Article Text

Abstract
Objective To examine the content and quality of written information provided by surgical centres for patients undergoing oesophagectomy for cancer.
Design Cross-sectional study of the content of National Health Service (NHS) patient information leaflets (PILs) about oesophageal cancer surgery, using a modified framework approach.
Data sources Written information leaflets from 41 of 43 cancer centres undertaking surgery for oesophageal cancer in England and Wales (response rate 95.3%).
Eligibility criteria All English language versions of PILs about oesophagectomy.
Results 32 different PILs were identified, of which 2 were generic tools (Macmillan ‘understanding cancer of the gullet’ and EIDO ‘oesophagectomy’). Although most PILs focused on describing in-hospital adverse events, information varied widely and was often misleading. Just 1 leaflet described survival benefits of surgery and 2 mentioned the possibility of disease recurrence.
Conclusions Written information provided for patients by NHS cancer centres undertaking oesophagectomy is inconsistent and incomplete. It is recommended that surgeons work together with patients to agree on standards of information provision of relevance to all stakeholders’ needs.
- QUALITATIVE RESEARCH
- SURGERY
This is an Open Access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/
Statistics from Altmetric.com
Strengths and limitations of this study
Excellent response rate.
In-depth analysis of written information for patients prior to major cancer surgery.
Makes a strong case to address this issue with future work (eg, development of nationally agreed patient information leaflets (PILs) informed by ‘core information sets’).
Verbal communication of information was not assessed, and it is therefore possible that ‘missing’ written information was discussed during clinical consultations.
Provision of written patient information does not guarantee if it has been read or understood; assessment of the comprehensibility of PILs was beyond the scope of this study.
Introduction
High-quality patient-centred information and communication is considered an essential part of clinical care.1 ,2 It is desired by patients and the public and is associated with increased patient and professional satisfaction, better adjustment to illness and improved quality of life.3–6 In cancer studies, population data demonstrate a common desire for comprehensive information on a range of topics including complex multidimensional treatment outcomes with opposing benefits and harms.7 Despite this, there is evidence that information provision may be insufficient or inappropriate.8 ,9 Clinicians sometimes underestimate patients’ needs and provide minimal information or overestimate the amount of information required, both of which may lead to confusion.10 ,11 Without appropriate information, it is difficult for patients to contribute to the process of shared decision-making (SDM) or make an ethico-legal authorisation for treatment through the process of informed consent.
The provision of high-quality information is particularly relevant in the care of patients with localised oesophageal cancer, the treatment of which is complex and associated with major morbidity and mortality. Even when treatment may be aimed at cure, long-term survival is only achieved in approximately one-quarter of patients.12 There are significant in-hospital mortality and morbidity risks, and deterioration in health-related quality of life (HRQL) is potentially irreversible.13 One useful adjunct in provision of information by clinicians is written information, which may act as an aide-mémoire, helping patients identify their individual information needs and making personalised shared decisions.14 Written information may be provided in a variety of formats. The evidence-based, validated decision aid is considered the highest standard of adjunct, but these are rarely available in surgical settings (which require comparative evidence from randomised studies), and no such material has been developed for oesophageal cancer treatments. Surgical teams in the UK and elsewhere in the world therefore rely on locally produced written patient information leaflets (PILs). In other disease areas, PILs have been shown to be of variable quality, contain complex language and are often poorly presented.15 Whether PILs are also comprehensive—that is, provide information that is both accurate and relevant to the patient population for whom they are designed—is uncertain. The aim of this study, therefore, is to systematically examine the content, completeness and quality of PILs for major cancer surgery, using oesophageal cancer as a case study.
Methods
National Health Service (NHS) hospital trusts in the UK performing oesophageal cancer surgery were identified from the National Oesophago-gastric Cancer Audit Report.12 This report includes all hospitals (n=43) performing this surgery in England and Wales. All 43 hospital websites were systematically searched for PILs, and clinical nurse specialists contacted (by telephone and/or email) to request electronic documents or paper copies by post. Up to three reminders were sent by telephone and email to optimise response rates. Included were English language versions of PILs about oesophagectomy (ie, describing operative techniques, complications and outcomes of surgery) as these are the source documents for subsequent translations. Excluded were leaflets solely describing background information about oesophageal cancer or non-surgical treatments (eg, chemotherapy, radiotherapy or endoscopic stenting). Each included leaflet was assigned a unique identifier (eg, PIL1, 2) to anonymise the information.
