Article Text

Abstract
Objectives Biological therapy represents important advances in alleviating rheumatoid arthritis (RA), but the effect on interstitial lung disease (ILD) has been controversial. The objective of this study was to assess the risk of such treatment for patients with ILD.
Design Case–control cohorts.
Setting Single centre in Japan.
Participants This study included 163 patients with RA who underwent biological therapy.
Outcome measured We assessed chest CT before initiation of biological therapy and grouped 163 patients according to the presence of ILD (with (n=58) and without pre-existing ILD (n=105)). Next, we evaluated serial changes of chest CT after treatment and visually assessed the emergence of ILD or its progression, which was referred to as an ‘ILD event’. Then, we also classified the patients according to the presence of ILD events and analysed their characteristics.
Results Tumour necrosis factor (TNF) inhibitors were administered to more patients with ILD events than those without ILD events (88% vs 60%, p<0.05), but recipients of tocilizumab or abatacept did not differ in this respect. Of 58 patients with pre-existing ILD, 14 had ILD events, and that proportion was greater than for those without pre-existing ILD (24% vs 3%, p<0.001). Of these 14 patients, all were treated with TNF inhibitors. Four patients developed generalised lung disease and two died from ILD progression. Baseline levels of KL-6 were similar in both groups, but increased in patients with ILD events.
Conclusions TNF inhibitors have the potential risk of ILD events, particularly for patients with pre-existing ILD, and KL-6 is a valuable surrogate marker for detecting ILD events. Our data suggest that non-TNF inhibitors are a better treatment option for these patients.
- Tumor necrosis factor inhibitors
- Rheumatoid arthritis
This is an Open Access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/
Statistics from Altmetric.com
Strengths and limitations of this study
-
Our study demonstrated the potential risk that tumour necrosis factor (TNF) inhibitors can exacerbate entrenched interstitial lung disease (ILD) and the use of non-TNF inhibitors seem to be favourable options for benefitting patients with ILD.
-
Since this study is a retrospective, we could not exclude the possibility of interaction with other agents.
-
Our data also suggest that KL-6 is a valuable surrogate marker for detecting ILD events.
Introduction
Rheumatoid arthritis (RA) is a generally progressive, systemic autoimmune process characterised by chronic erosive synovitis. Interstitial lung disease (ILD) is a common extra-articular manifestation of RA and is substantially more likely to cause morbidity and mortality.1 Recently, as the understanding of RA pathogenesis has advanced, clinical outcomes have improved greatly, particularly with the development of disease-modifying antirheumatic drugs and numerous biological therapies.2 Yet some of these agents have been reported to increase the risk of such lung infections as pneumocystis pneumonia and mycobacterial disease and have been associated with the progression of preclinical ILD and drug-induced lung toxicity.3–6 Therefore, since the optimal treatment for RA-ILD has not been determined, our usual treatment regimen is directed to the underlying type of interstitial pneumonia, whether that pattern is diagnosed by lung biopsy or presumed based on clinical presentation and findings of CT.7 ,8
Biological therapy represents an important advance in alleviating RA as a means of lessening symptoms, joint destruction and possibly lung disease in these patients.9 ,10 One therapeutic option has been the biological preparation, tumour necrosis factor (TNF) inhibitor, used despite the acknowledged risk of reactivating latent tuberculosis infection.11 Meanwhile, postmarketing surveillance revealed that the development of ILD after administration of TNF inhibitor was a rare event (0.5–0.6%).12 ,13 However, as recently reported, patients with RA developed a progressive and usual interstitial pneumonia or acute interstitial pneumonitis after receiving infliximab or etanercept, and some patients died from progressive ILD.14–16 Furthermore, the presence of pre-existing ILD at the initiation of TNF inhibitors was declared a risk factor for ILD exacerbation.17 ,18 In addition, a case of ILD exacerbation after treatment with tocilizumab, an anti-IL-6 receptor antibody, has also been reported.19 Considering these previous reports, the usefulness of biological therapy for ILD in patients with RA has been controversial. Hence, to assess the risk of ILD exacerbation after administration of biological therapy, we conducted a retrospective analysis of patients with RA at a major Japanese medical institution.
