Article Text

Abstract
Objectives This study aimed to assess the efficacy and safety of an integrative complementary and alternative medicine (CAM) approach in the management of lumbar herniated disc (LHD) with sciatic pain and investigate pain relapse, use of medical care and surgery rates in patients who actively chose non-surgical CAM treatment for LHD.
Study design/Setting This prospective observational study was undertaken at a Korean medicine hospital outpatient setting in Korea.
Participants A total of 128 consecutive patients with LHD with a numeric rating scale for leg pain of ≥5 completed 6 months of CAM treatment after recruitment from November 2006, and 73/128 participants (57%) attended follow-up 3 years later.
Interventions 6 months of CAM treatment (herbal medicine, acupuncture, bee venom pharmacopuncture, and Chuna manipulation).
Primary outcome measures Visual analogue scale (VAS) for low back and leg pain, Oswestry Disability Index (ODI), and Short Form (SF)-36 Health Survey.
Secondary outcome measures Neurological impairment (muscular weakness, sensory loss, Straight Leg Raise test), MRIs, recurrence of low back pain and/or radiating pain, and use of medical care.
Results 92 patients could be assessed for surgical state, of whom 4 replied that they had received surgery. 73 patients attended the 3-year follow-up. The baseline VAS of back pain (4.37±2.70) decreased after treatment (0.90±1.01; p<0.001) and was maintained at 3 years (1.12±1.64; p=0.19). The baseline VAS of leg pain (7.57±1.40) also decreased on treatment (0.82±1.18; p<0.001) and was sustained at 3 years (0.99±1.58; p=0.34). ODI scores declined from 40.74±16.15 to 9.84±9.67 (p<0.001), then decreased further to 6.30±7.19 (p<0.01). SF-36 scores increased from 34.96±13.30 to 69.20±14.96 (p<0.001), reaching 76.19±14.45 (p<0.001) at 3 years. 37 patients reported recurrence of pain and most chose CAM treatment for management of relapse symptoms.
Conclusions Although the absence of a control group prevents validation of effectiveness, many patients showed favourable long-term outcomes.
Trial registration number ClinicalTrials.gov Identifier: NCT01989403.
- COMPLEMENTARY MEDICINE
- PAIN MANAGEMENT
This is an Open Access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/
Statistics from Altmetric.com
Strengths and limitations of this study
It is a rigorous cohort observation on complementary and alternative medicine treatment over a period of 3 years.
The high compliance with treatment and low adverse reaction rate (one case of mild allergic reaction to bee venom).
Our findings provide no insight into which intervention(s) have the greatest impact on improvement. The comparative effectiveness of overall treatment and individual treatment modalities cannot be verified because of the integrative treatment modality and observational design.
The low long-term compliance rate (57%) is due to the strict follow-up inclusion criteria.
Introduction
Sciatica associated with lumbar herniated disc (LHD) is the most common cause of sciatica in working populations.1 Based on several randomised controlled trials (RCTs) on patients with LHD with sciatica that report no significant difference in long-term clinical outcomes between surgery versus non-surgery,2 ,3 guidelines generally agree that in the absence of symptoms requiring emergency surgery the first line of treatment should be conservative treatment, yet there is a lack of consensus regarding the type of treatment.4 Recently, conservative approaches for low back pain (LBP) are being evaluated multidimensionally and the options are not limited to conventional treatment but also include complementary and alternative medicine (CAM).5 A 2004 survey by Brunelli and Gorson reported that 43% of patients with peripheral neuropathy used CAM to manage their symptoms and the main reason for seeking CAM was due to the unsatisfactory management of symptoms with standard care.6 Korea has a dual medical system where western and Korean traditional medical doctors (KMDs) have equal individual treatment rights and the patient usually decides the means of primary healthcare. We recruited participants from consecutive outpatients visiting for treatment purposes and administered CAM treatment, excluding conventional treatment (eg, analgesics, physical therapy, injections) and published the 6-month results.7 The participants had severe leg pain, and 60% had previously been diagnosed as needing surgery for LHD at other hospitals or clinics.
