Article Text

Abstract
Objectives To synthesise contributing factors leading to medicine-related problems (MRPs) in adult patients with cardiovascular diseases and/or diabetes mellitus from their perspectives.
Design A systematic literature review of qualitative studies regarding the contributory factors leading to MRPs, medication errors and non-adherence, followed by a thematic synthesis of the studies.
Data sources We screened Pubmed, EMBASE, ISI Web of Knowledge, PsycInfo, International Pharmaceutical Abstract and PsycExtra for qualitative studies (interviews, focus groups and questionnaires of a qualitative nature).
Review methods Thematic synthesis was achieved by coding and developing themes from the findings of qualitative studies.
Results The synthesis yielded 21 studies that satisfied the inclusion and exclusion criteria. Three themes emerged that involved contributing factors to MRPs: patient-related factors including socioeconomic factors (beliefs, feeling victimised, history of the condition, lack of finance, lack of motivation and low self-esteem) and lifestyle factors (diet, lack of exercise/time to see the doctor, obesity, smoking and stress), medicine-related factors (belief in natural remedies, fear of medicine, lack of belief in medicines, lack of knowledge, non-adherence and polypharmacy) and condition-related factors (lack of knowledge/understanding, fear of condition and its complications, and lack of control).
Conclusions MRPs represent a major health threat, especially among adult patients with cardiovascular diseases and/or diabetes mellitus. The patients’ perspectives uncovered hidden factors that could cause and/or contribute to MRPs in these groups of patients.
- QUALITATIVE RESEARCH
- DIABETES & ENDOCRINOLOGY
- CARDIOLOGY
This is an Open Access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/
Statistics from Altmetric.com
Strengths and limitations of this study
To the best of our knowledge, it is the first systematic review conducted on qualitative research regarding the contributory factors leading to medicine-related problems from the perspectives of adult patients with cardiovascular diseases and diabetes mellitus.
The study undertook a comprehensive systematic review with a thematic synthesis approach.
Despite using studies from 12 countries, the analytical themes developed from the review comprised a high level of conceptual thinking that could be applied across different studies.
The review was restricted to the experiences of patients from 12 countries, which could limit the generalisability of the findings.
The qualitative studies (n=21) in the literature were limited, so further qualitative studies are needed to assess the contributory factors leading to medicine-related problems.
Introduction
Medicine-related problems (MRPs) emerged as a concept in the early 1990s as “the detrimental experience regarding drug therapy, which potentially or actually causes an interference with its desired outcome.”1 MRPs affect healthcare and economic situations and contribute to a tremendous increase in morbidity, mortality and healthcare expenditure worldwide.2–4
MRPs represent a major issue, particularly in chronic conditions such as cardiovascular diseases (CVDs) and diabetes mellitus (DM).5 The aforementioned conditions are expected to be the major source of morbidity by 2020.6 ,7 In addition, these two conditions are interrelated; it has been documented that DM is a key factor that leads to CVDs, as people with diabetes are three to four times more likely to have a CVD.8 ,9 Consequently, the combination of CVDs and DM, which can result in multiple complications, represents a major concern for healthcare professionals.
More specifically, patients with CVDs and/or DM are more susceptible to MRPs due to long-term use of medicines and the inevitable polypharmacy.7 ,10 ,11 However, many additional factors that contribute to MRPs in patients with CVDs and/or DM have gone under-reported.
Studies in the literature, which investigated risk factors contributing to MRPs in patients with CVDs/DM, were mainly quantitative; only a few studies were qualitative. Quantitative studies investigating risk factors contributing to MRPs involved either direct observations or were made retrospectively using data extracted from medical records.12–15 However, most of the studies reported old age and polypharmacy extensively; few studies reported gender, depression, education, cohabitation and immobilisations.16 Nonetheless, qualitative studies investigating contributory risk factors leading to MRPs have been rather limited.
Therefore, this review aims to explore and evaluate contributory factors leading to MRPs among adult patients with CVDs and/or DM from their perspectives.
Methods
We searched the PubMed, EMBASE, ISI Web of Knowledge, PsycInfo, International Pharmaceutical Abstract and PsycExtra databases for entries between January 1990 and March 2014. The search strategy evaluated articles obtained predominantly through databases. Additional articles were retrieved through the bibliography lists of published reviews, where applicable.