Data extraction and analysis
Content analysis
Analysis of the content of PILs was undertaken using modified framework methodology.16 This is a deductive approach used to analyse content by assigning themes and subthemes (ie, descriptive labels) which are outlined a priori and collectively comprise a framework. The framework was developed using information from systematic reviews summarising clinical and patient-reported outcomes following oesophageal cancer surgery17–19 and preoperative consent consultations between surgeons and patients. Two researchers (NSB and SS) independently read and re-read all PILs and mapped data into the themes and subthemes. Where new content was identified, that could not be labelled with an existing theme or subtheme, a new theme or subtheme was incorporated into the framework. The revised framework was then reapplied to PILs that had already been analysed. Following agreement of the final framework by the study team, resulting themes and subthemes were tabulated and descriptive statistics used to summarise the data (table 1). Relative ‘completeness’ was assessed by examining whether each PIL provided any information for every theme and subtheme included in the framework, regardless of its perceived quality or accuracy. Where themes included information about adverse events, reporting of risks (whether described numerically or narratively) and their implications was assessed. Evidence of variations in information was reported descriptively by presenting verbatim examples from the PILs.
Framework including all themes and subthemes
Quality assessment
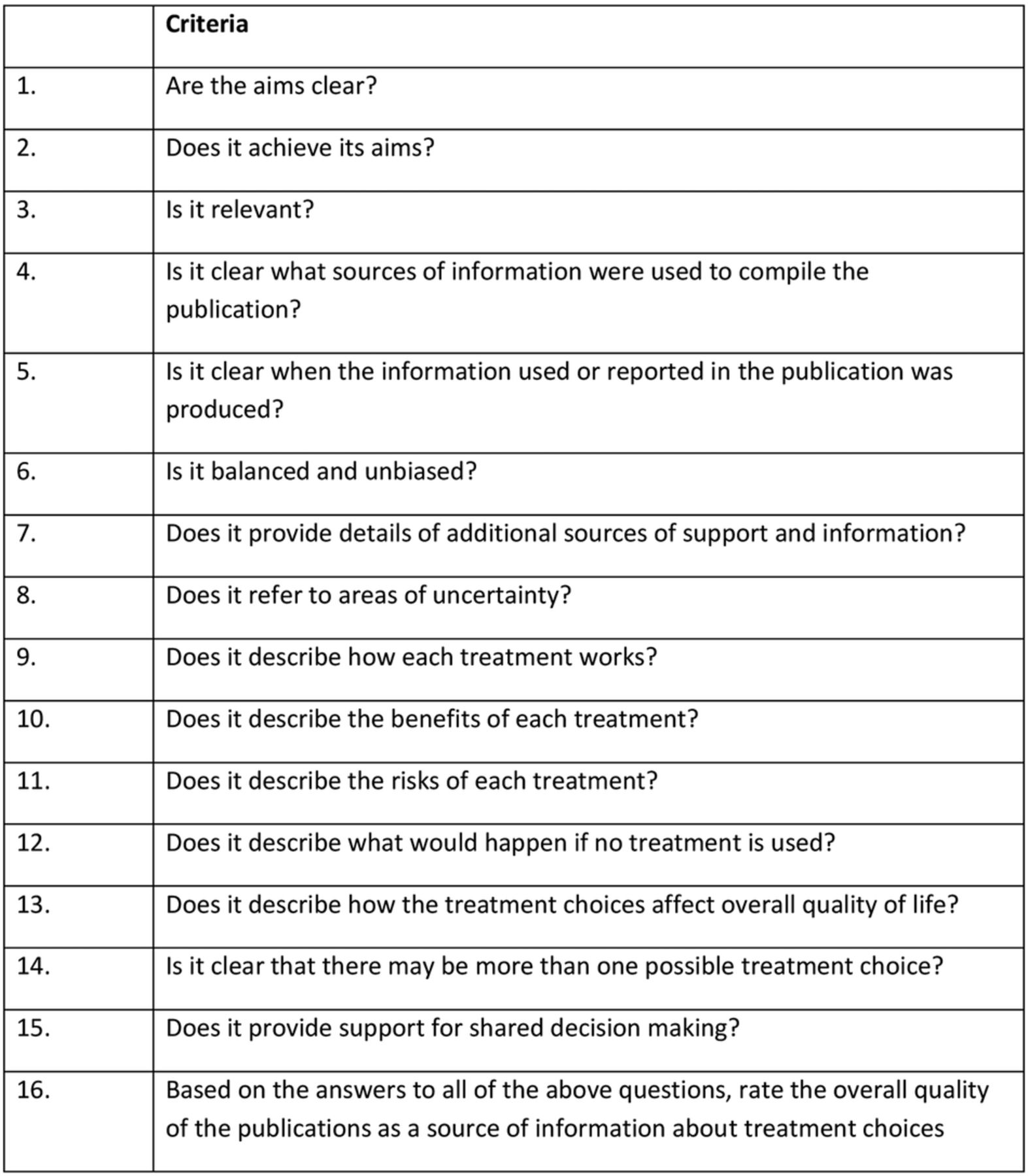
Quality criteria were independently assessed by two researchers (NH and JE) using the DISCERN tool.20 DISCERN requires responses to 16 questions using a five-point Likert scale ranging from one (low quality with serious or extensive shortcomings) to five (high quality with minimal shortcomings; figure 1), and evaluates the reliability of the materials and quality of the information on treatment choices. Scores for each PIL were used to calculate a mean rating for each question, and each assessor's scores were presented separately. Because an overall quality rating of the publication is included within the DISCERN tool, it was not considered necessary to combine scores from each question to produce a global score. Inter-rater reliability was not assessed as previous studies have found strong indexes of agreement between assessors when using this instrument.21 ,22

