Article Text

Abstract
Objectives The light-emitting diode (LED) fluorescence microscopy has made acid-fast bacilli (AFB) detection faster and efficient although its optimal performance in resource-limited settings is still being studied. We assessed the optimal performances of light and fluorescence microscopy in routine conditions of a resource-limited setting and evaluated the digestion time for sputum samples for maximum yield of positive cultures.
Design Cross-sectional study.
Setting Facility-based involving samples of routine patients receiving tuberculosis treatment and care from the main tuberculosis case referral centre in northern Nigeria.
Participants The study included 450 sputum samples from 150 new patients with clinical diagnosis of pulmonary tuberculosis.
Methods The 450 samples were pooled into 150 specimens, examined independently with mercury vapour lamp (FM), LED CysCope (CY) and Primo Star iLED (PiLED) fluorescence microscopies, and with the Ziehl-Neelsen (ZN) microscopy to assess the performance of each technique compared with liquid culture. The cultured specimens were decontaminated with BD Mycoprep (4% NaOH–1% NLAC and 2.9% sodium citrate) for 10, 15 and 20 min before incubation in Mycobacterium growth incubator tube (MGIT) system and growth examined for acid-fast bacilli (AFB).
Results Of the 150 specimens examined by direct microscopy: 44 (29%), 60 (40%), 49 (33%) and 64 (43%) were AFB positive by ZN, FM, CY and iLED microscopy, respectively. Digestion of sputum samples for 10, 15 and 20 min yielded mycobacterial growth in 72 (48%), 81 (54%) and 68 (45%) of the digested samples, respectively, after incubation in the MGIT system.
Conclusions In routine laboratory conditions of a resource-limited setting, our study has demonstrated the superiority of fluorescence microscopy over the conventional ZN technique. Digestion of sputum samples for 15 min yielded more positive cultures.
- Microbiology
This is an Open Access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 3.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/3.0/
Statistics from Altmetric.com
Strengths and limitations of this study
-
The design of this study allows test performance assessment under routine (real) resource constrain settings.
-
Blinding the microscopist on the clinical or laboratory diagnosis associated with the samples examined minimised bias in the interpretation of direct smear results.
-
However, our inability to obtain participant HIV status deprived us the ability to measure its impact on the performance of the techniques and the culture outcomes at different decontamination exposures.
Introduction
Globally, an estimated 1.4 million deaths occurred in 2011 as a result of infection with tuberculosis, one-fourth of the deaths were associated with HIV infection and most of it in resource-limited settings (RLS)1 where the burden of HIV infection is high. In Africa, tuberculosis (TB) is the leading cause of death among persons with HIV infection as the continent harbours 80% of the world HIV-TB cases.2 Nigeria and the Republic of South Africa are among the top five TB burden nations of the world. Sensitive, specific and inexpensive point-of-care diagnostic tools for rapid TB detection are lacking posing challenges to the optimal diagnosis of TB in RLS, particularly among persons with HIV infections whose sputum specimen often lack sufficient quantity of acid-fast bacilli (AFB) detectable on routine smear examination.3 ,4
The simplicity, inexpensiveness and predictive power of the Ziehl-Neelsen (ZN) sputum smear microscopy make it the applicable laboratory diagnostic tool of choice for tuberculosis in RLS.5 A properly performed positive sputum-smear is highly predictive of active TB.6 ,7 Unfortunately, the sensitivity of sputum-smear microscopy is low and its performance is often affected by lack of proper maintenance of equipment; trained manpower and quality assurance system in settings where resources are scarce.8 Even in centres with good quality assurance measures, smear microscopy detects only 40–50% of TB cases compared with about 80% yield by culture.9 However, it remains the only available tool for bacteriological diagnosis of TB in most RLS. Culture techniques are highly sensitive and specific, but the cost, technical complexity and time delay before results are available make culture not scalable for rapid detection and treatment of tuberculosis. Recent advances have made it possible to use molecular technology to detect mycobacterial DNA with great accuracy. However, these technologies still require a fairly developed laboratory with a reliable source of electricity.