The search strategy combined established methodological terms for qualitative research (qualitative research, qualitative studies, nursing methodological research, narrative analysis) and the following terms: Medicine (drug/medication) related problems, medicine (drug/medication) use, diabetes mellitus, cardiovascular diseases, patients’ perspectives, patients’ beliefs, patients’ attitudes, patients’ views, patients’ opinions, patients’ knowledge, patients’ behaviours and contributory factors. In addition, Medical Subject Headings (MeSH) relating to MRPs, CVDs/DM, risk factors and patients’ perspectives were explored.
Study selection
We included studies that utilised phone interviews, face-to-face interviews, focus groups and open-ended questionnaires published in peer-reviewed journals.
The inclusion criteria involved studies focusing on patients’ perspectives on the use of medicines and MRPs and were conducted on adult patients with CVDs and/or DM.
On the other hand, the exclusion criteria flagged studies that were quantitative in nature, studies with closed-ended questionnaires and studies focusing on conditions other than CVD/DM.
Initially, one reviewer (AA) conducted the search and screened titles. At this stage, studies with irrelevant titles were excluded. Next, the abstracts of the remaining studies were evaluated independently for inclusion by two reviewers (MG and ZA). Any disagreements that were encountered were resolved via a discussion. No language limits were applied. However, the search results only generated English studies. Figure 1 demonstrates the details of the data extraction process.

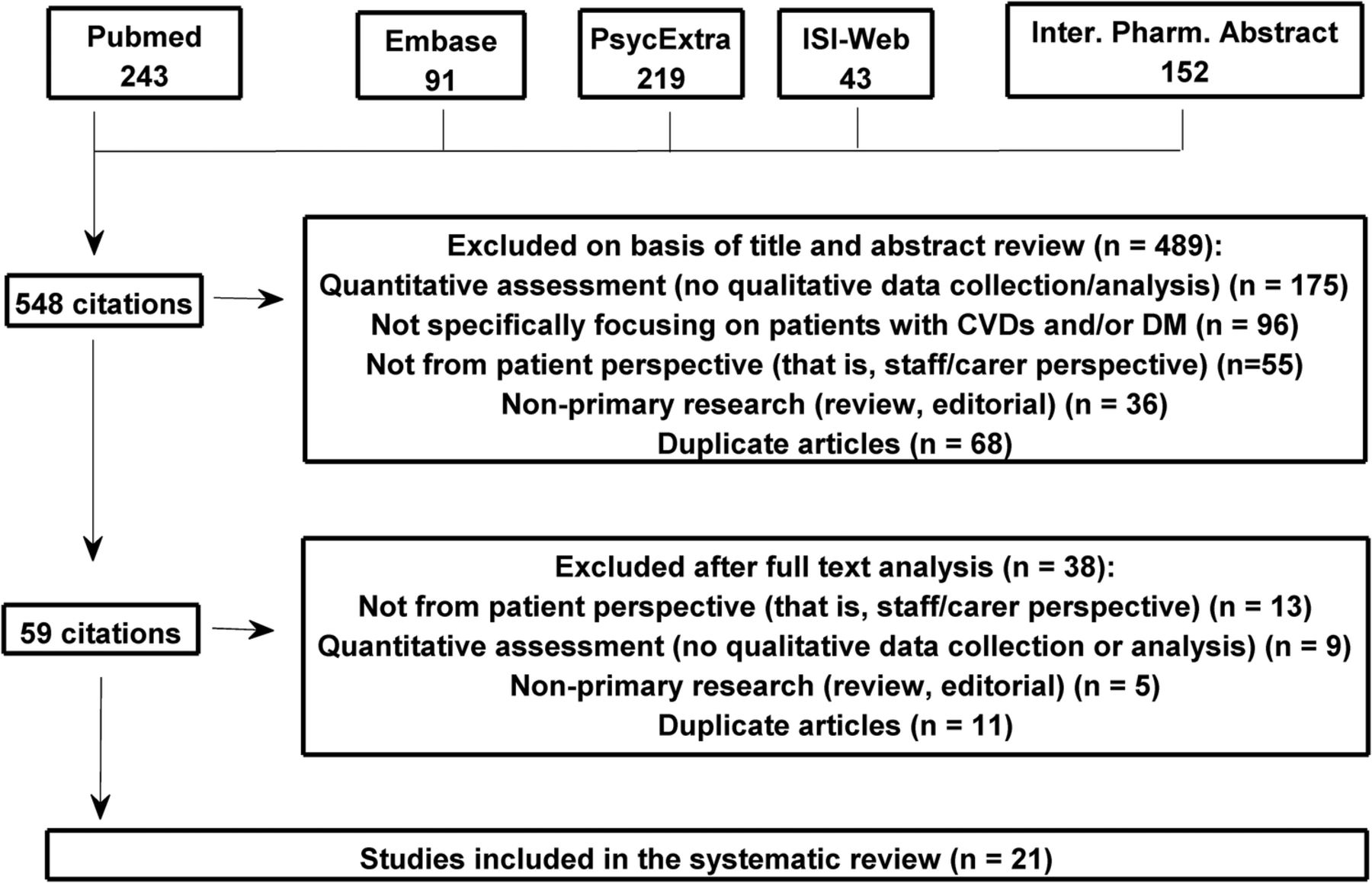{kind=link}
Data extraction and study selection process. CVD, cardiovascular diseases, DM, diabetes mellitus.
Data synthesis and analysis
In order to extract data from articles, we adopted the systematic review approach for qualitative research by Dixon-Woods et al.17 This allowed the emergence of broad concepts. Then, data was synthesised by utilising the thematic analysis approach,18 which enables extraction of concepts and hypotheses from multiple qualitative studies.
Based on the extracted results, we developed textual summaries and tables. From the textual summaries and tables, we identified emerging themes which described the meaning and content of the included studies. We then inspected similarities and differences across the textual summaries in order to avoid contradiction and reduce the developed number of themes. Subsequently, we agreed on the final list of themes through discussion and consensus.
