Article Text

Abstract
Introduction High-grade glioma (HGG) is a rapidly progressive and debilitating disease. Primary carers experience significant levels of distress which impacts on their experience of caregiving, the quality of care received and the community in terms of the increased reliance on healthcare due to the potential development of complicated grief. This paper describes the protocol for testing the efficacy and feasibility of an intervention for primary carers of patients with HGG in order to improve preparedness to care and reduce carer distress.
Methods Randomised controlled trial. The target population is carers of patients with HGG who are undergoing combined chemoradiotherapy. The intervention consists of 4 components: (1) initial telephone assessment of unmet needs of the carer, (2) tailoring of a personalised resource folder, (3) home visit, (4) ongoing monthly telephone contact and support for 12 months. The control arm will receive usual care.
Primary hypothesis This intervention will improve preparedness for caring and reduce carer psychological distress.
Secondary hypothesis This intervention will reduce carer unmet needs. The longer term aim of the intervention is to reduce patient healthcare resource utilisation and, by doing so, reduce costs. Assessments will be obtained at baseline, 8 weeks post intervention, then 4, 6 and 12 months. Participants will also complete a healthcare utilisation checklist and proxy performance status which will be assessed at baseline and monthly. 240 carers will be recruited. The sample size is 180. Multilevel mixed effects regression models will be applied to test the effect of the intervention.
Ethics Ethics approval has been gained from Curtin University and the participating sites.
Dissemination Results will be reported in international peer-reviewed journals.
Trial registration number Australian and New Zealand Clinical Trials Registration (ACTRN)12612001147875.
- HEALTH ECONOMICS
This is an Open Access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/
Statistics from Altmetric.com
Strengths and limitations of this study
This study uses a randomised controlled trial design to test an intervention for family caregivers of patients with high-grade glioma.
This study is trialling an intervention to address the high levels of distress demonstrated in carers in our pilot work, which was higher than that of the patient.
The cost-effectiveness of this intervention will also be determined.
No attention control.
Heterogeneous usual care received in both groups, although this mirrors usual clinical practice.
Introduction
High-grade glioma (HGG) is a term used to encompass grade III anaplastic astrocytomas, oligodendrogliomas and glioblastoma (grade IV). This is a rapidly terminal, progressive and debilitating group of diseases which deprives patients of function, cognition and personality, making this a highly distressing disease for patients, families and carers.1 Seventeen hundred new cases of malignant brain cancer are diagnosed each year in Australia.2 In a retrospective review of survival in over 10 000 patients with glioblastoma diagnosed over a decade (1998–2008), the median survival was 12.6 months with a 2-year survival rate of 15%.3 With the incorporation of temozolomide chemotherapy into standard care for HGG, the current median survival is expected to be in the region of 15 months4 and second-line treatment may have extended this further.5
The carers’ experience
Caring for someone with a brain tumour is unique because of the cognitive, personality and functional changes that occur. In addition to the general cancer-related caregiving issues, the impact of the disease on the patients’ ability to function leads to reduced quality of life, increased stress and carer burden.6 The diagnosis of a brain tumour is particularly stressful for carers because the prognosis is dire and life expectancy short. The cognitive changes and, in particular, personality changes associated with HGG lead to changes in family roles and relationships that are not regularly seen with other cancers, and can occur shortly after the initial diagnosis rather than solely at the end of the disease trajectory. Cognitive disability or dysphasia may also render the carer the primary communicator and medical decision maker. Furthermore, the legal inability of patients to drive adds transport to the carer's responsibilities.7 Carers of people with HGG also need to accommodate the neurological changes that characterise the disease, such as paralysis, seizures, vision and hearing loss. It is therefore unsurprising that these carers report increased stress and distress levels7a and decreased quality of life compared with carers of patients with cancers with a good prognosis.8 Carers of patients with primary malignant glioma report inadequate preparation and a lack of individualised support and information.9
A diagnosis of cancer brings changes in roles and care-related tasks. In the setting of HGG, these changes can occur rapidly after the diagnosis compared with other cancers where the change may be more related to a phase of aggressive treatment or the terminal phase. These care-related tasks may also incorporate new caring activities that require some new learning for the carer. Carers of patients with advanced cancer experience substantial loss in their self-identity, give up significant parts of their lives including work, and may move house to care.10 They are also often unable to take time out for self-care or to accept help in caring. Carers of people who die soon after diagnosis experience greater levels of depression than those caring for people with a long illness trajectory, and in some cases, these levels of depression are clinically significant and directly related to the patients symptomatology.11
Healthcare costs of HGG
Not only is HGG distressing for patients and carers, it also carries a high social and financial burden. In an Australian economic review of the cost of cancer published in 2007, ‘brain cancer’ was one of the most expensive cancers with the estimated lifetime cost of brain cancer per person being estimated at $1.9 million. In a country with universal healthcare, the federal government and society cover around half this cost.12 Interventions which may reduce costs to the healthcare system, patients diagnosed with HGG and their carers are clearly needed. The current healthcare system has substantive gaps in strategies which support carers uniformly and over time, in context of the illness of the person they are caring for, matched to their needs, and when they are providing care in their home. In times of crisis, carers are often left with emergency department visits as their only avenue of support, which are unable to meet these needs. It is a common occurrence that the patients’ length of stay in hospital is prolonged when their carers are experiencing carer fatigue and stress.