DISCERN criteria.
Results
Among 43 hospitals performing oesophagectomy, 41 (95.3%) provided leaflets. Ten centres used a generic written information leaflet (Macmillan ‘understanding cancer of the gullet’ (n=6) and EIDO ‘oesophagectomy’ (n=4)) either alone or in combination with a centre-specific PIL. Thirty PILs were designed by individual centres, providing a total of 32 leaflets for analysis.
Content analysis
Six information themes were established: (1) the benefits of surgery, (2) preparing for surgery, (3) operative and perioperative details, (4) in-hospital complications, (5) life after surgery and (6) long-term outcomes (table 1). Each PIL contained information about all six themes, although the amount and completeness of the information varied. Examples of information are provided in the form of quotes to illustrate key points.
Benefits of surgery
Twenty-five leaflets (78.1%) described the potential benefits of undergoing surgery, including curing the cancer and improving patients’ symptoms and quality of life:…surgery is performed in an attempt to produce good quality of life, to restore the ability to swallow, and hopefully a cure. [PIL 5]
None of the PILs discussed the length of time that might be required for quality of life to return to preoperative levels. Fourteen (43.8%) of the leaflets stated that surgery offers the only or best known cure for oesophageal cancer:Surgery is currently the only known way of curing this cancer. [PIL 3]
For growths in the oesophagus this is the most effective treatment as it removes the tumour. [PIL 21]
Other PILs presented different information, describing that other treatment options might be as effective as surgery:The benefits of the operation are dependent upon the extent and type of your cancer. For some types of oesophageal cancer, surgery alone or combined with chemotherapy offers the best hope of long term cure, but for other types similar long term cures are obtained with chemotherapy and radiotherapy. [PIL 20]
Only one of the PILs (3.1%) documented the chances of cure following oesophagectomy (see Long-term outcomes section).