Methods
Patient population and study design
For this retrospective review, we surveyed all patients who were diagnosed with RA in the Department of Rheumatology at Kameda Medical Center (Chiba, Japan), a 1000-bed tertiary care centre, from April 2006 to March 2012. We identified 163 patients with RA who received biological therapy, all of whom had previously undergone chest CT for screening of ILD and infections. Since the majority of pulmonary events have been reported to have occurred within 1 year after initiation of biological therapy,17 ,18 we established 1 year as a reasonable follow-up period for this study. To assess the emergence and progression of ILD, we excluded patients who lacked imaging data, who discontinued biological therapy due to infections or extrapulmonary adverse events within 1 year, or whose follow-up period was not verified as longer than 1 year. RA was diagnosed by rheumatologists on the basis of clinical symptoms, physical history and laboratory findings. The presence of ILD was confirmed by two pulmonologists and one radiologist. To assess the patients’ clinical characteristics and treatment, we grouped them according to the presence of ILD (with (n=58) and without pre-existing ILD (n=105)) and then compared their backgrounds.
Since many forms of toxicity and infection are induced in the lungs of patients given agents to treat RA, we routinely perform chest CT for detecting latent infection and ILD before initiation of biological therapy and take chest X-rays (CXR) every 3–6 months after its treatment. We reassess chest CT if a new lesion is detected on CXR or a patient reports respiratory symptoms for more than 2 weeks. For this study, the severity of ILD was visually assessed on chest CT images and classified for its vertical extent referring to the previous established method20: grade 0, ILD not determined; grade 1, ILD extended less than one-third; grade 2, extended more than one-third but less than two-thirds; and grade 3, extended more than two-thirds (figure 1). Serial changes of these scores were also evaluated by two pulmonologists and one radiologist, and ‘ILD events’ were defined as ‘worse than pretreatment status.’ Furthermore, to categorise the gravity of ILD events, we defined them as: ‘mild,’ ILD worsened but persisting in the same grade; ‘moderate,’ ILD increased 1 grade, for example, from level 0 to 1; and ‘severe,’ ILD grade increased by 2 levels. All clinical information was obtained from medical records. This retrospective and observational study was approved by the ethics committee of our institution.

Assessment of interstitial lung disease (ILD) on chest X-ray (CXR) and CT. The existence and severity of ILD was visually assessed on CXR and CT images.20 The extent of ILD was evaluated and classified as follows: grade 0, no ILD found on CT scan; grade 1, signs of ILD vertically extended less than one-third (A); grade 2, ILD vertically extended less than two-thirds but more than one-third (B); and grade 3, ILD vertically extended more than two-thirds (C).
Statistical analyses
We used the χ2 test, paired t-test or Mann-Whitney test, as appropriate, to compare the two groups of patients. These analyses were performed with SPSS V.21. Data were expressed as means with SDs. For all statistical analyses, a p value less than 0.05 was considered significant.
Results
Baseline characteristics
The patients’ baseline characteristics are shown in table 1. The mean age of this group, of whom 72% were female, was 60.9 years (±11.6 years), and the mean disease duration was 10.2 years (±11.0 years). The mean stage and class of RA were 2.4 (±1.1) and 2.1 (±0.5), respectively. Of 163 patients, 102 (63%) were given TNF inhibitors (6 received adalimumab, 63—etanercept and 33—infliximab). Meanwhile, of the 51 given non-TNF inhibitors, 36 (22%) received an anti-IL-6 receptor antibody (tocilizumab), and 25 (15%) had cytotoxic T-lymphocyte antigen 4-immunoglobulin (CTLA4-Ig; abatacept). Analysis of CT scans determined the presence of ILD in 58 patients (36%) at the initiation of biological therapy; in terms of the severity of ILD, 30 (52%) patients were classed in grade 1, 22 (38%) in grade 2 and 6 (10%) in grade 3. ILD events were detected in 17 patients (10%); 10 (6%) of whom had mild, 6 (4%) moderate and 1 (1%) severe progression. Two patients eventually died of ILD events.
