Article Text

Abstract
Introduction The benefits of physical activity for people with multiple sclerosis (pwMS) have been recognised. However, exercise regimens can be difficult to maintain over the longer term and pwMS may face unique barriers to physical activity engagement. Pilot research suggests the Nintendo Wii can be used safely at home by pwMS with minimal mobility/balance issues and may confer benefits. We have developed a home-based physiotherapist supported Wii intervention (‘Mii-vitaliSe’) for pwMS that uses commercial software. This is a pilot study to explore the feasibility of conducting a full scale clinical and cost-effectiveness trial of Mii-vitaliSe.
Methods and analysis 30 ambulatory, relatively inactive pwMS will be randomised to receive Mii-vitaliSe immediately, or after 6 months. Outcomes, measured at baseline and 6 and 12 months later, will include balance, gait, mobility, hand dexterity and self-reported physical activity levels, fatigue, self-efficacy, mood and quality of life. Interviews conducted on a purposive sample of participants will explore experiences of participation in the study and barriers and facilitators to using the Wii. Mean recruitment, adherence rate and standard deviations (SDs) of potential primary outcomes for the full trial will be estimated and precision summarised using 95% confidence intervals (CIs). Interview transcripts will be thematically analysed using a generic qualitative approach.
Ethics and dissemination National Health Service (NHS; ref 12/SC/0420) and university ethical approvals have been obtained as has NHS Research and Development permission from the relevant trust. A home risk assessment will be undertaken for all potential participants. All adverse events will be closely monitored, documented and reported to the study Safety Monitoring Committee. At least one publication in a peer reviewed journal will be produced and research findings presented at a national and international conference. With service users, we will coproduce a summary of the findings for dissemination on our research unit's website and elsewhere.
Trial registration number ISRCTN 49286846.
- Rehabilitation Medicine
This is an Open Access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/
Statistics from Altmetric.com
Strengths and limitations of this study
-
This pilot study will include a long-term (1 year) follow-up to consider adherence.
-
The intervention will incorporate individual tailoring, behavioural change strategies and home-based Wii use with physiotherapist guidance.
-
Mixed methods will be used.
-
Physical outcome assessments will not be blinded.
Introduction
Historically, people with multiple sclerosis (pwMS) have been advised to limit physical activity levels. However, over the last decade the salutary effects of exercise for pwMS have become evident,1–5 with no deleterious effects described.1 ,6–9 Physical activity has been shown to be associated with improvements in mobility, muscle strength and physical fitness.1 ,9–14 In a meta-analysis, planned and structured regular exercise was associated with a small improvement in quality of life (QoL) in MS.15 Other secondary benefits might include reduced fatigue, depression and anxiety and improved sense of well-being—although more rigorous trials are needed.14 ,16 Early intervention may help to slow or prevent the accumulation of physical disability.17 ,18
However, pwMS typically engage in dramatically lower levels of physical activity than the general population.2 ,4 ,19 This can lead to a downward spiral of deconditioning, fatigue, reduced self-efficacy, increased levels of disability4 as well as increased health risks (such as cardiovascular diseases, obesity, diabetes, etc). Psychosocial repercussions include reduced leisure, social contacts, role fulfilment and engagement in activities of daily living; all important for self-esteem and psychological well-being.
People with long-term disabling conditions such as MS face unique barriers to participation in physical activity20–28 including physical (eg, pain, fatigue, mobility limitations and overheating), psychological (eg, fear, embarrassment and lack of confidence) and environmental (transport, cost, lack of suitable facilities/trained staff) factors. While home-based activities overcome some of these, adherence to traditional exercise programmes is poor.29 Making exercise an enjoyable experience30–32 undertaken in a non-threatening and comfortable environment along with the provision of detailed guidance, monitoring and support may improve adherence.2 ,30 ,32 ,33
The National Institute for Health and Care Excellence (NICE) guidelines, the National Service Framework for long-term conditions and the Health Foundation highlight the importance of guided tailored self-management supported by health professionals34–38 to encourage engagement in physical activity and leisure and social pursuits.