The purpose of this study is to evaluate the feasibility of this model of integrative treatment as a valid alternative option for patients with LHD with sciatica and to investigate pain relapse, use of medical care and surgery rates in patients who actively chose non-surgical CAM treatment for LHD. In an attempt to answer this question, we report the 3-year follow-up results of a prospective cohort observational study on CAM treatment.
Methods
Design and ethics statement
LHD patients with a chief complaint of sciatica were recruited at Jaseng Hospital of Korean Medicine, Seoul, Korea, an integrative hospital that offers both western and Korean traditional medical services, from November 2006 to April 2007. A prospective cohort study was conducted and this study is a report of the 3-year follow-up analysis of a previous trial.7 The protocol has been registered at ClinicalTrials.gov under the registration number NCT01989403.8
Participants
The participants were recruited from outpatients who had not previously been treated for LBP at this hospital. The inclusion criteria were: (1) LBP with sciatica, with a numeric rating scale (NRS) leg pain intensity of 5 or higher and onset within 1 year; (2) sciatica due to LHD as confirmed by MRI and neurological examinations; (3) age 18-60 years; (4) written consent to attend 6 months of integrative CAM treatment and following assessment visits.
The exclusion criteria were: (1) other treatment regarding current LBP and/or sciatica (eg, surgery, nerve blocks, analgesic medication); (2) non-spinal or soft tissue problems potentially related to back pain or sciatica (eg, pregnancy, spinal tumour, rheumatoid arthritis); (3) history of spinal surgery, vertebral dislocation or fracture; (4) severe neurological symptoms (eg, cauda equina syndrome). Follow-up sessions were conducted annually through hospital visits on participants who had completed the 6 months of treatment and previous assessments, including MRI, physical examinations and surveys. The interviewer was not given any prior information about a participant before the interview and all participants provided written consent to participate in the study.
Interventions
Participants received integrative CAM treatment for back pain and sciatica. The contents of the treatment package were decided from LHD treatment frequently used in current clinical practice.9 The treatment package included herbal medicine, acupuncture, bee venom pharmacopuncture and Chuna therapy (Korean spinal manipulation). Treatment was conducted once a week for 24 weeks, except herbal medication which was taken twice daily for 24 weeks; (1) Acupuncture: frequently used acupoints (BL23, BL24, BL25, BL31, BL32, BL33, BL34, BL40, BL60, GB30, GV3 and GV4)10 ,11 and the site of pain were selected and the needles were left in situ for 20 min. Sterilised disposable needles (stainless steel, 0.30×40 mm, Dong Bang Acupuncture Co., Korea) were used; (2) Chuna therapy12 ,13: Chuna is a Korean spinal manipulation that includes high-velocity, low-amplitude thrusts to spinal joints slightly beyond the passive range of motion for spinal mobilisation, and manual force to joints within the passive range; (3) Bee venom pharmacopuncture14: 0.5–1 cc of diluted bee venom solution (saline: bee venom ratio, 1000:1) was injected into 4–5 acupoints around the lumbar spine area to a total amount of 1 cc using disposable injection needles (CPL, 1 cc, 26G×1.5 syringe, Shinchang medical Co., Korea); (4) Herbal medicine was taken twice a day in dry powder (2 g) and water extracted decoction form (120 mL) (Ostericum koreanum, Eucommia ulmoides, Acanthopanax sessiliflorus, Achyranthes bidentata, Psoralea corylifolia, Peucedanum japonicum, Cibotium barometz, Lycium chinense, Boschniakia rossica, Cuscuta chinensis and Atractylodes japonica). These herbs were selected from herbs frequently prescribed for LBP (or nerve root pain) treatment in Korean medicine and traditional Chinese medicine,15 and the prescription was further developed through clinical practice at Jaseng Hospital of Korean Medicine.9 In addition, recent investigations report that compounds of C. barometz inhibit osteoclast formation in vitro16 and A. japonica extracts protect osteoblast cells from oxidative stress.17 E. ulmoides has been reported to have osteoclast inhibitive,18 osteoblast-like cell proliferative and bone mineral density enhancing effects.19
Patients were given instructions by their physician at treatment sessions to remain active and continue with daily activities while not aggravating pre-existing symptoms. Also, ample information about the favourable prognosis and encouragement for non-surgical treatment was given.
