Article Text

Abstract
Objectives Treatment decision-making in colorectal cancer is often guided by tumour tissue molecular analysis. The aim of this study was the development and validation of a high-resolution melting (HRM) method for the detection of KRAS, NRAS and BRAF mutations in Greek and Romanian patients with colorectal cancer and determination of the frequency of these mutations in the respective populations.
Setting Diagnostic molecular laboratory located in Athens, Greece.
Participants 2425 patients with colorectal cancer participated in the study.
Primary and secondary outcome measures 2071 patients with colorectal cancer (1699 of Greek and 372 of Romanian origin) were analysed for KRAS exon 2 mutations. In addition, 354 tumours from consecutive patients (196 Greek and 161 Romanian) were subjected to full KRAS (exons 2, 3 and 4), NRAS (exons 2, 3 and 4) and BRAF (exon 15) analysis. KRAS, NRAS and BRAF mutation detection was performed by a newly designed HRM analysis protocol, followed by Sanger sequencing.
Results KRAS exon 2 mutations (codons 12/13) were detected in 702 of the 1699 Greek patients with colorectal carcinoma analysed (41.3%) and in 39.2% (146/372) of the Romanian patients. Among the 354 patients who were subjected to full KRAS, NRAS and BRAF analysis, 40.96% had KRAS exon 2 mutations (codons 12/13). Among the KRAS exon 2 wild-type patients 15.31% harboured additional RAS mutations and 12.44% BRAF mutations. The newly designed HRM method used showed a higher sensitivity compared with the sequencing method.
Conclusions The HRM method developed was shown to be a reliable method for KRAS, NRAS and BRAF mutation detection. Furthermore, no difference in the mutation frequency of KRAS, NRAS and BRAF was observed between Greek and Romanian patients with colorectal cancer.
- Molecular Biology
This is an Open Access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 3.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/3.0/
Statistics from Altmetric.com
Strengths and limitations of this study
-
This is a single-centre study that used a cohort of unselected Greek and Romanian patients with colorectal cancer.
-
We developed and validated a new fast and reliable HRM analysis protocol for KRAS (exons 2, 3 and 4), NRAS (exons 2, 3 and 4) and BRAF (exon 15) mutation detection.
-
The mutation frequency of KRAS, NRAS and BRAF was determined for the first time in Greek and Romanian populations.
-
The main limitation of the study was that not all the epidemiological data were collected.
Introduction
The RAS proto-oncogenes (HRAS, KRAS and NRAS) encode a family of highly homologous proteins. They participate in a signal transduction cascade, namely the RAS/RAF/MEK/ERK pathway, which regulates the growth and survival properties of cells. They are controlled by extracellular signals transmitted by the transmembrane receptor tyrosine kinase and epidermal growth factor receptor (EGFR).1
Two monoclonal antibodies (cetuximab and panitumumab) were designed as effective inhibitors of the EGFR. However, anti-EGFR therapy is not effective in patients harbouring activating mutations in genes of the RAS/RAF/MEK/ERK pathway.2
In total, activating mutations in the RAS genes, mainly in exons 2 and 3 (codons 12/13 and 61), occur in approximately 20% of all human cancers. Mutations in KRAS account for about 85% of all RAS mutations in human tumours, NRAS for about 15% and HRAS for less than 1%.1 Acquired mutations in exon 2 of the KRAS gene (at codons 12/13) are commonly used to identify patients with colorectal cancer who are unlikely to benefit from anti-EGFR therapy. However, more than half of patients with KRAS codons 12/13 wild-type colorectal cancer still fail to respond to anti-EGFR therapy, suggesting the involvement of mutations at other locations of the gene or other genes that act downstream of EGFR in the RAS/RAF/MEK/ERK pathway.3
Recent studies showed that mutations in exons 3 and 4 of KRAS, exons 2, 3 and 4 of the NRAS gene and exon 15 of the BRAF gene are associated with poor prognosis or resistance to anti-EGFR antibody in metastatic colorectal cancer.4–7 Additionally, it has been reported that patients harbouring any activating RAS mutations not only do not benefit from but may be harmed by panitumumab–FOLFOX4 treatment.6
High sensitivity and specificity are pre-requisites when selecting the appropriate method for somatic mutation detection. High-resolution melting (HRM) curve analysis is considered an accurate, fast and sensitive method that can be used for hereditary or somatic mutation screening.8 The HRM melting profile is a specific sequence-related pattern allowing discrimination between wild type sequences and homozygote–heterozygote variants. Since it is a more sensitive approach compared with direct sequencing, it allows the detection of even a minimal fraction of mutated cells.9 This is important when dealing with somatic mutations, where the percentage of mutant alleles in the DNA analysed can be very low in some cases.