Baseline characteristics of patients with and without pre-existing ILD
Comparisons of baseline characteristics between patients with (n=58) and without (n=105) pre-existing ILD are also shown in table 1. Patients with pre-existing ILD were older (66.1 vs 57.8 years, p<0.001), had a higher class of RA (2.3 vs 2.0, p<0.001) and had a greater proportion of male (45% vs 18%, p<0.001) and patients who were treated with TNF inhibitors (79% vs 53%, p<0.01) than those without pre-existing ILD. The duration of RA and proportion of patients who were treated with tocilizumab were similar in both groups. Of 58 patients with pre-existing ILD, ILD events were determined in 14 patients, a higher prevalence than in patients without pre-existing ILD (24% vs 3%, p<0.001). These results revealed that pre-existing ILD at the initiation of biological therapy was a risk factor for the subsequent exacerbation of ILD and resembled that statistic in previous reports.17 ,18 Accordingly, although the number of patients included in our analysis was small, the results assured that our data were valuable for more detailed analysis.
Comparison of patients with and without ILD events
The baseline characteristics of patients with and without ILD events are shown in table 2. Mean age, gender and stage/class of RA were not statistically different between the two groups. The proportion of patients with pre-existing ILD was higher in patients with later ILD events than in patients without ILD events (82% vs 30%, p<0.001). Additionally, more patients with ILD events received biological therapy with a TNF inhibitor than those without ILD events (88% vs 60%, p<0.05). The proportion of patients given tocilizumab (12% vs 23%, p=0.367) or abatacept (0% vs 17%, p=0.077) did not differ to a statistically significant extent between the ILD event-positive and event-negative groups.
Comparison between patients with and without ILD events
Characterisation of ILD events in patients with pre-existing ILD
On the basis of these results, patients with RA with pre-existing ILD had a higher risk of post-treatment ILD events than those without pre-existing ILD. Accordingly, to assess the risk factors for the former group, we next examined their clinical history.
A comparison between patients with and without pre-existing ILD who suffered post-therapy ILD events appears in table 3. Mean age, gender, stage/class of RA, RA and ILD-related data (rheumatoid factor and KL-6 in blood, and ILD grade) and baseline doses of prednisolone and methotrexate (MTX) did not differ at the level of statistical significance between patients with and without post-therapy ILD events. Notably, more