Finally, we coded the full list of papers for the presence or absence of themes. The codes were tabulated afterwards by country in order to inspect similarities and differences across countries.
Since our approach was qualitative, the presence of a theme in more than one paper did not indicate its importance in the studied population.19 However, a theme appearing in more than one paper did denote to a degree its validity. Thus, the number of studies within a specific theme was reported in this review.
Quality of synthesis assessment
The quality of papers was assessed using the checklist developed by Dixon-Woods et al.17 This assessment was based mainly on clarity, consideration of ethical issues, and transferability of the sample data and analysis across different settings. Furthermore, the critical appraisal skills programme criteria20 were used to rank the papers based on 10 questions that fulfilled the clarity, methods and results of the studies. Consequently, studies were grouped into low (one star: 0–3 points), medium (two stars: 4–7 points) and high quality (three stars: 8–10 points). Low-quality studies were not excluded, but caution was taken when interpreting their results.
Results
A total of 21 studies (including 836 participants) from 12 countries met the inclusion criteria (table 1) and were conducted in the following countries: Australia,21 Brazil,22 Cameroon,23 Canada,24 Croatia,25 Ireland,26 Malaysia,27 ,28 South Africa,29 Spain,30 Taiwan,31 the UK7 ,32–37 and the USA.38–40 The majority of the studies investigated type 2 DM (n=15); fewer studies investigated CVDs. Thus, only two studies investigated hypertension (HTN), one investigated heart failure and one studied CVDs in general. The remaining two studies investigated DM/HTN and DM/HTN/stroke, respectively. Eight studies used focus groups, 12 used interviews and one study used a mixture of these methods. The review covered areas related to patients, conditions and medicines.
Characteristics of the included studies
Narrative synthesis
The main findings of the review showed that contributory factors to MRPs involved three themes: patient-related (socioeconomic and lifestyle), medicine-related and condition-related factors. Table 2 lists the studies that reported or discussed each theme.
Themes and subthemes emerging from the studies
Patient-related factors
Socioeconomic-related factors
Patients from six countries reported socioeconomic factors leading to MRPs in DM and CVDs, including: beliefs, family history of the condition, poor finances, relationships with healthcare professionals (lack of communication and not enough education), inadequate knowledge and low self-esteem (table 2).