Physical activity is multifaceted and psychological factors play a crucial role in its initiation and maintenance. Adopting a multidisciplinary approach can help to support behaviour change and physical activity prescription. Social Cognitive Theory39 and in particular, the concept of self-efficacy40 ,41 has been proposed as a key mediator in the promotion and maintenance of physical activity42 ,43 and adherence32 ,44–46 and an important predictor of health status.47
The Wii overcomes some of the barriers to participation in physical activity highlighted earlier. It is low cost, can be used at home, and has broad appeal, incorporating variables known to enhance motivation, self-efficacy48 and adherence (such as self-monitoring, prompts, peer comparison and feedback about progress and performance) in the context of fun49–52 purposeful tasks.53 It offers opportunities for socialisation across the lifespan54 ,55 and participation in immersive virtual reality activities that might, in real life, be challenging due to physical limitations, or require further adaptation to enable participation (eg, golf). Games such as Wii Sports use significantly more energy than sedentary activities56–60 (though not as much as playing the sport itself).57 ,58
For the current study the Wii was deemed preferable over other newer more complex virtual reality platforms, such as the Xbox Kinect: it is low cost, requires less space, permits support from a therapist within the field of view and the Wii sensors are relatively ‘forgiving’ thereby facilitating use by people with impaired or compromised movement.61 Our findings will, nevertheless, have applicability to and relevance for other platforms and chronic conditions.
In conjunction with the Wii balance board, the Wii Fit Plus incorporates games requiring the user to shift his/her weight from side to side and forwards and back to control gameplay. A key feature of these systems is the provision of dynamic visual feedback about centre of gravity allowing training and adjustments of movement via biofeedback techniques. These recent advances in interactive gaming have created the potential for increasing physical activity and decreasing sedentary behaviour.62 It has been suggested that such games may be helpful for improving balance and core strength63 under the guidance of a qualified health/rehabilitation professional (who can advise on the selection of appropriate activities to challenge balance safely and gradually).
Wii games can be played for brief periods, at the individual’s convenience. Daily activity levels can be accumulated in short bouts of 10 min or more throughout the day (which is thought to be as effective as all in one go43 ,64), at differing levels, and a range of activities can be selected, depending on current symptoms65 and preferences. Creating a personalised representation of oneself (a ‘Mii’) may enhance self-efficacy via a greater sense of ‘presence’ and motivation.66
However, there are potential disadvantages. As with other physical activities, playing the Wii could lead to injury, discomfort67 ,68 or increased symptoms. Many of the reported injuries have been due to people exercising beyond their limitations and without resting adequately. The user manual69 provides guidance on how to use the Wii safely and onscreen prompts about resting are regularly provided. As the Wii software has been developed with a healthy population in mind, it is important to explore its acceptability to pwMS.70
While applications of the Wii are diverse71–82 and preliminary findings positive, the evidence base is limited and definitive answers require well-designed randomised controlled trials (RCTs). In this pilot study, we wish to explore whether a commercially available interactive gaming system, the Nintendo Wii, offers a safe, feasible way to provide opportunities in the home for increased physical activity for pwMS (which could lead to improvements in domains such as vitality, balance, mobility, QoL and well-being). To date, Wii research with people affected by MS is mostly preliminary. Early findings are promising, however, and suggest that the Wii might be helpful for balance83–85 and fitness.86
In a non-randomised pilot study Plow and Finlayson,86 found that pwMS who have mild balance and mobility limitations can use the Wii Fit safely at home. However, they also reported that Wii use declined after 3 months. They suggested that a more person-centred approach as well as the use of behavioural change techniques (such as motivational interviewing and problem solving) might help to promote longer term Wii use and foster intrinsic motivation. In a scoping review of the exergaming literature Plow et al87 recommended that trials incorporate longer term follow-up periods, employ mixed methods and follow patients from the clinical setting to the home. Others have suggested that an individualised approach is essential to take into account individuals’ beliefs, self-efficacy and perceptions about exercise31 and their self-identity, goals and expectations for improving health.70 ,88
Often research projects proceed rapidly to a full scale RCT, with vital, preparatory phases overlooked.89 This can result in a resource intensive and costly analysis of a conceptually or clinically flawed intervention. In this study, we have consulted with pwMS already using the Wii, and adapted existing guidance on using the Wii to develop a home-based physiotherapist supported Wii intervention for pwMS (Mii-vitaliSe). We will undertake a small pilot RCT of the Mii-vitaliSe intervention to explore the feasibility of a full-scale formal evaluation of effectiveness.90
Methods
Aim
To investigate the feasibility of conducting a multicentre definitive RCT to assess the clinical and cost-effectiveness of a home-based physiotherapist supported Wii intervention (Mii-vitaliSe) for pwMS.