The detection of smear positive cases is the priority in TB control programmes. These cases are infectious and contribute substantially to the transmission of the disease.10 ,11 In recent years, several new laboratory techniques have been developed to significantly improve the ability to diagnose active TB in populations. Fluorescence microscopy improves the sensitivity of sputum-smear detection of TB and has good specificity relative to the conventional ZN method. Inexpensive light-emitting diode-based (LED) fluorescence microscopes have been developed to make microscopy of smears stained by Auramine fluorescence dye easier, cheaper and faster with potentials for scalability to remote clinics in RLS.5 ,12–14
This study compared the performance of the standard but more expensive mercury vapour lamp fluorescence microscope (FM); the newer, less expensive LED based CysCope (CY) (Partec, Görlitz, Germany); and the Primo Star iLED (PiLED) (Carl Zeiss Inc, Germany) fluorescence microscopes in comparison to the conventional light (ZN) microscope against the gold (reference) standard of liquid culture in automated BACTEC MGIT 960 machine (Becton Dickinson Diagnostic Instrument Systems) for the detection of AFB from sputum samples of patients with clinical pulmonary tuberculosis (TB). In addition, we evaluated the optimal digestion time with Mycoprep (4% NaOH−1% NLAC and 2.9% sodium citrate) for liquid culture in this population. Prolonged decontamination time is reported to reduce the number of viable bacilli and different digestion methods yield a variable number of positive cultures.15–17
Methods
Study population
Three sputum samples (spot-morning-spot) were collected from 150 TB treatment naïve, consecutive patients with clinical diagnosis of pulmonary TB at the National TB and Leprosy Training Centre (NTBLTC), Zaria, Nigeria. Routine and referred cases of TB from northern Nigerian region receive TB treatment and care at this facility. The spot-morning-spot sample collection was the standard routine for the diagnosis of TB in Nigeria at the time of the study. The flow chart in figure 1 provides an overview of the study design. Ethical review was waived because in the opinion of the study centre review committee there was no potential risk to participants’ safety, privacy or confidentiality since there was no formal contact between investigators and participants either directly (interview, questionnaires, etc) or indirectly (medical records, personal identifiers, etc). The sputum specimens provided for routine clinical care services were completely anonymised before they were analysed for the study and there was no risk that the pooled samples can be de-anonymised through data linkages. This study was conducted from July to September 2009.

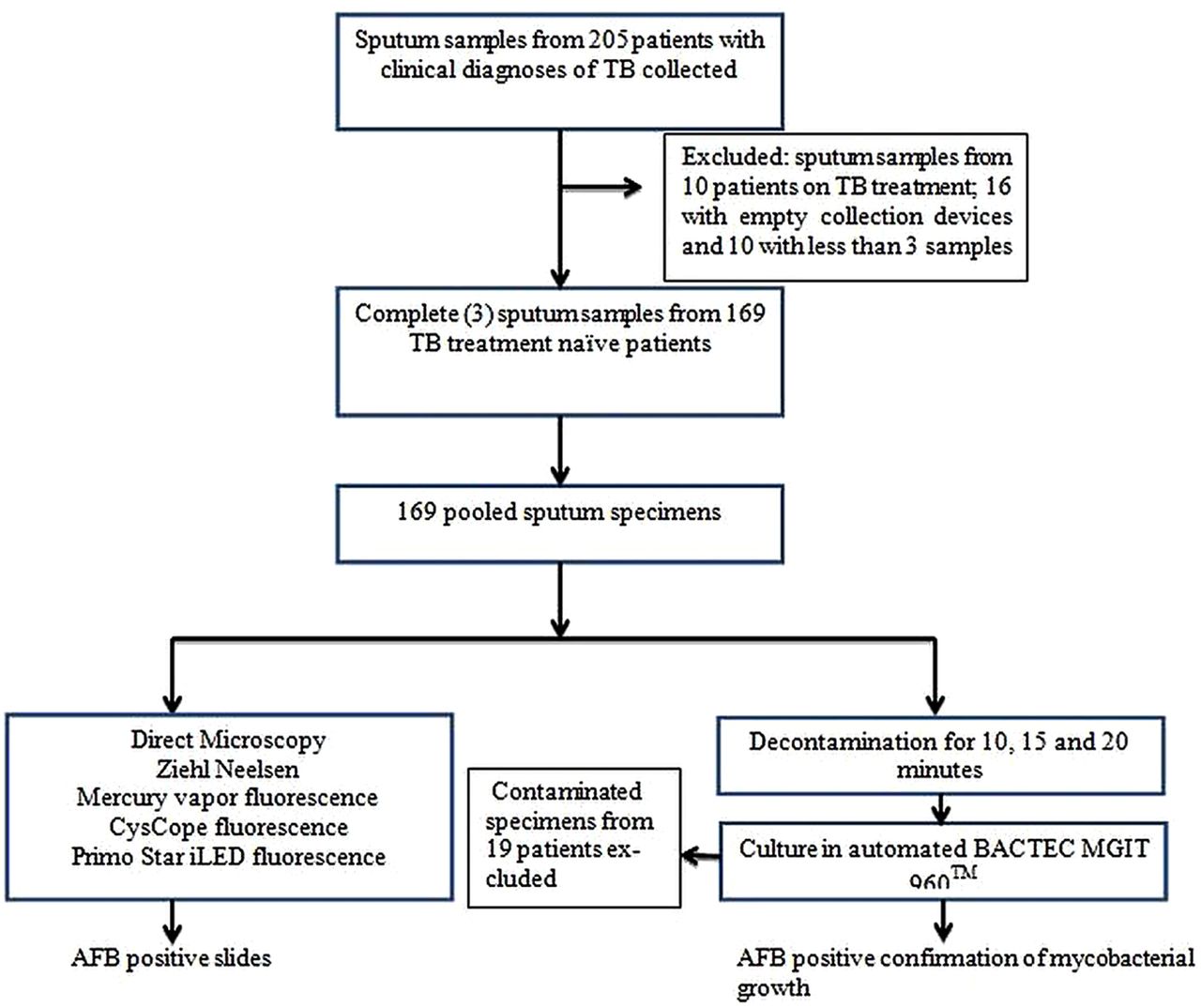{kind=link}
Flow chart for the study design involving 450 sputum samples from 150 patients with clinical tuberculosis.
Smear microscopy
