Article Text

Abstract
Objectives and hypothesis To examine the influence of gender of the baby on exclusive breastfeeding and incidence of postnatal depression (PND). We hypothesise that in a society with a male gender bias there may be more PND and less exclusive breastfeeding of the girl child.
Design Prospective study.
Setting The study was conducted in an urban, tertiary hospital in Delhi.
Participants Mothers delivering normally with their babies roomed-in.1537 eligible women participated in the study.
Primary and secondary outcome measures Exclusive breastfeeding within the first 48 h of life and score on the Edinburgh Postnatal Depression Scale (EPDS) were recorded.
Results 3466 babies were born in the hospital. There were 792 girls for every 1000 boys. Among primiparous women, the sex ratio was 901 girls per 1000 boys. For second babies, the sex ratio was 737:1000. If the first child was a girl the birth ratio fell to 632. 1026 mothers were exclusively breastfeeding. Exclusive breastfeeding of boys was significantly higher (70.8% vs 61.5%, p<0.001). The EPDS score was significantly higher with the birth of girls (EPDS 6.0±3.39 vs 5.4±2.87, p<0.01). Women with an EPDS score >11 were less likely to exclusively breastfeed (p<0.01).
Conclusions The results point to a pro-male gender bias evidenced by a low sex ratio at birth, higher EPDS score in mothers of girls and less breastfeeding of female children.
This is an Open Access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 3.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/3.0/
Statistics from Altmetric.com
Strengths and limitations of this study
-
Postnatal depression was evaluated using the widely validated Edinburgh Postnatal Depression Scale (EPDS) scoring system.
-
It was carried out in an urban hospital catering mostly to a middle-class clientele. The findings on sex ratio may therefore not be generalisable to other social groups.
-
We studied the initiation of exclusive breastfeeding in the first 48 h. More studies are needed to elaborate the effect of sex bias on the duration of breastfeeding.
-
EPDS scoring was performed in the first 48 h and would include mothers with transient postnatal blues not amounting to postnatal depression. Follow-up studies are needed to see that how many of them develop significant depression.
-
Although multiple regression analysis shows that higher depression score and female sex of the child are associated with lower odds of exclusive breastfeeding, a causal relationship is not implied.
-
High rate of sex-selective abortion may complicate the interpretation of results.
Introduction
Breast milk is the preferred food for all infants including premature and sick babies.1 UNICEF has promoted breastfeeding initiation within an hour of childbirth.2 ,3 It provides nutritional, immunological, developmental and psychological advantages to the child besides health advantages to the mother and economic benefits to the family.1 It establishes skin-to-skin contact providing warmth to the newborn. Suckling at the breast stimulates oxytocin release which further increases flow of milk from the breast. Breast milk reduces mortality in the first month of life.4 Early breastfeed initiation is also associated with increased exclusive breastfeeding (EBF) and longer duration of breastfeeding.5 The WHO and UNICEF launched the baby-friendly hospital initiative in 1991 to strengthen maternity unit practices to support breastfeeding.6 However in spite of all these promotions and the known benefits of breastfeeding, EBF and early initiation of breastfeeding are not often practiced. Factors intrinsic to the mother or baby may play a crucial role. One such factor is postnatal depression (PND) and there is evidence that mothers with PND are less likely to breastfeed.7 ,8
Expression of PND may extend from the more transient baby blues to a longer lasting depression going on for several weeks.9 In both conditions there are mood swings, crying jags, sadness, insomnia and irritability.10 ,11
The 10-question Edinburgh Postnatal Depression Scale (EPDS) is a validated, valuable and efficient way of identifying patients at risk for perinatal depression. It can be applied for depression screening during pregnancy.12 The scale has been used as early as the first or second postnatal day by Teissèdre in order to screen women at risk of PND. In his study, 1154 women completed the EPDS at 2–3 postnatal days and again at 4–6 weeks postnatal. He found that there was a highly significant positive correlation between EPDS scores on the two occasions (Spearman rank correlation r=0.59, p<0.0001).13 Although studies performed in the immediate postnatal period are likely to pick up many cases of postnatal blues, Dennis and McQueen14 found that mothers with an EPDS score >12 at 1 week postnatal were significantly more likely at 4 and/or 8 weeks to discontinue breastfeeding, be unsatisfied with their infant-feeding method, experience significant breastfeeding problems and report lower levels of breastfeeding self-efficacy.
