Article Text

Abstract
Introduction Amyotrophic lateral sclerosis (ALS) is the most common motor neurone disease. It occurs in two forms: (1) familial cases, for which several genes have been identified and (2) sporadic cases, for which various hypotheses have been formulated. Notably, the β-N-methylamino-L-alanine (L-BMAA) toxin has been postulated to be involved in the occurrence of sporadic ALS. The objective of the French BMAALS programme is to study the putative link between L-BMAA and ALS.
Methods and analysis The programme covers the period from 1 January 2003 to 31 December 2011. Using multiple sources of ascertainment, all the incident ALS cases diagnosed during this period in the area under study (10 counties spread over three French regions) were collected. First, the standardised incidence ratio will be calculated for each municipality under concern. Then, by applying spatial clustering techniques, overincidence and underincidence zones of ALS will be sought. A case–control study, in the subpopulation living in the identified areas, will gather information about patients’ occupations, leisure activities and lifestyle habits in order to assess potential risk factors to which they are or have been exposed. Specimens of drinking water, food and biological material (brain tissue) will be examined to assess the presence of L-BMAA in the environment and tissues of ALS cases and controls.
Ethics and dissemination The study has been reviewed and approved by the French ethical committee of the CPP SOOM IV (Comité de Protection des Personnes Sud-Ouest & Outre-Mer IV). The results will be published in peer-reviewed journals and presented at national and international conferences.
- PUBLIC HEALTH
- EPIDEMIOLOGY
This is an Open Access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/
Statistics from Altmetric.com
Strengths and limitations of this study
-
This is the first ambitious project to investigate the link between β-N-methylamino-L-alanine (L-BMAA) and amyotrophic lateral sclerosis (ALS) in France, taking advantage of the existing federation of BMAALS consortium members in the French network on ALS clusters detection and investigation.
-
The case ascertainment relies on multiple sources and, among those, on a common database shared by all French ALS referral centres, which collects information about patients since 2003. The study represents more than 47 million persons-years of follow-up.
-
We developed and validated a new analytical procedure for the determination of underivatised L-BMAA at trace levels in complex environmental matrices.
-
The rapid death of patients led to a major difficulty in finding living patients for questionnaires: patients’ relatives are interviewed, which can induce a bias in responses.
-
At the time of the writing, few patients have given their consent to a postmortem swab which can limit the impact of our study.
Introduction
Amyotrophic lateral sclerosis (ALS) is a debilitating and fatal neuromuscular disease with an incidence close to 2.5/100 000 person-years of follow-up (PYFU) in Europe.1 Two forms of the pathology coexist: familial ALS (FALS) accounts for approximately 10% of total cases and the remaining 90% occur sporadically (SALS, sporadic ALS). Historically, an association has been observed between a mutation on the superoxide dismutase 1 gene (SOD1) and FALS.2 However, other mutations3–8 have since been discovered, as C9orf72 (chromosome 9 open reading frame 72), TARDBP (TDP-43 encoding gene) and FUS (fused in sarcoma protein) are commonly identified in FALS cases.8–16
Although SOD1, FUS and TARDBP mutations have also been found in SALS cases,2 ,17 the current broad scientific consensus is in favour of a gene–environment interaction causing SALS: lifestyle factors, environmental exposure, occupational exposure and handling toxic compounds are among the many factors that can play a role in the appearance of the pathology. Among lifestyle factors, smoking is the factor that has been most documented and is mainly associated with a higher risk of ALS,18–23 whereas coffee and alcohol consumption are considered protective or not associated with ALS.18 ,24 ,25 Other associations have been proposed as occupational exposure to electromagnetic fields,23 ,26–29 frequent head trauma,30 ,31 contact with certain chemicals such as pesticides, formaldehyde, organic solvents and heavy metals.23 ,32–37 Another controversial hypothesis, often cited, is that physical activity, whether occupational or leisure related, is a risk factor for SALS.38–43 This theory is sustained by the higher risk of ALS in professional soccer players.31 ,44–49