Objectives
-
Test procedures (including administration of the self-reported outcomes and the physical assessments, delivery of the intervention, recording and monitoring of adverse events (AEs)), estimate recruitment and retention rates, and refine the selection of outcome measures in preparation for a definitive RCT to test the effectiveness of Mii-vitaliSe.
-
Collect data on the variability of outcome measures to inform a sample size calculation for a larger trial.
-
Estimate adherence rates via a self-reported daily play log (in terms of frequency, intensity, duration).
-
Determine the acceptability of randomisation and of the Mii-vitaliSe intervention to participants and obtain information about patterns of use/barriers to use.
-
Gather feedback from physiotherapists about their experiences of delivering Mii-vitaliSe.
Study design
A single centre wait-list controlled pilot study of Mii-vitaliSe plus usual care versus usual care alone (see figure 1) will be undertaken. Participants will be randomised to receive Mii-vitaliSe immediately or after 6 months (‘delayed’ group). The delayed group will continue their usual routines and receive the Mii-vitaliSe intervention after a 6-month delay. During this period, they will be asked to refrain from using the Wii and will act as controls for the immediate group.

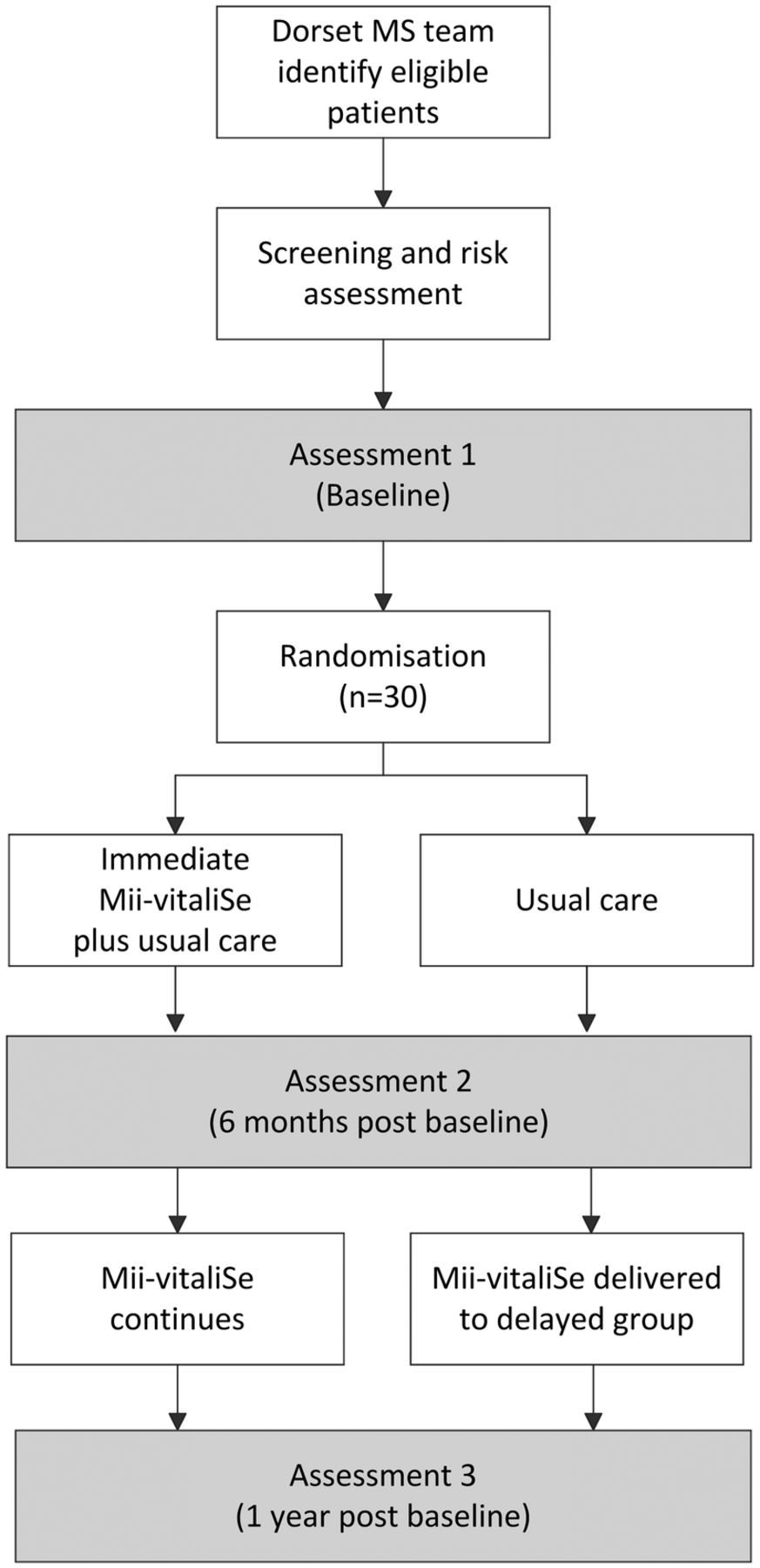{kind=link}
Mii-vitaliSe study flow chart.