Interventions for carers
There is currently a directive from the WHO and recent guidelines on the psychosocial support of carers that adequate psychological support should be provided to carers of patients receiving palliative care.13 ,14 Appropriate education and support interventions need to be trialled and implemented into practice to assist in meeting the needs of carers and reducing their psychological distress.
Psychosocial interventions for carers in a range of situations have been developed with various aims including improving carer understanding and ability to care, self-efficacy, quality of life, stress reduction, and communication and relationships in the family.15 Previous interventions include information provision and education, relaxation, counselling and support, and self-care.15–18 Hudson and colleagues have shown that psychoeducational support increases carers’ preparedness to care, carer competence, sense of reward and sense of having their needs met.19
Support for psychoeducational interventions specifically for HGG carers has emerged from the Netherlands in a recent small randomised controlled trial (RCT; n=56 patient-carer dyads).20 Carers in the intervention group attended six sessions with a psychologist who provided psychoeducation on disease-specific symptoms, strategies for problem solving and cognitive behavioural therapy to increase coping with the caring role. Compared with standard care, the intervention helped carers maintain stable mental functioning and improved their sense of mastery.20 Further large-scale research needs to be conducted to determine the effect of supporting carers from the time of diagnosis of HGG until bereavement.
Hudson and Aranda21 showed that support programmes for family carers of patients with terminal illness can improve carer preparedness, competence, psychological well-being and reduce unmet needs, but concluded more rigorous studies are needed. A meta-analysis of interventions with carers of patients with cancer concluded that small-to-medium effect sizes were appropriate for measuring psychological outcomes.15 Further research using adequately powered RCTs is needed to establish: when support should be provided, how to assess carer needs, and how to provide effective psychosocial support to carers.15–18
Preliminary data
Thus far several members of this team have carried out two investigations into the experience and needs of patients with HGG and their carers. The first was a qualitative study of the needs of patients with HGG and their carers in which semistructured interviews with 19 patients and 21 carers were carried out.7 ,22 ,23 Carers described the period immediately following diagnosis of HGG as a time of rapid change during which they had to renegotiate roles and relationships and learn to be a carer in a short period of time. They described a steep learning curve where they struggled with caring for partners with major disabilities such as hemiparesis, learning how to manage personal care and medications, dealing with seizures and participating in treatment decision-making.7 ,22
The second investigation, a multicentre (Western Australia (WA) and New South Wales (NSW)) quantitative study, examined the experiences of 113 patient-carer dyads at three time points during the disease trajectory: during chemoradiotherapy, and 3 and 6 months later. Results from the baseline data have been published.7a ,24 Carers reported significantly higher levels of distress than patients at baseline and 3 months and between a 1/4 and 1/3 of carers fell into the highest distress category at each time point. Almost 50% of carers reported high or moderate unmet supportive care needs. Their most important needs pertained to gaining information (eg, side effects, prognosis), coping and addressing psychological concerns, practical needs, coordination of care and adjusting to personality and behavioural issues of the patients.