On the Pacific island of Guam, ALS-Parkinsonism dementia complex (ALS-PDC), which presents similarly to ALS, occurred at 50 to 100 times the incidence seen worldwide in the 1950s.50 ,51 An epidemiological study established that consumption of a Chamorro diet was the only variable significantly associated with disease incidence.52 In 1967, Vega and Bell53 discovered a neurotoxin, β-N-methylamino-L-alanine (L-BMAA), in the genus Cycas, the seeds of which are used to make flour. Hence, L-BMAA could have been consumed by Chamorro people through multiple dietary sources, including cycad flour as well as meat from flying foxes and other animals that feed on cycad seeds.54–57 In the 1990s, L-BMAA was proposed as a cause of ALS-PDC.58 This hypothesis is supported by the presence of L-BMAA in brain tissues of patients with ALS-PDC and ALS from Guam and Canada, as well as by its absence in controls.55 ,56 ,59 In vitro and in vivo experiments also suggest that L-BMAA plays a role in neuropathological processes implicated in ALS. Indeed, the treatment of dissociated mixed spinal cord cultures with a concentration of L-BMAA around 30 µM caused selective motor neurone loss.60 Moreover, monkeys fed with large doses of the toxic acid from cycads developed neurological impairments: damaged motor neurones in the spinal cord produced a flaccid paralysis and then damaged neurones in the striatum and cortex, which produced Parkinsonism and behavioural changes.61 ,62 In rats, although the intraperitoneal injection of L-BMAA did not provoke any obvious motor dysfunction,63 it induced markers of oxidative stress in the liver and cellular changes in favour of apoptosis in motor neurones of the spinal cord.63 ,64 In neonatal rats, L-BMAA induced significant systemic changes in energy metabolism and amino acid metabolism (identification of initial metabolite changes for lactate, acetate, D-glucose, creatinine and 3-hydroxybutyrate).65 Together, these findings suggest that acute toxicity of L-BMAA induces developmental alterations that result in long-term effects on brain function. L-BMAA is also found to be associated with proteins in cyanobacteria55 ,66 ,67 and in brain tissue of patients with ALS.55 ,59 ,68 It has recently been proposed that L-BMAA may be misincorporated into proteins and thus may lead to protein aggregation, a hallmark of neurodegenerative diseases,69 ,70 inducing a chronic exposure to low levels of L-BMAA.69
First of all, L-BMAA was found to be produced by a wide range of cyanobacteria55 ,56 ,66 ,67 ,71–73; recently, it was shown that diatoms, the most common group of algae, could also produce it.74 However, the level of free or bound L-BMAA detected in cyanobacteria is controversial and the high concentrations reported in the first studies were challenged by several recent studies. L-BMAA could be transferred from cyanobacteria or diatoms via zooplankton to organisms at higher trophic levels.75 Cox and collaborators have interestingly highlighted the biomagnification (increasing accumulation of bioactive, often deleterious, molecules through successively higher trophic levels of a food chain) of L-BMAA in trophic chain,54 ,56 ,76 ,77 explaining the large amounts detected in flying foxes from Guam.54–57
Owing to eutrophication and, to a lesser extent, climate changes,78 ,79 cyanobacterial blooms seem to be increasing in freshwater ecosystems worldwide. France is not exempt from this phenomenon as different genera of cyanobacteria are found on its territory.80–83 Therefore, exposure of French patients with ALS to cyanobacteria, and thereby to cyanotoxins as L-BMAA,84 is a reasonable hypothesis that could potentially explain some ALS cases.
The French BMAALS program85 takes advantage of (1) the existing federation of BMAALS consortium members in the French network on ALS clusters detection and investigation, supported by INSERM (Institut National de la Santé et de la Recherche Médicale) and (2) of geoepidemiology to investigate patients’ environment (dwelling, occupational and leisure) in order to assess spatial association (not cause-and-effect) between ALS cases and a putative cyanobacterial exposure in combination with patients’ history about prior exposures. Furthermore, a case–control study will be performed to investigate the potential routes of contamination by L-BMAA, which are: (1) ingestion of contaminated drinking water or dermal contact in recreational water75 ,86–89; (2) consumption of aquatic or terrestrial food previously exposed to toxins55 ,75 ,84 ,90–93; (3) cyanobacterial dietary supplements which are rich in protein content73 ,94 ,95 and (4) inhalation or aerosolisation.96–99 To assess the exposure of patients to L-BMAA, a reliable quantification method has been developed and validated. To the best of our knowledge, this is the first ambitious project to investigate the link between L-BMAA and ALS in France.
Methods and analysis
BMAALS programme
The main objective of the BMAALS programme is to improve our knowledge on the putative links between the occurrence of ALS and the neurotoxin L-BMAA by studying the defined geographical regions in France. To reach our aim, the BMAALS group (a multidisciplinary consortium of epidemiological, neurological, chemical, microbiological and environmental experts) was created in 2011. The protocol was reviewed and approved by the ethical committee of the CPP SOOM IV (Comité de Protection des Personnes Sud-Ouest & Outre-Mer IV) on 10 February 2011.