Outcome measures
All assessments were conducted by trained physicians during visits to the hospital for follow-up purposes. Assessing doctors did not participate in any part of the treatment. The first follow-up period consisted of assessments performed at baseline and at 4, 12, 16, 20 and 24 weeks for the duration of treatment. Further results were obtained through the second follow-up period with annual follow-up visits at 1–3 years.
Outcome measures of back pain and referred pain were assessed using the visual analogue scale (VAS, 0–10),20 Oswestry Disability Index (ODI)21 and Short Form (SF)-36 Health Related Quality of Life Questionnaire.22 ,23 Levels of neurological damage were evaluated through assessments of muscular weakness and sensory loss. A Straight Leg Raise test (SLRT) of 60° or lower in the leg with radiating pain was considered a positive test result. Lumbar range of motion (ROM) was also checked to assess pain occurring within the normal range of motion. MRIs were conducted at baseline, 24 weeks and 1–3 years. Changes in size and severity of the main herniated disc causing radiating pain were evaluated by radiology specialists and KMDs and categorised into three groups (improved, worse or no discernible change) in comparison with the immediate previous MRI to track yearly changes and assess for correlations in subjective clinical symptoms and objective physical evaluation and MRI results. Recurrence of pain and use of medical care (type, frequency) were also investigated.
Statistical analysis
Descriptive analyses were performed using SPSS software for Windows (V.18.0, SPSS Corp., Chicago, Illinois, USA) for all data. Confirmatory analyses of single primary outcomes were not included in this study. Instead, changes from baseline for primary outcome measures were presented as mean differences with a 95% confidence interval (CI). The paired t test was conducted to assess whether the 24-week outcome results were sustained after completion of treatment.