Studies looking at the sex ratio at birth have shown that there is a strong gender bias in India, favouring boys.15–17 Jayachandran and Kuziemko18 have shown that boys tend to be breastfed longer. The EPDS score in relation to sex of the child has not been studied. Also the association between birth of girl babies (in a society with a male sex bias), EPDS score soon after birth and EBF has not been examined previously. We hypothesise that there may be a higher EPDS score and less exclusive early breastfeeding of girl children. Recognition of these possible barriers to EBF may allow more focused support to mothers that will promote breastfeeding and improve survival of the girl baby.
Ethics statement
Informed written consent was obtained from participants. Data and names of the respondents are kept confidential. The paper we propose to publish does not contain any identifying information, so no response the patients made can be attributed to any of the participants in the study.
Materials and methods
This was an observational cross-sectional study conducted between August 2010 and July 2011, at St Stephen’s Hospital, Delhi. Only mothers delivering normally with their babies roomed-in were invited to participate. Mothers who consented to participate were interviewed on each of the first 2 days after delivery to enquire about breastfeeding. The weight and sex of the baby, mother's education, history of previous births and socioeconomic status were recorded.
Mothers were administered EPDS on day 2.19 A Hindi translation of the EPDS was administered to mothers who preferred Hindi.20 This translation has been back translated and validated previously.21 The outcomes measured were EBF in the first 48 h and PND on EPDS.
Socioeconomic status was assigned grades 1–5 taking into account the skill levels and formal education using the ‘Major Groups and Skill Levels Classification’ of University of Warwick (table 1). International Standard Classification of Occupations (ISCO)-88 skill level 4 is considered grade 1 of socioeconomic status (academic), skill level 3 – grade 2 (vocational), skill level 2 – grade 3 (short education and skilled), and those not working (or semiskilled/unskilled) – grade 4.22
International Standard Classification of Occupations (ISCO)-88 major groups and skill level22
Education level was also graded as follows—grade 1: mothers who have not completed primary school education; grade 2: primary school graduates up to secondary school; grade 3: if they had passed up to higher secondary education; grade 4: college graduates and grade 5: mothers who have completed a postgraduate degree course.
Correlates of EBF were examined. The incidence of EBF in boys and girls was examined separately and also for primiparous mothers, separately from mothers who had had previous babies.
EPDS score in relation to sex of the child was also examined. Depression score above 11 on EPDS was considered as significant using a cut-off determined previously by Teissèdre.13 Pearson χ2 test was used to look for significance. OR and 95% CI of EBF were calculated. For proportions, 95% CI of the observed proportion is reported. Multiple regression analysis of correlates of EBF was also carried out. CI was calculated using the CIA software.23
Sample size calculation
We calculated that in order to get results that reflect the target population at the 95% CI with a margin of error of less than 2.5%, we would need to interview 1537 mothers.24
Results
During the study period 3466 babies were born at the hospital. There were only 792 girls for every 1000 boys. Among women delivering their first babies, there were 901 girls per 1000 boys. Among mothers delivering their second babies the sex ratio was 737 girls to 1000 boys. If first child was a girl the ratio in the second delivery fell to 632:1000, but if the first child was a boy the sex ratio in second children was 841:1000.
In total, 1537 mothers of singleton babies were enrolled in the study. The sex ratio in the study sample 797 girls per 1000 boys was similar to the sex ratio of overall deliveries. In total, 1026 mothers in the study group were exclusively breastfeeding their babies.
Babies with a birthweight 2.5 kg or heavier were more likely to be exclusively breastfed compared with those less than 2.5 kg (low birthweight; 68.2% vs 59.8%, p<0.01; figure 1). Multiparous mothers were more likely to be exclusively breastfeeding than primiparous mothers (71.6% vs 62.8%, difference=0.089, 95% CI 0.042 to 0.135).

Breastfeeding and birthweight (EBF, exclusive breastfeeding).
EBF was significantly higher among mothers of boys as compared with those of girls (70.8% vs 61.5%, p<0.001; figure 2). Gender of the baby had less influence on EBF of firstborn children. In total, 64.3% of primi boy babies and 61% of primi girl babies were exclusively breastfed (p=0.32). If the firstborn was a girl and the second baby was also a girl, 60% of the second children were exclusively breastfed compared with 77.3% if the second child was a boy (p=0.05). The chances of exclusively breastfeeding the baby were highest if there was a boy sibling in the family, 78.6% compared with 67.9% if there was no boy in the family (p<0.01; table 2).
Birth order two or more
Breastfeeding and sex of the child (EBF, exclusive breastfeeding).
