Article Text

Abstract
Introduction Obesity and type 2 diabetes (T2D) are highly prevalent among African migrants compared with European descent populations. The underlying reasons still remain a puzzle. Gene–environmental interaction is now seen as a potential plausible factor contributing to the high prevalence of obesity and T2D, but has not yet been investigated. The overall aim of the Research on Obesity and Diabetes among African Migrants (RODAM) project is to understand the reasons for the high prevalence of obesity and T2D among sub-Saharan Africans in diaspora by (1) studying the complex interplay between environment (eg, lifestyle), healthcare, biochemical and (epi)genetic factors, and their relative contributions to the high prevalence of obesity and T2D; (2) to identify specific risk factors within these broad categories to guide intervention programmes and (3) to provide a basic knowledge for improving diagnosis and treatment.
Methods and analysis RODAM is a multicentre cross-sectional study among homogenous sub-Saharan African participants (ie, Ghanaians) aged >25 years living in rural and urban Ghana, the Netherlands, Germany and the UK (http://rod-am.eu/). Standardised data on the main outcomes, genetic and non-genetic factors are collected in all locations. The aim is to recruit 6250 individuals comprising five subgroups of 1250 individuals from each site. In Ghana, Kumasi and Obuasi (urban stratum) and villages in the Ashanti region (rural stratum) are served as recruitment sites. In Europe, Ghanaian migrants are selected through the municipality or Ghanaian organisations registers.
Ethics and dissemination Ethical approval has been obtained in all sites. This paper gives an overview of the rationale, conceptual framework and methods of the study. The differences across locations will allow us to gain insight into genetic and non-genetic factors contributing to the occurrence of obesity and T2D and will inform targeted intervention and prevention programmes, and provide the basis for improving diagnosis and treatment in these populations and beyond.
- Epidemiology
This is an Open Access article distributed in accordance with the terms of the Creative Commons Attribution (CC BY 3.0) license, which permits others to distribute, remix, adapt and build upon this work, for commercial use, provided the original work is properly cited. See: http://creativecommons.org/licenses/by/3.0/
Statistics from Altmetric.com
Introduction
Ethnic minority and migrant populations in Europe have been disproportionately affected by obesity and diabetes compared with the host European origin populations (henceforth, Europeans).1–4 The prevalence of type 2 diabetes (T2D) in these populations, for example, is about three to five times higher than in Europeans.4 They also develop T2D at a younger age; and they have higher morbidity and mortality from T2D and related complications such as cardiovascular disease (CVD) than European populations.4 ,5 The little available information suggests that sub-Saharan Africa (SSA) migrants are particularly affected by obesity and T2D.3 In the Health Survey for England (HSE) 2004, the prevalence rates of T2D were 16.2% and 6% in SSA men and women aged ≥35 years compared with 5.1% and 2.4% in English general population men and women, respectively.6
Obesity and T2D prevalence rates are not only escalating among SSA migrants, but also in their home countries. The increasing levels of obesity and T2D in SSA countries have been unprecedented and pose huge challenges for many countries. While T2D seemed to be virtually absent, for example, in West Africa in the 1960s and 1980s (0.2–1.7%), today it has become a major health problem affecting almost 7% of the adult population.7–10 Projections indicate that the number of T2D patients in SSA will double from 14.7 million in 2011 to 28 million in 2020,11 undoubtedly among one of the highest growth rates of T2D worldwide.11 ,12 This correlates with the simultaneous increase of obesity in the same region.7 A systematic review found that the prevalence of obesity in urban West Africa has more than doubled over the past 15 years.9 The serious cardiovascular complications of obesity and T2D could overwhelm SSA countries that are already straining under the burden of communicable diseases.