Preparing for surgery
Many of the PILs described ways in which patients could prepare for surgery, such as smoking cessation (n=17, 53.1%), optimising nutritional intake (n=14, 43.8%) and exercise (n=12, 37.5%) before surgery:…you should aim to do some exercise every day. Doing some exercise daily or at least five days a week will help you get fitter and will also help you to get up and about quicker after the operation. [PIL 31]
Nine PILs (28.1%) explained the potential benefits of preparing for surgery:Stopping smoking even just a few weeks before your operation will make a big difference to your ability to recover from the surgery and reduce your risk of complications. [PIL 29]
Operative and perioperative details
Most PILs (n=30, 93.8%) described some technical aspects of the operation, although the amount and type of detail varied:This operation is called an oesophagectomy. [PIL 11—the only information provided about the operation]
An oesophagectomy involves removing most of the oesophagus including the cancer. The stomach is formed into a tube to replace the oesophagus, and is drawn up into the chest or neck where it is joined to the remainder of the oesophagus. The surrounding lymph glands close to the cancer will also be removed. [PIL 22]
This operation involves removing the lower part of the oesophagus (gullet) and the upper part of the stomach. In order to reach the stomach and the stomach the surgeon usually has to make two incisions (cuts). The first cut is down the middle of the tummy (laparotomy). Sometimes the surgeon will use a keyhole approach, in which case you would have five tiny cuts instead. During the laparotomy the stomach is free up to allow it to be pulled up into the chest. The second cut is around the right side of the chest to the back (thoracotomy). During the thoracotomy the right lung is temporarily deflated and the oesophagus freed up. The surgeon can then remove the tumour and join the remaining stomach to the remaining oesophagus in the chest. Occasionally an incision (cut) may be made in the side of the neck and the new join made higher up. This can be in addition to or instead of the thoracotomy. [PIL 29]
The need for drips and drains (such as central lines and chest drains) was documented in 26 leaflets (81.3%; table 2). Details about the anaesthetic were less frequently mentioned (n=12, 37.5%). All PILs documented the likely initial need for intensive therapy unit management following surgery, and 10 (31.3%) explained that availability of such care was a pre-requisite for proceeding with surgery.
Operative and perioperative details
In-hospital complications
All PILs provided some data about in-hospital complications. Areas most frequently described were respiratory problems and anastomotic leak (table 3). Details of the risks, potential severity or implications of these complications were often presented differently. This is described below, using three of the subthemes (anastomotic leak, inoperability at planned surgery and in-hospital mortality) as examples.
In-hospital complications
Anastomotic leak
Of the 28 leaflets mentioning anastomotic leak, 27 (96.4%) described the meaning of this in lay terms. Descriptions varied between leaflets:Internal wound leak. [PIL 12]
If the joins made during the operation fail to heal. [PIL 9]
A leak where the tube is joined to your stomach and throat. [PIL 16]
A leak where the stomach and gullet are stitched together. [PIL 26]
This may happen if the join between the stomach and oesophagus fails to heal, leaving a hole. [PIL 2]
Seven (25.0%) quantified the risk with rates ranging from 2.8% to 10%. In some PILs, words were used in place of numbers to describe risk and these ranged from ‘rare’ and ‘small risk’ to ‘the most serious problem’. One PIL used words (small risk) and numbers (less than 10% chance) to describe the chances of anastomotic leak after oesophagectomy. An explanation of the possible implications of anastomotic leak was provided in 12 (42.9%) studies. These ranged from conservative treatment to the need for further surgery and a return to the intensive care unit:Usually without the need for further surgery. [PIL 16]
Mostly means delaying your ability to drink or eat until the leak heals by itself. [PIL 17]
If a leak does occur it may be necessary to re-operate to control the leak. This would mean opening the chest up again and going to intensive care afterwards. [PIL 7]
Inoperability at planned surgery
Eleven PILs mentioned the possibility of not proceeding with the operation because of the chance of inoperability at the time of surgery. The risk of inoperability was quantified numerically in one PIL (1 in 20), and in others, words such as ‘sometimes’ and ‘occasionally’ were used. Some PILs provided descriptions of the implications of this outcome, which mainly related to alleviating swallowing difficulties:If this happens, the surgeon may insert a tube (stent) instead, to make eating and swallowing easier for you. [PIL 1]
Although other PILs suggested that alternative treatments may be possible, none mentioned that these would be palliative rather than curative in intent.
In-hospital mortality
The possibility of dying in hospital after oesophagectomy was mentioned in 17 (53.1%) PILs. Some described this outcome without any explanation of the risk:Sometimes there can be a major complication that can lead to a prolonged stay in hospital or even death. [PIL 5]
Other PILs explained the chance of in-hospital death using numerical estimates (ranging between 1% and 10%) with two providing proportions as well as percentages. Words such as ‘small risk’, ‘small chance’ or ‘some risk’ were used to describe this outcome.