Results
A total of 4184 LBP and patients with leg pain were screened and 150 eligible patients were enrolled in the study and started treatment. 128 patients completed the 6 months of treatment and first follow-up. Twenty-two patients discontinued treatment and participation due to surgery or personal reasons.
The mean duration of treatment for the 22 patients who prematurely terminated treatment was 6.91±4.59 weeks. Of these patients, eight underwent lumbar operations at an average of 6.75±4.30 weeks after participating in the study. The remaining 128 patients who completed treatment did not receive any treatment other than that assigned in the protocol and were followed up annually, while 73 patients completed the 2nd follow-up period to 3 years postbaseline. The participants’ demographic characteristics and medical history were assessed at baseline (table 1).
Patient characteristics at baseline
The authors lost contact with most of the 55 patients who failed to attend the 3-year follow-up. The main reason for failure to attend the 3-year follow-up was loss of contact (n=36) and other personal reasons (figure 1).
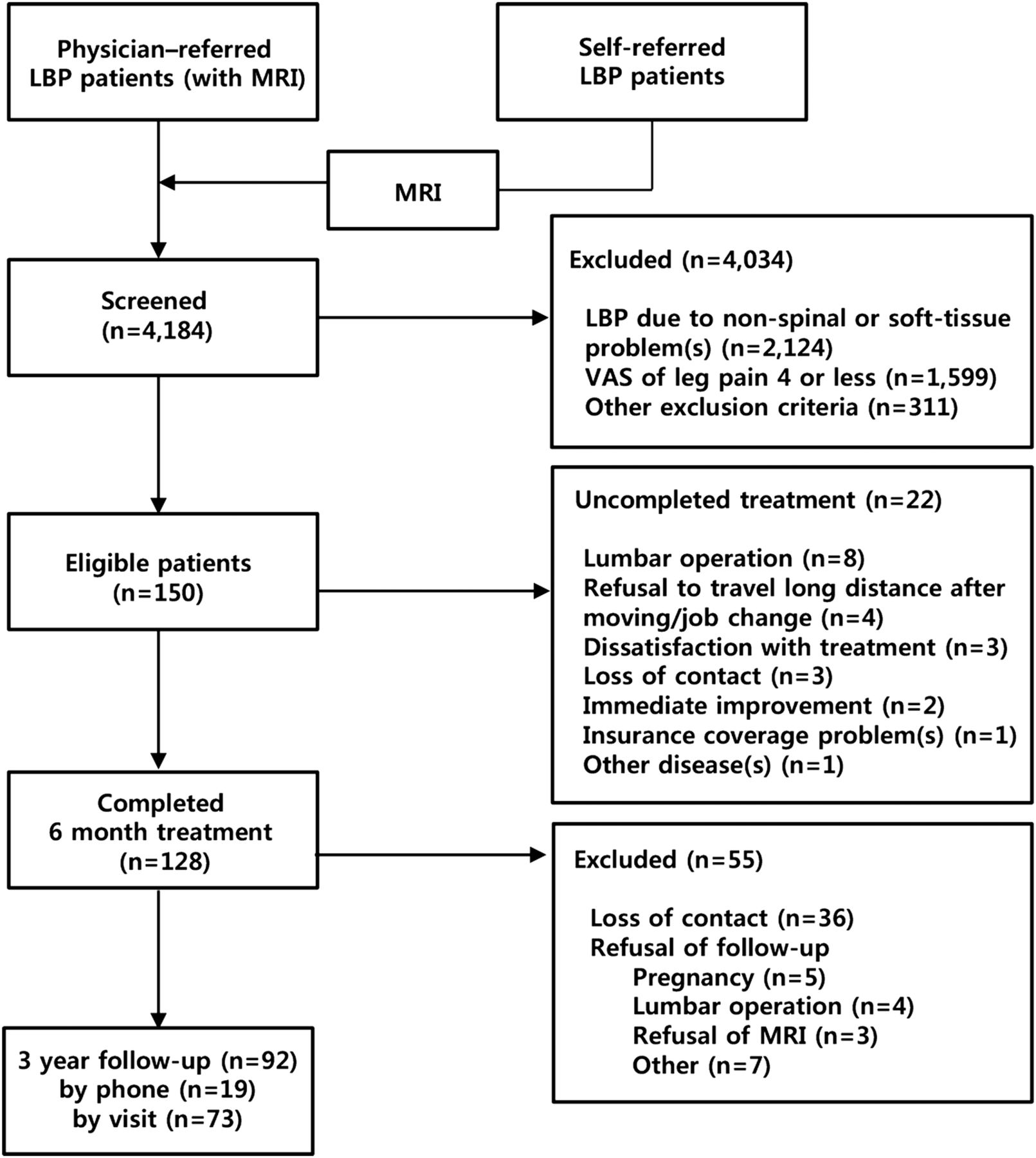
Flow diagram of study (LBP, low back pain; VAS, visual analogue scale).
We compared the outcomes (VAS, ODI, SF-36 scores) of each follow-up with the immediate previous evaluation over the second follow-up period. The pain intensity of LBP in the 73 patients showed a steady and significant decrease up to 1 year, which increased slightly at the 3-year follow-up. Pain intensity for sciatica showed a stable and significant decrease up to 24 weeks, but no significant change was observed from 1 to 3 years. ODI and SF-36 scores decreased significantly up to 1 year and showed no significant change at 3 years. Differences in VAS for LBP, leg pain and ODI scores from baseline were maintained above the minimal clinically important difference (MCID) at 1, 2 and 3 years (table 2).