The three sputum samples from each patient were pooled. Four direct smears were made from each of the pooled sputum samples with applicator sticks on clean grease-free slides; measuring 2 cm×3 cm, and not too thick. The first slide was stained with Ziehl-Neelsen (ZN) stain according to the WHO recommended protocol described elsewhere.18 Briefly, the smear was air dried and fixed by gently passing it over a flame 2–3 times. One per cent strong carbol-fuchsin was applied to the slide and heated with a Bunsen flame intermittently three times and allowed to stain for 15 min. The stain was rinsed off with tap water and 3% acid alcohol was applied on the smear for 3 min. Methylene blue (0.3%) was then added for up to 1 min and rinsed off with tap water. Positive and negative controls were included in the process. Slide examination was performed with light microscope at ×1000 magnification and the AFBs identified were graded according to the International Union against Tuberculosis and Lung Disease (IUATLD) and the WHO smear grading scale.19
The second, third and fourth slides were air-dried, heat-fixed and stained with Auramine O-phenol for 15 min rinsed with tap water, decolourised with 1% acid alcohol for 2 min then rinsed with water and counterstained with 0.1% potassium permanganate for 2 min. The slides were rinsed with water then allowed to dry in air before examination under FM, CY and PiLED microscopes, respectively. The AFBs were visualised and graded at magnifications of ×200 and ×400 according to a protocol describe by Lehman.20 A total of 100 microscopic fields were examined before a slide was recorded as positive (if at least an AFB was seen) or negative (if no AFB was seen). Positive smears were graded as scanty (actual) if there were: 1–9 AFBs in at least 100 fields; +1: 10–99 in 100 fields; +2: 1–10 per field in at least 50 fields; and +3: if there were more than 10 per field in at least 20 fields. Absence of any AFB was graded as negative smear. Each slide was examined by three independent readers to ascertain the presence of AFB and grade positive smears. The slide readers were blinded on the clinical and laboratory diagnoses of the participants whose samples were studied.
Specimen culture
Each of the 150 pooled sputum specimens were decontaminated with BD Mycoprep (Beckton Dickinson Diagnostic Systems, Sparks, Maryland, USA) which consists of 1% N-acetyl-l-cysteine (NALC), 4% sodium hydroxide and 2.9% sodium citrate. An equal amount of Mycoprep was added to the sputum, homogenised and allowed to act for 10, 15 and 20 min, respectively. After the respective digestion period, phosphate-buffered saline was added to stop the digestion and decontamination reaction. This was then centrifuged under refrigerated conditions with uniform centrifugation time of 15 min and a relative centrifugal force (RCF) of 3000×g. The supernatants were discarded and the sediments re-suspended with 1 mL of phosphate-buffered saline to make a final volume of 2 mL. Then 0.5 mL of each was inoculated into Mycobacterium growth indicator tubes (MGIT) and incubated in the automated BACTEC MGIT 960 machine (Becton Dickinson Diagnostic Instrument Systems), which monitors growth. Positive and negative control culture tubes were also set up along each test using Mycobacterium tuberculosis H37Ra (ATCC 25177—attenuated strain) and sterile distilled water, respectively.