Beliefs regarding CVDs/DM were reported as a problem in three studies from the UK.32 ,34 ,36 Patients perceived that DM was given by God and higher powers had control over their condition. One patient reported:‘God has given me this disease of sugar. Whatever happens, it happens because God wants it to happen.’
Moreover, a family history of DM was reported in three studies from the UK34 ,36 and the USA.38
In addition, poor finances were reported by patients in four studies from Ireland,26 South Africa,29 Croatia25 and the USA.39 A lack of necessary finances prevents patients from buying the appropriate food (for their diet)29 and from going to doctors.26
Consequently, the financial situation implicated the relationship of the patients with the healthcare professionals. Patients have reported that they were not getting value for their money from healthcare providers.26 For instance, one patient reported:I don't mind paying when I'm sick, but it's very expensive to pay the GP when I'm only getting a check-up with the nurse.
Thus, the patients felt victimised by healthcare professionals25 ,26 ,29 and reported a lack of communication with healthcare professionals.18 They described doctors as either too busy to see them26 ,27 or not giving enough information about diagnosis and medicines.32 ,33 ,37 Other patients reported having been belittled by doctors.25 In another study, patients accounted for the lack of communication with healthcare professionals due to language barriers.33
Subsequently, patients reported a lack of knowledge as a major cause for type 2 DM.25 This situation led to the lack of motivation about their disease and affected the intake of medicines. Patients asserted the need for further education and training about their condition.
A lack of knowledge resulted in patients’ low-self esteem because of their condition.25 ,40 Hence, patients felt unaccepted socially, less comfortable with their colleagues and less worthy, from being diabetic.25 ,40
Lifestyle-related factors
Lifestyle-factors were reported in studies from 11 countries and included: diet (excessive alcohol/caffeine intake), lack of exercise, lack of time to see the doctor, obesity, smoking and stress.
Diet was a major issue stated in 16 studies (table 2). In this respect, patients had different behaviours towards their diet. For instance, one group of patients admitted the importance of a healthy diet, yet could not control their diets.22 ,31–33 Thus, one participant reported22:Regarding the diet, I try to fight so as not to eat certain foods, but sometimes I can't help myself.
In this respect, patients appreciated the importance of a healthy diet in controlling DM,32 yet overestimated its importance to be beyond medicines.31 They were also aware that a poor diet, including excess alcohol24 and caffeine intake,24 ,29 exacerbated their conditions. Another group of patients misunderstood the concept of a healthy diet. They believed that eating bitter foods could control DM,33 or applied portion sizes to their diets.40 In the latter case, patients had difficulty eating smaller portions and/or even changing their favourite foods. On other occasions, patients claimed that diet quality was responsible for DM.26
In addition, a lack of exercise was reported in 11 studies from five countries, including Brazil,22 Canada,24 the UK,32–36 South Africa29 and the USA.38–40 A group of patients overestimated the importance of exercise, claiming that it can cure any existing disease.31 Patients reported difficulty exercising although they were aware of its importance.36 ,40 They justified their work, travel, stress, the weather and lack of time as the reasons behind their decreased physical exercise.22 ,33 ,34 ,36 ,39 A lack of time was more reported in women whose culture expected them to stay indoors after they got married.36
Moreover, obesity was described in four studies (Brazil,22 South Africa,29 the UK32 and the USA38) as a cause of DM. Patients blamed weight gain as the cause for their increase in blood glucose level and diabetic complications.32 ,38 Moreover, they attributed insulin to be one of the causes of obesity.32
Stress emerged in five studies from three countries, including Ireland,26 the UK32 ,34 ,35 and the USA.38 Stress was identified as a result of changes in culture and climate, poor housing and migration of ethnic minorities.38 Patients considered stress to be a major cause of their condition.26 ,32 ,34 ,35 ,38 ,40 For instance, one patient reported:In 1998, my mother died, and I was unable to go to the funeral. During these months, I developed diabetes.
Patients also perceived that stress control could be an effective way to cure their condition34 since stress led to a poor diet, smoking and a lack of exercise.
Medicine-related factors
Medicine-related factors were found in 14 studies from 11 countries and included two types of factors: those related to the use of medicines and those related to knowledge about medicines.