The aim of this study was the development and validation of an HRM method for the detection of KRAS, NRAS and BRAF mutations in colorectal patients. Additionally, we aimed to compare for each one of these genes mutation frequency in Greek and Romanian patients with colorectal cancer.
Methods
Samples and DNA extraction
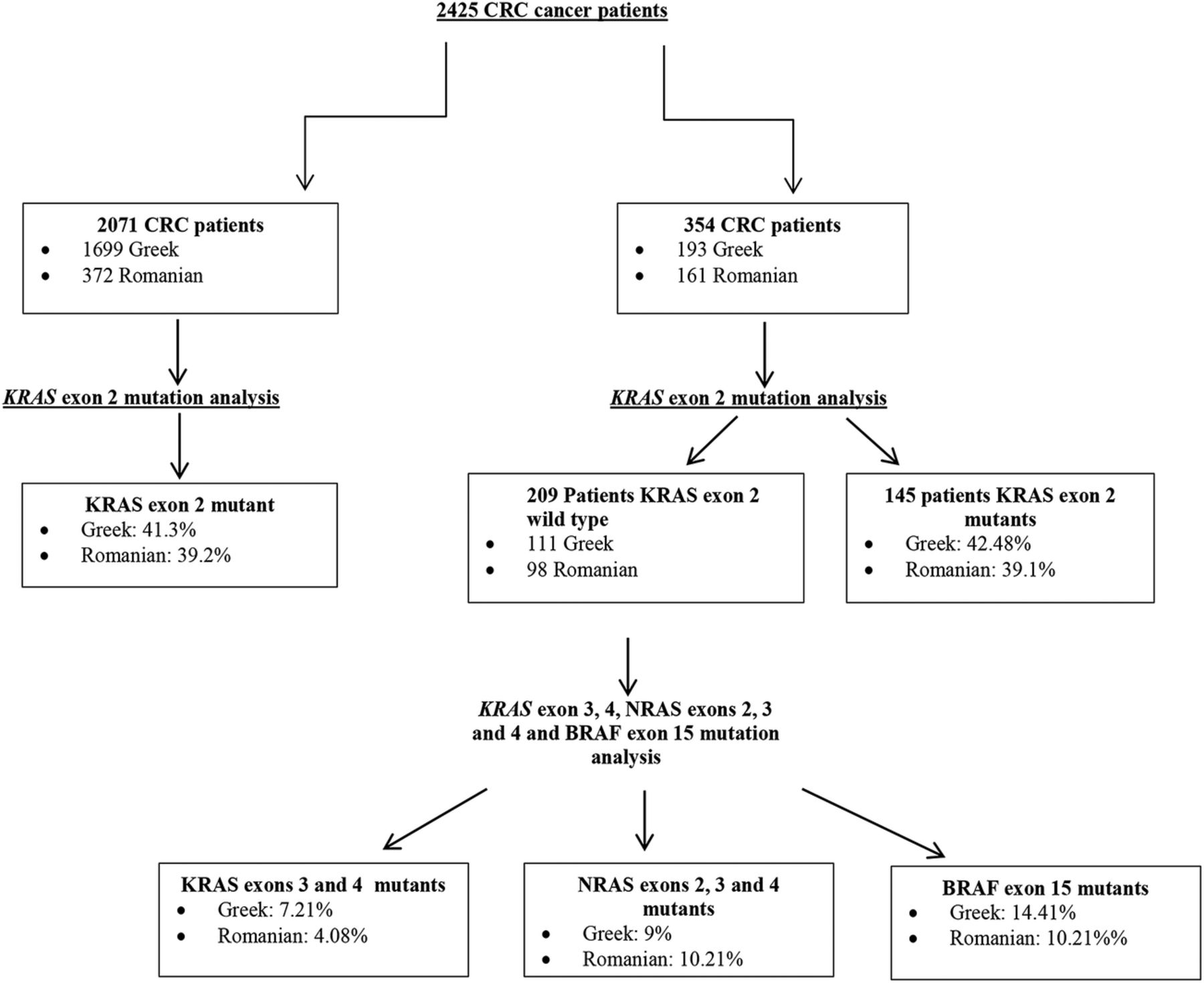
A total of 2425 patients with colorectal cancer participated in the study (figure 1). In total, 2071 patients with colorectal cancer were analysed for KRAS exon 2 mutations. One thousand six hundred ninety nine of them were of Greek origin and 372 of Romanian origin. Additionally, a consecutive series of 354 patients was selected to perform the full KRAS, NRAS and BRAF mutation analysis. The material selected for mutation analysis was formalin-fixed and paraffin-embedded (FFPE) sections from the primary colorectal tumour. Informed consent was obtained from all patients before testing. The study was approved by the ethical committee of ‘Agii Anargiri’ Cancer Hospital.