The protocol is organised in six steps:
-
An exhaustive ascertainment of all incident ALS cases was performed for the period under study and in the areas under surveillance.
-
Based on this case ascertainment, geostatistical analyses will allow identification of clusters, characterised as abnormal aggregates of affected people, according to incidence calculations.
-
A population-based case–control study will be performed taking into account notable clusters previously identified.
-
Mapping of factors conducive to algae blooms will help assess indirect exposure of patients to cyanobacteria and, by extension, to cyanotoxins.
-
Collection of tap water, fruits and vegetables from the gardens (among those cultivating), as well as irrigation water will assess direct exposure of patients to L-BMAA. These results will be compared with findings from control environments.
-
Postmortem analysis of voluntary SALS-donors’ and control-donors’ brains will permit evaluation of bioaccumulation of L-BMAA in French patients.
Case ascertainment
Spatial and temporal dimensions
The programme covers the period from 1 January 2003 to 31 December 2011 and involves 10 counties from three French areas (equivalent to districts or subdistricts in some other countries), namely Limousin with 3 departments out of 3, Languedoc-Roussillon with 2 departments out of 5 and Rhône-Alpes with 5 departments out of 8 (figure 1). Owing to the long study period (9 years) and the extended area (5 230 000inhabitants), this represents more than 47 million individuals PYFU (table 1).
Populations in the areas under study

Areas under study in the BMAALS programme. BMAALS is a French project with collaboration between three regions: Limousin, Languedoc-Roussillon (2 departments out of 5) and Rhône-Alpes (5 departments out of 8).
Case ascertainment methodology
The methodology applied here is consistent with that used for the the French register of ALS in Limousin (FRALim register).100 Case ascertainment began with the creation of the consortium in 2011 and is now complete.
Patients were required to meet the following inclusion criteria: (1) living in the area under study at the time of diagnosis; (2) diagnosed with ALS that is definite, probable or probably laboratory supported (excluding clinically possible cases) according to El Escorial revised criteria (EERC)101 ,102 and (3) they were identified by at least one source of ascertainment (out of three). After obtaining authorisations from CCTIRS (Comité Consultatif sur le Traitement de l'Information en matière de Recherche dans le domaine de la Santé) and CNIL (Commission Nationale de l'Informatique et des Libertés), nominative data are obtained from the French national coordination of ALS referral centres, public and private hospitals in the areas of interest, and health insurance data related to long-duration diseases.
First source: French national coordination of ALS referral centres
Since 2003, all French ALS referral centres share a common database (Ictrals and then CleanWeb) that collects information about patients. The CleanWeb database was authorised by the CNIL on 27 May 2011. Two kinds of information are gathered: (1) sociodemographic data (first and last name, age, birthday, current address and date of death if applicable) and (2) clinical data such as EERC, form of onset (spinal or bulbar), symptoms, ALS functional rating scale-revised, manual muscular testing and103 diagnosis delay.104
Second source: public and private hospitals
Hospital medico-administrative data from inpatients with a G12.2 code, corresponding to motor neurone disease according to the international classification of disease 10th version in any of their medical records (principal, related, significantly associated or documentary associated diagnosis), were collected. New cases so determined were further analysed by a neurologist to confirm the ALS diagnosis and EERC.
Third source: health insurance bodies
Health insurance bodies were asked to help by identifying patients declaring a long-duration disorder coded ALD n°9, specific to ALS according to the French Haute Autorité de Santé. Four important French institutions agreed to participate: the principal one was the “régime général”, which concerns 75% of the French population, and the three others were specific to subgroups of people: (1) the “régime agricole, mutuelle sociale agricole” for those in the agricultural domain, (2) the “régime social des indépendants”, which deals with artisans, traders, industrialists and private professionals and (3) the “caisse nationale militaire de sécurité sociale” for military employees. For patients recruited from these sources, EERC was also reviewed in a centralised way.
In order to verify the completeness of the recruitment of incident ALS cases in the period of time and area of interest, we will use a capture–recapture method (figure 2).105 ,106 Matching multiple sources of information from a unique population allows for estimation of the number of cases unidentified by any source, the total number of cases and the exhaustiveness of each source.

Multiple sources of case ascertainment. For the application of a capture–recapture method, three sources were solicited: (1) the French national coordination of amyotrophic lateral sclerosis (ALS) referral centres, (2) public and private hospitals and (3) health insurance structures.