Factors related to the use of medicines included medicine non-adherence and polypharmacy. Medicine non-adherence was reported in 10 studies from seven countries, including Brazil,22 Canada,24 Croatia,25 Malaysia,27 ,28 Spain,30 Taiwan,31 the UK7 and the USA.39 ,40 Patients justified non-adherence to medicines as difficulty following the treatment regimen,25 depression and stress,40 forgetfulness in taking the medicines,7 ,22 ,27 ,28 ,30 a lack of routine in taking the medicines,24 changes in medicine routines24 and the inconvenience of taking insulin. For instance, patients asserted that oral hypoglycaemics are more convenient to take than insulin30:I prefer pills more than insulin. You know, swallowing a pill causes no pain. And when I know I will eat more I just take another pill or an extra half.
Furthermore, intentional non-adherence was reported in some studies where patients changed their insulin doses depending on their food regimen.30 In another scenario, patients stopped taking their medicines when they exercised, acting on the assumption that exercise reduces blood sugar level. Thus, patients changed the dose/regimen of their medicines to fit with their daily activities.7
Poylpharmacy was reported among patients with type 2 DM in two studies from Brazil22 and Canada.28 Polypharmacy caused inconvenience in taking medicines22:Medication: this has been my biggest problem in this current phase. I take medication for blood pressure, circulation, diabetes, vitamins. I used to mix up the time of each, but today, thanks to orientation, I'm overcoming this stage.
Factors relating to knowledge about medicines included lack of knowledge about how the medicines worked, fear of the chemical nature of medicines and their side effects and a lack of belief in medicine.
The lack of knowledge about how medicines worked was described in three studies in Canada,24 the UK7 and Spain.30 Patients could not identify most of their medicines apart from the diuretics, which they called ‘water pills.’24 Moreover, patients could not understand how their medicines worked, even when they read the patient information leaflet.30
This lack of knowledge created fear in patients regarding the chemical nature of medicines, the side effects of medicines and being obliged to take medicines all of their lives.7 ,26 ,27 ,30–32 ,35 For instance, patients referred to oral hypoglycaemic agents and insulin as ‘pharmaceutical toxins.’31
Additionally, patients were afraid of the side effects and complications of medicines. They attributed various side effects to medicines, including hypoglycaemia and gastrointestinal disturbances to insulin,32 kidney failure to oral hypoglycaemic agents,31 and nausea/vomiting to antihypertensive agents.30 In the last case, a patient reported:I don't like them (medicines); they have lots of side effects. They can make you sick… I think that I might get worse instead of better.
These fears promoted a lack of belief in medicines among patients.21 Subsequently, patients started to believe in natural remedies as an alternative to medicines.30 ,32 ,38 They referred to natural therapies as ‘a cure’ that should be used alongside traditional medicines.38 In another scenario, patients believed that natural therapies were superior to medicines.32 In this respect, natural therapies reported for curing DM included natural drinks (composed of minerals and water),38 and plant products (such as aloe vera, arnica, cactus, silk cottonwood tree, tree spinach and violet water).32
Condition-related factors
Condition (clinical)-related factors were reported from 11 countries as a major theme. Factors included a lack of knowledge/understanding of the condition, fear of the condition and its complications, stress from the condition and a lack of control over the condition.
Lack of knowledge/understanding of the condition (CVDs/DM) emerged as a major theme in 11 studies from seven countries, including Australia,21 Cameroon,23 Canada,24 Malaysia,27 ,28 Spain,30 the UK32 ,33 ,35 ,37 and the USA.38
For CVDs, patients expressed a lack of knowledge about their heart failure, HTN and stroke. Patients with heart failure did not know enough about their disease symptoms.21 Moreover, hypertensive patients did not understand the nature of their disease,28 ,30 struggled to define their condition24 and considered it an underlying risk factor to myocardial infarction rather than a disease.35 Patients justified their lack of knowledge by citing short consultations with physicians, not obtaining enough information from physicians and obtaining information from non-medical sources such as television and magazines. For instance, one patient reported:Anything I know about blood pressure I've read in books, the doctor tells me absolutely nothing … High blood pressure: factors related to compliance with treatment 127. I want him to tell me where high blood pressure comes from.
