Article Text

Abstract
Objectives Despite a growing body of literature, uncertainty regarding the influence of physician dress on patients’ perceptions exists. Therefore, we performed a systematic review to examine the influence of physician attire on patient perceptions including trust, satisfaction and confidence.
Setting, participants, interventions and outcomes We searched MEDLINE, Embase, Biosis Previews and Conference Papers Index. Studies that: (1) involved participants ≥18 years of age; (2) evaluated physician attire; and (3) reported patient perceptions related to attire were included. Two authors determined study eligibility. Studies were categorised by country of origin, clinical discipline (eg, internal medicine, surgery), context (inpatient vs outpatient) and occurrence of a clinical encounter when soliciting opinions regarding attire. Studies were assessed using the Downs and Black Scale risk of bias scale. Owing to clinical and methodological heterogeneity, meta-analyses were not attempted.
Results Of 1040 citations, 30 studies involving 11 533 patients met eligibility criteria. Included studies featured patients from 14 countries. General medicine, procedural (eg, general surgery and obstetrics), clinic, emergency departments and hospital settings were represented. Preferences or positive influence of physician attire on patient perceptions were reported in 21 of the 30 studies (70%). Formal attire and white coats with other attire not specified was preferred in 18 of 30 studies (60%). Preference for formal attire and white coats was more prevalent among older patients and studies conducted in Europe and Asia. Four of seven studies involving procedural specialties reported either no preference for attire or a preference for scrubs; four of five studies in intensive care and emergency settings also found no attire preference. Only 3 of 12 studies that surveyed patients after a clinical encounter concluded that attire influenced patient perceptions.
Conclusions Although patients often prefer formal physician attire, perceptions of attire are influenced by age, locale, setting and context of care. Policy-based interventions that target such factors appear necessary.
This is an Open Access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/
Statistics from Altmetric.com
Strengths and limitations of this study
Comprehensive review of the topic strengthened by robust methodology, expansive literature search, stringent inclusion and exclusion criteria, and use of an externally validated quality-tool to rate studies.
Filtering studies by the conceptual understanding that culture, tradition, patient expectations and settings influence perceptions allow for unique insight regarding whether and how physician attire influences perceptions.
Unique findings including the fact that attire preferences vary by geographic location, patient age and context of care.
The inclusion of a diverse number of study designs and patient populations introduces potential for unmeasured confounding or bias.
Although we created uniform measures to apply across all studies, diverse outcomes reporting related but ill-defined patient perceptions or preferences may limit inferential insights.
Introduction
The foundation of a positive patient–physician relationship rests on mutual trust, confidence and respect. Patients are not only more compliant when they perceive their doctors as being competent, supportive and respectful, but also more likely to discuss important information such as medication compliance, end-of-life wishes or sexual histories.1 ,2 Several studies have demonstrated that such relationships positively impact patient outcomes, especially in chronic, sensitive, and stigmatising problems such as diabetes mellitus, cancer or mental health disorders.3 ,4
In the increasingly rushed patient–physician encounter, the ability to gain a patient's confidence with the goal to optimise health outcomes has become a veritable challenge. Therefore, strategies that help in gaining patient trust and confidence are highly desirable. A number of studies have suggested that physician attire may be an important early determinant of patient confidence, trust and satisfaction.5–7 This insight is not novel; rather, interest in the influence of attire on the physician–patient experience dates back to Hippocrates.8 However, targeting physician attire to improve the patient experience has recently become a topic of considerable interest driven in part by efforts to improve patient satisfaction and experience.9 ,10
For physician attire to positively influence patients, an understanding of when, why and how attire may influence such perceptions is necessary. While several studies have examined the influence of physician attire on patients, few have considered whether or how physician specialty, context of care and geographic locale and patient factors such as age, education or gender may influence findings. This knowledge gap is important because such elements are likely to impact patient perceptions of physicians. Furthermore, the existing literature stands conflicted on the importance of physician attire. For instance, in a seminal review, Bianchi6 suggest “patients are more flexible about what they consider ‘professional dress’ than the professionals who are setting standards.” However, a more recent review reported that patients prefer formal attire and a white coat, noting that “these partialities had a limited overall impact on patient satisfaction and confidence in practitioners.”11 This dissonance remains unexplained and represents a second important knowledge gap in this area of research.