No significant difference in EBF was found related to maternal age, socioeconomic status, maternal education and working status.
The EPDS score was significantly higher in mothers giving birth to a girl child (mean EPDS score 6.0±3.39 compared with 5.4±2.87, p<0.01). The depression score was significantly lower in mothers with at least one male child when compared with those with no male child (5.21±3.25 vs 5.9±3.2, p<0.01; table 2). Significantly more mothers of girl babies had an EPDS score higher than 11 compared with mothers of boys (9.7% vs 5.4%, difference in proportion=−0.045, CI −0.072 to −0.019).
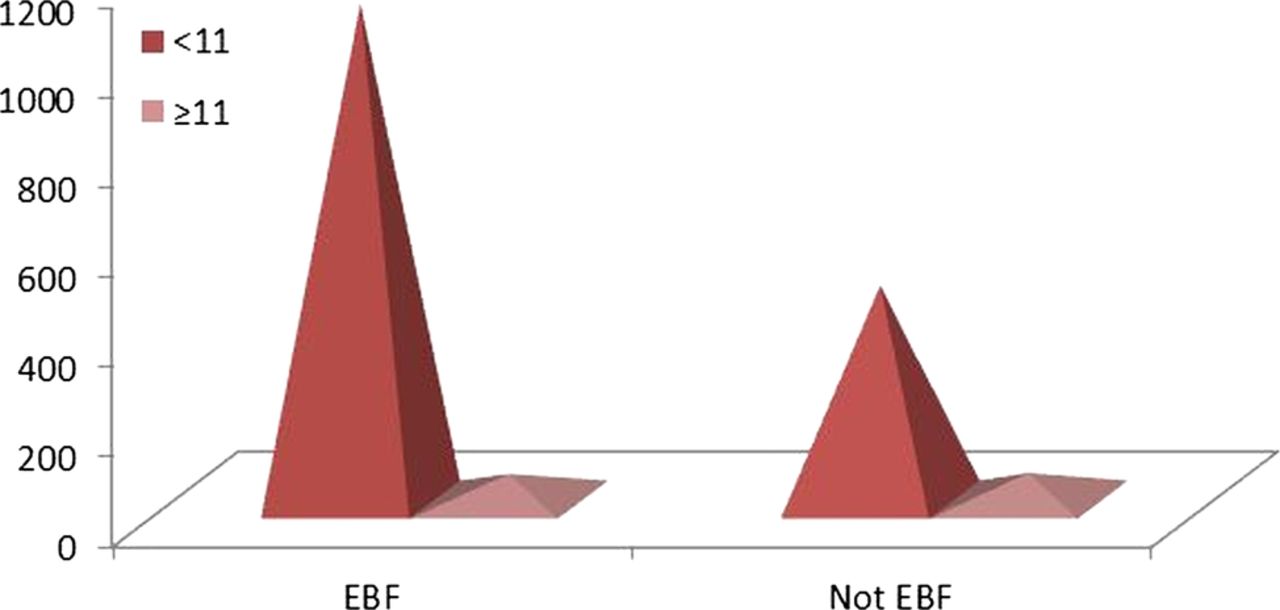
Higher EPDS score is associated with EBF rates. Only 52.4% mothers with a score ≥11 were exclusively breastfeeding compared with 67.8% in those with a score <11 (p<0.01; figure 3).

{kind=link}
{kind=link}
{kind=link}
Breastfeeding and postnatal depression (EBF, exclusive breastfeeding).
Multiple logistic regression analysis indicated that birth of a female baby (OR=0.69, 95% CI 0.56 to 0.87), high EPDS score (OR=0.53, 95% CI 0.36 to 0.80) and low birthweight (OR=0.72, 95% CI 0.55 to 0.95) are associated with lower odds of EBF. This analysis suggests that sex of the baby, EPDS score and birthweight are significant independent factors influencing EBF.
Discussion
Low female-to-male sex ratio is used as an index of sex bias in a community and can result from antenatal sex screening and selective abortion of female babies.25 In India, the male:female sex ratio is 914:1000. Sex ratio at birth is a better index of antenatal sex selection than the overall sex ratio.20 Previous studies have shown that sex ratio was particularly low in second children if the first was a girl.17 ,26
The same phenomenon was seen again in the fresh cohort studied here. The sex ratio in second order deliveries was 792 girls to 1000 boys but it was 632:1000 when the first child was a girl.