Study workflow, patient distribution and mutation frequencies.
DNA extraction was performed from a 10 µm thick section of the FFPE tissue sample. Pathological review was obtained for all samples and macrodissection was performed to ensure tumour cell content (TCC) of >75%, when possible. The tumour area was marked by comparison with the corresponding H&E-stained slide. DNA was extracted using the NucleoSpin Tissue Kit (Macherey-Nagel) according to the manufacturer's instructions.
Mutation analysis
KRAS and NRAS exons 2, 3 and 4 and BRAF exon 15 mutation analysis was performed using an HRM analysis. PCR cycling and HRM analysis were performed on the Rotor-Gene 6000 (Corbett Research). The intercalating dye used was SYTO 9 (Invitrogen). More specifically, PCR assays were carried out in 25 μL reaction volume containing 100 ng of genomic DNA, 1×PCR buffer, 2.5 mmol/L MgCl2, 200 nmol/L of each primer, 200 µmol/L of each dNTP, 5 µmol/L of SYTO 9, 1.25 U of HotStarTaq (QIAGEN Inc., Valencia, CA; 5 U/µL) and PCR grade water.
Primer pairs for BRAF, KRAS exon 4 and NRAS exon 4 were designed with primer-BLAST software (http://www.ncbi.nlm.nih.gov/tools/primer-blast). Primer pairs for KRAS exons 2 and 3 and NRAS exons 2 and 3 were previously described8 ,10 ,11 (table 1). The PCR conditions were: initial denaturation at 95°C for 15 min, followed by 40 cycles of 15 s at 95°C, 30 s at the annealing temperature and 15 s at 72°C. For the HRM analysis profile, samples were denatured with an initial hold of 95°C for 1 s and a melting profile from 72°C to 95°C rising at 0.2°C. The annealing temperature was 56°C for all amplicons, except for KRAS exon 2 for which we used an annealing temperature of 67.5°C. All HRM reactions were run in triplicate.
Primer sequences and amplicon length of the high-resolution melting experiment
Whenever equivocal results between HRM and sequencing were observed in KRAS exon 2 amplicon, an alternative mutagenic PCR-RFLP (Restriction Fragment Length Polymorphism) method was used to test for mutations in codons 12/13 of the KRAS gene.12
Sequencing analysis
For the Sanger sequencing reaction, PCR amplification products were purified using the NucleoFast 96 PCR Clean-up Kit (Macherey-Nagel), according to the manufacturer's protocol. Seven μL of the purified product were used for the sequencing reaction using the BigDye Terminator v1.1 Cycle Sequencing Kit (Applied Biosystems Inc., Fostercity, California, USA). Sequencing reaction products were purified prior to electrophoresis using the Montage SEQ96 Sequencing Reaction Kit (Millipore Corporation). Sequencing analysis was performed on an Applied Biosystems 3130 Genetic Analyzer.
Sensitivity
The sensitivity test was performed using genomic DNA reference standards with defined allelic frequencies (Horizon diagnostics).
KRAS G12D, NRAS G12D, NRAS Q61K and BRAF V600E heterozygous DNAs (allele frequency 50%) were diluted with wild-type DNA in order to obtain a mutant to wild-type allelic ratio of 25%, 12.5%, 10%, 7.5% and 5%, respectively.
Statistical analysis
Statistical analysis was performed using either Fisher's exact or χ2 tests. A p value less than 0.05 was considered as the cut-off for statistical significance. Statistical analysis was performed with the MedCalc software V.12.7.2.