Intervention development
This intervention was developed using the UK Medical Research Council framework for developing and evaluating complex interventions.25 The content of the intervention was based on preliminary data,7 ,22 identification of key components from other studies and a conceptual model to explain individual responses to caregiving.26 Hudson26 proposed a conceptual model and identified important key variables in identifying and understanding the individual response and experience of carers in the setting of palliative care, namely preparedness to care, sense of control, competence, self-efficacy, anxiety, depression and distress, social support, information, a sense of reward, meaningfulness, positive emotions, optimism, respite and relationship with the patient. Our intervention aims to cover all these areas. The following stakeholders participated in development of the resource: medical oncologists, neurosurgeons, radiation oncologists, palliative care physicians, psychiatrists, psychologists, social workers, occupational therapists, nurses (neuro-oncology cancer nurse coordinator, palliative care nurse coordinator, seizure education nurse, diabetes education nurse, and continence advisor), experienced representatives from Carers WA and the Cooperative Trials Group for Neuro-Oncology (COGNO), as well as consumer representatives.
Feasibility pilot study
The intervention has been piloted with 10 carers in WA. The pilot enabled the trained neuro-oncology research nurse to trial intervention delivery, all components of the intervention and assessments used and receive feedback from carers. Additional content was added to the resource following this piloting. Feedback from participants was overwhelmingly positive regarding the value and structure of the intervention.
Aims
This RCT aims to enable carers of patients with HGG to sustain their caregiving role and minimise their distress. The primary objective is to assess the efficacy of a supportive educational intervention for carers in improving the primary carer preparedness to care and reducing their distress.
Primary hypothesis
Carers who receive the intervention will feel more prepared for caring and experience less psychological distress as the patient's disease progresses.
Secondary hypotheses
Carers who receive the intervention will have fewer unmet needs than those in the usual care group.
Carers who receive the intervention will have a better quality of life than those in the usual care group.
This intervention will reduce patient healthcare resource utilisation and, by doing so, will reduce costs.
Methods
Trial design
A multicentre, non-blinded prospective, phase III RCT. The CONSORT guidelines27 are being followed for recruitment and monitoring of response rates and withdrawals. On completion of consent and baseline survey, the carer is randomised to the intervention or control group. The trial schema is shown in figure 1.

Trail schema (HGG, high-grade glioma).
Settings
Recruitment is occurring at two oncology providers in WA. Additional funding for sites in Victoria and NSW is being sought.
Sample recruitment
A consecutive sample of adult primary carers of patients with HGG is being recruited. Eligibility criteria:
Primary carer of patient with HGG who is currently undergoing active treatment with chemotherapy, radiotherapy or combined chemoradiotherapy and within 2 months of initial diagnosis.
Patient is currently attending the neurosurgical, medical or radiation oncology outpatient departments of a participating site.
Age 18 years and above.
Sufficient understanding of verbal and written English language.
Primary carer has no mental, cognitive or functional disability.
Willing and able to comply with study requirements, timing and nature of required assessments.
No familial, sociological or geographical condition potentially hampering compliance with the study protocol, including alcohol dependence or drug abuse.
No severe intercurrent medical or psychotic illness that in opinion of the investigator would jeopardise the ability to participate in the study intervention or assessments.
Recruitment
Depending on site, screening for eligibility is carried out by the medical oncologists, radiation oncologist, neurosurgeons, or neuro-oncology cancer nurse coordinator, at the start of treatment for HGG. As carers often attend the medical appointments, the clinicians are able to briefly discuss the study with patients and their carers and request their permission to provide their contact details to the research assistant. After potential participants are identified, the research assistant invites the carer and patients to participate and provides information regarding the study. Participants are given time to consider the study before written informed consent and the baseline questionnaires are obtained. The first participant of the study was enrolled in February 2014. At the beginning of September 2015 50 participants had been randomised for the study in WA.
Randomisation
Participants are registered when they complete informed consent and the baseline questionnaire and then subsequently randomised. Intervention delivery is planned to start within 28 days of randomisation. Participants are stratified by the patient's European Cooperative Oncology Group (ECOG) score (0–1 or ≥=2) and participating site to achieve an even distribution to each study arm of cases of differing severity and from the different sites.