The reasons for the increased susceptibility of ethnic minority groups and migrants to obesity and T2D are poorly understood. Increased T2D prevalence and complications in African populations in SSA and industrialised countries have been attributed to delayed diagnosis and poor management due to low socioeconomic status. However, ethnic differences persist even when demographic, socioeconomic status, behavioural and clinical parameters have been taken into account,13 suggesting that other factors such as genetic predispositions might be important. The validity of this finding, nonetheless, is limited because of the heterogeneity of migrants studied so far. Heritability estimates for T2D range up to 40%,14 ,15 but genetic variations thus far identified contribute only a small fraction of the inherited risk.16 While genetic factors alone cannot explain the increasing prevalence of obesity and T2D, it is clear that the high prevalence of obesity and T2D is a result of a complex interplay of environmental and genetic factors that are likely to vary in different settings and among different population groups. Genetic predispositions and interactions between environmental and genetic factors may be involved in the onset and development of diseases such as obesity and T2D among migrant populations. The ‘thrifty genotype’ and ‘thrifty phenotype’ hypotheses are considered to be the underlying mechanism of the gene–environment interaction contribution to disease susceptibility.17–21 While gene–environment interactions may play an important role in disease susceptibility, research in this area, particularly within the context of human migration, is in its infancy.
The high levels of obesity and T2D among migrant populations may also be influenced by lifestyle changes following migration3 as well as psychological stress.22 Evidence from cohort studies demonstrate the importance of lifestyle factors such as physical inactivity and smoking on obesity and T2D.23–27 However, among migrant populations, interventions to reduce obesity and T2D have often been ineffective,28 and efforts often fail to meet the specific needs of ethnic minority and migrant populations.29 The local circumstances of ethnic minority and migrant populations, such as socioeconomic development of the groups, race relations and access to healthcare and preventive services, may differ greatly among industrialised countries.30 ,31 These differential contexts can influence health behaviour, psychosocial stress and healthcare use among ethnic minority and migrant groups, and subsequently lead to differences in CVD health outcomes between similar populations living in different countries.
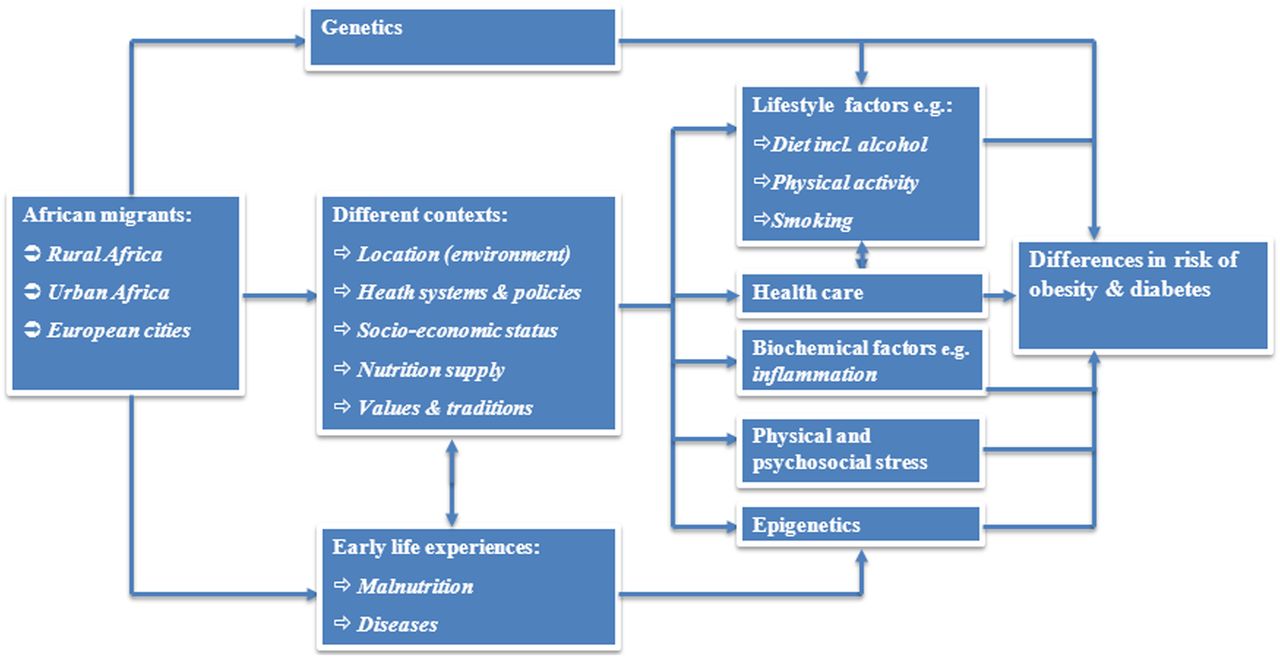
The Research on Obesity and Diabetes among African Migrants (RODAM) project—an European Commission funded project—aims to understand the reasons for the high prevalence of obesity and T2D among African migrants by (1) studying the complex interplay between environmental exposures and genetics and their relative contributions to the high prevalence of obesity and T2D; (2) to identify specific risk factors within these broad categories to guide intervention programmes and (3) to provide a basic knowledge for improving diagnosis and treatment. A conceptual model of the RODAM project is presented in figure 1.32 It shows that following migration, migrants may be exposed to varied contexts, such as different opportunities for socioeconomic development, different availability of food supply, different health systems and policies and different cultural traditions; and these differences may influence their health behaviour, physical and psychosocial stress and subsequently lead to differences in obesity and T2D risks.