This methodology of case ascertainment uses the same three sources that have been previously applied in the FRALim register100 (first register of ALS in France, located in Limousin, for the period 2000–2011). We estimated, thanks to the capture–recapture analysis, an exhaustiveness of the register of 98.4% (95% CI 95.6% to 99.4%), yielding a low number of false-negative cases100 (ie, missed cases). Data from private neurologists were not obtained because most lacked computerised records and a retrospective chart review was not feasible.
Geoepidemiology
Geographic information systems (GIS) will be used to structure and analyse geographic information collected or produced in the context of the programme. In France, the legal geodesic network reference, established by the French Institut National Géographique et Forestière (IGN), is RGF93 (the French geodesic network set up in 1993). Thus, all cartography carried out by the BMAALS consortium will be projected in RGF93.
To ensure comprehensive data analysis, we have decided to investigate three levels as described below (figure 3).

The three levels considered for geostatistical analyses. Aims and methodologies applied are represented for each of the three levels: from the smallest geographic unit for calculating ALS incidence; through the average geographic unit for studying the cyanobacteria extent; to finally the largest geographic unit for assessing exposure of patients with ALS (ALS, amyotrophic lateral sclerosis; P, phosphorus; N, nitrogen).
First level, smallest geographic unit: ALS incidence
According to Knox,107 a cluster in epidemiology is defined as “a geographically bounded group of occurrences of sufficient size and concentration to be unlikely to have occurred by chance”. Recently, Elliott and Wartenberg108 wrote that “the term disease cluster is poorly defined but implies an excess of cases above some background rate bounded in time and space”. Thus, those imprecise definitions do not explain clearly what a cluster is: how many cases do we need for considering having a cluster?
When considering a rare disorder such as ALS, one inherent issue is the small number of events. Therefore, it is necessary to consider a large population obtained by aggregating cases over many years and/or by using a large geographical area. Indeed, individual clusters should not be investigated unless a sufficient number of cases is reached (five or more) and relative risks (RR) in a particular area are higher than 20.109 ,110 However, among five articles published since the year 2000 and dealing with spatial clustering of ALS, only one team found clusters with high RR (table 2).111
Spatial clustering of ALS
In the BMAALS programme, overincidence clusters are defined as areas where RR is found as being greater than 1.8, while underincidence zones are those characterised by an RR lesser than 1.
After case ascertainment, addresses of patients included in the programme will be geocoded. Districts defined as life areas are the chosen grouping units with which to measure expected cases. According to the French Institut National de la Statistique et des Etudes Economiques (INSEE), a life area is the smallest territory unit in which inhabitants have access to common equipment and services.
Expected case values depend on the demographical structure (age and sex) of the exposed population, given their observed incidence in the 10 studied counties (table 1). Then a standardised incidence ratio (SIR) will be determined by calculating the ratio between the number of observed cases and the number of expected cases. The significance of SIR compared with global incidence will be evaluated using a Poisson distribution (95% confidence). Geostatistical analyses, based on Kulldorff statistics, will be performed to identify areas of significant overincidence or underincidence as compared with the referral incidence value, which is the global incidence in the whole area under study.26
This first cartography is useful for tracking interesting sites for patients’ interview.
Second level, average geographic unit: cyanobacterial bloom investigation
Numerous physical parameters favour the extensive propagation of cyanobacteria, such as warmer temperatures, particular rainfall patterns, windiness and consequently the intensity of thermal stratification of the water column.114–116 Moreover, bloom-forming cyanobacteria have been shown to be favoured by high alkalinity and associated high pH.117 The increasing magnitude and frequency of cyanobacterial blooms is also related to the nutrient enrichment (phosphorus, P, and nitrogen, N) of freshwater118–122 and input of micronutrients such as iron and molybdenum.123 ,124 A recent model has identified higher risk lake environments where a more targeted monitoring of cyanobacterial biovolumes should be focused: water colour 10–20 Pt/L, alkalinity >1 mEq/L, retention time >30 days and total P >20 µg/L.125
All these parameters should be considered when carrying out descriptive cartography and tracing the history of cyanobacterial blooms. To do that, we will make use of various free-to-access databases such as: Basias (Bureau de Recherches Géologiques et Minières, BRGM), which compiles lists of plants located on French territory that are susceptible to the release of P, N and nutrients in water; data furnished by water agencies concerning measurements of industrial pollutant emissions and wastewater treatment plants; ADES portal (Accès aux Données sur les Eaux Souterraines), which gives access to water channelling points and water consumption quality control. Moreover, a convention with Météo France, the French organisation for meteorology, has been signed to retroactively view climate conditions over the period 2003–2011 and before. All these data will be integrated into our GIS to create a complete database, and also to identify sites of interest for sampling.
