Article Text

Abstract
Introduction Postoperative atrial fibrillation (AF) occurs in 30–40% of patients after cardiac surgery. Identification of recurrent postoperative AF is required to initiate evidence-based management to reduce the risk of subsequent stroke. However, as AF is often asymptomatic, recurrences may not be detected after discharge. This study determines feasibility and impact of a self-surveillance programme to identify recurrence of postoperative AF in the month of posthospital discharge.
Methods and analysis This is a feasibility study, using a cross-sectional study design, of self-screening for AF using a hand-held single-lead iPhone electrocardiograph device (iECG). Participants will be recruited from the cardiothoracic surgery wards of the Royal North Shore Hospital and North Shore Private Hospital, Sydney, Australia. Cardiac surgery patients admitted in sinus rhythm and experiencing a transient episode of postoperative AF will be eligible for recruitment. Participants will be taught to take daily ECG recordings for 1 month posthospital discharge using the iECG and will be provided education regarding AF, including symptoms and health risks. The primary outcome is the feasibility of patient self-monitoring for AF recurrence using an iECG. Secondary outcomes include proportion of patients identified with recurrent AF; estimation of stroke risk and patient knowledge. Process outcomes and qualitative data related to acceptability of patient's use of the iECG and sustainability of the screening programme beyond the trial setting will also be collected.
Ethics and dissemination Primary ethics approval was received on 25 February 2014 from Northern Sydney Local Health District Human Resource Ethics Committee, and on 17 July 2014 from North Shore Private Hospital Ethics Committee. Results will be disseminated via forums including, but not limited to, peer-reviewed publications and presentation at national and international conferences.
Trial registration number ACTRN12614000383662.
- postoperative
- atrial fibrillation
- screening
- monitoring
- electrocardiogram
- prevention
This is an Open Access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/
Statistics from Altmetric.com
Strengths and limitations of this study
This study investigates the novel concept of educating patients to undertake self-surveillance for recurrence of postoperative atrial fibrillation.
The main strength of this study is that it utilises innovative technology to screen for atrial fibrillation, which is non-invasive, quick and easy for the patient to use. The single-lead ECG recording is interpreted by a validated automated algorithm and is available for immediate review by a health professional remotely.
This is a feasibility study and therefore, the results will determine the feasibility of patient self-monitoring, and inform the design and refinement of a future large-scale intervention and implementation study.
Introduction
Atrial fibrillation (AF) is one of the most common cardiac events following cardiac surgery, occurring in 30–40% of patients.1 ,2 The incidence of postoperative AF is predicted to increase as the population ages and increased numbers of elderly people undergo cardiac surgery.3 Postoperative AF increases the risk of inhospital mortality, prolongs length of stay, and postdischarge increases costs and complications, such as stroke, renal failure and gastrointestinal complications.4 While new onset postoperative AF is generally considered to be transient and reversible,1 ,5 it may recur in up to 8% of patients in the 2 years following surgery, with an annual incidence of 2%.6 ,7 This is a likely underestimate of the actual rate due to asymptomatic AF and lack of routine surveillance.7 As postoperative AF is an independent predictor of worse long-term outcomes, including stroke and death,4 ,5 ,8 surveillance for recurrence of AF and routine screening for AF-related complications should occur postdischarge in any patient who experiences postoperative AF and is at risk of recurrent AF.8 Increased risk is associated with patient's age over 65 years, and modestly with valve surgery, and prior heart failure and hypertension.3 However, in current practice, the everyday surveillance for recurrence of postoperative AF largely falls on the patients themselves.
There is little published information on patients’ understanding and knowledge of AF, and their capacity to undertake such surveillance postcardiac surgery. Previous surveys have demonstrated that people with AF have poor knowledge of AF and the related symptoms, and are generally unaware or not concerned with their elevated risk of stroke.9–11 Patients’ education, which is individualised, has been demonstrated in a systematic review to produce most benefits for patient's self-care capability12 and thereby reduces complications and readmissions.13 No study was found that reported techniques to improve patient's capability to provide self-care following postoperative AF.
New technology that is portable, quick and easy to use increases the capability of individuals to undertake surveillance postdischarge. Utilising an iPhone-based 30 s single-lead ECG, the AliveCor heart monitor (iECG; figure 1), we have been able to successfully identify previously undetected AF in 1.5% of ambulatory community residents aged ≥65 years.14 The iECG has a validated automatic algorithm for detection of AF15 which, when used in the field, maintains a high sensitivity (98.5%) and specificity (91.4%).14 The algorithm provides an immediate automated interpretation of the ECG which is available to the treating doctors in real time through a secure server. Under the direction of a healthcare professional, it is possible that patients could use this technology in the postdischarge period to monitor for recurrence of AF.