patients with ILD events had been treated with bucillamine (measured at baseline) than those without ILD events (29% vs 2%, p<0.01), although the number of patients treated with bucillamine was very small. All patients with ILD events had been treated with TNF inhibitors, especially during the administration of infliximab, and this study group included more individuals than the group without ILD events (TNF inhibitor usage 100% vs 73%, p<0.05; infliximab usage 36% vs 7%, p<0.05). Other agents such as tocilizumab and abatacept produced a similar risk of ILD events.
Comparison of patients with pre-existing ILD with and without later ILD events
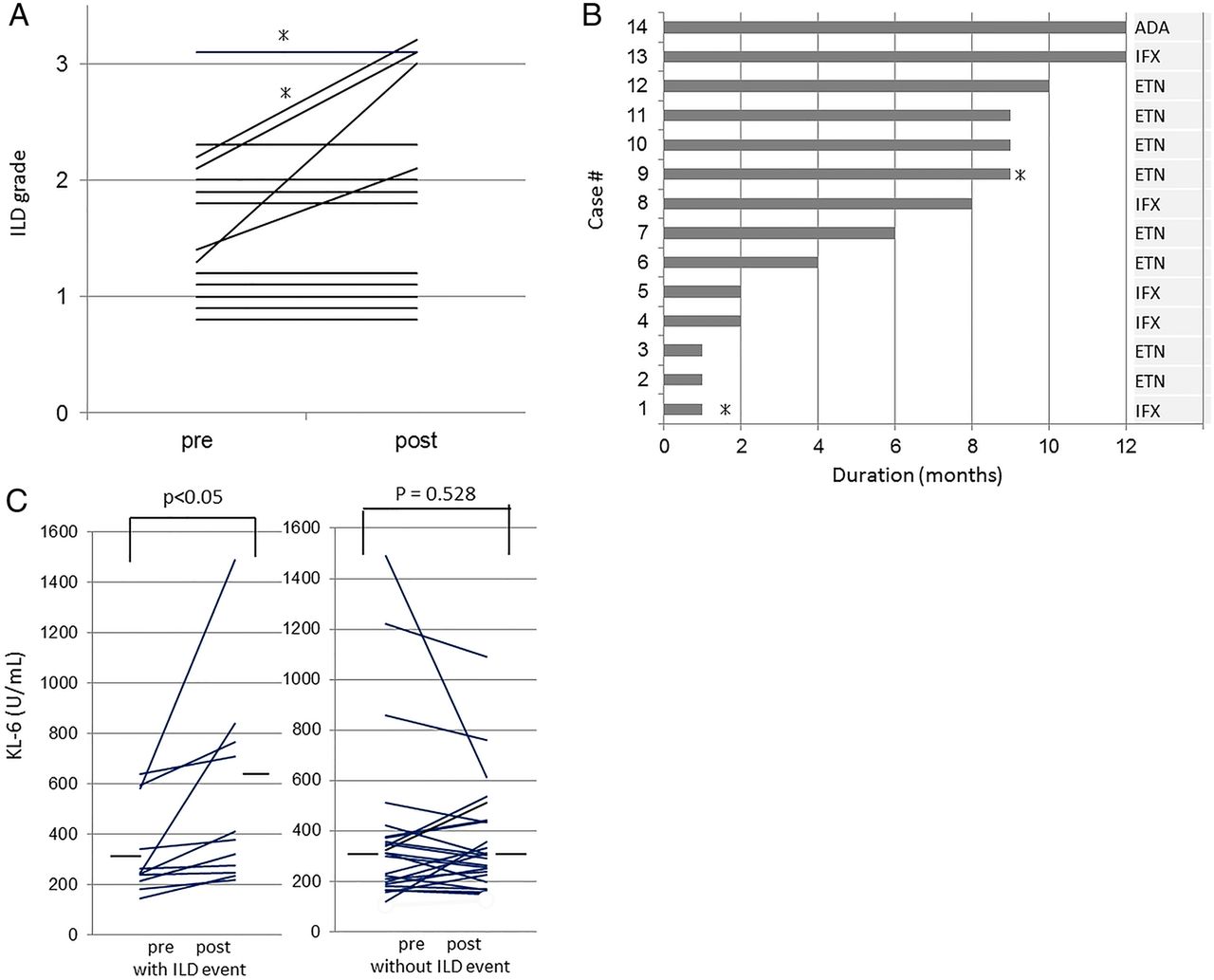
Of the 14 patients with post-therapy ILD events, 4 had exacerbations of their pulmonary disease, as noted on CT scans, to the degree that all lung tissues were involved (severity grade 3). A total of nine patients discontinued TNF inhibitors, and/or ILD treatment including prednisolone was started, but two of these patients died from ILD events (figure 2A). Meanwhile, we had carefully observed five other patients who had mild progression with continuing TNF inhibitors, but further progression of ILD was not detected. As for the period between the initiation of TNF inhibitor treatment and the detection of ILD events, five patients (36%) were diagnosed within 2 months, and a total of seven patients (50%) had an ILD event within 6 months (figure 2B).

Interstitial lung disease (ILD) events in patients with pre-existing ILD. (A) Of 58 patients assessed, 14 had pre-existing ILD (24%) and had ILD events within 1 year after the initiation of biological therapy. Ten patients had mild progression of ILD (in the same ILD grade), six had moderate progression (grade 1–2 or grade 2–3) and one had a severe progression (grade 1–3). Four patients had exacerbated ILD visible on CT scans involving all lung tissues (severity grade 3), and two of such patients died from ILD events (asterisks). (B) All patients were treated with tumour necrosis factor inhibitors; abatacept (ADA) in one patient, etanercept (ETN) in eight patients and infliximab (IFX) in five patients. ILD events were detected in five patients (36%) within 2 months and a total of seven patients within 6 months. Two patients who were treated with ETN or IFX died from ILD events (asterisks). (C) Baseline levels of KL-6 were not statistically significantly different for patients with and without ILD events (339±172 vs 388±347 U/mL, p=0.951). KL-6 levels were higher in patients with ILD events (339±172 vs 29±372 U/mL, p<0.05), but not in the absence of an ILD event (388±347 vs 360±226 U/mL, p=0.528).