Results
Sensitivity test
Using HRM we were able to detect 5% of mutant KRAS G12D in wild-type DNA, 5% of mutant NRAS G12D allele in wild-type DNA, 7.5% of mutant BRAF V600E allele in wild-type DNA and 7.5% of mutant NRAS Q61K allele in wild-type DNA (figure 2). Using the sequencing method for the same mutations we were able to detect 12% of mutant alleles in wild-type DNA.
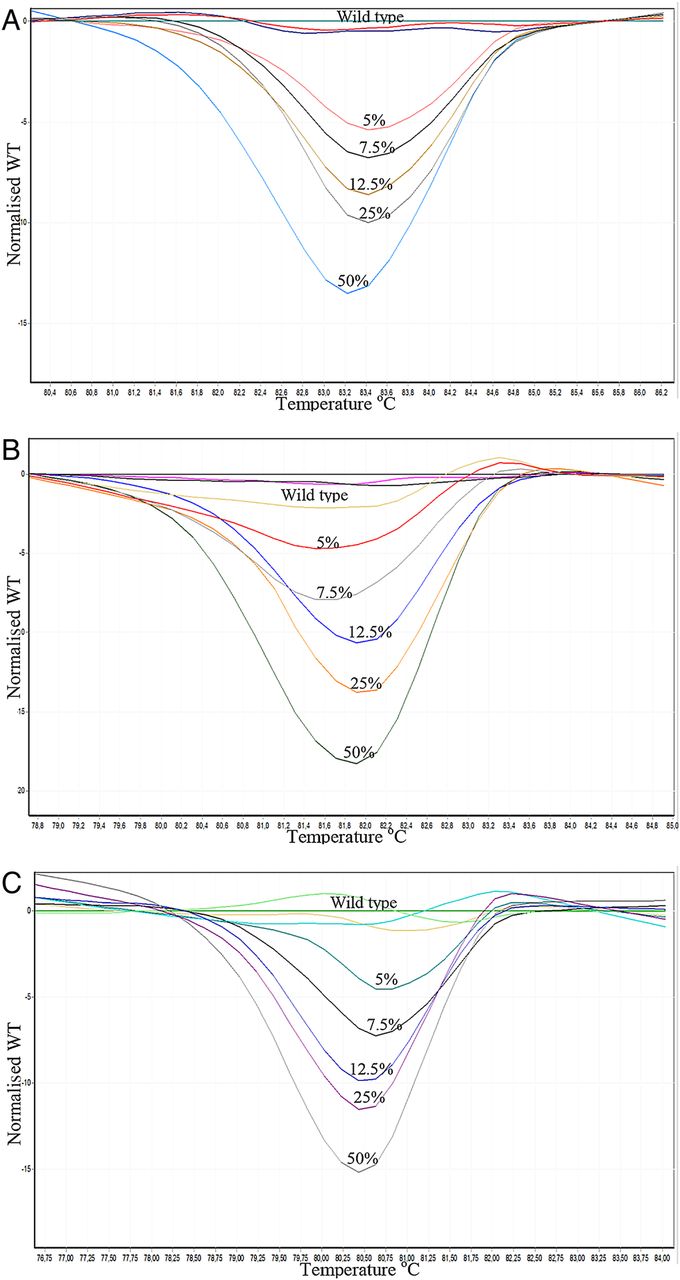
Difference graphs of the sensitivity test. Serial dilutions were performed in order to obtain a mutant to wild-type allele ratio of 50%, 25%, 12.5%, 7.5% and 5%. (A) NRAS G12D allele in wild-type DNA. (B) NRAS Q61K allele in wild-type DNA. (C) BRAF V600E allele in wild-type DNA.
KRAS exon 2 mutation analysis
KRAS exon 2 mutations were detected in 702 of the 1699 Greek patients with colorectal carcinoma (CRC) analysed (41.3%) and in 39.2% (146/372) of the Romanian patients (figure 1). There was no statistically significant difference between the two groups (p=0.5). In total, 77.3% of the mutations were detected in codon 12 and 22.7% in codon 13. The most prevalent mutation was c.35G>A (p.G12D) accounting for 29.48% of all the exon 2 mutations followed by c.38G>A (p.G13D) and c.35G>T (p.G12V; 19.36% each; figure 3). In three samples no mutation could be detected by sequencing analysis, while HRM showed an abnormal melting profile which is indicative of the presence of a mutation. In these cases an alternative PCR-RFLP method was used.12 The results obtained indicated the presence of a mutation in codon 12 in one case and in codon 13 in the other two cases.