Life after surgery
At least some information about postoperative symptoms or quality of life were covered in all leaflets with details about pain, eating and fatigue most commonly mentioned (table 4). The amount of information provided varied between leaflets:
After this operation you will need to make lifelong changes to your eating and drinking habits. [PIL 25]
There should be no specific restrictions on your diet but when part of the oesophagus and stomach are removed you may find it difficult to eat large meals, so you are advised to eat small meals more often. It is not uncommon for people to suffer with lack of appetite but it is in your best interest if you can encourage yourself to take diet. [PIL 11]
Life after surgery
Fewer PILs discussed changes in physical (n=22, 68.8%), emotional (n=9, 32.1%), role (n=11, 34.3%) and sexual (n=7, 21.9%) function. Eighteen PILs (56.3%) provided information about routine follow-up schedules after hospital discharge.
Long-term outcomes
Few PILs addressed the subject of prognosis after surgery. Two PILs (6.3%) made general comments about the possibility of recurrence:There is always a possibility that the cancer can recur. [PIL 17]
A further PIL indirectly mentioned the issue:You can ask about prognosis at the outpatient appointment. [PIL 28]
In another, ‘recurrence of the problem’ was listed as a complication of surgery, but was not explained further. Only one PIL (3.1%) provided a numerical quantification of survival:Overall about 1 in 4 people will be cured. [PIL 2]
Quality assessment
Mean DISCERN scores for each question ranged from 1.0 to 5.0 (figure 2). The lowest scoring question related to disclosure of the sources of information used to compile the leaflet, as none of the PILs reported this. Reviewer number 2 scored PILs more highly for 10 of the 16 questions but differences were small.

{kind=link}
{kind=link}
Mean DISCERN score for each question.
Discussion
This novel study examined the content, completeness and quality of PILs for major cancer surgery, using oesophageal cancer as a case study. While it demonstrates that most PILs described technical aspects of the operation, the amount of detail provided varied, and more complex issues were less frequently or incompletely discussed. Most PILs did not mention the chances of long-term survival, and information about the potential complications of surgery was conflicting. Some 11 PILs (34.4%) highlighted the possibility of inoperability at planned surgery, although none specified the implications of this serious event, which converts treatment from curative to palliative intent. Nationally agreed standard information sheets with information of importance to surgeons and patients are recommended, to improve current practice. It is acknowledged, however, that designing a definitive information leaflet is likely to be challenging.
Clinical decision-making for patients considering oesophagectomy for cancer may be particularly important. Oesophageal cancer has a dismal prognosis because even after potentially curative treatment, approximately 50% of patients develop recurrent disease within 2 years and this group rarely regain preoperative HRQL levels.23 ,24 HRQL data can be used to inform clinical decision-making, and there is evidence to suggest that patients consider this important.25 Unfortunately, however, most of the information leaflets within this review did not contain details about the effects of surgery on HRQL. Of those mentioning improvements in HRQL as a reason to undergo surgery, none disclosed crucial information about the amount of time this might take and that in the case of recurrence, HRQL may never recover. Instead the PILs focused predominantly on adverse events following surgery, similar to preoperative consultations with clinicians.25 This may be perhaps because surgeons are familiar with disclosing information about serious events such as complications, whereas communicating details about prognosis is perceived to be difficult due to its sensitive and complex nature.26
In addition to providing patients with important and understandable information, PILs may enhance SDM, which consists of patients and clinicians engaging in dialogue, using best available evidence, to determine preferences and plan treatment.27 In the context of cancer surgery, this process may involve discussion of details about the procedure, including risks and benefits, which are then weighed up by the patient and surgeon in order to reach a collaborative decision. Although SDM sounds appealing and its use is supported by international government policies,1 ,2 ,28 it is unlikely that SDM is implemented in routine surgical practice.29 Combined with the issue that patients may struggle to retain all of what is said during consultations,30 information provision prior to surgery remains challenging. For this reason, additional written communication, such as PILs, is likely to be essential. PILs should, therefore, provide accurate information that patients consider important and can understand. This study has identified variation in the type of written information provided to patients and that this is sometimes inconsistent and conflicting. Information about adverse events was particularly confusing. It was often unclear whether the risks related to published literature, national audit data, or an individual centre or surgeon. Moreover, the reported risk of in-hospital death was as high as 10% in some PILs, yet others described the risk as ‘small’ and similarly, the chance of anastomotic leak was given as ‘less than 10%’ and ‘small chance’ within the same leaflet. Although there is evidence to suggest that the addition of graphs, diagrams or numbers to narrative descriptions may improve patients’ understanding, it is imperative that these are not contradictory and this warrants further consideration.31 ,32