{kind=link}
A conceptual model for the RODAM project.
Methods
To achieve RODAM study goals, a multidisciplinary consortium of researchers from Europe (University of Amsterdam, Utrecht University, London School of Hygiene and Tropical Medicine, Charité—Universitätsmedizin Berlin, German Institute of Human Nutrition) and Africa (University of Ghana, Kwame Nkrumah University of Science and Technology and the International Diabetes Federation (IDF), African region) with broad experience on chronic diseases in Africans and African migrants have joined forces. As a central feature of the RODAM project, at all study sites, highly standardised protocols of quantitative and qualitative assessments are applied for participant recruitment and topic-related investigations.
Study population
Assessing the role of gene–environmental interactions in risk factors, such as obesity and T2D, among migrant populations requires a highly standardised approach and relatively homogeneous migrating and non-migrating populations. For this reason, we concentrate on a relatively homogenous SSA migrant population to enable comparisons of the prevalence of obesity and T2D between SSA migrants living in different European countries and their compatriots living in rural and urban SSA as outlined in the WHO Global Consultation on Migrant Health report.33 Consequently, adult Ghanaians (aged ≥25 years) are recruited in rural and urban Ghana, and in the cities of Amsterdam, Berlin and London. Ghanaians are one of the largest SSA migrant groups in Europe.34–36 The 2009 estimates by the Office for National Statistics recorded 93 000 Ghanaian-born people living in the UK. The majority of Ghanaians in the UK are concentrated in London boroughs of Southwark, Lambeth, Newham, Hackney, Haringey, Lewisham, Croydon, Merton and Brent.34 In Germany, 22 000 people are officially registered as Ghanaians, the majority of whom are concentrated in Berlin, Hamburg and North-Rhine Westphalia.35 In the Netherlands, in 2009, there were approximately 20 000 officially recorded Ghanaians. The majority of these are concentrated in southeast Amsterdam.36
Recruitment of the study participants
Engagement of Ghanaian community
Previous work in the Netherlands and a feasibility study among African communities in the UK show that involvement of the community leaders enhances study participation and may help prevent a low response rate relating to language barriers and lack of understanding about the relevance of the study.37 ,38 The RODAM project, therefore, involves the Ghanaian community leaders in all sites. This includes working with religious communities (eg, churches and mosques), endorsement from local key figures and establishing relationships with healthcare organisations that serve these groups. In addition, the project team provides information about the study via local media aim at the Ghanaian population (eg, Ghanaian radio and TV stations).
