Article Text

Abstract
Introduction There is growing interest in the use of low tidal volume ventilation in patients undergoing general anaesthesia. However, its potential benefit has long been debated and conflicting results have been reported. We describe here the protocol of a systematic review and meta-analysis for investigating the beneficial effects of low tidal volume ventilation in patients undergoing general anaesthesia.
Methods and analysis Data sources include PubMed, Scopus, Embase and EBSCO. Patients undergoing general anaesthesia will be included irrespective of type of surgery. The intervention is low tidal volume ventilation or protective ventilation, and the control is conventional ventilation. The quality of included trials will be assessed by using Delphi consensus. Outcomes include new onset lung injury, atelectasis, arrhythmia, levels of inflammatory biomarkers, arterial oxygenation, partial pressure of carbon dioxide and alveolar–arterial oxygen gradient. Conventional approaches for meta-analysis will be used, and heterogeneity will be investigated by using subgroup analysis and meta-regression if appropriate. The Bayesian method will be used for the synthesis of binary outcome data.
Ethics and dissemination The systematic review was approved by the ethics committee of Jinhua hospital of Zhejiang university and will be published in a peer-reviewed journal and will be disseminated electronically and in print.
Registration details The study protocol has been registered in PROSPERO (http://www.crd.york.ac.uk/PROSPERO/) under registration number CRD42013006416.
- mechnical ventilation
This is an Open Access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 3.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/3.0/
Statistics from Altmetric.com
Introduction
It is estimated that 234.2 million cases (95% CI 187.2 to 281.2) of major surgery were carried out worldwide in 2004, corresponding to about one operation for every 25 people.1 Postoperative pulmonary complications associated with general anaesthesia are a major cause of perioperative mortality and morbidity.2–4 The induction of general anaesthesia may cause a significant decrease in lung volume and atelectasis, which in turn results in impairment in gas exchange and pulmonary mechanics.5 ,6
A large body of evidence from animal experiments has demonstrated that mechanical ventilation can initiate lung injury, even in healthy lungs.7–9 Serpa Neto and colleagues, in a meta-analysis of 20 papers involving 2822 patients without acute respiratory distress syndrome (ARDS), found that protective ventilation with lower tidal volumes was associated with a decrease in lung injury (risk ratio (RR) 0.33, 95% CI 0.23 to 0.47; p<0.001) and mortality (RR 0.64, 95% CI 0.46 to 0.89; p=0.007).10 However, five observational studies included in this meta-analysis accounted for approximately 85% of both the number of patients and events in the primary analysis of lung injury prevention.11 Furthermore, the effect of positive end-expiratory pressure (PEEP) was not explored in this meta-analysis, as PEEP levels were comparable between the study and control arms in some studies but significantly different in other studies. As a result, the use of lung protective ventilation in patients undergoing major surgery still remains controversial.11 ,12
Since 2009, a number of prospective randomised trials have been performed to investigate the efficacy of lung protective ventilation in patients without ARDS.13–21 We describe here the protocol of a systematic review to investigate whether lung protective ventilation is beneficial in patients undergoing major surgery. This systematic review has been registered with PROSPERO (the NIHR International Prospective Register of Systematic Reviews) under registration number CRD42013006416.
Methods
Search methods for identifying studies
Electronic searches
We will search the databases PubMed, Scopus, EBSCO and Embase from inception to November 2013. There will be no language restrictions in the electronic search for trials.
Search terms/search strategy
The search strategy has been developed for PubMed and consists of terms related to surgery and lung protective ventilation (table 1). The PubMed strategy will be adapted for the other databases.
PubMed search strategy
Study inclusion criteria
Studies to be included
Studies meeting the following criteria will be included: (1) the study population should consist of patients undergoing mechanical ventilation after induction of general anaesthesia, and can include adults and/or children; (2) the intervention should be lung protective ventilation while the control arm uses the conventional ventilation strategy. Exclusion criteria include: (1) non-experimental studies (observational studies, case–control studies or secondary analysis of data from randomised controlled trials (RCT)); (2) animal studies; and (3) articles such as reviews, comments and letters.
Intervention
Lung protective ventilation, that is, mechanical ventilation with low tidal volumes with or without the differential use of PEEP and/or recruitment manoeuvres. Low tidal volume is defined as ≤8 mL/kg of predicted body weight.
Comparison
Ventilation strategy using the conventional tidal volume of ≥8 mL/kg of predicted body weight as the control.