AliveCor heart monitor.
Study aims
This study aims to:
Determine the feasibility of patients using an iECG to identify recurrence of AF in the early postdischarge period (i.e, 4 weeks postdischarge) following cardiothoracic surgery;
Determine if providing a brief inpatient AF education programme improves patient knowledge;
Explore the experience of the participant in using the iECG in the home setting, and acceptability of the intervention;
Inform the development of a future larger scale trial.
Methods and analysis
Design
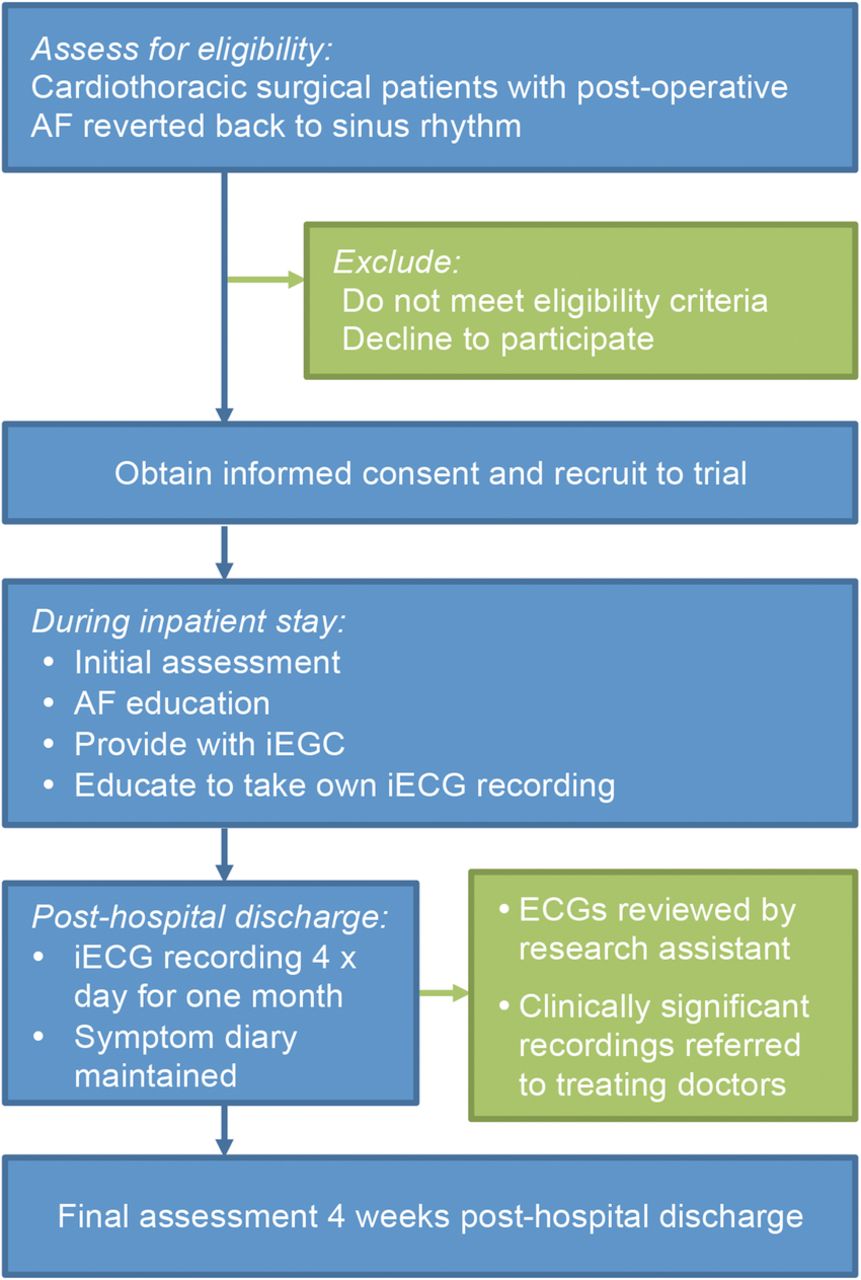
This study is a feasibility study, using a cross-sectional study design, of monitoring to detect the recurrence of AF postdischarge from hospital (figure 2; ACTRN12614000383662). We also use a prepost study design to evaluate a brief educational module on AF. The study period is from 25 March 2014 until 28 April 2015. The intervention will be offered at two hospital sites in Sydney, Australia: The Royal North Shore Hospital and The North Shore Private Hospital. Recruitment will occur between 25 March 2014 to 28 March 2015 at The Royal North Shore Hospital and between 4 August 2014 to 28 March 2015 at The North Shore Private Hospital.