Block randomisation to treatment arm within each strata is carried out using a computer-generated randomisation table. Allocation to the treatment arms is carried out by the principal investigator rather than the nurse delivering the intervention. The treatment site is not informed which arm patients are randomised to, but blinding is not practical due to the nature of the intervention.
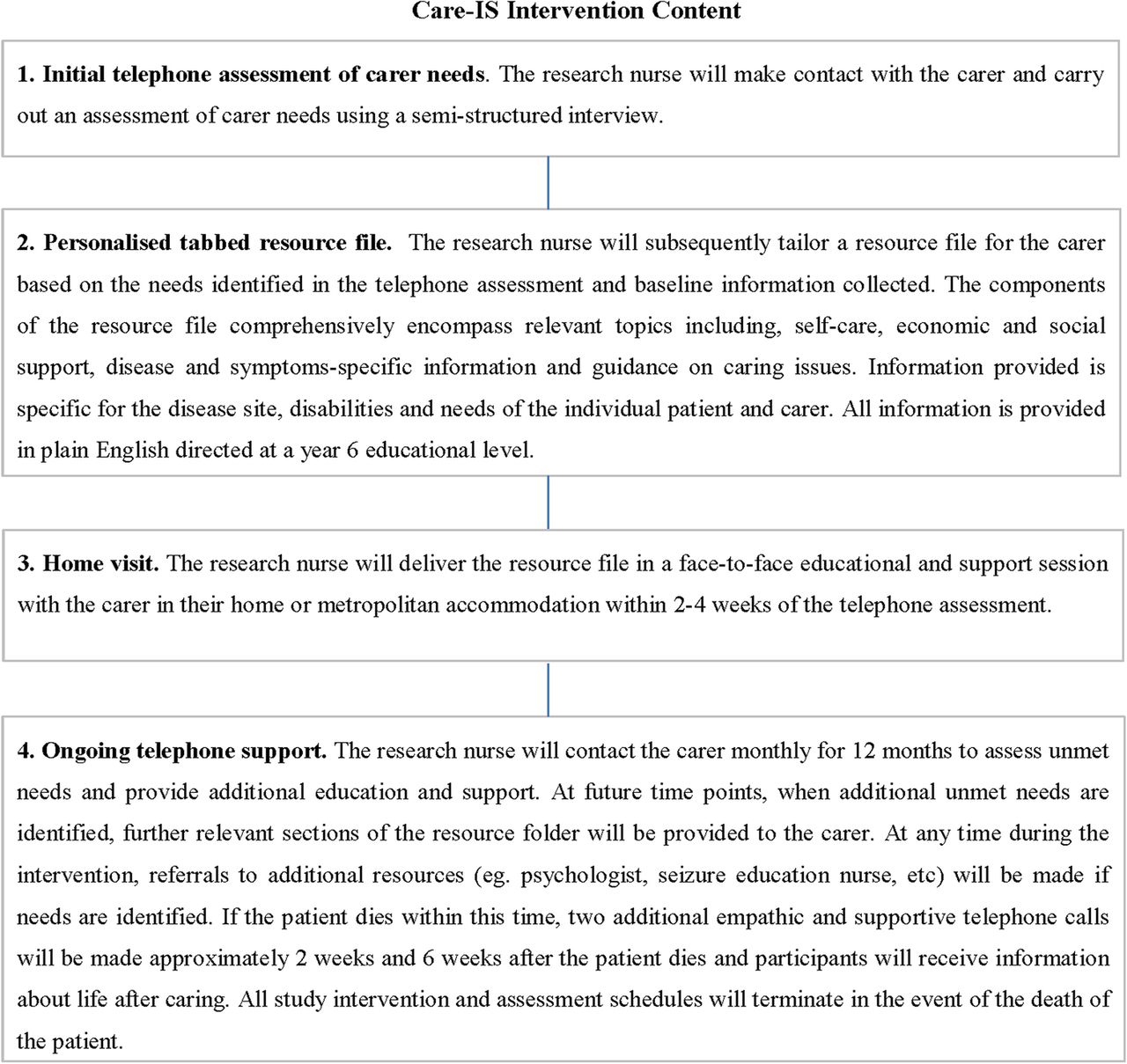
Intervention content
There are four main aspects to this intervention: initial telephone assessment of carer needs; a personalised tabbed resource file; home visit and ongoing telephone support (figure 2). All aspects of the intervention are documented and standardised in an evidence-based study manual which also contains resources for the intervention nurses.