Strengths and limitations
This novel study, with excellent response rates, analysed the content and quality of PILs in oesophageal cancer surgery. Whether the findings would be similar in other disease sites is uncertain. PILs from Scotland and Northern Ireland were not included because the Oesophago-gastric National Audit does not encompass data from cancer centres in these countries. Additionally, verbal communication of information was not assessed, and it is therefore possible that ‘missing’ written information was discussed during clinical consultations. Moreover, provision of written patient information does not guarantee if it has been read or understood. It is possible that in striving for completeness of information, readability may be compromised. While the DISCERN score partly addresses this, it requires a subjective judgement from the reviewer. Assessing the readability of PILs has been described in several published studies and found to be poor;33 ,34 however, these assessments have limitations. Readability formulae based on word length disregard patients’ familiarity with the (often complex) vocabulary associated with their illness, thereby potentially overestimating the difficulty of the text. Moreover, patients’ ability to comprehend written information is influenced by presentation (font type, size and/or illustrations) and reader characteristics such as motivation and stress. For these reasons, readability assessments were not undertaken within the present study.
Implications for research and practice
The development of nationally agreed PILs with agreed information of importance to surgeons and patients should improve the content of PILs. This could be achieved using ‘core information sets’, which can be defined as a minimum set of information to be communicated to all patients undergoing a certain procedure. This ‘core’ information can then be used as a platform for further discussions, tailored to individual patient needs. Results from this review (together with data obtained from literature reviews of clinical and patient-reported outcomes, the national oesophago-gastric audit database and consent consultations between patients and surgeons) have informed development of a ‘core information set’ for patients undergoing oesophageal cancer surgery.35 This involved patient participation as well as input from clinical experts (surgeons and nurses) in order to reach consensus. It is recommended that PILs pertaining to oesophageal cancer surgery incorporate this ‘core information’ as a minimum. Integration of this information into a standardised national PIL for oesophageal cancer surgery may help to ensure that patients receive high-quality information prior to surgery, presented in a way that is considered to be both acceptable and useful.27 It will also be necessary to embed similar information into consent consultations and subsequently evaluate their effectiveness using a patient-based outcome measure.36 This should help to revolutionise the process of SDM in complex areas such as cancer surgery, and work to develop, refine and evaluate this process is currently ongoing in our institution.
Conclusion
This study shows that current written information provided for patients by NHS cancer centres undertaking oesophagectomy is inconsistent and incomplete. It is recommended that surgeons work with patients to agree on standards of information provision of relevance to all stakeholders’ needs and that a uniform approach is used nationally. The development of a ‘core information set’ has established the broad areas that are considered most important among stakeholders;35 however, the details of exactly how to discuss such information remain uncertain. Further work is needed to develop optimal methods for surgeons to use data from core information sets in practice. The risk data communicated also need to be informed by high-quality evidence from RCTs especially when comparative information about alternative treatment approaches is presented, to inform SDM.
References
Footnotes
Twitter Follow Natalie Blencowe at @NatalieBlencowe
Contributors NSB and JMB designed the study. NSB and SS performed data analysis, with guidance from KNA, and NH and JE undertook the DISCERN quality assessments. NSB and AGKM wrote the first draft and all authors contributed to subsequent drafts and reviewed the final manuscript.
Funding NSB and AGKM are NIHR Academic Clinical Lecturers and SS is a N5 NIHR Academic Clinical Fellow. This paper presents independent research funded by the National Institute for Health Research (NIHR). This work was undertaken with the support of the MRC ConDuCT-II Hub (Collaboration and innovation for Difficult and Complex randomised controlled Trials In Invasive procedures—MR/K025643/1).
Competing interests None declared.
Provenance and peer review Not commissioned; internally peer reviewed.
Data sharing statement All authors had full access to all of the data in the study and can take responsibility for the integrity of the data and the accuracy of the data analysis.