{kind=link}
{kind=link}
Study flow. AF, atrial fibrillation; iECG, iPhone ECG.
Study population
All cardiothoracic surgery patients who were admitted to hospital in stable sinus rhythm and subsequently experienced postoperative AF following cardiac surgery, and who reverted or were cardioverted to sinus rhythm prior to discharge. Patients must be able to provide informed consent and be ≥18 years old. Patients will be excluded if they are non-English speaking or have insufficient cognitive capacity for the consent and interview process or are not returning home or are unable to be contacted via telephone in the postdischarge period.
Enrolment and randomisation procedures
Potential participants will be identified from the cardiothoracic wards by the ward staff in consultation with the research assistant. The research assistant will assess eligibility against the inclusion/exclusion criteria, and approach all eligible participants during their inpatient stay. The research study and the commitment involved will be clearly described in lay terms. Potential participants will be afforded every opportunity to ask questions about the study without prejudice, and to choose whether or not to participate. Participation in the study is entirely voluntary and choosing not to participate will not in any way affect any future treatment. There are no rewards or incentives for participation in the study. The participant will be enrolled into the study after the informed consent process has been completed. As this is a pre–post study and all participants will receive the intervention, there will be no randomisation and the study will not be blinded.
Baseline assessment
The baseline assessment will be performed during the inpatient stay. Sociodemographic and clinical data will be collected from the medical record and the participant.
Assessment measures:
Demographic data: age, gender, education level.
Medical history:
Data on admission for surgical procedure(s), preoperative left ventricular function and comorbidities, including thyroid function/status, obstructive sleep apnoea and pulmonary disease, will be collected.
Calculation of stroke risk using CHA2DS2-VASc score.16
Postoperative complications assessed according to major adverse cardiac events (MACE).17
AF knowledge: using a modified version of the Atrial Fibrillation Knowledge Scale18 (permission for modification obtained from original authors; see online supplement 1).
A 30 s lead-1 ECG to determine baseline heart rhythm: assessed using the iECG.
Intervention
During their inpatient stay, participants will receive brief individualised education regarding AF and its health risks specifically in relation to stroke. Participants will be educated regarding the spectrum of AF symptoms and the need to monitor and discuss any symptoms with their doctors or treating healthcare professionals. Additionally, participants will be provided with AF educational material from the Atrial Fibrillation Association (http://www.atrialfibrillation-au.org) to take home. All participants will be provided with an iPhone and the AliveCor Heart monitor (iECG) for the duration of the study period. Participants will be taught how to record their own 30 s ECG recording using the iECG and shown how to complete the symptom diary.
Postdischarge from hospital, participants will be asked to record an iECG four times per day for 4 weeks. Participants will be advised to take additional iECG recordings, as soon as practicable, if they experience AF symptoms. Each iECG automatically transmits to a secure server where each recording will be analysed by a previously validated automated AF algorithm.15 All iECG data on the server are coded for each participant and therefore, are not identifiable. The research assistant will review each iECG and the algorithm diagnosis, and all ECG's with suspected AF will be over-read by a cardiologist from the research team. If AF, or any other clinically significant event is identified, the research assistant will contact the participant to arrange for urgent follow-up with their treating doctors, and will advise the treating doctors and specialists of the findings.
Participants will also be asked to keep an AF symptom diary for 4 weeks. They will be asked to self-report on the occurrence of any AF-related symptoms including palpitations, dizziness and syncope and any medical or hospital presentation related to these.
Follow-up assessment
A follow-up assessment will be performed 4 weeks posthospital discharge, either in the participant's home or in the outpatient clinic. The research assistant will reassess the MACE and AF Knowledge Scale. The research assistant will also compare the 4 weeks of iECG readings with the AF symptom checklist and discuss the results with the participant. On completion, a letter summarising the participant's specific outcomes will be sent to their treating doctors. The participant will also be invited to participate in a process evaluation interview (as outlined in Process Measures) to explore their experience using the iECG and factors related to future sustainability.
Study outcomes
Primary outcome
Feasibility of patient self-monitoring for AF recurrence using an iECG. Assessment measures include:
Acceptability and patient's willingness to participate in the programme (measured using recruitment data including the reasons provided for non-participation);
Participants’ ability to learn to use the iECG technology and successfully take their own recordings;
The compliance of participants to the intervention (measured by the number of iECG recordings they record over the 1 month, that is, are they achieving the requested target of three to four recordings each day);
The ability of the iECG to identify recurrences of AF (measured using data from each participant obtained from the iECG—reviewed for the presence of AF by the research assistant and the automated algorithm).
Secondary outcomes
The proportion of patients identified with recurrent AF.