Therefore, to shed light on these issues, we conducted a systematic review of the literature hypothesising that patients will prefer formal attire in most settings. Additionally, we postulated that context of care will influence patient perceptions on attire, such that patients receiving care in acute-based or procedure-based settings are less likely to be influenced by attire.
Methods
Information sources and search strategy
We followed the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) when performing this systematic review.12 With the assistance of a medical reference librarian (AH), we performed serial searches for English and non-English studies that reported patient perceptions related to physician attire. MEDLINE via Ovid (1950–present), Embase (1946–present), and Biosis Previews via ISI Web of Knowledge (1926–present) and Conference Proceedings Index (dates) were systematically searched using controlled vocabularies for key words including a range of synonyms for clothing, physician and patient satisfaction (see online supplementary appendix). All human studies published in full-text, abstract or poster form were eligible for inclusion. No publication date, language or status restrictions were placed on the search. Additional studies of interest were identified manually searches of bibliographies. Serial searches were conducted between 2 July 2013 and May 2014; the search was last updated 15 May 2014.
Eligibility criteria and study selection
Two authors (CMP and MM) independently determined study eligibility; any differences in opinion regarding eligibility were resolved by a third author (VC). Studies were included if they: (1) involved adults ≥18 years of age; (2) evaluated physician attire; (3) reported patient-centered outcomes such as satisfaction, perception, trust, attitudes or comfort; and, (4) studied the impact of attire on these outcomes. We excluded studies involving only paediatric and psychiatric patients because perceptions of attire were felt unreliable in these settings.
Data extraction and synthesis
Data were extracted from all included studies independently and in duplicate on a template adapted from the Cochrane Collaboration.13 For all studies, we abstracted the number of patients, context of clinical care, physician specialty, type of attire tested, method of assessing the impact of attire and outcomes including patient trust, satisfaction, confidence or synonyms thereof. When studies included paediatric and adult patients, we included the study but abstracted data only on adult patients when possible. Study authors were contacted to obtain missing or additional data via electronic mail. Owing to clinical and methodological heterogeneity in the design, conduct and outcomes reported within the included studies, formal meta-analyses were not attempted. Descriptive statistics were used to report data. Inter-rater agreement for study abstraction was calculated using Cohen’s κ statistic.
Definitions and classification
Physician attire was defined as either personal or hospital-issued clothing, with or without the donning of a white physician coat (recorded separately whenever possible). We considered formal attire as a collared shirt, tie and slacks for male physicians and blouse (with or without a blazer), skirt or suit pants for female physicians. Attire that did not meet these criteria was defined as casual (eg, polo shirts and blue jeans). Donning of hospital-issued or physician-owned ‘scrubs’ was recorded when these data were available.
To understand whether culture-influenced perceptions of physician attire, we assessed study outcomes by country and region of origin. Studies were also further categorised as follows: context of care was defined as the location where the patient was receiving care (eg, intensive care, urgent care, hospital or clinic). A clinical encounter was defined as a face-to-face clinical interaction between physician and patient during which the physician was wearing the study specific attire or the attire of interest. Acute care was defined as care provided in an emergency department, intensive care unit or urgent care unit; all other settings were classified non-acute. We defined family medicine, internal medicine, private practice clinics and inpatient medicine wards as studies involving medicine populations whereas studies that included patients from various specialties (eg, internal medicine and surgery) or various locations (eg, clinic, hospital were classified as being ‘mixed.’ Reports that included dermatology, orthopaedics, obstetrics and gynaecology, podiatry and surgical populations were classified as ‘procedural’ studies.