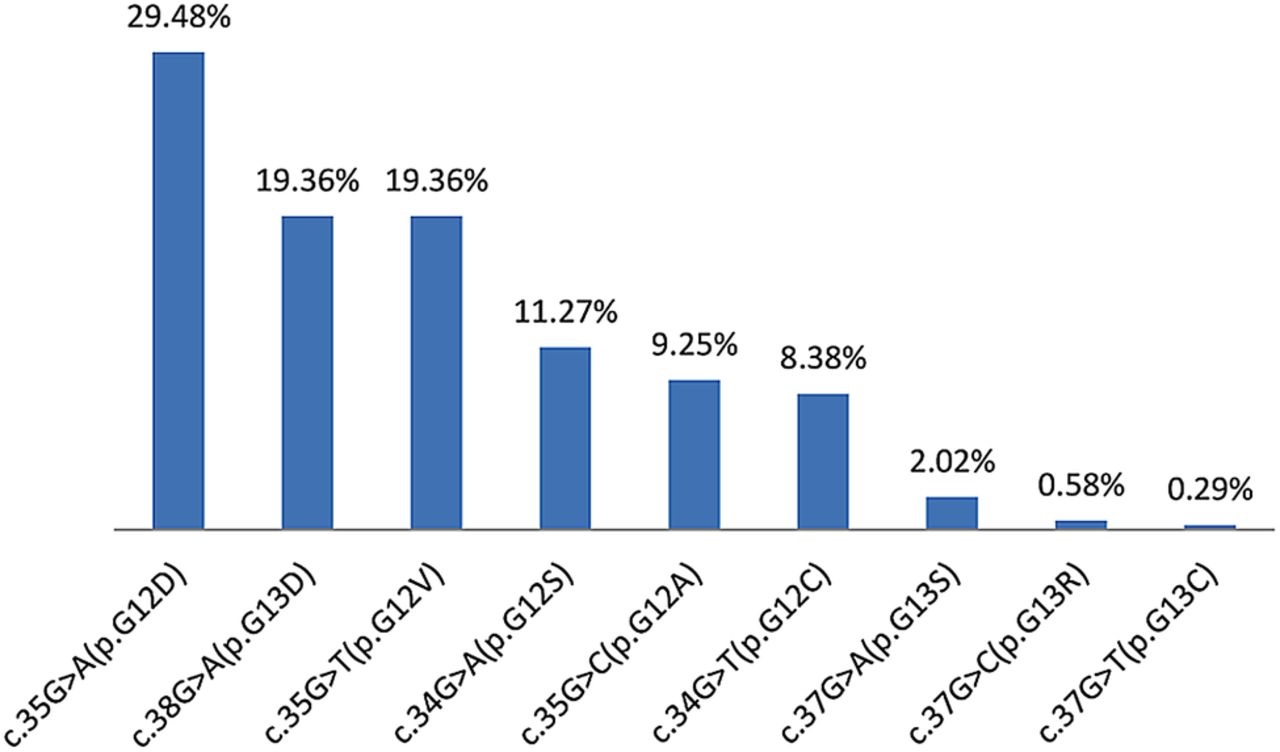
Distribution of the different mutation types found in KRAS exon 2 (codons 12 and 13) patients with mutant colorectal carcinoma. Percentages refer to the group of mutated tumours.
Full KRAS/NRAS (exons 2, 3 and 4) mutation analysis
DNA from 354 consecutive patients (193 of Greek origin and 161 of Romanian origin) was subjected to KRAS/NRAS (exons 2, 3 and 4) and BRAF (exon 15) analysis. In total, 145 (82 Greek, 63 Romanian) of them were found to carry a mutation in exon 2 of the KRAS gene. The combined mutation frequency was 40.96% (42.48% for the Greek population and 39.1% for the Romanian population; figure 1).
The remaining 209 (111 Greek, 98 Romanian) exon 2 wild type CRC samples were screened in parallel by HRM and sequencing analysis for mutations in exons 3 and 4 of KRAS, exons 2, 3 and 4 of NRAS and exon 15 of BRAF (figure 1). There was a 99% concordance between the two methods. All mutations detected by Sanger sequencing were also detected by HRM.