This design has the potential to minimise the impact of disappointment that those allocated to a non-intervention group might experience, while ensuring those in the delayed group receive the full intervention with an emphasis on safety aspects. Delivering the intervention to those in the delayed group may increase compliance with refraining from use for a 6-month period. This design also permits a preliminary consideration of long-term (1 year) follow-up (immediate group only). The randomised controlled component allows testing of procedures, design, etc in preparation for a full scale trial. Follow-up periods are sufficient for novelty value to diminish and patterns of use to be established.
Service user involvement
Following INVOLVE principles,91 services users have been involved in all stages of the research so far, including the development of this protocol. A service user consultation was held to inform the content and format of the Mii-vitaliSe materials and aspects of the study design. Service users will be represented on the trial steering group and will continue to provide ongoing input into the study.
Data protection and data storage
All information collected during the course of the study will be kept strictly confidential and any information that leaves Poole Hospital/Bournemouth University will contain no personal details. Questionnaires will be allocated a participant ID; they will not contain names or any identifying details. Only authorised members of the research team will have access to the study data.
Data will be collected and retained in accordance with the Data Protection Act 1998. Study documents (paper and electronic) will be retained in a secure location during and after the trial has finished. All source documents will be retained for a period of 5 years following the end of the study.
Compliance
The Chief Investigator will ensure that the study is conducted in compliance with the principles of the Declaration of Helsinki (1996) and in accordance with all applicable regulatory requirements including, but not limited to, the Research Governance Framework and Trust policies and any subsequent amendments.
Sample size considerations
A ‘rule of thumb’ of 30 is common for pilot studies.92 A sample size of 30 (15 in the immediate and 15 in the delayed arm) will be adequate given the specific quantitative aims of this pilot.
Objective 1 is to estimate the recruitment rate to help in planning recruitment for a full scale RCT. Precision of this estimate will be based on the width of the 95% CI. With a total sample size of 30 people recruited, the recruitment rate will be estimated with a precision of ±11% (assuming a recruitment rate of approximately 40% based on experiences of running a RCT of a fatigue management programme for pwMS93).
Objective 2 is to estimate the SD of potential primary outcome measures in preparation for a formal sample size calculation for a larger RCT. Assuming these outcomes are standardised, so that they have a SD of 1, the precision (as summarised by standard error) will be 0.13. When using this estimate for a later sample size calculation it will be inflated as suggested by Browne.94 Estimating the effect size for the Mii-vitaliSe intervention is not an aim of this pilot, but would be the aim of a later full scale RCT.
Objective 3 is to estimate the degree of adherence of participants to Mii-vitaliSe. For each individual this will be summarised as the number of days on which activities were performed divided by the number of days agreed with the physiotherapist in their action plan. The potential range is 0–1, and the SD will be at most 0.17 (NQuery Advisor). With a sample size of 30, average adherence will be estimated with precision ±0.06 (ie, width of 95% CI).
Participants
Thirty ‘inactive’ (see eligibility criteria) pwMS aged 18 or over, will be recruited from the Dorset MS Service. Individuals excluded from the research project will continue to be seen as per usual care.