To standardise and compare outcomes across studies, the following terms were used to indicate positive perceptions or preference for a particular attire: satisfaction, professionalism, competence, comfort, trust, confidence, empathy, authoritative, scientific, knowledgeable, approachable, ‘easy to talk to’, friendly, courteous, honest, caring, respect, kind, ‘spent enough time’, humorous, sympathetic, polite, clean, tidy, responsible, concerned, ‘ability to answer questions’ and ‘took problem seriously.’ Conversely, terms such as scruffy, aloof, unkempt, untidy, unpleasant, relaxed, intimidating, impolite, rushed were considered negative outcomes denoting non-preference for the tested attire.
Risk of bias in individual studies
As recommended by the Cochrane Collaboration, two authors independently assessed risk of study bias using the Downs and Black Scale.14 This instrument uses a point-based system to estimate the quality of a given study by rating domains such as internal and external validity, bias and statistical power. A priori, studies that received a score of 12 or greater were considered high quality. Inter-rater agreement for adjudication of study quality was calculated using Cohen’s κ statistic.
Results
Of 1040 citations, 45 studies met initial inclusion criteria. Following exclusion of duplicate and ineligible articles, 30 studies were included in the systematic review (figure 1).1 ,5 ,15–42 Included studies ranged in size from 77 to 1506 patients. Although many studies did not provide gender information, when identified, a similar number of male and female participants were included across studies (33% male vs 67% female in 25 studies).1 ,5 ,15 ,16 ,19–21 ,23–28 ,30–36 ,38–42 Three studies performed in obstetric and gynaecology populations included only female patients.20 ,23 ,36 Inter-rater agreement for agreement on eligibility and abstraction of data were excellent (κ=0.94 and 0.90, respectively).

Study flow diagram.
Many of the included studies were conducted in the USA (n=10);1 ,17 ,19 ,20 ,22–24 ,31 ,36 ,37 however, other geographic locations including Canada (n=2),16 ,35 UK, Ireland and Scotland (n=5),18 ,25 ,26 ,34 ,39 Asia (n=4),5 ,21 ,28 ,41 other European nations (n=5),29 ,30 ,33 ,38 ,40 Australia and New Zealand (n=2),27 ,32 the Middle East (n=1)15 and Brazil (n=1)42 were also represented. With respect to temporality, 22 of the 30 included studies were published within the last decade1 ,5 ,15 ,16 ,19–23 ,25 ,26 ,29–33 ,36 ,38–42; however, several studies were published more than 10 years ago.17 ,18 ,24 ,27 ,28 ,34 ,35 ,37 Seven studies specified the inclusion of patients who had at least a high school or college-level education1 ,15 ,16 ,20 ,35 ,38 ,40; however, the remaining studies did not report the educational level of their population.
With respect to the specialties where studies were performed, a number of medical disciplines including internal medicine, surgery, obstetrics and gynaecology, family practice, dermatology, podiatry and orthopaedics were represented. The context of care within the 30 individual studies varied substantially and spanned hospitalised and outpatient settings. Medical and surgical clinics, emergency departments, hospital wards, private family practice clinics, urgent and intensive care units, and military-based clinics were also featured in the included studies (table 1).
Characteristics of included studies
Of the 30 included studies, 28 studied specific patient perceptions and preferences regarding physician attire,1 ,5 ,15–31 ,33–37 ,39–42 while 2 only measured preference attire.32 ,38 In total, more than 32 unique patient perceptions were reported across the included studies. The most common patient perceptions studied were confidence in their physician (n=12), satisfaction (n=9), professionalism (n=7), perceived competence (n=7), comfort (n=6) and knowledge (n=6). Studies obtained input from patients regarding how attire influenced their perceptions of physicians through a variety of measures, including written questionnaires, face-to-face question/answer sessions, and surveys either before or following clinical care episodes. The instruments used to obtain patient input regarding physician attire included pictures of male and female models dressed in various attire, written descriptions of attire, as well as feedback regarding physician encounters either before or after a clinical service was provided to the patient.