Owing to differences in the population registration systems across European countries as well as in Ghana, different approaches are needed for the recruitment of the study populations across different locations. For example, there is a population register in the Netherlands where the Ghanaian migrants could be identified and randomly selected for the study. In Ghana, the UK and Germany, the situation is quite different as there are no population registers that will allow for the easy identification of these populations. It is important, however, to adopt the recruitment strategies that are comparatively as similar as possible across different locations. We describe below the various recruitment strategies in each site.
Recruitment strategy in Ghana
In Ghana, two cities (Kumasi and Obuasi) and 15 villages in the Ashanti region are served as the urban and rural recruitment sites. The initial sampling frame was the list of enumeration areas (EAs) in the Ashanti region from the 2010 census. A multistage random sampling procedure was adopted to arrive at the sampling of 30 EAs. EAs were stratified, weighted and a random sample of rural and urban EAs was selected. There are over 2000 urban EAs and more than 1000 rural EAs. The first stage was to group the districts into two main categories: districts with a high number of urban (Kumasi and Obuasi) areas and districts with a high number of rural EAs. The next stage of sampling was to put the EAs together in each of the categories and take a weighted random sample of 10 for Kumasi and 5 for Obuasi, respectively. The procedure was repeated for the rural EAs by adding all the EAs in the selected districts and weighted from the first stage together after which a simple random sample procedure was adopted to select the total number of rural EAs (15) required for the study. Letters are sent to all selected health and community authorities to notify them of the start of the study. We send team members to the various communities to stay among them. Once within the community, the team then organise mini clinics in the field for a period of 1–2 weeks depending on the sampled population and responsiveness of respondents.
Recruitment strategy in the Netherlands
In the Netherlands, Ghanaian participants were randomly drawn from Amsterdam Municipal Health register. This register contains data on country of birth of citizens and their parents, thus allowing for sampling based on the Dutch standard indicator for ethnic origin. All selected participants aged ≥25 years were sent a written invitation combined with written information regarding the study and a opting out response card. Participants are reminded by phone or home visit after 2 weeks if there is no response. After a positive response, an appointment for physical examination at a local health centre is made over the phone followed by a confirmation letter of the appointment, and a digital or paper version of the questionnaire (depending on the preference of the participant) is sent to the participant's home address.
Recruitment strategy in the UK
The UK has no population register for migrant groups. Consequently, Ghanaian organisations are served as the sampling frame. Lists of these organisations have been obtained from the Ghanaian Embassy and the Association of Ghanaian Churches in the UK in the boroughs known to have the greatest concentration of Ghanaians. Lists of all members of their organisations, if available, have also been requested, from which a number of all participants aged ≥25 years are invited to participate in the study. The selected participants receive a written invitation combined with written information regarding the study and a opting out response card. Participants are sent a confirmation letter of the appointment for a physical examination at a local health centre, church or community centre, including a digital or paper version of the questionnaire (depending on the preference of the participant) if they agreed to participate in the study.
Recruitment strategy in Germany
In Berlin, a list of Ghanaian individuals (born in Ghana, or Ghanaian passport holders) was provided by the registration office and that was supplemented with contact details of members of Ghanaian organisations and churches in Berlin. From this combined list, all participants aged ≥25 years have been invited to participate in the study. In addition, a written invitation combined with written information regarding the study and a response card has been sent to the selected participants. Participants are reminded after 2 weeks if there is no response. After a positive response, the participants are contacted by phone to schedule date and location of the interview with a trained research assistant or opt for the digital online version. Subsequent to the completion of the questionnaire, a date for physical examination is then scheduled.
Informed written consent is also obtained from each participant prior to the enrolment in the study. In addition, an external independent Ethical advisor has been appointed by the RODAM Steering Committee to oversee the ethical issues in the RODAM study.
Power and data analysis
In the presented study, we aim to sample 6250 individuals comprising five subgroups of 1250 each from the five locations. For phenotypic, genetic and epigenetic studies, subsets are selected. In order to estimate the statistical power with regard to different sample sizes in the three types of data, we evaluated three distinct types of statistical power calculations with regard to the type of survey.