Outcome
Primary outcomes are incidence of acute lung injury (ALI) and ARDS. ALI and ARDS are defined according to the Berlin definition or the American-European Consensus Conference (AECC) definition.22 ,23 ARDS is defined as the acute onset of hypoxaemia (the ratio of partial pressure of arterial oxygen to fraction of inspired oxygen (PaO2/FiO2)≤200 mm Hg), with bilateral infiltrates on frontal chest X-ray, in the absence of left atrial hypertension (determined by pulmonary capillary wedge pressure <18 mm Hg). ALI was defined by using the same variables but with a less stringent criterion for hypoxaemia (PaO2/FiO2≤300 mm Hg). The Berlin definition states that: (1) onset should be within 1 week of a known clinical insult or new/worsening respiratory symptoms; (2) chest imaging should show bilateral opacities that cannot be fully explained by effusions, lobar/lung collapse or nodules; and (3) respiratory failure not fully explained by cardiac failure or fluid overload should be present; objective assessment may be needed to exclude hydrostatic oedema if no risk factor is present. ARDS is divided into three mutually exclusive categories of mild (200<PaO2/FiO2≤300 with PEEP or continuous positive airway pressure (CPAP)≥5 cm H2O), moderate (100<PaO2/FiO2≤200 with PEEP≥5 cm H2O) and severe (PaO2/FiO2≤100 with PEEP ≥ 5 cm H2O).
Clinical outcomes are intensive care unit length of stay (LOS), hospital LOS and mortality. These definitions may differ across component studies, and we will retrieve the data according to the following definitions:
-
Oxygenation: arterial pH value, PaCO2, PaO2, PaO2/FiO2, alveolar–arterial oxygen gradient
-
Complications: atelectasis, new onset arrhythmia
-
Inflammatory markers in serum and bronchoalveolar lavage fluid: interleukin-6 (IL-6), interleukin-8 (IL-8)
Type of studies
We will include any RCT.
Data collection and analysis
Selection of studies
The initial search and selection of potentially relevant studies by inspection of titles and abstracts will be conducted by three review authors. XHu will search Embase, LChen and XZhang will search PubMed, XZhu and JHuai will search EBSCO, and XZhu and LChen will search Scopus. All these review authors will conduct searches independently. Any disparities will be resolved by a third opinion. The full text of eligible studies obtained in the first step will be reviewed. Any mistakes in the first step or uncertainty about the inclusion or exclusion of a study will be resolved by careful review of the full text article. Corresponding authors will be contacted if further information is needed.
Data extraction and management
A standard form for data collection will be developed. Data will be gathered at study level. The information collected on component studies will include study population, setting, type of surgery, description of surgery (eg, elective vs urgent), blood transfusion, fluid balance, mean or median age, sex (the proportion of male patients), tidal volume settings in the study and control arms, use of recruitment manoeuvres, and PEEP level. If a study reports age separately for the study and control arms, the weighted mean difference will be reported in our analysis. Three investigators (XZ, LC, XH) will independently extract data from component studies and any disagreement will be settled by consulting a fourth investigator (ZZ).
Assessment of the quality of included studies
Quality assessment of all included randomised controlled trials will be based on Delphi consensus (table 2), which covers the following eight aspects: sequence generation, allocation concealment, blinding, eligibility criteria, baseline characteristics, use of point estimates and variability, intention-to-treat analysis, and sample size calculation.24
Format for assessment of methodological quality adapted from Delphi consensus
Statistical analysis and data synthesis
Two categories of data will be reported as study endpoints in the present analysis: binary outcome measuring the risk of specific events (such as the occurrence of ALI, new onset arrhythmia and death) and continuous outcomes (such as the level of inflammatory markers, LOS, PaO2/FiO2 and PaCO2).
Report of effect size
The effect size of component studies will be pooled by using the inverse-variance method.25 Mantel–Haenszel methods will be used in situations where there are few events. For instance, because mortality is expected to be low in patients undergoing general anaesthesia, the Mantel-Haenszel method will be used for the synthesis of RR or OR for mortality. For continuous outcomes, we will use the mean difference as the effect size. However, because the types of inflammatory markers vary across studies, even if two studies report the same marker, the sample used can be different. We believe that it is more relevant to report whether the use of lung protective ventilation can reduce proinflammatory cytokines, while absolute values are not so important. Therefore, we will use standardised mean difference to combine these results, in which the standard deviations are used to standardise the mean differences to a single scale.
Assessment of heterogeneity
Heterogeneity will be assessed by using statistic I2, where I2=0% suggests no observed heterogeneity, and larger values indicate increasing heterogeneity. I2 will be calculated according to the equation I2=100% × (Q−df)/Q, where Q is the Cochran heterogeneity statistic. We predefine that I2>50% indicates statistically significant heterogeneity.26 A random effect model will be used to synthesise the pooled effect size when there is significant heterogeneity; otherwise, a fixed effect model will be used.