As figure 2C illustrates, baseline levels of KL-6 were not statistically significantly different between patients with and without ILD events, but those levels increased in the former patient group at the time of ILD events (339±172 vs 529±372 U/mL, p<0.05).
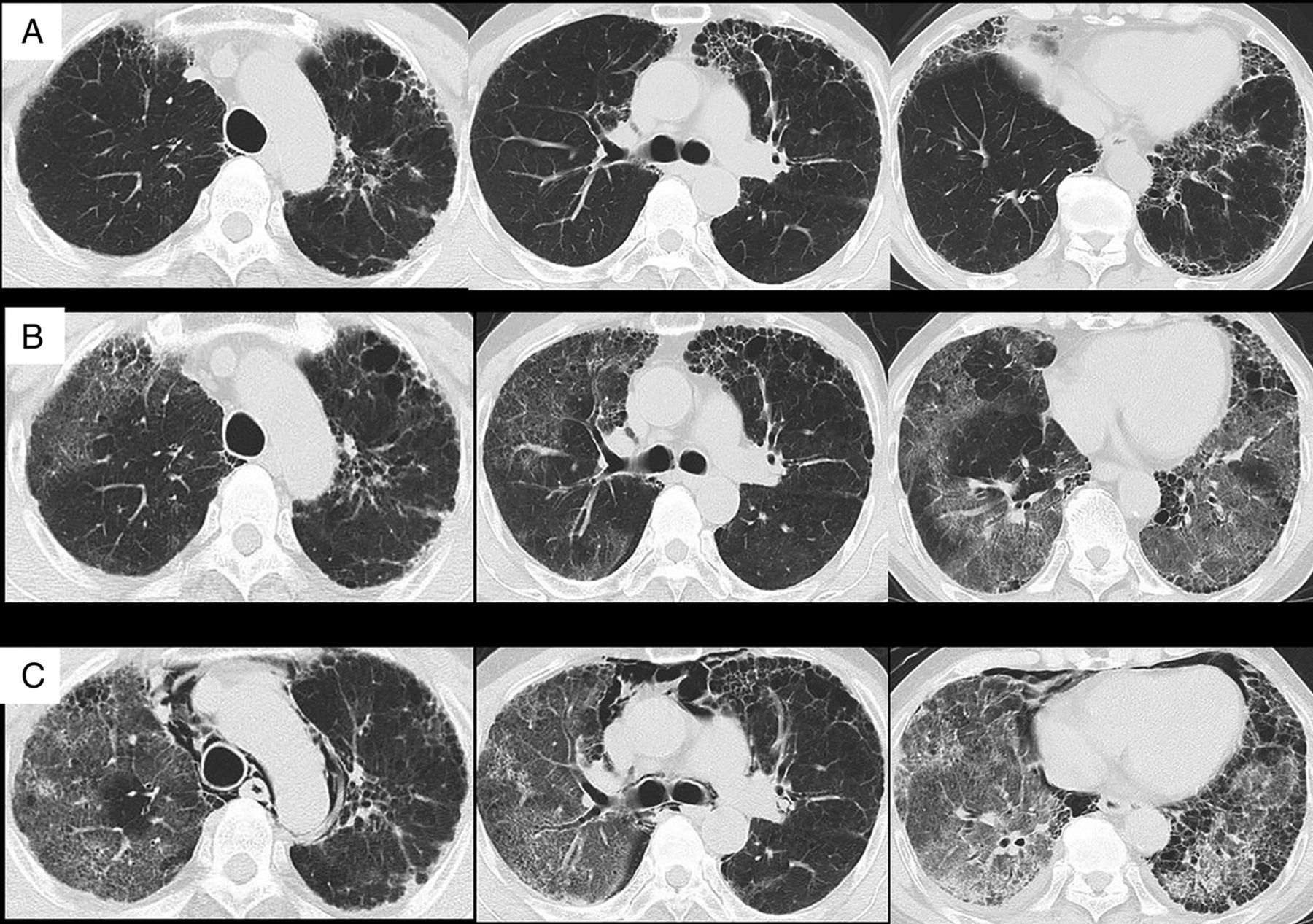
A representative clinical course of ILD events after initiation of TNF inhibitor is briefly described here. The patient was a 73-year-old man with RA (stage II, class 2) who had received 8–20 mg/day of prednisolone and bucillamine. Ciclosporin A was added to ameliorate RA-related symptoms, but the disease activity did not decrease. Although he manifested ILD, we decided to administer etanercept, 25 mg, once a week (figure 3A). After this treatment, his RA-related symptoms dramatically diminished and the disease activity stabilised. However, 9 months after the initiation of etanercept, he presented with a 2-week period of dry cough and shortness of breath. A CXR and chest CT revealed the typical diffuse ground glass opacities of this condition (figure 3B). However, there was no evidence of bacterial, pneumocystis or viral infections. Accordingly, we considered a differential diagnosis of ILD acute exacerbation and drug-induced pneumonitis. Since his hypoxia was rapidly progressive, we started intravenous methylprednisolone and cyclophosphamide pulse therapy and oral ciclosporin A in addition to antibiotics and cotrimoxazole. However, his condition and CT findings worsened, and he died 2 weeks after the detection of ILD events (figure 3C).

{kind=link}
{kind=link}
{kind=link}
Radiological findings for a patient with representative progressive interstitial lung disease (ILD) events after initiation of etanercept therapy. This patient's chest CT images (A) at the initiation of etanercept therapy showing ground glass opacity and traction bronchiectasis predominantly in bilateral lower lobes. Nine