Eligibility criteria
Inclusion criteria
-
Clinically definite diagnosis of MS
-
Aged 18 or above
-
Fulfil home risk assessment criteria (see below)
-
‘Inactive’ (physically active on fewer than 5 days/week for ≥30 min)
-
Living within Poole/Bournemouth conurbations
-
Suitable television
Exclusion criteria
-
Have only mild symptoms (equivalent to an Adapted Patient Determined Disease Steps (APDDS) Scale95 score of 1) or require at least intermittent or unilateral constant assistance (cane, crutch or brace) to walk 100 m with or without resting (equivalent to an Expanded Disability Status Scale (EDSS) score96 of 6 or more)
-
Relapse within the past 3 months requiring corticosteroids
-
Already participating in exercise/rehabilitation research
-
Any medical condition placing participant at risk from exercise participation/using Wii
-
Owns a Wii and uses it regularly (weekly or more)
-
Unwilling/unable to comply with protocol
Risk assessment
This will be undertaken at home by the study researcher (who is a senior physiotherapist) to assess balance on the Wii balance board and the suitability of the home environment for setting up the equipment and using the Wii.
Participants will be considered eligible if:
-
They can maintain independent standing balance with eyes open for 1 min.
-
The physiotherapist clinically judges that they demonstrate adequate balance reactions while on the Wii balance board97 and are able to step off safely forwards, backwards and sideways.
-
Their home environment is suitable (with minor modifications, if appropriate and possible).
Identification and recruitment
Recruitment will be via the Dorset MS Service. Potential participants will be identified by the multidisciplinary Dorset MS team. A member of the MS team will go through a screening checklist to identify potential participants and will then either send or give them an invitation letter with a simple one-page summary (‘Key Facts’) about the study, participant information sheets, the APDDS Scale, a question about current levels of physical activity and a reply slip and pre-paid return envelope. Participants will be asked to return the reply slip and their responses if they wish to find out more about the study. A follow-up reminder letter with another copy of the information pack will be sent if a reply is not received within 2 weeks.
Screening procedure
The study researcher will telephone those who have expressed an interest in the research, describe the study in more detail, answer questions and go through the remaining screening criteria (see section ‘Exclusion criteria’) over the telephone. Those not eligible will be informed over the telephone. Individuals who fulfil the study criteria will be visited at home for the risk and home suitability assessment. Minor modifications to the home environment to facilitate the safe use of the Wii balance board will be discussed with the potential participant and documented.
Individuals not eligible to take part will continue to be seen as per usual care.
Informed consent process
Informed consent will be taken by the Good Clinical Practice (GCP) accredited study researcher in individuals’ homes, providing they satisfy the risk and home assessment criteria.
Randomisation
To ensure good allocation concealment, random allocation will be email based and administered by the study statistician. Randomisation will be carried out on a 1:1 basis and will utilise a computer-based random sequence generator. Variable-sized blocks will be used to ensure approximately equal numbers in the two trial arms. No stratification will be used.
Outcome measures
As this is feasibility work, a broad range of outcomes has been included. Participants will be requested to complete the outcomes even if they stop using the Wii. A detailed description of outcome measures is included in the web supplement.
Outcomes will be assessed at baseline and at 6 and 12 months. Physical assessments (administered at similar times of the day to reduce the confounding effect of fatigue98) will be undertaken at the hospital by the study researcher and a clinical scientist. Self-reported questionnaires (presented in a large font) will be completed by participants in their homes, at their own convenience and pace.
Demographic/descriptor variables
Age, sex, education, employment, marital status, ethnicity, household composition, time since diagnosis, disease course, relapse history, medication, comorbidities.
Adverse events
Defined as any undesirable outcome, such as injury, falls, discomfort, pain, relapse. These will be recorded and reviewed by an independent Safety Monitoring Committee (comprising a neurologist and a physiotherapist).
Balance, gait mobility
Hand dexterity/coordination
-
Nine-hole peg test108
Self-efficacy
Psychological well-being and QoL
Adherence
Measuring adherence is challenging117 ,118 and while some have relied on the data captured by the Wii console, this approach is problematic (eg, other family members could use a participant's Mii). In this study, adherence will be defined as the total number of days on which activities are performed divided by the number of days agreed with the physiotherapist in the action plan. We will also collect information related to duration and intensity119 ,120 as well as the data stored on the Wii console.
Process measures
-
Daily play log (date/time, whether played, AEs (eg, pain, tenderness, soreness, fatigue, dizziness, headaches, aching, stiffness, falls), activity, duration, intensity,119 ,120 enjoyment, fatigue, reasons for non-use, free-text comments).