Change in pain, functional status and quality of life at 3 years from baseline
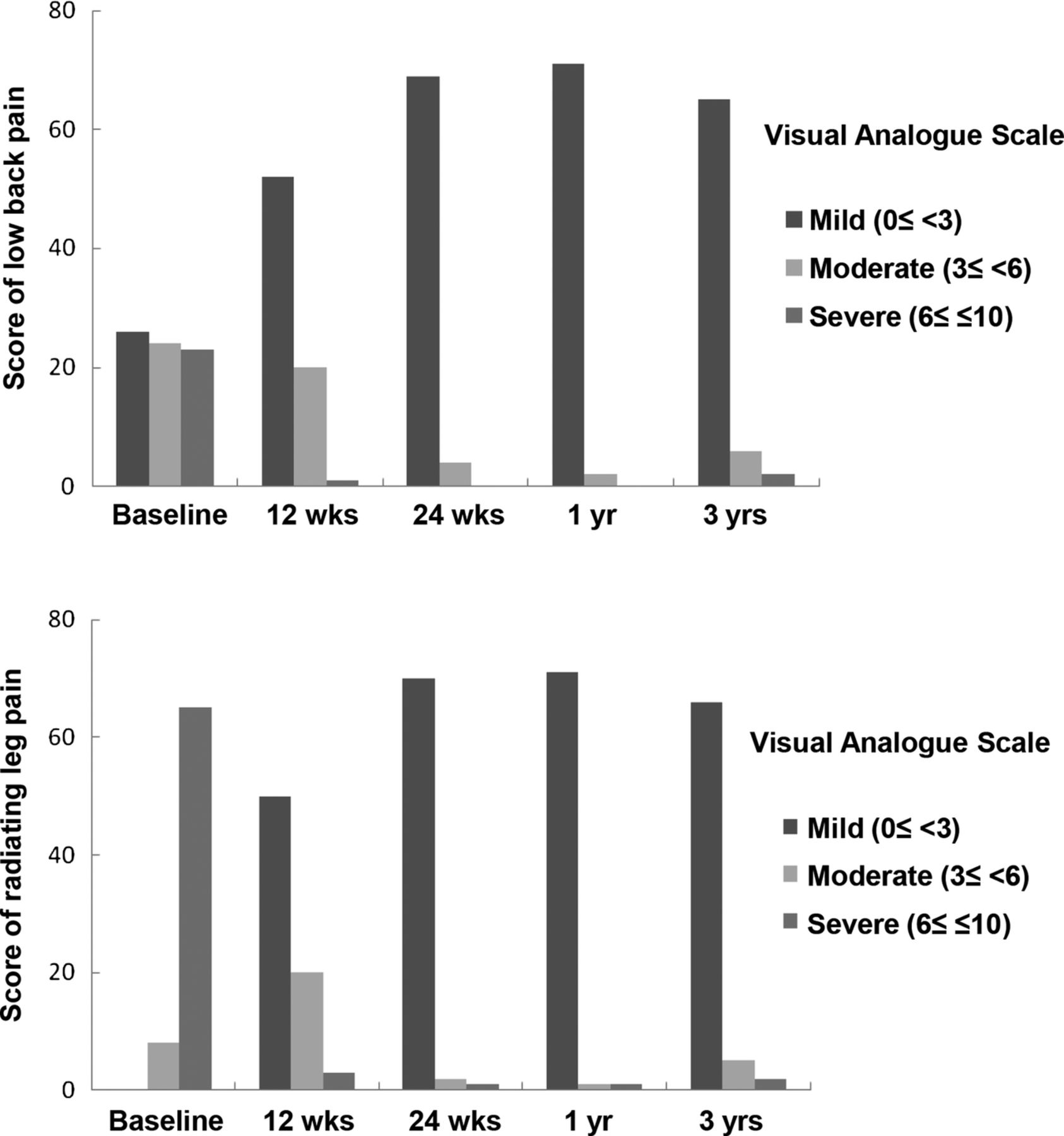
For LBP at 3 years, 65 patients (89%) reported almost no or mild pain (VAS<3), 6 (8%) reported moderate (3≤VAS<6) and 2 (3%) reported severe pain (6≤VAS≤10). For sciatica, 66 patients (90%) had almost no or mild pain (VAS<3), 5 (7%) had moderate (3≤VAS<6) pain and 2 (3%) had severe pain. In ODI scores, 58 patients (79%) could be considered as having had almost no difficulty with daily life (ODI<10), 15 (21%) as having had mild functional disability (10≤ODI<30) and none as having had severe functional disability (ODI≥30). In SF-36 scores, 35 patients (48%) reported scores of 80–100, 26 (36%) reported scores of 60–80 and 12 (16%) reported scores of 30–60 (figure 2).

{kind=link}
{kind=link}
Distribution of pain classified by pain severity over time.