Phenotypic association: For the phenotypic association analysis, we assumed a prevalence of T2D of <5% in rural Ghana, 6–7% in urban Ghana and >12% in Europe.32 ,39 For obesity, we assumed a prevalence of <5% in rural Ghana, 17% in urban Ghana and 30% in Europe.2 ,39 In general, we aim for a power of 0.90 with α=0.05 (including Bonferroni correction). Using these parameters a sample size of approximately 1230 is needed in the rural Ghana, urban Ghana, Amsterdam, London and Berlin subsets to detect a difference between the group proportions of 5%. T2D was defined as fasting plasma glucose ≥7 mmol/L, or pre-existing antidiabetic medication or glycated haemoglobin (HbA1c) ≥6.5%.40 Generalised obesity was defined as body mass index (BMI) ≥30 kg/m2, and central obesity as a waist circumstance >102 cm in men or >88 cm in women.41 ,42
Genetic association: The present study aims to genotype a substantial part of the total sample among patients with diabetes (cases) and non-diabetes (controls). The genotyping will be based on a standard single nucleotide polymorphism array platform suitable for performing genome-wide association study as well as candidate gene analysis or related approaches. Using the statistical power calculator on binary traits for a case–control study design (S Purcell; http://pngu.mgh.harvard.edu/), assuming an allele frequency of 0.25, a prevalence of 16%, a relative risk of 1.3 and 1.6 (Aa and AA rep.), a D’ of 1, the number of cases of 1000 (1:2 case–control ratio) and a type I error rate of 0.05, approximately 540 cases are considered sufficient to obtain a power of 0.90. Although the latter necessary sample size is covered by our study, it should be noted that correction for multiple tests, that is, if more than one genetic variant is tested, is not considered here. Nevertheless, candidate gene or related association approaches within this single study setup have sufficient statistical power to detect moderate and low effect sizes.
Epigenetic association: To explore the influence of epigenetic factors on the main outcomes, we will first assess the differences in methylation levels among Ghanaians living in rural and urban Ghana and Europe and their relative contributions to the differences to obesity and T2D that may be observed. With a study power of 0.80 and α=0.05 (and SD±0.10%), at least 64 people per group are needed to detect a mean percentage difference in methylation density of 5%. When multiple correction is taken into account, about 300 individuals per group of participants are needed. Epigenome-wide analysis will be performed. Association analysis of the DNA methylation profiles and obesity and T2D and related phenotypes will subsequently be performed. Promising loci will then be validated using next-generation bisulfite sequencing.
Simple tables, proportions, mean and median values will be used to examine the data. Multivariable linear and logistics regression analyses will be used to assess the differences and to identify specific relevant factors and their relative contribution to the differences in body indices and fasting glucose (continuous and binary traits) between Ghanaian migrants and non-migrants.
Data collection
Data collection is composed of questionnaire/interviews, physical examination and biological samples. The methods for data collection in RODAM are identical in all locations following standard operating procedures and applying standardised tools. Questionnaires have been adapted to the local circumstances in Ghana, the Netherlands, the UK and Germany, where needed. For example, for all sites, modification of questions with respect to educational system or social security system was made. Before data collection, a 2-day training course in the Netherlands was organised for all those involved in data collection, on the overall project's procedures. The training involved the administration of the different questionnaires, physical examinations, processing of blood and urine samples in the laboratory and transport and storage of samples. The work package leaders, in turn, train all recruitment team members in each site on all aspects of the study. Interviewers are recruited among Ghanaian-speaking residents in Europe, are introduced to the aims and procedures of the study and are instructed and trained on the use of the questionnaires. Research assistants also receive the online tutorial for the Oracle Clinical data entry system. The performance of each interviewer or research assistant is monitored during the initial interviews and physical examinations. Feedback is provided and changes were initiated if needed. The RODAM coordinator monitors data collection at all study sites to ensure standardisation of methods.