The cultures that indicated positive growth were removed from the machine and the presence of AFB confirmed by ZN smear microscopy. Those that do not indicate growth after 42 days were classified as negatives as recommended by the manufacturer and as was the standard practice. All cultures were performed at Zankli Research laboratory while all microscopy were performed at the NTBLTC, Zaria to minimise interference with the outcome of culture or direct microscopy results.
Statistical analysis
The raw data generated from the smear microscopic examinations of the 150 matched samples by the four different microscopes as well as the data generated after the same samples were cultured following decontaminations (digestions) at 10, 15 and 20 min were organised into cell counts in which descriptive values were provided along with frequencies and proportions. Measures of accuracy for the different smear examinations: sensitivity, specificity, positive and negative predictive values were evaluated through decision matrix tables while concordance and disagreements between the microscopic examination by each of the three fluorescence microscopes and the conventional light (ZN) microscope based on the final classification of samples by the gold standards (outcomes of MGIT cultures) were examined in matched sample tables for positive and negative final outcomes as previously recommended for comparative analysis of diagnostic procedures performed on same samples (patients).21 Comparison between the fluorescence microscopies to the conventional ZN microscopy for differences in performance together with their 95% CIs was performed using the McNemar's test. Significance of association was set at 0.05 α and all probabilities were two-tailed.
Results
Of the 150 matched (paired) samples, AFBs were detected in: 44 (29%) of the ZN smears examined under light microscope; 60 (40%) of the AR smears examined with FM; 49 (33%) of the AR smears examined with CY; and 64 (44%) AR smears examined with PiLED fluorescence microscopes. MGIT cultures of the 150 specimen yielded 72 (48%), 81 (54%) and 68 (45%) AFB confirmed growths after decontamination for 10 (A), 15 (B) and 20 (C) min, respectively, prior to incubation.
Among the positive AFB tests graded, ZN light microscopy produced the highest proportion of samples with scanty AFBs on examination 21/44 (48%), followed by PiLED fluorescence microscopy 12/64 (19%), then CY 8/49 (16%) and FM had the least scanty AFB-positive counts 3/60 (5%). However, after the samples with scanty positive AFBs were incubated in A, B and C MGIT culture groups, the proportions of confirmed mycobacterial growths in the sequence above were as follows: (1) ZN: 14/21 (67%), 9/21 (42%) and 11/21 (52%); (2) PiLED: 5/12 (42%), 7/12 (58%) and 5/12 (42%); (3) CY: 6/8 (75%), 4/8 (50%) and 3/8 (38%); finally (4) FM: 0/3 (0%), 1/3 (33%) and 1/3 (33%). A summary of the positive AFB outcomes from the direct smear examinations by microscopy types, grades and the proportions of graded smears confirmed by the MGIT cultures were provided in table 1.
Proportions of positive graded direct smears confirmed by cultured specimen decontaminated at 10 (A), 15 (B) and 20 (C) min obtained from 150 matched samples
A comparison of the direct smear test results with the final culture outcomes to measure the performances of the direct smear techniques against the gold standards showed that of the 44 AFB-positive samples identified by the ZN microscopy; 36 (81.8%), 29 (65.9%) and 31 (70.5%) were culture confirmed after 10, 15 and 20 min decontamination, respectively. Similarly, of the 60, 49 and 64 AFB-positive samples identified by the FM, CY and PiLED microscopy techniques the frequencies and proportions of the culture confirmed samples were: 44 (73.3%) 36 (60) and 35 (58.3%) for FM; 39 (79.6%), 33 (67.3%) and 33 (67.3%) for CY; and 43 (67.2%) 39 (56.3%) and 39 (56.3%) for PiLED at decontamination times of 10, 15 and 20 min, respectively. There were near identical frequency distributions for the true positive (TP), false positive (FP), false negative (FN) and true negative (TN) for the ZN and CY microscopy techniques while the FM microscopy yielded a pattern of distribution similar to that of PiLED technique as shown in the decision matrix of table 2.