Care-IS intervention content.
Intervention nurse training and quality assurance
In WA, training has been provided by the multidisciplinary team involved in developing the intervention and Carers WA. The WA intervention nurse and a CI experienced in communication skills training will travel to train intervention nurses at other sites. The training will include communication skills training, role plays and familiarisation with each component of the intervention. Intervention nurses at other sites will individualise local resource information in order to integrate with current practice models, but all sites will utilise the same educational information and framework. Each intervention nurse will pilot delivery of the intervention to five carers. Tape recordings of intervention delivery will be assessed for adherence to the protocol for the piloting and a random 5% of carer home visits.
Usual care
The control arm will receive ‘usual care’ which may include currently available educational resources which generally focused on the patient rather than carers, and are not specific to the role of caring for patients with HGG. The patient may also have access to a cancer-specific care coordinator and/or oncology nursing staff. Medical or nursing staff will provide reactive referrals for both groups as per usual practice where needs are identified within the course of routine clinical care, including referrals to a psychologist, seizure education nurse, palliative care and other appropriate available services.
Full standard medical care and supportive management as clinically indicated is allowable on both arms.
Measures
Primary outcome measures are: carer preparedness measured by the Preparedness for Caregiving Scale28 and carer distress measured by the Distress Thermometer (DT).29 ,30 Secondary outcome measures are carer anxiety and depression measured using the Hospital Anxiety and Depression Scale (HADS),31 carer quality of life measured by the Caregiver Quality of Life Index—Cancer,32 carer competence measured by the Carer Competence Scale,33 carer supportive care needs measured by the ‘Partner and Caregivers Supportive Care Needs Scale’34 and ‘Brain Tumour Specific Supportive Carer Needs for Carers Survey’35 and health economic cost-consequences measured using a checklist of services used.
All measures pertain to the carer except the ECOG performance status36 and healthcare utility assessments which involve information about the patient. The patient will also be asked to complete the EuroQoL-5D (EQ-5D)37 at baseline. Figure 3 describes the measures being used and when each assessment is collected.

{kind=link}
{kind=link}
{kind=link}
Measures and reliability.
Data collection time points
The main collection points are baseline and 8 weeks, 4, 6 and 12 months. Data collection is completed by the research assistant for both groups. Patient performance status and health economic measures are collected monthly via phone calls. Participants are prompted by up to three phone calls for each time point. Participants who withdraw are followed up for patient survival and a bereavement call will be made.
Ethical considerations
The current version of the protocol at Sir Charles Gairdner Hospital (SCGH) is V.1.3. All of the Human Research Ethics Committees (HREC) conduct random independent audit, and this study may be audited under these auspices. Protocol modifications will be submitted for ethical approval as an amendment to all committees and disseminated to investigators. This study was registered with the Australian and New Zealand Clinical Trials Registration: ACTRN12612001147875 on 30 October 2012.
The purpose of the study will be clearly explained to participants verbally and in writing. Informed consent will be gained from both the participating carer and the patient. Participation is voluntary and study withdrawal is possible at any time. In order to minimise the risk of distress, it will be made clear to patients that participation (or non-participation) will not influence potential future availability of medical treatment. Carer and patient confidentiality will be protected under standards recognised by Australian Good Clinical Practice (GCP) guidelines and applicable Privacy Acts and Regulations. All data generated in this study will remain confidential. All information will be stored securely at Curtin University and will only be available to people directly involved with the study and who have signed a Confidentiality Agreement.