Geographic statistics will then be performed in order to classify each administrative unit (eg, municipality) according to four parameters: (1) the number of days of sunshine, (2) temperature, (3) the area of stagnant water (included dams and ponds) and (4) data on P and N withdrawal. For the last one, anthropogenic factors will also be considered as industrial and agricultural activities can impact on N and P release (use of organophosphorus compounds, for example). This multicriteria approach will yield an index of proliferation of cyanobacterial blooms. The same will be carried out with watersheds as there is an aggravating effect from upstream to downstream of P and N inputs. Finally, a coefficient correlation will be measured between SIR and the calculated index.
This database will also gather information about all plants on French territory, the high-voltage electricity network and stretches of water (ponds, rivers, etc). Hence, it will give a general overview of patients’ and controls’ industrial and dwelling environments. Geographic statistics based on classification of municipalities as previously described will be used to highlight interesting particularities.
Further analysis of cyanobacterial blooms will involve using a fluorimetric probe to detect the emission and excitation wavelength of phycocyanin, a pigment almost exclusively specific to cyanobacteria.126 Water sampling will permit the identification of cyanobacterial species. Gathering information about conditions favourable for cyanobacterial blooms will allow us to model their expansion notably in terms of meteorology and nutrient inputs. Through the use of previously collected data, we will be able to ascertain if there were cyanobacteria prior to patients' diagnosis and the species present, and therefore if there was a risk of L-BMAA presence in water.
Third level: large geographic unit: questionnaire for a case–control study
This part aims to highlight differences in life habits between patients SALS and controls. Criteria for selecting patients with ALS are as follows: (1) familial history cases are excluded; (2) last known address must be in an overincidence or underincidence area and (3) if possible, vicinity with other affected people, which may suggest a close source of an environmental risk factor leading to ALS. Controls will be matched on age at diagnosis, sex and city and should not present any neurological pathologies. Chosen patients and controls will be submitted to a semistructured interview, for example, systematic questions with the possibility of free interview to look in more depth at particular issues raised. The questionnaire has been developed by the consortium specifically for the BMAALS programme.
On the basis of the initial results of clustering,26 a number of clusters to investigate was selected a priori: 3 overincidence areas in Limousin, 2 in Languedoc-Roussillon and 4 in Rhône-Alpes; with an expected number of 4 patients in each cluster (and 4 controls), this will represent a total of about 72 interviews. The same number of interviews for patients and controls will be performed in underincidence areas. Owing to the short survival time of the disease, the number of living patients diagnosed between 2003 and 2011 is low. Thus, when necessary, relatives will be questioned.
Cyanobacterial and L-BMAA hypotheses are tested via questions about: (1) drinking water; (2) bathing habits; (3) food consumption including dietary supplements (to be specified if applicable), the type of supplement is informed and (4) irrigation water, if any. The aim of the questionnaire is to obtain a comprehensive description of patients’ habits in all aspects of their lives. Hence, it will be made clear that questions are not just about the time immediately preceding the diagnosis.
To assess exposure to cyanotoxins indirectly, an ad hoc questionnaire is a useful supplement to direct collection of environmental samples.127 Hence, samples will be taken in case and control environments to test for the presence of cyanobacteria in water (the same probe as described above) and for further chemical analysis (in water and food).
To ensure that L-BMAA is most likely to be implicated, the questionnaire also covers items already described in the literature such as dwelling location (urban/rural), occupation, presence of certain industries in the dwelling environment, toxic exposure during employment or hobbies, participation in sport, physical trauma, alcohol and tobacco consumption.23 ,26 ,32 ,33 ,48 ,128–131 As there is probably a long latency period between exposure and appearance of ALS132 ,133 and given that L-BMAA exists in a protein-associated form which could act as an endogenous neurotoxic reservoir over time,55 an in-depth study will involve gathering details of dwelling since birth (in order to collect their precise residential history), and for other items from age 13. Indeed, the French population is regularly subject to migratory flows (figure 4) and it has to be considered in our study.