months after initiation of this treatment, he developed a 2-week period of dry cough and shortness of breath. A chest CT (B) revealing the ground glass opacities extending throughout the whole lung. Based on the treatment guideline of tumour necrosis factor-alpha inhibitors for rheumatoid arthritis,29 we diagnosed ILD acute exacerbation or drug-induced pneumonitis and started intravenous methylprednisolone and cyclophosphamide pulse therapy, and oral ciclosporin A. Although pneumomediastinum appeared 1 week after the introduction of these agents, it was stabilised without surgery. However, the patient's declining condition and ILD (C) caused his death 2 weeks after the ILD events occurred.
Discussion
This retrospective evaluation of patients who were treated with biologicals clearly demonstrated the potential risk that TNF inhibitors can exacerbate entrenched ILD. We found that (1) 14 of 58 patients with RA with pre-existing ILD (24.1%) had subsequent ILD events, denoting a related response to the administration of TNF inhibitors. This number represents a greater prevalence than previously reported (0.5–0.6%).12 ,13 (2) Of ILD events in patients without pre-existing ILD, 3% (3/105) had this adverse effect, which is still higher than that previously reported from the data of postmarketing surveillance.12 ,13 (3) Non-TNF inhibitors, such as tocilizumab and abatacept, did not increase the prevalence of ILD events, and (4) KL-6 levels were increased in patients with ILD events, but not in those without an ILD event. This is, to our knowledge, the first report of a comparison of TNF-α inhibitors and non-TNF inhibitors for their impact on ILD, particularly in patients with pre-existing ILD. Our data indicate that TNF inhibitors have the potential risk of ILD progression in patients with RA, especially those with pre-existing ILD, and that assessment of KL-6 provides the detection of these events.