As this study will require reflection by carers on their care needs and the deterioration of their relative, there is a potential for increased distress of participants. Psychological distress will be assessed at each time point. If a research assistant identifies a carer as having high levels of anxiety or depression (HADS score of >15 for either anxiety or depression) the patient's treating clinician will be notified and referrals will be made for supportive care in the usual, pre-existing referral pathways. Any serious adverse events considered related to the intervention will be reported as required by regulatory authorities.
Study governance
The steering committee for this study includes the following authors: GKBH, AKN, EAL, LM, JLP, TS, RM and PH. The steering committee will be responsible for study design, start, and evaluating and reporting of the results of the trial. The steering committee will meet at least every 6 months throughout the study.
Study sponsorship: monitoring, audit, quality control and quality assurance
The trial is sponsored by Curtin University and the University of WA. The lead author can be contacted at: g.halkett@curtin.edu.au. Trial investigators will permit authorised third parties access to data relating to participants. This will include access for monitoring and Ethics Committee review. The funders and sponsors will not be involved in data analysis or reporting; however, they will be provided with copies of any publications arising from the study.
Sample size and power calculation
Two co-primary end points will be used: carer preparedness and carer distress at 4 months. Using a 5% significance level, two-tailed testing of differences between two independent groups (usual care and intervention), a sample of 64 patients per group (128 total), has 80% power to detect group differences of 0.5 SDs (moderate effect size; considered clinically significant) for carer preparedness.38 This sample size is based on means of 20 and 22.5 (SD=5, range 0–32) for carer preparedness.19 Having previously used the DT with carers,7a we propose that we will be able to reduce the number of carers with high levels of distress from the expected 33% in the control group to 13% (20% difference) in the intervention group at 4 months post baseline. To detect this difference between groups (with 5% significance and two-tailed testing), we will need a sample size of 78 carers per arm (156 in total). Thus, a sample size of 156 at post intervention testing will be sufficient for both primary end points.
We have considered whether there may be site-level differences. Our previous work using the DT showed that at baseline and 3 months, intraclass correlation coefficient values were 0, that is, no evidence of site-level clustering was found. Hence, it is not necessary to account for clustering design effects.
Based on our previous studies where 98% of eligible carers were approached, with a 67% consent rate, we estimate 35% attrition from baseline to 4 months postdiagnosis, implying that 240 carers are needed at baseline (manuscript under review). To achieve 240 carers at baseline, 364 will need to be identified as eligible and 356 to be approached. The final sample size of 240 patients at baseline (with attrition, 156 at 4 months), as calculated using the two primary outcome measures, allows us to test for effect sizes of the same magnitude for the secondary outcomes at 3 months. Assuming a 20% drop-out between the 3-month and 6-month follow-up based on our previous studies, the sample size will be approximately 62 per group. This sample size has power of 80% to detect an effect size of 0.51 for preparedness and a difference of 23% on the DT—effects of similar magnitude to those at 4 months.
Data management and analysis
Data management and storage will occur at Curtin University. Full details about data management for this study can be found in the SCGH ethics protocol. A data management committee is not needed for this study. All data entry will be subject to a 10% check, and analysis will be discussed and guided by the steering committee. No interim analysis is planned. The final trial data set will be available to the steering committee and the full protocol and participant-level data set will be available through the principal investigator.
Intervention effects will be assessed by conducting linear and logistic random effects models incorporating a time by group interaction or latent growth curve modelling to determine whether trends across the three data points within the course of the patients’ treatment differ between the carer groups.39 The models will adjust for confounders and effect modifiers as necessary. Models will be fitted for primary and secondary outcome measures. Model assumptions, such as normality assumptions, will be tested and appropriate methods used to ensure assumptions are met. Missing data for specific time points and from loss to follow-up will be dealt with through multivariate multiple imputation or full information maximum likelihood methods as appropriate.
Cost-consequence analysis
The following costs will be calculated:
Carer-related costs related to brain tumour-specific supportive care needs—will be costed based on information from both data collected in our pilot study and costs recorded using the checklist of services completed by carers in the intervention and control groups.
Patient healthcare utilisation costs—healthcare system costs will be calculated for patient admissions and length of stay in hospital using the Diagnostic Related Groups (DRG) and the relevant national efficient price by allocating the DRG that matches closest to the patient admission information. Cost of emergency department presentations will be based on allocation of the closest Urgency Related Group. Hospice and residential care costs will be derived from Australian Institute of Health and Welfare data.