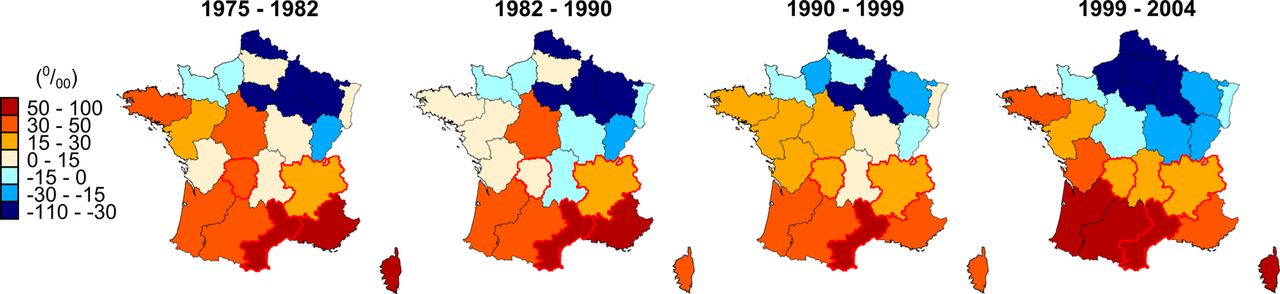
Residential migration rate of the French population. These maps reflect the intraregional mobility of the French people from 1975 to 2004. The residential migration rate is expressed per 1000 persons. (Data from INSEE, Institut National de la Statistique et des Etudes Economiques).
All information gathered will be used to map the spaces where patients live for further analysis to identify common places, and also to further analyse the cyanobacterial history of these areas.
Chemical and microbiological approaches
An analytical procedure has been developed and validated in our programme for the determination of underivatised L-BMAA at trace levels in complex environmental matrices (cyanobacteria, biofilm, food, human brain tissue, plasma or urine) using solid-phase extraction based on mixed mode sorbent to concentrate and clean up real complex samples.134 The methodology of quantification relies on liquid chromatography (LC) coupled to tandem mass spectrometry (LC-MS/MS). The proportion of free and then bound L-BMAA in cyanobacterial proteins will be measured.
In parallel, a microbiological study will be undertaken involving the culture of axenic cyanobacteria strains from various origins and ecosystems (terrestrial, aquatic, fresh water, sea water or brackish water), as was conducted in seminal work by Cox et al.67 By using the analytical method described above, free L-BMAA will be quantified in environmental and biological samples. Moreover, kinetic experiments will assess whether L-BMAA production is constitutive or if variations of concentration are observed over time. Finally, isotopic incorporation experiments using various labelled amino acid should help identify the putative precursors of L-BMAA.
Implications of results for searching theoretical models
A synthesis of the results of the steps described above aims to develop a cyanobacterial proliferation model based on environmental and microbiological data, on the one hand, and to detail population exposure to L-BMAA relying on the detection of the presence of L-BMAA in patients’ environment, on the other. First, environmental data will serve to identify climatic parameters (sunshine, temperature, rainfall and wind patterns) favourable for cyanobacterial blooms; microbiological analyses will allow one to determine propitious conditions leading to L-BMAA production by cyanobacteria. Population exposure will be studied by (1) comparing industrial occupation between overincidence and underincidence areas; (2) assessing the risk of exposure through public facilities and infrastructure and (3) examining differences in habits between cases and controls.
Discussion
The present project aims to better describe the link between ALS, the neurotoxin L-BMAA and cyanobacteria through the use of case ascertainment, spatial clustering, questionnaires and chemical analyses.
Food frequency questionnaires prove to be reliable for long-term recall, from 8 to 24 years135–139: hence, they appear to be a good alternative to food diary recall for diseases with a potential long-term incubation. However, the BMAALS project concerns three French regions which are irregular in terms of population density: Rhône-Alpes has about 141 inhabitants/km2 (in 2009), Languedoc-Roussillon about 95 inhabitants/km2 (in 2007) and finally, the least populated of the three is Limousin with 43 inhabitants/km2 (in 2010; INSEE figures). This heterogeneity, combined with the long period studied (2003–2011) and the rapid death of patients, led to a major difficulty in finding living patients for questionnaires, in particular in Limousin. So patients’ relatives are interviewed, which can induce a bias in responses.140 To avoid any misinterpretation of the question concerning dietary habits, it is clearly clarified that it concerns habits before diagnosis and first symptoms. Moreover, we have also developed a self-administered questionnaire given to all patients with ALS (not only those included in our programme) and will compare answers between patients since 2012 and those from 2003 to 2011 (ancillary study).
Likewise, owing to the fact that ALS is a rare disorder, areas of significant underincidence are characterised by the absence or almost absence of patients. With regard to multiple source case ascertainment, we recognise that some patients might be missed because of the difficulty in diagnosing ALS in elderly people due to the confusion between ALS symptoms and decline due to ageing. Another important issue is the low participation rate for postmortem analysis: at the time of the writing, few patients have given their consent to a postmortem swab, thereby perhaps reducing the impact of our study.