There was a male bias in breastfeeding too. More boys were being exclusively breastfed than girls. Jaychandran and Kuziemko hypothesise that since breastfeeding inhibits postnatal fertility, a mother might limit the nursing of an infant if she wants to continue having children. Mothers of girl children may want a boy soon and so may limit the duration of their feeding.18 Kimani et al27 also found sex of the child to be one of the factors for suboptimal breastfeeding in Kenya (n=4299).
Gender of the baby and PND
Our study found that depression score was higher in mothers of girls. The influence of gender of the baby on PND in mothers has been reported before. Adewuya et al28 in a study on Nigerian women found female sex of the baby was one of the predictors for PND (OR 2.74, CI 1.87 to 4.03). Chandran et al29 in Tamil Nadu, south India, showed that birth of a daughter, when a son was desired, was an important risk factor for depression. In a study of women in Iran also, gender of the child was found to be an important factor contributing to PND.30 Mothers who conceive a female fetus have higher levels of β-human chorionic gonadotropin. This along with other similar hormonal changes may be a biological explanation for the child's gender to affect PND.31 ,32 However this has not been elucidated clearly as yet.
Our study of EPDS was carried out on the second day after delivery. Mothers with low EPDS score could be those with postnatal blues and not all of them will have persistent PND. Only follow-up study will identify those with persistent PND. Our study protocol aimed at investigating early breastfeeding did not examine the issue of long-lasting depression in mothers of girl children.
PND and breastfeeding
We found that mothers with higher EPDS score were less likely to be exclusively breastfeeding. The effects of PND on EBF have been reported earlier. Dennis and McQueen33 also found that mothers with an EPDS score >12 at 1 week postnatal were significantly more likely at 4 and/or 8 weeks to discontinue breastfeeding, be unsatisfied with their infant-feeding method, experience significant breastfeeding problem and report lower levels of breastfeeding self-efficacy. In a cohort of 1745 Australian women it was found that the median duration of breastfeeding was 26 weeks for women with early-onset depression, 28 weeks for women with late-onset depression and 39 weeks for women without depression.34 Dennis and McQueen33 found maternal depression to be associated with delayed initiation and Ip et al8 found its association with early discontinuation of breastfeeding.
The birth of a girl child is associated with greater depression, and lower EBF in girls could be mediated by depression. To examine the effects of depression on EBF we studied EBF in mothers of girls who had a high EPDS score against those with a low score. We found that in mothers of girls with a higher depression score, only 47.7% were exclusively breastfeeding compared with 63% with low depression levels (difference in proportion=0.154, 95% CI −0.26 to −0.028; table 3). To look at the influence of sex of the child on EBF independent of associated depression, we performed multiple logistic regression analysis which showed that female sex of the child was independently associated with lower odds of EBF even after adjusting for depression. The comparison between the female OR in table 4 (0.66) and the one in table 5 (0.69) suggests that controlling for PND and birthweight does not affect the gender difference in EBF much.
Breastfeeding by EPDS and sex of child
Table showing correlates of exclusive breastfeeding and postnatal depression
Multiple logistic regression analysis
The results point to a pro-male gender bias. Mothers of girls may need more help to overcome PND and for improving breastfeeding rates. This in turn could enhance the survival of girl children and improve the sex ratio in the country.
This study does suffer from some shortcomings in as much as it was carried out in an urban hospital catering mostly to a middle-class clientele. The findings on sex ratio may therefore not be generalisable to other social groups. Studies in other populations are needed to confirm our findings.
We studied EBF in the first 48 h. More studies are needed to elaborate the effect of sex bias on the duration of breastfeeding.
We studied the EPDS score in mothers within 48 h of delivery. Many of those with high scores may be suffering from postnatal blues rather than full-fledged PND. Further studies performed later in the postnatal period need to be carried out to examine how many of these mothers with high initial scores have longer lasting PND. Although multiple regression analysis shows that higher depression score and female sex of the child are associated with lower odds of EBF, a causal relationship is not implied.
In India the sex ratio is affected by antenatal sex determination and sex-selective feticide.25 High rate of sex-selective abortion may complicate the interpretation of results.
References
Footnotes
-
Contributors AJ conceived the research project with JP. AJ collected the data. VS helped with the analysis of data and statistics. PK and PT helped with the write-up and review of literature.
-
Funding This research received no specific grant from any funding agency in the public, commercial or not-for-profit sectors.
-
Competing interests None.
-
Ethics approval St Stephen's Hospital Ethics Committee.
-
Provenance and peer review Not commissioned; externally peer reviewed.
-
Data sharing statement Original mastersheet containing anonymised patient data is available with the author and can be provided to anyone requesting the same.