Similarly, patients with DM lacked knowledge about the disease and misunderstood its causes and complications.23 ,25 ,27 ,29 ,32 ,33 ,36 Regarding the DM condition and causes, patients’ perceptions of DM were influenced by other people's accounts and experiences.32 Patients viewed the condition as an illness that took away their health and strength,36 changing their lifestyle.25 They could not differentiate between types 1 and 2 DM,27 considered high sugar intake to be the cause of DM, and perceived DM to be sexually and genetically transmitted.23 ,33 Moreover, patients believed that diabetes was not dangerous if it did not require insulin.32 Patients were only aware of the microvascular complications (such as foot disease) of DM.26 Moreover, they were aware of the disease's signs and symptoms (such as dry mouth, tiredness, dizziness, irritation, blurred vision, micturition and extreme thirst) only after they encountered them.28 ,38
The lack of knowledge about the condition created fear in patients’ minds of the disease itself38 and they could not accept the disease easily.25 ,33 One patient reported38:Diabetes is a disease that kills you little by little.
Diseases additionally resulted in stress about the condition, which was particularly observed in patients with multiple comorbidities.36 For instance, diabetic patients who had asthma as a comorbidity could not exercise due to asthma symptoms, such as shortness of breath and swollen feet and joints:They tell you to exercise … but I can't move around a lot because I have a problem with my leg (arthritis). If I walk a little, then it swells up.
As a result, patients were not able to control their condition,22 ,26 which led to frustration, depression and anxiety.
Discussion
To the best of our knowledge, this review is the first systematic analysis of the perspectives of adult patients with CVDs/DM on contributory factors leading to MRPs. We explored patients’ knowledge, beliefs and behaviours towards medicines. The majority of studies evaluated patients with DM; only a few studies evaluated patients with CVDs. The three themes emerging from this review included: patient-related (socioeconomic-related and lifestyle-related), clinical-related and medicine-related factors.
Patient-related factors
Socioeconomic-related factors
Socioeconomic factors (genetic, cultural behaviour and financial situations) affected patients’ perceptions of disease and the medicines contributing to MRPs. Patients perceived genetic factors and religious beliefs to be the cause of their DM.19 ,21 Patients from Christian and Muslim backgrounds named God as the cause for their DM. These attitudes were confirmed by other studies which showed that religious values contributed to MRPs.41 ,42 In addition, patients felt socially stigmatised by their DM, which affected their self-esteem. They also blamed their financial situation for contributing to MRPs, since their finances prevented them from having the right diet and being able to afford doctors’ visits. The cost of therapy has been perceived as being important, particularly with chronic conditions such as CVDs.43 Thus, the value that patients receive from healthcare professionals for their money was unsatisfactory. In fact, doctors’ attitudes towards the patients played an important role in patients being compliant with their regimens.44 This problem was significant in ethnic minorities where a lack of communication between doctors and patients lead to misunderstanding.41 Patients confirmed the need for further information and training, emphasising the importance of getting information from healthcare professionals.
Lifestyle-related factors
Lifestyle factors were perceived as a vital component for the control of conditions (CVDs/DM). Patients felt that they needed to adjust their diet, engage in physical activity and manage their moods to cope with conditions. In relation to diet, they either did not understand the concept of a healthy diet or they had difficulty managing a good diet. Thus, some patients assumed that a healthy diet meant eating less food, eating ‘bitter food’ or eating ‘natural food.’ Other patients overestimated the importance of diet as being more crucial than medicines. This overestimation can be attributed to the fact that the frequency of meals could serve as a reminder to take medicines.43 In addition, patients were aware of the necessity of physical exercise but blamed the weather, work, lack of time and stress for their not exercising.43 Stress was a major factor that patients blamed for not taking medicines on time and for eating a poor diet.