The hypothesis of L-BMAA exposure as an environmental risk factor in ALS pathology is controversial, notably because of the contradictory results. Intoxication assays with the toxin yielded uneven results.141 With regard to experimental designs, it appears that the neurotoxic effect of L-BMAA: (1) depends on the mode of administration, (2) is species dependent and (3) genetic predisposition may also be at play.142 For example, two teams failed to develop a mouse model by daily oral administration of L-BMAA (0.001 and 0.5 g/kg),143 ,144 whereas Spencer and collaborators have developed a simian model by the daily oral administration of L-BMAA with doses ranging from 0.1 to 0.3 g/kg.61 ,62 Furthermore, other murine models based on intraperitoneal and intracerebroventricular injections of L-BMAA in mice and rats lead to effective behavioural changes.63 ,145–151 Other work strengthens the L-BMAA hypothesis by highlighting the implication of the toxin in other degenerative diseases such as Alzheimer's disease (AD), Parkinson's disease and pigmentary retinopathy.55 ,56 ,59 ,68 ,152 ,153 Although the mechanism of action is not yet completely understood, it seems that L-BMAA neurotoxicity involves: (1) direct action on N-methyl-D-aspartate receptors; (2) activation of glutamate receptor 5, (3) induction of oxidative stress154 ,155 and (4) association to protein due to mischarging of transfer RNA.69 Moreover, a recent study has shown that L-BMAA leads to an increase in the insoluble TAR DNA-binding protein 43 (TDP-43),156 the aggregation of this protein being an important hallmark in neurodegenerative diseases.157 To further support our seminal hypothesis, it is interesting to note that microcystin-leucine-arginine, a cyanobacterial toxin, has been shown to be involved in AD.158 ,159
Another debatable point concerns the quantification of L-BMAA, given that the concentrations measured vary depending on the analytical method used (figure 5). The crucial issue is to develop a method that distinguishes L-BMAA from its isomers and amino acids to achieve a selective titration method. Currently, the most widely used L-BMAA quantification method is LC-MS/MS.68 ,72 ,75 ,90–92 ,160 A prederivatisation step, prior to LC separation, has also frequently been described using 6-aminoquinolyl-N-hydrosuccinimidyl carbamate (6-AQC), a fluorescent derivative agent. In that case, the analyte was either detected by fluorescence or by tandem MS. However, a major drawback of this prederivatisation is the likelihood of false-positive results.161 A comparison of five standard methods, namely high-pressure LC with fluorescence detection (HPLC-FD), ultra HPLC (UHPLC)-MS/MS, UHPLC-MS/MS with AQC or propyl chloroformate derivatisation and UHPLC with ultraviolet detection shows that they all clearly distinguish L-BMAA from other amino acids.162 One team succeeded in detecting L-BMAA in brains from patients with ALS-PDC or AD by using HPLC-FD and samples derivatised with 6-AQC,55 ,56 ,59 ,68 while other teams failed to detect any L-BMAA in patients’ brains by using HPLC-FD with samples derivatised with 9-fluorenylmethylchloroformate (FMOC) or by gas chromatography (GC).163 ,164 These results suggest that either HPLC-FD with a 6-AQC derivatisation is more sensitive than HPLC-FD with an FMOC derivatisation or 6-AQC derivatisation generates false-positive results. The GC method has been improved to enhance recovery but was still inefficient in detecting L-BMAA in brains of mice fed with it.165 This was later made possible, but it is still not efficient in human tissues.166 This illustrates the importance of continuing to improve analytical methods.

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
L-BMAA quantification in molluscs throughout the world. A comparison of three quantification methods and teams highlights discrepancies in L-BMAA titration. Does that reveal a difference in selectivity of the method or the existence of a gradient of the neurotoxin? L-BMAA levels are expressed as µg L-BMAA/g dry weight±SE (FD, fluorescence detection; L-BMAA, β-N-methylamino-L-alanine; LC, liquid chromatography; LC-MS/MS: LC coupled to tandem mass spectrometry; HPLC, high-pressure LC; rHPLC: reverse phase HPLC; SPE, solid phase extraction; UHPLC, ultra HPLC).