Questionnaire/interviews
All the participants who agree to participate in the study receive an appointment for a structured interview. The interviews are conducted by trained interviewers of Ghanaian background and last for about 60–120 min. To increase participation rate, the participants are given a range of options including interviews in participants’ homes and digital or paper version of the questionnaire, depending on the preference of the participant. The interviewers conduct the interviews in the preferred language of the respondent either in English, German, Dutch or Ghanaian languages. The interview is based on a structured health questionnaire, and contains questions on demographics (age, sex, marital status, household composition, religion), socioeconomic position (education level and parental education, employment status and parental employment status, occupational status and wealth), migration-related factors (premigration history, age at first migration, age at arrival in the current location, duration of residence, cultural distance and ethnic identity), psychosocial vulnerability (perceived discrimination, social support, mastery, recent negative life events and current depression), health status (self-reported general health and presence and history of diseases, family history of diseases), and health behaviour (eg, dietary behaviour, physical activity, alcohol and smoking, perceived body weight and body shape and adherence to medications) by using appropriate validated instruments (table 1). For example, physical activity is measured using the WHO Global Physical Activity Questionnaire (GPAQ) V.2.43 Dietary behaviour is determined by a Food Propensity Questionnaire (FPQ), specifically developed in RODAM to include Ghana-specific foods. In addition, a 24 h dietary recall questionnaire will be administered to a subset of the study population in each site (n=5*100).
Variables measured in the RODAM questionnaire
All participants who complete the questionnaire are invited for physical examination in the local research clinic or in a health centre. At the start of the visit, the study and the procedures involved are explained to each participant and informed consent is signed if not already carried out so at home.
After informed consent is given, physical measurements are made and biological samples, fasting blood and urine samples are collected.
Physical measurements
Physical examinations are performed with validated devices according to standardised operational procedures. Physical examinations comprise assessment of anthropometrics (weight, height, trunk, waist circumference and hip circumference), Bioimpedance Analysis (BIA), blood pressure and Ankle-Brachial Index (ABI) measures (table 2). The portable stadiometer SECA 217 is used for height measurement, the SECA 877 for weight measurement, measuring tape for abdominal and hip circumference and BODYSTAT 1500 MDD analyser for BIA. Blood pressure is measured three times using validated semiautomated device (The Microlife WatchBP home) with appropriate cuffs in a sitting position after at least 5 min rest. ABI is measured with The Microlife WatchBP Office ABI with appropriate cuffs in a supine position after at least 10 min rest. Each participant receives a summary of his/her main results accompanied by an explanation and the recommendation to contact his/her GP if the results are abnormal.
Physical examination variables measured in RODAM
Biological material
Blood samples
Fasting venous blood samples are collected by trained research assistants in all sites. All blood samples are manually processed and aliquoted immediately after collection by a trained technician or research assistant according to standard operational procedures, and then temporarily stored at the local research location. Immediate processing and cryopreservation at the research location has the advantage of preserving any highly labile molecules in the samples. Standardised procedures ensure that each sample is collected, handled, processed, transported and stored in the same way across the sites. The samples are then transported to the respective local laboratories (Durrer Center for Cardiogenetic Research at the AMC, Amsterdam; Kwame Nkrumah University of Science and Technology, KCCR, Kumasi, Faculty of Infectious and Tropical Diseases, LSHTM, London & Institute of Tropical Medicine and International Health, Berlin), where samples are checked, registered and stored at −80°C. These samples include EDTA whole blood, heparin plasma and serum. In addition, on the spot, fasting plasma glucose level is assessed by validated hand-held device (Accu-Chek Performa metre+Accu-Chek Inform II test strip (Roche, Germany) in all sites to provide accurate glucose determination as blood glucose concentration tends to decline over time in blood samples.53
Morning urine sample
Participants are asked to bring the first early morning urine in a clean jar. The urine sample is tested with a dipstick in the Urysis 1100 (Combur 7, Roche) on the spot, to determine pH, glucose, ketones, leucocytes, nitrite, protein and erythrocytes. One sample per participant is transported, together with the blood samples, to the respective local laboratory and stored at −80°C.