In two cases an abnormal melting profile was observed by HRM, while no mutation could be detected using sequencing analysis. The first case concerned the NRAS exon 2 amplicon and the second the NRAS exon 3 amplicon. Since there was not an alternative method to validate the results obtained by the two methods, these samples were excluded from the study.
Automated sequencing of the HRM PCR products confirmed the presence of 32 mutations, with the following distribution: 12 in KRAS (4 in exon 3 and 8 in exon 4), 20 in NRAS (15 in exon 2, 4 in exon 3 and 1 in exon 4; table 2).
Mutation frequency detected in Greek and Romanian KRAS exon 2 wild-type populations
Thus, in our study 15.31% of wild-type KRAS exon 2 (codons 12/13) samples harbour a mutation in KRAS exons 3 and 4 and NRAS exons 2, 3 and 4 (figure 4). This result is comparable with those obtained in other recent studies.3 ,6 ,13

KRAS exons 3 and 4, NRAS exons 2, 3 and 4 and BRAF exon 15 mutation frequency in 209 KRAS exon 2 wild type patients with colorectal cancer.
BRAF mutation analysis
Among the 209 KRAS exon 2 wild-type patients tested BRAF exon 15 mutations were detected in 26 of them (12.44%; table 2). The mutual exclusivity of KRAS (exons 3 and 4), NRAS (exons 2, 3 and 4) and BRAF mutations was confirmed, since none of the patients with a KRAS/NRAS mutation presented a simultaneous mutation at one of the other RAS exons tested or at BRAF.
There was no statistically significant difference in the mutation frequency of the genes tested or the mutation distribution between the two populations (tables 2 and 3). Among KRAS exon 2 wild-type cases only 72.25% (151/209) remained wild type for all regions studied, while 15.31% harboured additional RAS mutations and 12.44% BRAF mutations. This means that an additional 16.38% of the patients tested (27.75% of the KRAS exon 2 normal group) are unlikely to benefit from anti-EGFR therapy, reducing the percentage of patients to be treated from 59.04% to 42.66%.
Types of RAS/BRAF mutations detected in KRAS exon 2 wild-type Greek and Romanian populations
Discussion
Mutation detection in any of the genes involved in the RAS/RAF/MEK/ERK pathway has a great impact on CRC treatment decision and patient management. Thus reliable molecular methods are needed to identify such mutations. HRM analysis is considered a highly specific and sensitive method that is currently widely used in somatic mutation detection.8 ,14 ,15
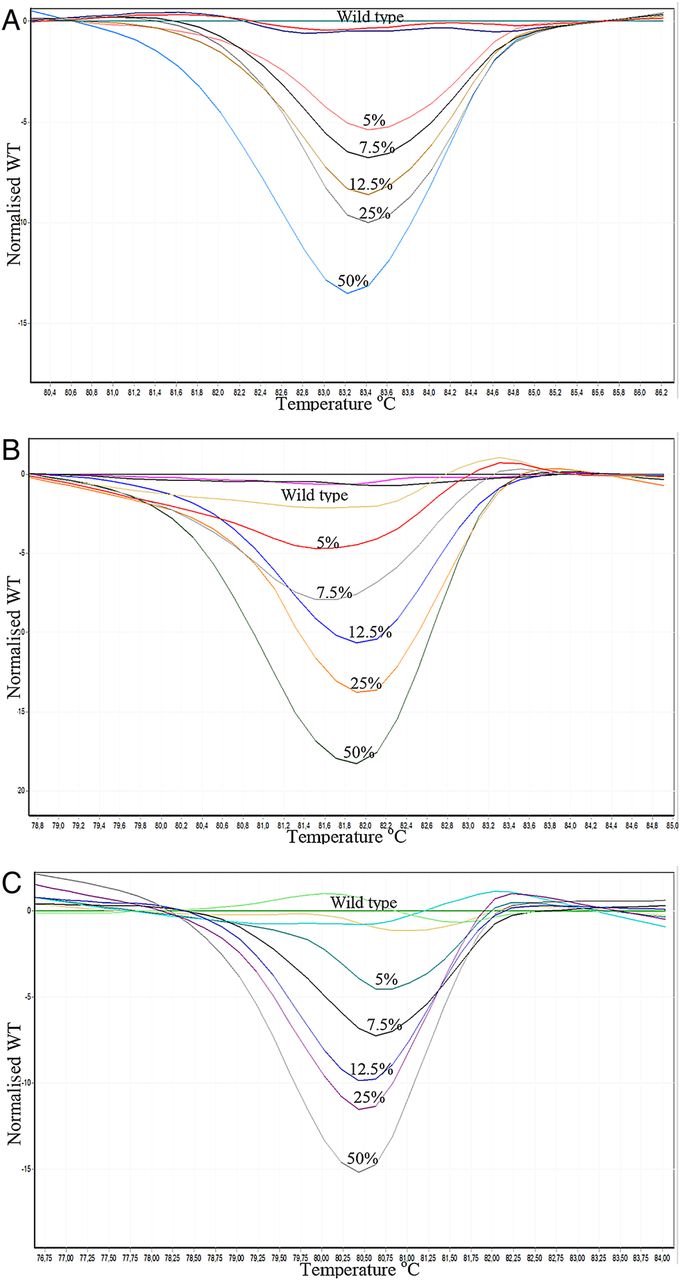
The HRM analysis we used generated specific melting profiles that allowed the discrimination between wild type and mutated samples (figure 5). It was proved to be reliable since all mutations detected by Sanger sequencing were also detected by HRM. Additionally, HRM analysis is much faster and cost effective compared with sequencing analysis. Thus, it can be used as a fast screening method to detect mutant samples. However, further characterisation of the specific mutation requires sequencing analysis.