A preference for specific physician attire or positive influence of physician attire on patient perceptions was reported in 21 of the 30 studies (70%).1 ,5 ,15 ,16 ,19–21 ,25–27 ,30 ,32–36 ,38–42 When patients voiced a preference or were influenced by physician attire, formal attire was almost always preferred followed closely by white coats either with or without formal attire. In studies from the Far East, traditional attire was associated with increased patient comfort with their physician5 ,21; however, this was not the case in the single study from the Middle East where traditional apparel was not preferred by patients over formal attire.15 Notably, patient age was often predictive of attire preference with patients older than 40 years of age uniformly preferring formal attire compared to younger patients in seven studies.19 ,27 ,28 ,32 ,34 ,38 ,40 Conversely, younger patients often felt that scrubs were perfectly appropriate or preferred over formal attire.26 ,36 ,38 ,41 These preferences extended to items such as facial piercings, tattoos, loose hair, training shoes and informal foot wear in three studies among younger patients.19 ,32 ,41 Regardless of attire, being well-groomed in appearance and displaying visible nametags were viewed favorably by patients when this question was specifically asked in the included studies.
Influence of geography on attire preferences
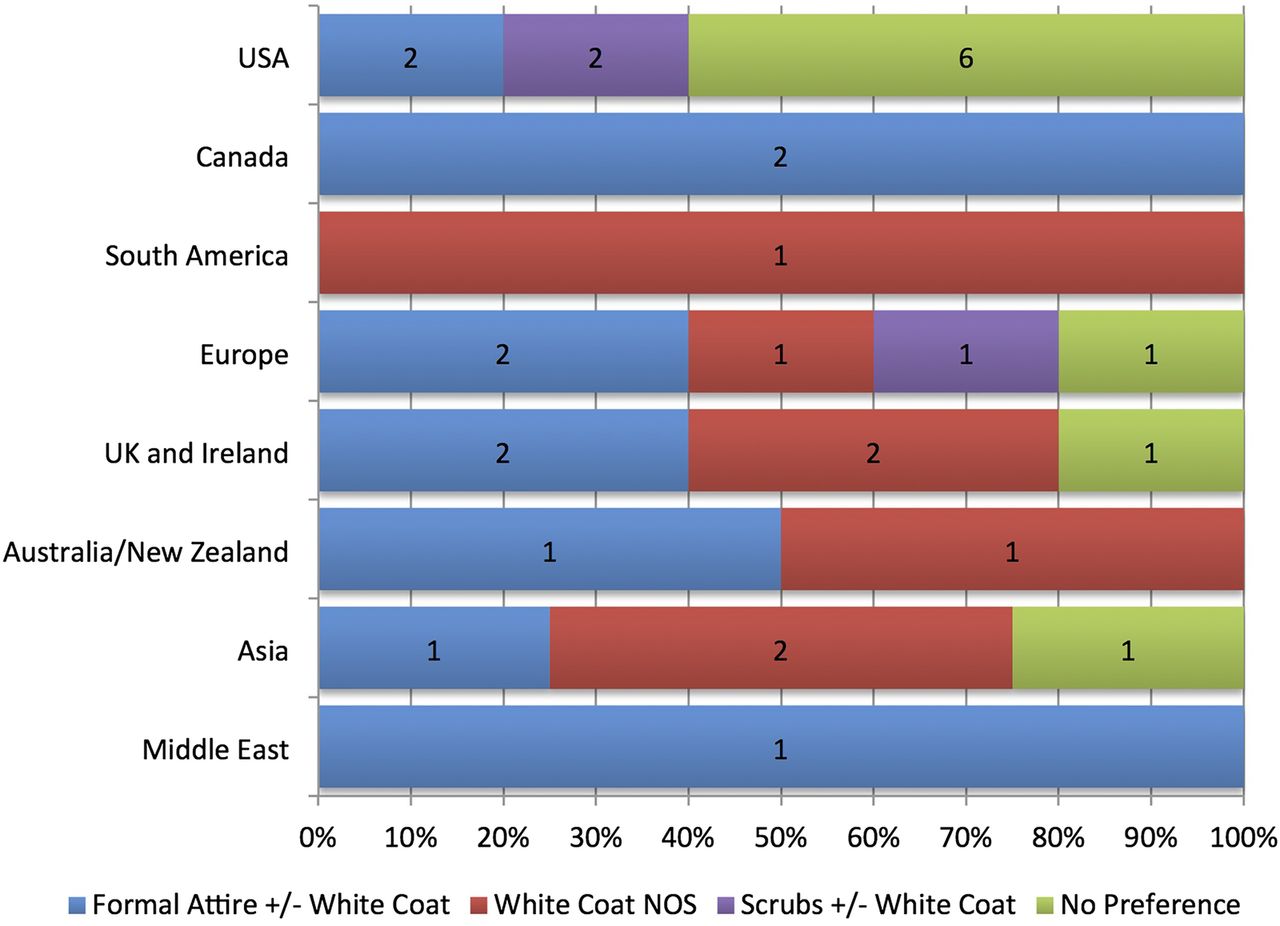
Geography was found to influence perceptions of attire, perhaps reflecting cultural, fashion or ethnic expectations. For instance, only 4 of the 10 US-based studies reported that attire influenced patient perceptions regarding their physician. In comparison, Canadian studies reported a preference for formal attire and a white coat.16 ,35 Similarly, among five studies from the UK, Scotland and Ireland,18 ,25 ,26 ,34 ,39 four reported that patients preferred formal attire or white coats.25 ,26 ,34 ,39 Similarly, four of five studies from other European nations found that patient preferences, trust or satisfaction were influenced by physician attire.30 ,33 ,38 ,40 Of these four studies, three studies found a preference for formal attire or white coats30 ,33 ,40 compared to one where scrubs were preferred38 (figure 2).

Stacked bar chart showing variation in patient preference for physician attire across geographic regions.