Subgroup analysis
Subgroup analysis will be used to explore heterogeneity among component studies. We believe that differential use of tidal volume, PEEP and recruitment manoeuvre (open lung technique) between the study and control arms may confound outcome, and so we will perform subgroup analysis on these variables. Furthermore, patients undergoing urgent surgery may differ from those undergoing elective surgery in that they may have risk factors for ARDS (sepsis, shock, organ failure, multiple blood transfusions) and therefore have a different basal status compared with those undergoing scheduled major surgery. Subgroup analysis will also be performed on patients undergoing urgent versus elective surgery. Meta-regression analysis can be employed if the modifying covariates are continuous variables. In the meta-regression model, an outcome variable is predicted according to the values of one or more explanatory variables.27
Sensitivity analysis
Sensitivity analysis will be performed by excluding studies with poor methodological design in order to test the robustness of our results.
Publication bias
Publication bias will be assessed by using Begg's rank correlation test and Egger's regression test.28 A funnel plot will be used to visually assess the presence of publication bias. The OR is plotted on the x-axis against its precision on the y-axis, and asymmetrical distribution of component studies may indicate potential publication bias. Begg's rank correlation test uses the Spearman rank correlation to investigate the relationship between the standardised effect size and sample size or variance in effect size.29 In Egger's regression test, the standard normal deviate (the OR divided by its SE) is regressed against the estimates precision. The intercept of the regression line provides an estimate of asymmetry—the larger its deviation from origin, the more significant the asymmetry.30
Assessment of small-study effects
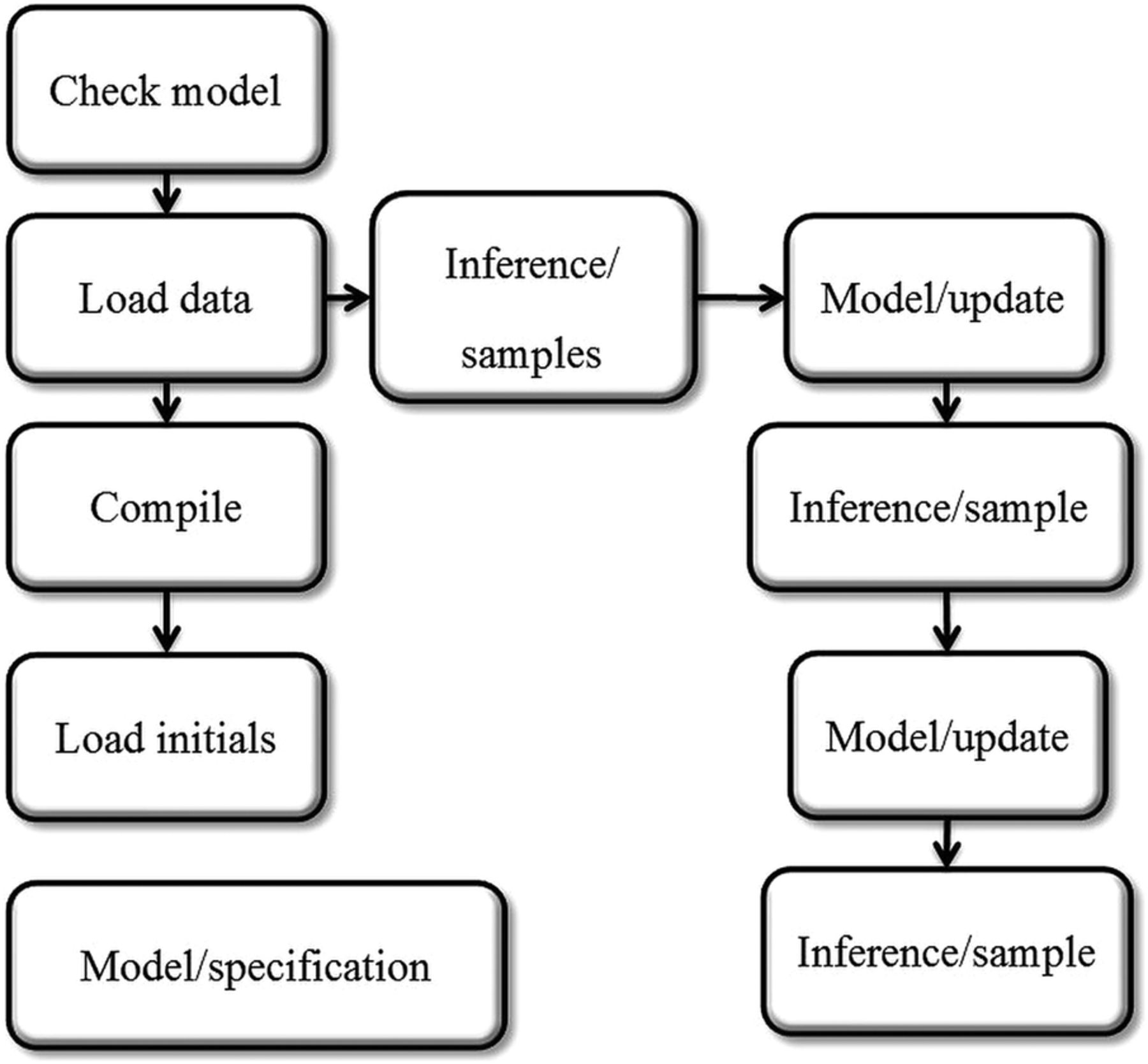
Because the sample sizes of some component studies are expected to be relatively small, a small-study effect may be present.31 As a result, we plan to use the full Bayesian approach to address this issue. Bayesian methods provide a unified modelling framework which overcomes issues including those related to the appropriate treatment of small trials, with flexibility allowing for non-normal distribution for random effects.32 The effect of lung protective ventilation compared with conventional intervention in pulmonary complications, new onset arrhythmia and other binary outcome variables will be assessed by Bayesian random-effect models using WinBUGS V.1.4. The code for the random effect model and the fixed effect model in WinBUGS is given in table 3. Figure 1 shows the WinBUGS flowchart.
Script for running WinBUGS

{kind=link}
WinBUGS flow chart.
Discussion