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Normalised graphs of the high-resolution melting analysis containing wild type and mutant samples. (A) NRAS exon 2 amplicon. (B) NRAS exon 3 amplicon. (C) BRAF exon 15 amplicon.
The high sensitivity of the method was confirmed in our experiments, since we achieved a sensitivity of mutant/wild-type allele detection that ranged between 5% and 7.5% (depending on the mutation type and amplicon), while sequencing analysis had a sensitivity of 12–15%. It has been reported that HRM is a more sensitive method compared with Sanger sequencing, however, it has also been reported that this method can give some false-positive results due to bad DNA quality, especially when the starting material is FFPE tissue.16 Thus, whenever equivocal results are obtained, an alternative method should be used in order to confirm the presence of a mutation. In our study, three samples were positive for a mutation in KRAS exon 2 amplicon by HRM, but were negative by sequencing. For this amplicon an alternative PCR-RFLP approach was used and the results obtained verified the presence of mutations in all three samples. Additionally, two cases that concerned NRAS exon 2 and NRAS exon 3 amplicons were positive by HRM and negative by sequencing. Since there was no alternative method to validate the results obtained by the two methods these samples were excluded from the study.
Another important factor affecting sensitivity is appropriate tissue selection. We consider the existence of pathological review for all samples crucial. Using macrodissection we ensured a per cent TCC of >75.
Until recently, analysis of patients with colorectal cancer who would respond to anti-EGFR therapy involved only mutation detection of KRAS exon 2, which has a frequency of 40%.17–19
Almost all information on the molecular features of human malignancies is derived from European and US patients. There is, however, growing evidence that these findings may not be applicable to all ethnic groups. It has been reported that KRAS exon 2 (codons 12/13) mutation percentage in CRC is lower in Asian and Middle Eastern populations (24%) than in European and Latin American populations (36% and 40%, respectively).20 However, even in Asian and Middle Eastern populations there is heterogeneity in mutation rates among different ethnicities.21 It is unclear if this is due to different genetic backgrounds or due to environmental and lifestyle differences between the nations.
In our study KRAS exon 2 mutation frequency was 41.3% (702/1699) in Greek patients and 39.2% (146/372) in Romanian patients. These results are similar to those obtained in European populations.20 There was no statistically significant difference between the two populations (p=0.5).
The presence of mutations in codons 12/13 of the KRAS gene was believed to be a specific determinant of failure to respond to anti-EGFR therapy. However, there is still quite a significant number (35–50%) of wild-type patients who do not benefit from the treatment.6 ,13 ,22 Recently it was shown that additional KRAS and NRAS mutations occur in a substantial proportion of patients with metastatic colorectal cancer and that they have a predictive value.4–7 However, data concerning mutation frequency of the RAS mutations other than KRAS exon 2 are very limited.