-
Physiotherapist feedback: Participant contacts will be recorded using a template. At the end of the intervention period the physiotherapists will be interviewed about the ease of delivering the intervention and any problems encountered.
-
Semistructured interviews will be conducted (at home/via telephone) on a purposive sample of participants selected to represent factors pertinent to expectations/experiences of participating in the study and receiving Mii-vitaliSe (such as age, gender, employment status, disease severity, prior experience of home console systems). These will comprise 50% of participants from each group at the 6-month follow-up and at the 12-month follow-up, the ‘immediate’ group only.
Health utilisation
Economic evaluation would be an important component of future research. We will pilot an existing measure of healthcare utilisation developed for a RCT of a fatigue management programme.93 We will provide participants with a resource use log to aid completion of the questionnaire.
Mii-vitaliSe intervention
Drawing upon a literature review, existing materials121–125 and our knowledge of best practice in physiotherapy and psychological interventions in MS, guidance and resource materials for using the Wii were developed. The research team worked in partnership with a service user panel (8 patients from the Dorset MS Service with experience of using the Wii and familiarity with the Wii Sports and Wii Fit Plus software). A workshop was held to discuss the Mii-vitaliSe intervention. The following aspects were discussed:
-
Safety aspects, patterns of usage, benefits/drawbacks, problems identified and whether/how they could be overcome.
-
Factors contributing to longer term use.
-
Feedback about the Wii Sports and Wii Fit Plus software.
-
Which outcome domains are most relevant/meaningful to service users.
-
Feedback on the format and content of a draft daily play log.
After an iterative process of revision, LF and ST produced a set of materials to be used as part of a physiotherapist-supported home-based Wii intervention (Mii-vitaliSe). These include:
-
General information about the Wii and Mii-vitaliSe;
-
Safety and technical information;
-
Guidance on warm up/cool down exercises;
-
A guidance book and personal activity workbook;
-
Games descriptors for Wii Sports, Wii Sports Resort and Wii Fit Plus;
-
Tips on goal-setting and overcoming barriers;
-
Signposts to useful resources (eg, websites, forums);
-
Quotations from pwMS who attended the consultation workshop about their experiences of using the Wii.
The Mii-vitaliSe intervention is underpinned by principles of self-management, social cognitive, motivational interviewing and cognitive behavioural theories. It incorporates a workbook to enable individually tailored goal setting, monitoring and the identification of facilitators and barriers to engagement with Mii-vitaliSe.
Mii-vitaliSe intervention
Session 1: Orientation to the Wii in the hospital setting (week 1)
The physiotherapist goes through the guidance book with the participant to cover:
-
The benefits of physical activity
-
A practical demonstration of using the software (Wii Sports, Wii Sports Resort and Wii Fit Plus) safely
-
Creating a ‘Mii’
-
Familiarisation with the controls
Session 2: Training and individualised assessment in the hospital setting (week 2)
Participants will be guided through warm up/cool down exercises and given the opportunity to try out activities safely under supervision. The physiotherapist and participant will discuss appropriate activities, taking into account physical capabilities, and personal preferences.
Session 3: Installation of Wii at home and starting individual programme (week 3)
The physiotherapist will install the Wii equipment in participants’ homes to interface with their television. Participants will be provided with Wii Sports, Wii Sports Resort and Wii Fit Plus, asked to use their Mii when playing, and to log any other software used via the daily play log. The physiotherapist will reiterate safety advice (eg, the importance of the safety strap, taking a graded approach and frequent rests, etc). The physiotherapist will agree an individualised programme with the participant, indicate ways this could be progressed and provide guidance on keeping the daily play log and on setting/recording goals.
Ongoing support and monitoring
This will be followed by independent home use supported by a combination of telephone support (week 5—to identify and resolve any early difficulties encountered; week 12 to encourage progress, support people to overcome any barriers) and home review visits (weeks 7 and 16) at which the physiotherapist will reassess the individual and provide support and discuss possible progression/modification of the activities. Thereafter, ongoing monitoring, support and encouragement will be provided via monthly contact (phone/email) from the physiotherapist.
Usual care
The Dorset MS service offers pwMS multidisciplinary support. Patients are reviewed annually by the team at an outpatient clinic or home visit appointment. This includes a medical review by a neurologist and specialist MS nurse and a therapy review by a physiotherapist and occupational therapist. On completion of the review and necessary assessments, medical and therapy treatment is modified as required. If patients experience a deterioration of their symptoms before the next review they can self-refer to the service. This may take the form of advice regarding relapse management or specific intervention.