Observations of change in size of the main herniated disc by MRI at baseline, 24 weeks and 1–3 years revealed temperamental changes with many cases showing fluctuations in volume. Of the patients who displayed abnormality in neurological and physical examinations, most recovered to normal range in muscular weakness, sensory loss, SLRT and lumbar ROM by week 24 (table 3).
Changes in the physical examination findings and herniated disc as assessed by MRI up to 3 years
Twenty-seven (37%) of 73 patients reported having sought medical care for recurrence of LBP and/or sciatica at 3 years, of which 23 patients (85%) continued with CAM and the rest opted for conservative treatment such as medication, physical therapy, exercise or nerve block injection (table 4).
Use of healthcare service by 27 patients with low back pain and/or sciatica recurrence (after the pre-defined 6 months of treatment) at 3 years
Ninety-two of 128 patients answered whether they had undergone surgery at 3 years and only 4 patients (4%) reported having received surgical operations.
Discussion
Patients with sciatica due to LHD reported improvement in leg pain and ODI scores above MCID from week 8 during the 24 weeks of CAM treatment. Clinically significant improvements in LBP also became apparent and most patients no longer presented neurological disorders from week 24. We found moderate time by group interaction difference in VAS for LBP and ODI scores in subgrouping by duration of LBP and significant time by group interactions in VAS for LBP when subgrouped by operation recommendation.7 In additional investigations over 3 years, patients showed further improvement or maintained their improved state. Cases with continuous neurological disability were few.
In cases of recurrent pain, most patients (23 of 27 patients, 85%) reselected CAM therapy and only a few cases sought conventional treatments. Thirty-six of 73 patients reported minimal levels of pain intensity and functional disability that did not require further treatment at the 3-year follow-up. The fact that a high percentage returned to CAM suggests a high satisfaction rate and these results imply that CAM could be considered an effective treatment option for patients with LHD neurological symptoms.
One of the major strengths of our study is that it is a rigorous cohort observation on CAM treatment over a period of 3 years. All participants underwent multidimensional pain and functional ability assessments including MRI and physical examinations.
The combined approach of integrative treatment is similar to real-world settings and the collected data can be highly informative to clinicians as examinations and treatment were performed under circumstances comparable to typical Korean medicine clinics. During the 24 weeks of treatment, patients were subjected to an intense regimen of integrative treatment, but the high compliance rate of 85.3% (128 of 150) indicates that patients were highly satisfied with the treatment. Additionally, the fact that no side effects other than a mild allergic reaction to bee venom occurred is noteworthy.
Previous long-term follow-ups of studies focusing on neurological injury due to intervertebral disc displacement are mainly comparisons of the effects of surgical versus non-surgical treatment. Leiden-The Hague Spine Intervention Prognostic Study Group compared early surgery versus prolonged conservative care given by family practitioners, with conservative care consisting mainly of counselling, guidance from a physiotherapist and prescription of painkillers.2 The long-term follow-up results at 1 and 2 years showed no significant difference between the two groups in leg pain and lumbar function. However, 46% of the patients allocated to the non-surgical group received surgery and the results were intention-to-treat analysed. As-treated analysis was performed in the Spine Patient Outcomes Research Trial study and the long-term follow-up results at 1 and 2 years all showed superior results in SF-36 bodily pain and physical function scales in the surgery group compared to non-operative care (active physical therapy, counselling and education with home exercise instructions and prescription of non-steroidal anti-inflammatory drugs).25
In studies comparing conventional non-surgical treatment (eg, education, rest, pain medication, physical therapy, etc) and CAM non-surgical treatment (eg, hot compress using Chinese medicine, electroacupuncture, Chinese herbal injection, Chinese tuina, etc), CAM treatment showed better results in lumbar functional scores at 6 months’ short-term follow-up.
A systematic review on the effectiveness of conservative treatments for lumbosacral radicular syndrome evaluated injections, traction, physical therapy, bed rest, manipulation, medication and acupuncture, deducing that corticosteroid injections and traction did not have sufficient evidence to be recommended as treatment options and that it was difficult to reach a conclusion whether the other treatments should be prescribed by clinicians or whether a certain type of treatment is superior to others.26
A recent review of eight studies on the efficacy of Chinese herbal medicine for lumbar disc herniation compared with conventional treatment analysed the results of 5 studies reporting that Chinese herbal medicine was better than conventional medicine and two studies stating that clinical outcomes were better in Chinese herbal medicine groups than in physiotherapy and placebo groups.27 However, all trials were of poor methodological quality.