TNF is a pleiotropic cytokine, beneficially as well as detrimentally involved in inflammatory and immunological responses and functions in cellular differentiation, proliferation and death.21 Since the overproduction of TNF is known to play a role in not only RA but also inflammatory bowel diseases as well as psoriasis vulgaris, etc, TNF inhibitors are currently used to moderate these diseases. Recently, increased levels of TNF have been linked with idiopathic pulmonary fibrosis (IPF), and current studies using animal models revealed that TNF antagonists may be a promising agent for its treatment.21–23 However, in a previous placebo-controlled clinical trial for patients with IPF, etanercept did not improve their clinical outcomes.24 Meanwhile, TNF, which also possesses antifibrotic ability, suppressed the expression of matrix genes and the ability of TGF-β to induce collagen and connective tissue growth factor.25 Furthermore, patients with RA receive many disease-modifying antirheumatic drugs; among such agents, MTX induces pneumonitis and can worsen RA-related pre-existing ILD of unknown aetiology, and bucillamine generates the synthesis of vascular endothelial growth, which was reported to be associated with the pathogenesis of IPF and to mediate the activation of tyrosine kinase.26–28 In our retrospective analysis of patients with RA with pre-existing ILD, we found that similar prednisolone and MTX doses were given to patients with and without ILD events, but bucillamine was more frequently used in the patients with ILD events. Therefore, our data and previous reports suggest that one of the mechanisms of ILD exacerbation after initiation of TNF-α inhibitors is considered to be caused by the interaction of cytokine responses of these agents. Further studies to detect the changes of numerous cytokine concentrations in bronchoalveolar lavage fluid and serum after therapy with biologicals will be likely to expose the underlying mechanism of ILD events.
Our survey of biological therapy for RA also revealed that pre-existing ILD is a probable risk factor in the onset of further ILD events. This result resembles those in previous cohorts of patients treated with disease-modifying antirheumatic drugs or biological therapies.17 ,18 ,26 In another retrospective review of 24 patients with ILD events after the initiation of TNF inhibitors, 10 patients (42%) died of ILD progression, and the mortality rate was extremely high in patients with pre-existing ILD (62%).18 Elsewhere, in 122 patients with RA with ILD events, the mortality rate for ILD progression was high (29%), and additional risk factors included advanced age (>65 years), late onset, administration of immunosuppressants and pre-existing ILD.17 On the other hand, a recent meta-analysis of ILD events in patients with RA revealed that leflunomide and tocilizumab may cause ILD progression to the same extent as MTX and TNF inhibitors do,26 but in our hands, the proportion of tocilizumab recipients with progressive disease was no different between patients with and without post-therapy ILD events. However, we expect to re-evaluate the effect of tocilizumab and abatacept on ILD progression in a larger population. Additionally, our data indicated that patients’ KL-6 content increased above the baseline during ILD events. Hence, this pneumonitis indicator is considered to be a valuable surrogate marker for signalling ILD events in patients with pre-existing ILD.
This study had some limitations. First, the participants were located at a single centre, and the number included was relatively small. However, similar results from previous studies strongly reinforce our conclusion that TNF inhibitors constitute a risk factor for inciting ILD events.17 ,18 Hence, our comparison of TNF inhibitors and non-TNF inhibitors, and the detailed analysis of relevant characteristics assure the veracity of our data. Second, because this was a retrospective analysis, we could not verify or evaluate such important data as pulmonary function and pathological features of ILD. Additionally, since more of our patients with ILD events had been treated with bucillamine than those without ILD events, a prospective re-evaluation would verify our data and match patients’ characteristics in terms of disease-modifying antirheumatic drug use.
In conclusion, our study reveals that TNF inhibitors have the potential risk of ILD events in patients with pre-existing ILD and KL-6 can be used for the detection of such events. KL-6 testing and the use of non-TNF inhibitors seem to be favourable options for benefitting these patients.
Acknowledgments
We thank Phyllis Minick for excellent assistance in the review of English.
References
Footnotes
-
Contributors TN, KA and SM designed and performed experiments, and contributed to writing of the manuscript. TN, KA and NK contributed to clinical data analyses. KA and KT contributed to the interpretation of the results. All authors approved the final version of the manuscript.
-
Funding This research received no specific grant from any funding agency in the public, commercial or not-for-profit sectors.
-
Competing interests None.
-
Ethics approval Ethics committee of Kameda Medical Center.
-
Provenance and peer review Not commissioned; externally peer reviewed.
-
Data sharing statement No additional data are available.