It has been shown that HPLC-FD overestimates L-BMAA concentration, due to low selectivity, with estimates in the high µg/g range rather than in the more realistic ng/g to low µg/g range. The LC-MS/MS method is more selective and gives more reliable results.160 One major argument in favour of using underivatised methods is that the universal 6-AQC derivatisation of primary and secondary amines could lead to misidentification of L-BMAA in complex matrices.161 The method we propose here,134 based on LC/MS-MS, over-rides the derivatisation step, unlike another recent new method developed,167 and allows the quantification of L-BMAA at trace levels, but it remains to be adapted for quantification of L-BMAA in all the matrices needed in the programme.
Inability to detect L-BMAA in patients’ brains casts doubt on its bioaccumulation. Addressing this issue, we can argue that: (1) L-BMAA crosses the blood–brain barrier (BBB)61 ,62 ,166 ,168 and (2) there is a scientific consensus on the bioaccumulation of L-BMAA in trophic chains, which has been shown by several teams in seafood.75 ,90–92 ,169 Together, these results suggest that L-BMAA after having crossed the BBB can be bioaccumulated, as it is concentrated in brains of other organisms.57 ,75 ,91 Furthermore, a brief review of the literature reveals that L-BMAA has been quantified in the brain using MS.55 ,56 ,59 ,68 ,164 Glover et al170 showed that failure to detect L-BMAA cannot be considered proof of absence of the compound because of its reactivity with metal ions in the sample matrix and the formation of metal adducts during electrospray ionisation MS. However, this problem should be overcome by quantifying the matrix effect by using spiked samples with pure standards.134
Nonetheless, finding putative sources of L-BMAA contamination is proving very difficult. To illustrate this point, we can cite Karlsson et al70 who demonstrated L-BMAA clearance: in 7-month-old neonatal rats, there is no detectable free or protein-associated L-BMAA. The authors suggest that observed long-term protein changes and cognitive impairments in adult animals exposed to L-BMAA as neonates171–174 are due to mechanisms initiated during development. Hence, the clearance mechanism may lead to the inability to detect L-BMAA in patients’ brains, but that does not mean that L-BMAA is innocuous pathologically. Besides, neonatal contamination is conceivable as Andersson et al175 have shown that L-BMAA can be transferred to neonates during lactation via breast milk. This new route of contamination conspicuously complicates the identification of an environmental risk factor. Moreover, as ALS is probably a gene–environment disease, attention must also be paid to genetic and epigenetic factors.176–179 For example, genetic susceptibility to environmental toxins—heavy metals, solvents/chemicals and pesticides/herbicides—has been reported.180
It is of major importance to identify environmental risk factors causing SALS. The protocol presented here aims to study the link between L-BMAA and ALS in France by characterising exposure modalities, either individual or collective, to cyanobacteria and more precisely to the L-BMAA toxin. Thanks to the questionnaire, it also intends to shed light on other assumptions formulated in literature as putative origins for SALS (as occupational exposure and sports practising). Finally, our results could be used to generate a guide of precautions against behavioural risk leading to exposure to L-BMAA.
In conclusion, the results of this project should help to (1) give a clear picture of ALS distribution over 10 French counties; (2) identify clusters where environmental factors may play a greater role than elsewhere; (3) provide information about some environmental specificities of ALS clusters, especially regarding factors related to cyanobacteria presence and proliferation as also BMAA presence and (4) see to what extent the BMAA hypothesis seems to be relevant regarding the explanation of SALS clusters within the large French area considered. Despite limitations mainly due to i) interviews of patients' relatives and ii) the controversy on L-BMAA analysis, this programme is of importance because it is the first to investigate the cyanobacteria hypothesis in France.
Acknowledgments
The authors thank all institutes which collaborated with case ascertainment. The authors gratefully acknowledge William Francis for careful editing of the manuscript.
References
Footnotes
-
Contributors PC, BM, P-MP, MD-C, FB, EL, VB, DJB, WC, VP and AM were involved in the study conception and design. PC, BM, MN, EL, VB, GB, WC, NP and RJ-M have participated in case ascertainment. AD is responsible for questionnaires. AM and OP were involved in the cyanobacteria study. VP, AC and SEA are responsible for chemical analyses. FB and J-PL are geoepidemiologists. LB, ML, EM and EA are environmentalists. FP, JB and VR are anatomopathologists. AD wrote the manuscript, which was finally approved by BM, PC, FB and P-MP. All authors read and approved the final manuscript.
-
Funding This work is supported by the French National Research Agency (ANR) grant number programme ANR-11-CESA-0014 (Project “BMAALS”).
-
Competing interests None.
-
Patient consent Obtained.
-
Ethics approval Comité de Protection des Personnes Sud-Ouest & Outre-Mer IV.
-
Provenance and peer review Not commissioned; externally peer reviewed.