There are also weaknesses and limitations in our study. One particular limitation is due to the innate nature of a prospective cohort study where we cannot draw any definite conclusions regarding treatment efficacy. Owing to the lack of a control group, we are unable to conclusively comment on the effectiveness of individual treatments or on the comparative effectiveness of this integrative package to conventional treatment modalities.
Perhaps the most significant limitation is the low long-term compliance rate. The 3-year follow-up was conducted only on patients who had completed the 24 weeks of treatment and the 1 and 2-year follow-up sessions, leaving 73 of the original 128 participants (57%) who initially completed treatment. The study design was conceived with the aim of comparing the patient's state each year with that in the previous year to track changes multidimensionally and the reason for the increasing loss of follow-up may be partly explained by the strict follow-up inclusion criteria. MRI and assessments of neurological and physical function required regular visits to the hospital as they could not be replaced with phone interviews or online assessments. A large proportion of the study population refused further participation in the study due to personal reasons; some no longer required treatment, while others refused to travel long distances after moving.
We lost track of many patients in the course of this study and this may be due in part to the rapidly changing communications industry in Korea. Many Koreans are replacing home phones with internet or personal mobile phones and frequently changing personal contact information. Also, while there was an increasing loss of follow-up patients, it cannot be decisively said that the patients who did not attend the 3-year follow-up were necessarily in worse medical states. As seen in table 1, the baseline characteristics of dropout patients did not differ greatly from follow-up patients and as we had made it known to the participants prior to follow-up that all MRIs and tests were free of charge, it is possible that patients in worse medical conditions were more committed to the yearly check-ups.
The results of a meta-analysis on the effectiveness of integrative Chinese medical therapies including tuina on the patients with LBP showed that groups receiving tuina with Chinese herbal medicine and tuina with acupuncture showed better pain and functional status than groups receiving tuina alone.28 Our results also reflect the discussions of CAM clinicians on selecting effective treatment methods for disc herniation patients and the outcome of those consultations was an integrative treatment package consisting of herbal medicine, acupuncture, bee venom pharmacopuncture and Chuna manipulation. The reason for this multimodality approach is that each approach has different targets, effects, mechanisms and time-windows and no single therapy is clearly superior to others or unequivocally successful.
Although integrative treatment may be considered pragmatic, this leads to another limitation. A combined approach makes it difficult to discern the level of contribution of individual factors. Current clinical guidelines29 ,30 suggest that the composition of integrative treatment should be based on a coherent theoretical basis and evidence-based effectiveness. However, the present study treatment was pre-decided through clinical experience and preferential consensus of KMDs. Therefore, this study requires further consideration of such factors as evidence-based effectiveness and cost-effectiveness in treatment construction for a more organised gradient intervention.
These limitations notwithstanding, the study results show that the patients with herniated disc included in the present study were able to control their symptoms using only CAM without the help of conventional treatments31 ,32 during the treatment period. Only a few people reported the need for conventional treatment at the second follow-up also.
This study is one of the few studies and only study conducted in Korea, to evaluate the effects of CAM treatment in patients with LHD with sciatica multidimensionally using standardised imaging and examinations. In the current study, integrative treatments were proven safe and brought about improvement in pain, functional disability, quality of life and neurological disorders. Further investigations and RCTs are required to assess the comparative benefits of integrative CAM treatment to contemporary conventional medicine.
References
Footnotes
Contributors IHH drafted the study and MRK and IHH wrote the final manuscript. JSS, JHL, BCS and MSL contributed to the study design and made critical revisions. All authors have read and approved the final manuscript.
Funding This research received no specific grant from any funding agency in the public, commercial or not-for-profit sectors.
Competing interests None.
Ethics approval The study protocol was approved by the Institutional Review Board of Jaseng Hospital of Korean Medicine.
Provenance and peer review Not commissioned; externally peer reviewed.
Data sharing statement No additional data are available.