The team operates a help-line between 9:00 and 11:00 Monday to Friday and there is an answer-phone out of hours. The team is available to discuss problems with patients and action appropriate treatments in a timely way. If therapy is required (occupational therapy/physiotherapy) this is offered by the MS specialist therapists and patients can be assessed and treated at home, as an outpatient, in work or a gym environment. Education, support and advice regarding disease modifying therapies, management of symptoms and carer support is available from the specialist nurse.
Statistical analysis
Recruitment and retention rates for the study and SDs of potential primary outcome measures will be estimated, and precision summarised using 95% CIs. For each individual, adherence will be summarised ((the number of days on which activities were performed divided by the number of days recommended by the physiotherapist)×100%). These data will be collected via participant-completed daily play logs. We will estimate mean adherence (%) in the first 6 months of using the Wii by combining data from months 1–6 for the immediate group and months 7–12 for the delayed group. We will estimate adherence in the second 6 months of using the Wii using data from months 7–12 in the immediate Wii group.
We will develop and test out data analysis procedures in preparation for developing a statistical analysis plan for a later RCT. This will involve (1) capitalising on the randomised nature of the study by comparing outcomes between study arms at 6 months (in months 1–6 the immediate Wii group will have been using the Wii, and the delayed group will not have been using the Wii), (2) analysing within person change over 6 months of using the Wii (ie, months 1–6 in the immediate group and months 7–12 in the delayed group) and (3) analysing within person change over 12 months of using the Wii (ie, months 1–12 in the immediate group).
Qualitative analysis
The interviews will be recorded, transcribed and thematically analysed using a generic qualitative approach126–131 and involving inter-researcher and service user interpretation/discussion. Free-text comments in the daily play logs will be collated and summarised. Themes developed will inform the design of a future trial and the selection of outcome measures.
Participant withdrawal from study and/or from research follow-up
If a participant withdraws from the study, the study researcher will be informed and will contact the participant. Provided the participant is willing to give a reason, the study researcher will find out why he/she wishes to withdraw from the study. The study researcher will also determine whether he/she wishes to continue to be included in the research follow-up or wishes to withdraw. If the participant wishes to withdraw from the research follow-up the study researcher will determine whether he/she gives permission to retain data collected before withdrawal for use at final analysis, or whether this information should be destroyed. No data will be used in the analysis without a participant's consent.
Adverse events
All AEs and their possible relation to the Mii-vitaliSe intervention will be closely monitored, documented and reported to the study Safety Monitoring Committee. The Safety Monitoring Committee will consider the events and offer advice to the project team. Participants will be asked to report all AEs related to use of the Wii to either the physiotherapists delivering Mii-vitaliSe or to the study researcher. These will be recorded on a case report form. In addition there will be a section on the daily play log to record AEs (including pain, tenderness, soreness, fatigue, dizziness, headaches, aching, stiffness, nausea, falls or near falls). The physiotherapists will ask participants whether they have experienced any AEs related to using the Wii in their monthly monitoring phone calls. The Dorset Multiple Sclerosis team will notify the research team of any AEs that become known to them.
The Chief Investigator will assess an AE to establish if it should be classified as a Serious Adverse Event (SAE) according to the National Research Ethics Service definition. If the AE is not defined as ‘serious’, it will be recorded in the study site file and the participant will be followed up by the research team. The AE will be documented in a participant's MS Service notes (where appropriate). Reports of related and unexpected SAEs will be submitted to the Research Ethics Committee within 15 days of the CI becoming aware of the event, using the ‘Report of SAE form for non-CTIMPs’ (V.3, April 2007), published on the NRES website. The sponsor will be notified within 24 h.
Project management and safety monitoring
The study researcher will deal with the day-to-day management and coordination of the study and will call on other members of the project team as appropriate. The Chief Investigator will be responsible for the overall management of the project. The CI, study statistician, and study researcher will have regular meetings to discuss study progress. The study steering group will meet twice yearly to monitor progress. A Safety Monitoring Committee comprising two independent advisors (a neurologist with expertise in MS and clinical trials and a physiotherapist with expertise in risk assessment and management of service users with neurological disability) will review any AEs and make recommendations to the study steering group (eg, adapting the protocol/stopping the study, as necessary).
