. Adverse reactions, especially severe drowsiness, were far less common following this regime. With increasing age and increasing BMI, a double dose of cyclopentolate can be administered safely. When a double dose of cyclopentolate 1% is necessary in young and/or low BMI participants, ie children up to at least 6 years of age and low BMI participants of all ages, the objective refraction should be performed in a hospital setting, or at least in a location where vital functions can be monitored. We propose to make adjustments in the (inter)national guidelines for objective refraction in children. This advice would be especially applicable for settings without facilities to monitor vital functions. This survey shows once again that cyclopentolate is a potent drug that can cause moderate adverse reactions to the CNS in children. For young children and children with a low BMI, the risk of a seriously adverse reaction is rare; however, the possibility of an occurrence should always be taken into consideration. Finally, we recommend general adjustment of product documentation.
Acknowledgments
The authors thank TFH (Thomas) Vissers for his bibliographical assistance. The authors thank MHL (Marleen) Vermeulen-Jongen, B (Brigitte) Simonsz-Toth and M (Marieke) Kwantes for their enquiries in participating patients and thereby enabling our study. The authors thank the group of research assistants for their excellent work. The authors thank P (Pierre) Raap and A (Alexander) Leijenaar for their technical support in preparing the manuscript. The authors especially thank G (Gordon) Melville for his English editing of the manuscript.
References
Footnotes
Contributors HMvM was involved at every stage from the literature search, planning and design of the study, data abstraction, data analysis, data interpretation and writing. MVJ was involved with the study plan and design and writing. DG was involved with data abstraction, data analysis and especially in data interpretation and writing. NESD was involved with data interpretation and editing the manuscript for important intellectual content. She is the guarantor.
Funding This research received no specific grant from any funding agency in the public, commercial or not-for-profit sectors.
Competing interests None declared.
Provenance and peer review Not commissioned; externally peer reviewed.
Data sharing statement No additional data are available.