Transfer of biological material to dedicated centres for biochemical analyses and genotyping
From the local research centres, the two aliquoted samples, one urine sample and a 2 mL EDTA are then transported to Berlin for biochemical analyses including glucose metabolism (fasting glucose, HbA1c, insulin), lipid profile (total cholesterol, high-density lipoprotein cholesterol, low-density lipoprotein cholesterol and triglycerides), electrolytes and renal function (creatinine, albumin, sodium, potassium, calcium), uric acid metabolism (uric acid), liver metabolism (alanine transaminase, aspartate aminotransferase, γ-glutamyl transpeptidase), oxidative status and iron metabolism (ferritin) and inflammation (high-sensitivity C reactive protein); and a 4 mL EDTA whole blood sample is transported to Nottingham for DNA extraction and genotyping. Shipping of the samples from European sites is carried out using styrofoam boxes filled with dry ice and from Ghana in dry shippers filled with liquid nitrogen. Numerous factors including temperature, packaging, courier, sample type, import/export requirements, seasons, costs and transit time/ship days can affect biological specimen integrity during transportation domestically and internationally. Hence, staff involved with shipping the specimens have been trained in order to minimise factors that might affect the integrity of the specimens. In addition, training regarding legal or regulatory aspects of shipment of specimens such as Material Transfer Agreement (MTA) has been given. Each centre maintains a shipment log to record the receipt and dissemination of shipments sent from the centre. Each shipment entry is given a unique shipment number.
Qualitative interviews of perception and knowledge of obesity and T2D
Interventions to reduce obesity and T2D have often been ineffective particularly in migrant populations.28 This may, in part, relate to poor perceptions and knowledge about both conditions. Access to preventive and curative services may depend on a wide range of factors including knowledge of services and how to use them, health beliefs and attitudes, language barriers, the sensitivity of services to differing needs and the quality of care provided. Gaining in-depth insight into these factors requires qualitative methodology. Thirty-two individual interviews with people with diabetes and eight focus groups (including up to eight participants per group) with lay healthy individuals will be held at each location. Segmentation categories for purposive sampling for people with diabetes are gender, duration of diabetes, BMI status and age. Each individual interview and focus group interview is conducted by trained interviewers using the same themes across all sites and had duration of 60–90 min. Interviews are recorded, transcribed and analysed using qualitative data software. A coding framework of themes is developed based on the RODAM theoretical framework and social representations theory.54 ,55 Coding is carried out inductively and deductively through a constant comparative approach. All transcripts are coded separately by two independent researchers and are systematically discussed and compared for inter-rater reliability.
Current status of the study
The RODAM project study is currently enrolling participants from five localities in four countries. As of January 2014, we have examined and interviewed 3868 participants (rural n=1057, urban Ghana n=863, Amsterdam n=1011, London n=597 and Berlin n=340) who fulfilled the RODAM eligibility criteria. Blood and urine samples from these participants have been stored at the local sites in Ghana, Amsterdam, London and Berlin. Part of these samples have been successfully shipped from the study sites to Charité—Universitätsmedizin Berlin for biochemical analyses, and to Source Bioscience in Nottingham for DNA extraction. Genotyping will start once all the data collection is completed. The data collection for the qualitative part of the project is ongoing in rural and urban Ghana, Amsterdam and London. Database has been built and the outline of the data storage structure has been defined. The data analysis will begin once the data cleaning is completed.