Six studies included patients from Asia, Australia and New Zealand.5 ,21 ,27 ,28 ,32 ,41 Of the four Asian studies,5 ,21 ,28 ,41 two were performed in Korea5 ,21 and two in Japan.28 ,41 Both studies from Korea concluded that physician attire and white coats positively influenced patient confidence, trust and satisfaction.5 ,21 While one Japanese study reported that the majority of patients older than 70 years preferred white coats, satisfaction was not statistically affected by white coats during consultations.28 Conversely, another study from Japan found that formal attire with a white coat was considered the most appropriate style of dress for a physician.41 However, the two studies conducted in Australia and New Zealand found that patients preferred white coats and formal attire when rating physicians.27 ,32 Similarly, the single study from the Middle-East found that 62% of patients preferred male physicians to wear formal attire whereas 73% preferred female physicians to wear a long skirt. As with the single study from Brazil, there was also a significant preference for a white coat to be worn, regardless of physician gender.15 ,42
Influence of clinical encounters on attire preference
Of the 30 included studies, 12 studies surveyed patients regarding their opinions about physician attire following a clinical encounter.5 ,17 ,18 ,22–24 ,27–29 ,31 ,37 ,39 Within these 12 studies, only 3 (25%) reported that attire influenced patient perceptions of their physician.5 ,27 ,39 Formal attire without white coat was preferred in one of the three studies39; a white coat with other attire not specified was preferred in two studies.5 ,27 However, in the remaining nine studies, patients did not voice any attire preference following a clinical encounter suggesting that attire may be less likely to influence patients in the context of receiving care.
Conversely, clear preferences regarding physician attire were reported in 16 of 18 studies where patients received either written descriptions (n=1)19 or pictures of physician attire without a corresponding clinical interaction with a physician (n=17).1 ,15 ,16 ,20 ,21 ,25 ,26 ,30 ,32–36 ,38 ,40–42 The majority of these studies (n=10) preferred formal attire either with or without a white coat1 ,15 ,16 ,19 ,30 ,32 ,34 ,35 ,40 ,41; three studies reported a preference for scrubs with or without white coats,20 ,36 ,38 whereas a white coat with other attire not specified was preferred in five studies (figure 3).21 ,25 ,26 ,33 ,42

Stacked bar chart showing variation in patient preference for physician attire with clinical encounters.