The costs and outcomes of delivering the intervention will be compared using cost-outcomes (cost-consequence) analysis, a variant of cost-effectiveness analysis in which components of incremental costs and outcomes are computed and listed without any attempt to aggregate these results into a formal ratio. Cost-outcomes analysis provides a more comprehensive presentation of information than other types of economic evaluation and is appropriate for complex interventions that generate outcomes that cannot meaningfully be expressed using a single metric such as those in this study.40 The consequences (outcomes measures as described above) and net costs (cost of the intervention—any cost savings produced by the intervention) will be tabulated to allow an analysis of the cost per net change in the outcome individually and aggregated by type for the outcomes detailed below:
Carer-related outcomes: (1) increase preparedness for caring; (2) reduction in carer distress; (3) increase in carer quality of life; (4) reduction in carers’ brain tumour-specific supportive care needs; (5) increase in carer competence.
Patient healthcare utilisation outcomes: (1) reduction in patient admissions and length of stay in hospital; (2) reduction in hospice and residential care requests; and (3) reduction in the number of presentations to emergency departments and unplanned admissions from outpatient clinics.
Publications
A writing group will be formed by the steering committee and all authors will meet ICMJE criteria for authorship. Professional writers will not be used for publications arising from this study. Results will be disseminated in the peer-reviewed literature and by presentation at national and international scientific meetings. Results will be communicated to the consumer advisory group and through study funders and collaborators including Cancer Council WA, Carers WA, and the WA Cancer and Palliative Care Network.
Discussion
HGG is a rapidly progressive, terminal disease which also deprives patients of function, cognition and personality. These unique characteristics mean HGG is a highly distressing disease for carers, and an expensive disease for the wider community. Patients are frequently admitted to hospital or alternative care due to carer fatigue or lack of preparation for care at home. Australian data confirm both the psychological and financial costs of HGG.12
This study will provide evidence on whether using a preparedness for caring intervention reduces carer distress, improves carer outcomes and reduces patient healthcare resource utilisation and overall costs. If this research study has positive outcomes and is cost-effective, this intervention could be feasibly implemented in routine clinical practice. This randomised phase III trial is designed to provide evidence for changes in practice and policy in Australia and elsewhere. If we can demonstrate positive carer outcomes and cost-neutrality or even cost-savings, we would be in an ideal position to advocate for routine provision of similar services. Furthermore, if successful, the intervention model may be relevant to test in carers of patients with other rapidly progressing cancers or neurodegenerative diseases.
Conclusion
This is the first study internationally to systematically test a nurse-led home intervention to address carers levels of distress and lack of preparedness to care for their relative following a diagnosis of HGG. The proposed intervention package consists of an initial phone assessment, nurse-led home visit, tailored resource manual and ongoing telephone contact. We anticipate that this intervention will reduce carer distress and improve their level of preparedness to care for the patient with HGG.
References
Footnotes
Contributors GKBH, AKN, EAL and LM were involved in initial study conception, trial design, intervention development, protocol and manuscript preparation and ethics application. JLP, MA and PH provided input into trial design, protocol and manuscript preparation. TS was involved in trial design, statistics advice, protocol and manuscript preparation. RM was involved in trial design, health economic evaluation, protocol and manuscript preparation. AL was involved in intervention development and protocol development. AK was involved in intervention development, nursing perspective and manuscript preparation. SF was involved in intervention development, consumer perspective, manuscript preparation. JC was involved in intervention development, nursing perspective, protocol preparation, ethics application, intervention nurse involved in piloting intervention and current trial.
Funding This project has been funded by a Cancer Council of WA research grant and the WA Cancer and Palliative Care Network, Department of Health Western Australia. Additional funding is being sought to fund the national study.
Competing interests None declared.
Ethics approval Curtin University of Technology (HR173/2013), Sir Charles Gairdner Hospital (2013-172), St John of God Hospital (Subiaco and Murdoch; 671), Western Australia.
Provenance and peer review Not commissioned; peer reviewed for ethical and funding approval prior to submission.