Discussion
SSA migrants to Europe belong to one of the fastest growing migrant groups in Europe today.56 The unprecedented high levels of CVDs and related risk factors, such as obesity and T2D, have huge clinical care and public health implications. Consequently, the need to get detailed insights into the possible underlying determinants of obesity and T2D and related complications to help support the preventive efforts as well as clinical management is increasingly being recognised. This is particularly so in major European cities where some of these populations form a major part of the patient population.31 Simultaneously, African countries are facing huge challenges regarding obesity and T2D and related complications.7 ,9 This issue was recently highlighted in the meeting of the general assembly of the United Nations on Non-Communicable Diseases in 2011 as an important epidemic of our times (http://www.un.org/en/ga/president/65/issues/ncdiseases.shtml). Unfortunately, the established health education and lifestyle interventions mainly in the European host populations may not be applied in migrant populations and other world regions such as Africa because of differences in susceptibility, nutrition, social circumstances and culture. Still, in Africa and among African migrants, data are highly fragmentary and based on heterogeneous populations. Consequently, the magnitude of the problem is uncertain and the relative contribution of risk factors is undefined. Thus, it is difficult to set rational priorities for targeted health interventions and policies and to monitor progress towards set goals. Knowledge on health-related outcomes that are directly associated with the migration process will allow for the most effective and appropriate use of interventions, efforts and investments to improve and promote the health of these populations.51
Comparative studies such as RODAM have an enormous potential for migrant populations and for the countries from which they have migrated from. For migrant populations, it provides indications of how exposure to different environmental circumstances might influence health outcomes. This is highly relevant in that the industrialised countries themselves differ greatly in terms of opportunities for socioeconomic development of the migrant groups, race relations and access to healthcare and preventive services.57 These differential contexts can undoubtedly influence health behaviour and healthcare use among migrant groups, and subsequently lead to differences in health outcomes between similar migrant populations living in different countries.30 ,32 For the countries of origin, the rapid increases of obesity and T2D following migration to high-income countries give a clear indication of the vulnerability of the population left behind as many of these countries continue to westernise.57
The high prevalence of obesity and T2D among migrant groups obviously is a result of a multitude of different factors. Thorough understanding of the factors is a prerequisite for efficient intervention and prevention. The rigorous characterisation of biochemical parameters and specific environmental factors as well as epigenetic factors will allow comparing the major pathophysiological aspects of obesity and T2D between African migrants and their compatriots who did not migrate. Epigenetic data have a huge potential to point to, as yet, unrecognised pathophysiological pathways in obesity and T2D, and thus reveal options for improved diagnosis and treatment.
The RODAM project will deliver up-to-date data on obesity and T2D among SSA migrants in Europe and their home country. This will allow us to draw conclusions on the magnitude of the problem and deduce the attributable risk of migration from rural to urban environment as well as migration to Europe for obesity and T2D. Our findings on the influence of migration (from Africa to Europe) will help healthcare providers and health policy stakeholders to better understand and predict comparable developments in other African populations and in other parts of the world; and to (re)direct efforts to the most obvious changes induced by migration that affect obesity and diabetes.
References
Footnotes
-
Correction notice This article has been corrected since it was published Online First. The license has been change to CC BY and the funding statement has been updated.
-
Acknowledgements The authors are very grateful to the advisory board members for their valuable support in shaping the methods, and to the Ghanaian volunteers participating in this project.
-
Contributors CA, EO-D, Ad-GA, LS, JA, FM, ID, MBS, JS, K-KG, SB, AH-Z, AEK and KS developed the original grant proposal. CA, EB and KM prepared the first draft with the support of all authors. All authors read and approved the final manuscript.
-
Funding This work is supported by the European Commission under the Framework Programme (grant number 278901). Professor Smeeth's contribution was supported by the Wellcome Trust, grant number WT082178.
-
Competing interests None.
-
Patient consent Obtained.
-
Ethics approval Ethical approval of the study protocols has been requested at all sites from the respective ethics committees in Ghana (School of Medical Sciences/Komfo Anokye Teaching Hospital Committee on Human Research, Publication & Ethical Review Board), the Netherlands (Institutional Review Board of the AMC, University of Amsterdam), Germany (Ethics Committee of Charite-Universitätsmedizin Berlin) and the UK (London School of Hygiene and Tropical Medicine Research Ethics Committee) before data collection began in each country
-
Provenance and peer review Not commissioned; peer reviewed for ethical and funding approval prior to submission.
Linked Articles
- Correction