Influence of context of care on patient preferences for attire
Context of care also influenced attire preference. For example, six studies conducted in general medicine outpatient clinics reported that patients preferred formal attire with or without a white coat,1 ,15 ,34 ,35 ,40 ,41 while three reported preference for a white coat with other attire not specified.5 ,21 ,25 Only two studies reported no attire preferences in this specific medical discipline in this setting.28 ,29 Conversely, four of five studies conducted in acute care settings reported no attire preferences17 ,18 ,31 ,37; only one study reported a preference of formal attire with or without a white coats.16 Of the seven procedural studies that included patients from obstetrics and gynecology, gastroenterology, emergency care and surgery,19 ,20 ,22 ,23 ,33 ,36 ,39 three reported either no specific preference for attire22 ,23 ,39 or preference for scrubs over other attire.20 ,36 Only two of the seven studies reported preference for formal attire or white coats in these settings.19 ,33 Studies categorised as being ‘mixed’ in context (n=6) correspondingly reported heterogeneous preferences, spanning no preference for attire, to preference for formal attire, white coat and scrubs with white coats only24 ,26 ,30 ,32 ,38 ,42 (figure 4).

{kind=link}
{kind=link}
{kind=link}
{kind=link}
Stacked bar chart showing variation in patient preference for physician attire across contextual aspects of care.
Risk of bias within included studies
We assessed risk of bias within the included 30 studies using the Downs and Black Quality Scale. Studies with higher quality were characterised by the fact that they more commonly reported characteristics of included and excluded patients and provided more accurate descriptions of attire based interventions. Using this scale, 8 of the 30 included studies were associated with higher methodological quality (table 2). Inter-rater agreement for study quality adjudication was excellent (κ=0.87).
Risk of bias within included studies
Discussion
In this systematic review examining the influence of physician attire on a number of patient perceptions, we found that formal attire with or without white coats, or white coat with other attire not specified was preferred in 60% of the 30 included studies.1 ,5 ,15 ,16 ,19 ,21 ,25–27 ,30 ,32–35 ,39–42 However, no specific preference for physician attire was demonstrated in nine studies and preference for scrubs was noted in three procedural studies. Importantly, we found that elements such as patient age and context of care in addition to geography and population appear to influence perceptions regarding attire. For example, patients who received clinical care were less likely to voice preference for any type attire than patients that did not, perhaps exemplifying the importance of interaction over appearance. Similarly, older patients and those in European or Asian nations were more likely to prefer formal attire than those from the USA Collectively, these findings shed new light on this topic and suggest that although professional attire may be an important modifiable aspect of the physician–patient relationship, finding a ‘one-size-fits-all’ approach to optimal physician dress code is improbable. Rather, ‘tailored’ approaches to physician attire that take into account patient, provider and contextual factors appear necessary.
In an ever-changing medical landscape, patient satisfaction has become a focal point for providers and health-systems. Therefore, preferences regarding physician attire have become a topic of considerable interest as a means to improve first-impressions and perceptions regarding quality of care. Why may patient perceptions and preferences vary so greatly across studies? Multiple reasons are possible. First, our review supports the notion that patients often harbour conscious and unconscious biases when it comes to their preferences regarding physician attire.7 ,37 For example, while many patients did not report an attire preference when directly surveyed, several of our included studies found that images of patients dressed in white coats or formal suits were more often associated with perceptions of trust and confidence even if patients also expressed no specific preferences regarding attire.16 ,17 ,37 In support, studies that included physician encounters were less likely to find specific preferences (3/12 studies) compared to studies conducted outside of a physician–patient meeting (18/18 studies). These likely subconscious beliefs are important to acknowledge, first, especially patients from a ‘baby-boomer’ generation who often conflate formal attire with physician competence and confidence.19 ,34 Second, the influence of cultural aspects on attire expectations is likely to be substantial on attire preferences. As noted in our review, studies originating from the UK, Asia, Ireland and Europe most often expected formal attire with or without white coats; attire that did not include these dress-codes were least preferred. Third, the influence of context of care on expectations regarding physician dress is important to acknowledge. A defined ‘uniform’ for physicians may be an expectation for certain patients and/or specific settings. Finally, it is important to remember that sartorial style is but skin-deep and not a surrogate for medical knowledge or competence. Even the best-dressed physicians are likely to fare poorly in the eyes of their patients if medical expertise is perceived absent.