Despite being the standard of care for the treatment of ARDS,33 it is not clear whether lung protective ventilation offers benefits in healthy lungs. General anaesthesia requiring mechanical ventilation is widely employed during surgery, when the lungs under mechanical ventilation are mostly healthy. The conventional ventilation strategy recommends the use of high tidal volume (10–15 mL/kg predicted body weight) to prevent anaesthesia-induced hypoxaemia and atelectasis. On the other hand, the marked decrease in lung volume following laparotomy might, to some extent, be similar to the findings in patients with ARDS, where only 30–40% of alveoli are normally aerated due to alveolar collapse.34 Lung protective ventilation in this setting might be a rational strategy to prevent ventilator-induced lung injury.
A systematic review has been published by Serpa Neto and colleagues,10 suggesting that lung protective ventilation was associated with better clinical outcomes among patients without ARDS. However, there are major differences between the above study and our planned meta-analysis.
First, five out of 20 clinical trials included in Neto's study were observational studies, which might have significantly compromised the quality of the evidence, and should be regarded as hypothesis generating rather than hypothesis validating.35 In comparison, we will include only prospective randomised trials.
Second, medical patients without ARDS were also included in Neto's study. However, diagnosing ARDS is at times challenging. Among 255 patients who did not meet the clinical diagnostic criteria of ARDS, clinical autopsy found evidence of diffuse alveolar damage in 28 (11%) patients.36 Interestingly, the difficulty of diagnosing of ARDS has not been improved by the Berlin ARDS definition, which had a sensitivity of 89% and specificity of only 63%.37 The benefit of lung protective ventilation is therefore expected and self-explanatory. In our planned meta-analysis, we will only include patients undergoing major surgery in order to minimise the confounding effect of clinical diagnosis.
Last, but not the least, the sample sizes in component studies are relatively small, potentially giving rise to the so-called small-study effect.38 The common approach to meta-analysis is to assume that summary statistics have a normal likelihood, which however is usually not tenable in small trials. One approach to this problem is the use of the Bayesian method. In our analysis, we will employ the Bayesian method for both random-effect and fixed-effect models.
In conclusion, the current meta-analysis is aimed at investigating the beneficial effects of lung protective ventilation including low tidal volume with or without the use of PEEP and/or recruitment manoeuvre, in patients undergoing major surgery. We hope that the result of this meta-analysis will provide additional evidence on the practice of mechanical ventilation during the perioperative period in these patients.
References
Footnotes
-
Contributors BDu conceived the idea and designed the study; ZZhang drafted the manuscript; LZhu, LChen and XZhu collected the data and helped with statistical analysis; and LChen, XHu and JHuai helped to abstract data and review the manuscript.
-
Competing interests None.
-
Ethics approval The study was approved by ethics committee of Jinhua hospital of Zhejiang university.
-
Provenance and peer review Not commissioned; externally peer reviewed.