In three recent studies (performed by Guedes et al,13 Vaughn et al3 and Douillard et al6) KRAS exons 3 and 4 mutation frequency was investigated in KRAS exon 2 wild-type patients (number of patients included: 201, 513 and 641, respectively). In these studies KRAS exon 3 mutation frequency ranged between 3.7% and 6.5% (weighted average 4.1%), while that of KRAS exon 4 mutations ranged between 3.3% and 6.5% (weighted average 4.9%). In our study the mutation frequency of KRAS exons 3 and 4 was found to be 1.9% (4/209) and 3.8% (8/209), respectively (χ2=1.8, p=0.2 and χ2=0.27, p=0.6, respectively; table 2). Additionally, there was no statistically significant difference in the mutation frequency between the two populations.
Even less data exists concerning NRAS mutation frequency. Two of the aforementioned studies (performed by Vaughn et al,3 and Douillard et al6) also analysed NRAS gene in KRAS exon 2 wild-type patients.13 Mutation frequency of NRAS exon 2 was 1.9% and 3.4% (weighted average 2.77%), while exon 3 was mutated with a percentage of 3.1% and 4% (weighted average 3.64%). In our study the mutation frequency for NRAS exon 2 was 7.18% (15/209) which is higher compared with previous studies (χ2=9.06, p=0.003), while the mutation frequency of exon 3 does not differ significantly, 1.9% (4/209; χ2=1.14, p=0.3).
NRAS exon 4 mutation in CRC seems to be a very rare event with a frequency of <0.2%.23 In our study only one sample was found to carry a mutation in this exon (0.28% of the total patients studied).
Thus, according to recent data 12–17% of wild-type KRAS exon 2 (codons 12/13) patients harbour a mutation in KRAS exons 3 and 4 and NRAS exons 2, 3 and 4.3 ,6 ,13 In our study this percentage was 15.31% (figure 4).
In our study BRAF mutations were present in 12.44% of KRAS exon 2 wild-type patients. This result is comparable with the results obtained in other studies.6 ,23 ,24 There was no statistically significant difference in the mutation frequency between the two populations analysed (table 2).
In 354 consecutive patients with CRC KRAS exon 2 mutations were detected in 40.96% of the cases. In the remaining 59.04% exon 2 wild-type patients we detected 15.31% additional RAS mutations and 12.44% BRAF mutations, reducing the proportion of true wild-type patients from 59.04% to 42.66%. This means that 27.75% of the KRAS exon 2 wild-type patients are unlikely to benefit from anti-EGFR treatment (figure 4). The selection of patients eligible to receive anti-EGFR treatment helps reduce the costs of unnecessary treatment. This percentage will probably increase with the addition in the mutation analysis of more genes that participate in the signalling pathways controlled by EGFR, such as the HRAS gene, which is the third member of the RAS family and PIK3CA gene that participates in the PI3K-AKT pathway.
Conclusions
The HRM method we developed proved to be a cost effective, rapid and sensitive approach for KRAS, NRAS and BRAF mutation screening. To the best of our knowledge this is the first study reporting KRAS, NRAS and BRAF mutation frequency in Greek and/or Romanian patients with colorectal cancer. The KRAS exon 2 mutation frequency observed was 41.3% (702/1699) and 39.2% (146/372) in Greek and Romanian patients, respectively. Additionally, our findings indicate that in 209 wild-type KRAS exon 2 patients, full KRAS, NRAS and BRAF mutation analysis led to the detection of additional 15.31% patients with colorectal cancer with exon 3 or 4 KRAS mutations or with NRAS mutations and 12.44% with BRAF exon 15 mutations. No difference in the mutation frequency was observed between the Greek and Romanian population. We conclude that more than one-fourth of the KRAS exon 2 wild-type patients present with mutations in other genetic positions which confer resistance to anti-EGFR therapy.
References
Footnotes
SN and EP contributed equally.
-
Contributors SN participated in the manuscript preparation, performed literature search and provided tumour samples for analysis. EP participated in the manuscript preparation and carried out the majority of molecular genetic analysis. AA was involved in the critical revision of the manuscript and carried out part of the molecular analysis. DLS, EC, CV, AC, SK, GA, NZ, EA, NT, NP and HPK provided the tumour tissue, reviewed and edited the manuscript. GN coordinated the study and was responsible for the final revision and approval of the manuscript.
-
Funding This research received no specific grant from any funding agency in the public, commercial or not-for-profit sectors.
-
Competing interests None.
-
Patient consent Obtained.
-
Ethics approval Ethical committee of ‘Agii Anargiri’ Cancer Hospital.
-
Provenance and peer review Not commissioned; externally peer reviewed.
-
Data sharing statement No additional data are available.