Our results must be interpreted in the context of important limitations. First, like all systematic reviews, this is an observational study that can only assess trends, not causality, using available data. Second, the inclusion of a diverse number of study designs and patient populations creates a high-likelihood of unmeasured confounding and bias. Third, only eight of the included studies were rated as being at low risk-of-bias using the Downs and Black scale. This finding reflects in general the limited quality of this literature and suggests that while physician attire may be important, more methodologically rigorous studies are needed to better understand and truly harness this aspect to improve patient satisfaction. Fourth, a wide variety of related but often ill-defined patient perceptions or preferences were measured within the included studies; although we collapsed these categories into more uniform measures, our ability to draw insights from these diverse outcomes is limited. Finally, we specifically did not take into consideration risk of infection associated with attire. Since a recent study examined this in considerable detail,11 our review complements the literature in this regard.
Despite these limitations, our review has notable strengths including a thorough literature search, stringent inclusion and exclusion criteria, and use of an externally validated quality-tool to rate studies. Second, our review was guided by the conceptual understanding that culture, tradition, patient expectations and settings influence perceptions related to physician attire. Filtering and assessing studies in this fashion provided us with insights when, if and how physician attire influences patient perceptions. Finally, we also included 16 new articles that have been published since the last comprehensive review of this topic6; inclusion of these new studies (including a substantial number of studies from diverse countries and healthcare settings) lends greater external validity and importance to our findings.
How may hospitals and healthcare facilities use these data to effect policy decisions? Our review suggests that formal attire is almost always preferred with respect to physician attire may be unwise given the heterogeneous evidence-base and methodological quality of available data. After contacting human resource professionals, other administrators and researching information available on their public websites at all 10 of the top 10 2013–2014 US News & World Report Best Hospitals, we found that 5 had written guidelines calling for formal and professional attire throughout their institutions. Our findings suggest that such sweeping policies that apply to all healthcare specialties, settings and acuities of care may paradoxically not improve patient satisfaction, trust or confidence. Rather, interventions that test the impact of when and how care is delivered, types of patients encountered, and approaches used to measure patient preferences are needed. In order to better tailor physician attire to patient preferences and improve available evidence, we would recommend that healthcare systems capture the ‘voice of the customer’ in individual care locations (eg, intensive care units and emergency departments) during clinical care episodes. The use of a standardised tool that incorporates variables such as patient age, educational level, ethnicity and background will help contextualise these data in order to derive individualised policies not only for each area of the hospital, but also for similar health systems in the world.
In summary, the influence of physician attire on patient perceptions is complex and multifactorial. It is likely that patients harbour a number of beliefs regarding physician dress that are context and setting-specific. Studies targeting the influence of such elements represent the next logical step in improving patient satisfaction. Hospitals and healthcare facilities must begin the hard work of examining these preferences using standardised approaches in order to improve patient satisfaction, trust and clinical outcomes.
Acknowledgments
The authors gratefully acknowledge the assistance of Drs Edwards, Gallagher, Stelfox, Fischer, Kocks, Gherardi, Chae, Dore, Maruani, Wilkinson, Baddini-Martinez, and Budny who provided additional unpublished data for this study.
References
Supplementary materials
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
Files in this Data Supplement:
- Data supplement 1 - Online supplement
Footnotes
Contributors VC, CMP, SS and MM were involved in the concept and design. VC, CMP, SS, MM, AH and JJP were involved in the analysis and interpretation of data. VC, CMP, SS, MM, AH and JJP were involved in the drafting and critical revision. VC, CMP, SS, MM, AH and JJP were involved in the final approval.
Funding VC is supported by a career development award from the Agency for Healthcare Research and Quality (1K08HS022835-01).
Competing interests None.
Provenance and peer review Not commissioned; externally peer reviewed.
Data sharing statement The authors have posted their data sets on Dryad.