Monitoring and audit
The study will be monitored and audited in accordance with Poole Hospital NHS Foundation Trust (PHFT) policy. All trial related documents will be made available on request for monitoring and audit by PHFT and the Research Ethics Committee. Regular meetings will take place with the study monitor.
Ethical considerations and dissemination
The study has been reviewed and given a favourable opinion by the National Health Service (NHS) South Central Hampshire B Research Ethics Committee (ref: 12/SC/0420). Poole Hospital NHS Foundation Trust is acting as the sponsor. The study will be performed subject to Research Ethics Committee (REC) approval, including any provisions of Site Specific Assessment (SSA), and local Research and Development (R&D) approval. This study will be conducted in accordance with the Research Governance Framework for Health and Social Care and GCP.
It is likely that majority of the participants in the study will have fatigue, and so we will try to minimise the impact that participation in the study has on their fatigue (eg, by staggering questionnaire load and providing a refreshment break during the physical assessments, offering taxi transport to the hospital).
We aim to disseminate the results of this research working closely with service user partners and the funder. It is anticipated that at least one publication in a peer reviewed journal will be produced and we intend to present the findings at a national and international conference. In collaboration with our service users we will produce a short report suitable for the general public. Further dissemination to pwMS will be via our unit's website, the Wiihabilitation website and (with their permission) MS charities and the Chartered Society of Physiotherapy. We also plan to disseminate findings via press releases and social media.
Discussion
This pilot study will assess the acceptability and suitability of a home-based physiotherapist supported Wii intervention (Mii-vitaliSe) to increase activity levels in pwMS. Mii-vitaliSe addresses limitations highlighted in the literature by incorporating home-based activity, behavioural change principles, employing mixed methods and including a long term follow-up period. Findings from this study will establish whether a full scale RCT is feasible and, if supportive of proceeding to a full trial, will inform its design and conduct. The decision on whether to progress to a full trial will be made by the trial steering group. No specific criteria have been set. If found to be effective in a full trial, Mii-vitaliSe could increase activity levels in a group of people known to have low activity levels overall and could be readily implemented in a healthcare system such as the NHS. Technological developments in this field are ongoing with rehabilitation software currently being developed for the Nintendo Wii and other platforms. The general principles and findings from this research will have relevance for the next generation of software and platforms and also for other chronic conditions.71 ,87
Acknowledgments
The authors would like to thank the individuals who attended the patient and public involvement (PPI) workshop to inform the development of the Mii-vitaliSe intervention. They also thank Mrs Jo Hickson and Mrs Kelly Saunders for attending the PPI workshop, for providing invaluable feedback about draft Mii-vitaliSe materials and the physical assessment protocol and for agreeing to be members of the study steering group. The authors also thank Dr Kate Jupp and Dr Mark Cossburn for agreeing to be members of the study Safety Monitoring Committee. They thank Dr Delva Shamley for commenting on an early version of the protocol.
References
Supplementary materials
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
Files in this Data Supplement:
- Data supplement 1 - Online supplement
Footnotes
-
Contributors ST, PT, CH, SC and SB were involved in the conception of the study and ST and PT led the design. ST with PT wrote the initial grant application and protocol. CH, SC and SB advised on clinical aspects related to the grant application, SP led the medical physics component of the study, RS advised on technical aspects and KG advised on qualitative aspects. LF refined aspects of the draft protocol as part of her PhD studies. ST drafted the manuscript, LF and PT provided detailed feedback and all other authors critically reviewed and approved the final version.
-
Competing interests PT is a member of the MS Society Grant Review Panel for Care and Services Research. PT is also a member of the Advisory Board for the Sativex Registry. The Board provides an independent review of safety data for patients prescribed Sativex. Bournemouth University receives a fee from GW Pharma to cover time spent at meetings, and travel expenses.
-
Funding The study is funded by a project grant awarded by the Multiple Sclerosis Society in the UK (ref no. 933/10). The study is included in the National Institute of Health Research Clinical Research Network (NIHR CRN) portfolio (ID 13130).
-
Ethics approval NRES Committee South Central—Hampshire B (ref 12/SC/0420).
-
Provenance and peer review Not commissioned; peer reviewed for ethical and funding approval prior to submission.