Patient knowledge of AF (measured using a modified version of the Atrial Fibrillation Knowledge Scale).
Estimation of stroke risk of the participants identified with recurrent AF (using CHA2DS2-VASc score).
Qualitative data regarding acceptability of patient use of the iECG.
Process measures
A detailed process evaluation will be undertaken to better appreciate factors that might influence sustainability beyond the trial setting. After each participant completes the programme, a process evaluation will be performed related to participant's experiences with the iECG. Semistructured interviews will be conducted addressing the ease of use of the iECG, and the benefits and challenges of the programme. The process evaluation interview will be audio taped to ensure accurate transcription of the information, with the written consent of the participant. The audio recording will be transcribed verbatim in a non-identifiable form and the recording deleted.
Statistical considerations
Primary analyses will be conducted using SPSS for Windows (V.19.0). New episodes of AF will be expressed as true positives divided by total number screened with accompanying 95% CIs. χ2 tests will be used to compare new cases by gender and to identify associations between AF incidence and age-group or AF risk factors. AF knowledge level will be compared preintervention and postintervention using paired t tests. Continuous variables will be reported as means± SDs, and categorical variables as numbers and percentages. Within subject differences between baseline and follow-up will be analysed using Wilcoxon signed ranks tests for non-parametric variables (two tailed p<0.05 considered significant).
As the primary outcome is feasibility and acceptability, a power calculation was not performed. A sample size of 50 participants was chosen to maximise the probability of reaching data saturation during thematic analysis of the interviews and during review of process measures such as reasons for declining participation. Analysis will be limited to complete cases to avoid artificially increasing precision around the estimates by imputing values or carrying baseline values forward. As the study is a pilot study, no interim analyses are anticipated. Interview data will be transcribed verbatim and analysed using general interpretive methods.19 Transcripts will be reviewed independently for general themes by two researchers and consensus reached.
Ethics and dissemination
National Health and Medical Research Council ethical guidelines for human research will be adhered to, and written and informed consent will be obtained from all participants. The Anzac Research Institute will administer the study. Implementation and conduct of the study will be monitored by the project management committee (authors) who have extensive experience in qualitative research and conducting clinical trials in cardiovascular disease. The results of this study will be disseminated via the usual scientific forums, including peer-reviewed publications and presentations at international conferences.
Conclusions
Postoperative AF is thought to be mainly transient and reversible. Research suggests it affects up to 8% of patients in the 2 years following surgery; however, this is a likely underestimate of the actual rate due to asymptomatic AF and lack of routine surveillance. This observational study aims to determine the feasibility and impact of self-screening using innovative technology in the postdischarge period for people who have had a transient postoperative episode of AF after cardiac surgery. The study also aims to explore the effectiveness of providing brief AF education during the inpatient stay. The study will inform the design and refinement of a future intervention for large-scale research and implementation.
We anticipate this study will demonstrate that it is possible to identify recurrence of paroxysmal AF in the postdischarge period. Early identification of AF recurrence will reduce the risk of stroke and ultimately reduce stroke burden.
References
Supplementary materials
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
Files in this Data Supplement:
- Data supplement 1 - Online supplement
Footnotes
Contributors NL, SBF, RG, AK, DM, AK, JO and LN contributed to the study design, protocol development and acquisition of funding. NL is responsible for the initial drafting of the manuscript, and acquisition of data. NL, SBF, RG, AK, DM, AK, JO and LN contributed to critical revision of the manuscript for important intellectual content; provided final approval of version to be published; and are responsible for data analysis and interpretation.
Funding This work was supported by a competitive grant from the Cardiothoracic Surgery Research and Education Fund, Sydney Medical School Foundation, University of Sydney. AliveCor provided ECG Heart Monitors for study purposes. The investigators are not affiliated with nor have any financial or other interest in AliveCor. Ms Lowres is funded by a National Heart Foundation Postgraduate Scholarship (PP12S6990). Dr Neubeck is an NHMRC early career fellow (APP1036763).
Competing interests Prof Freedman reports grants, personal fees and non-financial support from Bayer Pharma AG outside the submitted work; grants and non-financial support from Boehringer Ingelheim outside the submitted work; grants and personal fees from BMS/Pfizer outside the submitted work; personal fees from Servier outside the submitted work; personal fees from Astra-Zeneca outside the submitted work; and consulting fees from Gilead outside the submitted work. All other authors have no competing interests to disclose.
Ethics approval This study received formal ethical approval on 25 February 2014 from the Northern Sydney Local Health District Human Resource Ethics Committee (HREC/13/HAWKE/415), and on 17 July 2014 from the North Shore Private Hospital Ethics Committee (NSPHEC 2014-006).
Provenance and peer review Not commissioned; externally peer reviewed.