Medicine-related factors
Medicines were recognised by patients as a contributing factor to MRPs with regard to lack of knowledge about medicines, lack of belief that medicines are good, difficulty taking medicines on time and fear of side effects. Patients reported a lack of knowledge about how the medicines worked, called them pharmaceutical toxins and preferred herbal remedies to medicines. This point was emphasised in another study41 that stated that patients’ lack of awareness about the use of their medicines led to MRPs. Furthermore, patients reported skipping medicine doses due to forgetfulness or they did not take their medicines on purpose (at the time of exercise). Forgetfulness in terms of taking medicines was observed more often in patients who did not have regular meals.43 At other times, patients were scared of the side effects and complications of medicines. The medicines’ side effects caused physical discomfort for patients, who started to doubt the therapy's effectiveness and skipped their medicines.43
Condition-related factors
Condition (clinical) factors reported by patients revealed a lack of knowledge about the disease and its cause, a lack of control over the disease and the existence of comorbidities with the disease.43 Patients were accordingly not fully aware of their condition and perceived it in most cases as being a risk factor leading to other diseases. Moreover, they misidentified the causes and complications of their condition. Once the education about the condition was provided, patients felt scared and frustrated, which induced a lack of control over the disease. Moreover, the existence of comorbidities with the main condition worsened the patients’ adherence to treatment and advice.
Strengths and weaknesses of the review
This review proposes a systematic and comprehensive approach to qualitative studies of contributory factors to MRPs of adult patients with CVDs/DM. We adopted a thematic synthesis approach to eligible studies regarding the treatment experiences from patients’ perspectives. The studies involved 836 participants. However, despite the diversity of the participants and different contexts in the studies, we were able to develop themes that indicated an overlap among the studies.
We used recognised methods from the literature regarding patients’ experiences/perspectives in order to synthesise and develop analytical themes.18 ,45 We included the details of each study in relation to the aims, participants, settings and methods applied. We rated the studies’ qualities based on methods from the literature. In this respect, we found that studies with the highest ratings contributed most to the final analytical themes.
One limitation of the review is that it was restricted to the experiences of those patients involved in the studies. Moreover, perspectives and beliefs of non-English speaking patients and those seeking palliative care were not integrated into this review due to lack of studies representing them. Thus, the review was extracted from studies in 12 countries only. Therefore, the generalisability of the findings of this review to patients from different countries (other than the 12 aforementioned countries) may be difficult. However, the analytical themes developed offer a high level of conceptual thinking that can be applied across different contexts.
Implications of the research
This review examined the contribution of patients’ perceptions, behaviours and beliefs in understanding different aspects of underlying risk factors that may lead to MRPs. Syntheses of the qualitative research on such risk factors should complement the findings from quantitative research. Having a systematic review when planning new qualitative research may help to avoid unintentional examination of questions that have already been extensively researched. Finally, the findings of this study on patients’ perspectives could better inform the development of future screening tools and interventions for avoiding MRPs. Additionally, our results may also increase researchers’ knowledge of generic issues in this field, even when attempting to target a specific ethnic or cultural group.
Implication towards practices
Patients’ perspectives about medicine use and factors affecting their treatment regimen are often different from the medical viewpoint. Worldwide, people with CVD and/or DM widely perceive that their conditions are principally stress-related conditions and fear addiction or dependence on medicines, which leads to non-adherence to required treatments. These misconceptions and fears commonly cause people to reduce or stop treatment. If we are to be successful at minimising and preventing MRPs, incorporating patients’ perspectives as well as considering medical records are of paramount concern. An increased understanding between doctors and their patients must play a part in future strategies for reducing MRPs in patients with CVDs and/or DM.
Conclusions
This thematic synthesis of qualitative studies on patients’ perspectives of the potential risk factors of MRPs shows that underlying factors that may lead to MRPs require further in-depth research. Factors influencing patients’ success in treatment included patient-related (socioeconomic and lifestyle), medicine-related (fear of medicine, non-adherence and polypharmacy) and condition-related factors (fear of condition and its complications). In summary, more qualitative research should be conducted on patients with CVDs and/or DM to understand and address issues related to the treatment regimens and to subsequently reduce the cost of undesired hospital admissions resulting from MRPs.
References
Footnotes
Contributors AAH participated in protocol development, literature searching, data extraction, data analysis and manuscript preparation. MG participated in protocol development, data analysis, literature searching, data extraction and manuscript preparation. HA participated in protocol development, data analysis and manuscript preparation. ZA participated in protocol development, literature searching, data extraction and manuscript preparation. All authors have read and approved the final manuscript.
Funding This research received no specific grant from any funding agency in the public, commercial or not-for-profit sectors.
Competing interests None.
Provenance and peer review Not commissioned; externally peer reviewed.
Data sharing statement No additional data are available.