Decision matrix for the evaluation of performance of the direct smear methods against the different gold standards for the 150 matched samples
The levels of agreement and differences between the convention ZN microscopy and each of the fluorescence microscopy techniques with respect to the final culture results were demonstrated by the concordance and discordance cells displayed in table 3. Cells were discordant if the outcomes of the two techniques disagreed, otherwise they were concordant. The statistical significance of the difference in the performance of the techniques compared was derived from the discordant cell. The sum of the frequencies of the discordant cells, for example, that explained the differences between ZN and CY were 7, 4 and 2 for the positive culture results which showed less consistent divergence compared with 6, 6 and 7 for the negative culture results of the same techniques. The sum of the discordant frequencies between ZN and FM, and between ZN and PiLED were higher relative to those between ZN and CY.
Matched sample frequency cells for the agreement and discordance between the standard of care (ZN smear) and FM, CY and PiLED smears on the culture positive and negative specimens
The ZN technique was consistently less sensitive compared with any of the fluorescence techniques against any of the gold standards. The FM fluorescence technique was 11.1%, 8.6% and 5.9%; CY method was 4.2%, 4.9% and 3.1% while PiLED was 9.7%, 12.3% and 11.8% more sensitive than ZN microscopy for the different digestion times of 10, 15 and 20 min, respectively (Pfm=0.027, 0.023, 0.289; Pcy=0.450, 0.134, 0.479 and Piled=0.046, 0.004, 0.043). Conversely, the FM was: 10.2%, 13.1% and 14.6%; CY was 2.5% 2.5% and 3.6%; and PiLED was 16.6%, 1.4% and 14.6% less specific compared with the ZN microscopy for the same digestion times above (Pfm=0.182, 0.016, 0.006; Pcy=0.684, 0.684, 0.131 and Piled=0.006, 0.131 and 0.004). They were also less predictive than the ZN technique (table 4).
Summary measures of performance of the direct smear diagnostic tests for 150 matched samples and the statistical differences in sensitivity and specificity of FM, CY and PiLED in comparison with ZN
Discussion
The findings of this study further confirm the previously reported superior performance of fluorescence microscopy over the conventional ZN technique for AFB detection.22–24 The direct smear staining sensitivities of FM and PiLED fluorescence techniques are on the average 10% more sensitive than the standard of care (ZN method). The reverse is however true for specificity, the fluorescence methods are less specific than ZN by similar percentage points and these differences are statistically significant. Similar trends of high sensitivity and low specificity were observed in the performance of fluorescence microscopy in comparison with the conventional ZN technique24–26 Within the fluorescence techniques FM and PiLED have similar performance measures with little or no differences which is in agreement with the reported findings by Marais et al.27 The CY technique appears to be less sensitive compared with FM and PiLED but on the average have 4% staining sensitivity advantage over the conventional ZN. Similar findings were reported from a resource constrained setting with comparable optimal technical conditions in which such differences were found to be marginally significant statistically.20 However, both CY and ZN staining techniques have higher specificities compared with FM and PiLED across all the three reference (gold) standards used.
Although less sensitive, the ZN staining seems to be the most predictive: a positive test has the highest chance of being a true case of TB while a negative test is less likely to harbour the disease. The CY has similar predictive probabilities; however, these measures are affected by disease burden. In high prevalence settings, the positive predictive value of a test increases because it is more likely that those who test positive truly have disease than if the test was performed in settings with low prevalence. Likewise, in settings with low prevalence it is more likely that those who test negative truly do not have the disease. In contrast, sensitivity and specificity measures are less susceptible to influence by disease prevalence. The search for an optimal tuberculosis diagnostic test is motivated by the unacceptably low sensitivity of the conventional ZN smear microscopy over which fluorescence microscopy has shown consistent superiority. In this setting, the TB prevalence is high and may be driven by HIV. Priority should therefore be given to sensitivity over predictive value since failure to detect TB in patients coinfected with HIV is more likely to increase morbidity and mortality among those with HIV infection than false detection of TB.
In addition to improved TB case detection in samples with low-density bacilli, which is aided by its low-power objective, previous studies reported that fluorescence microscopy requires less than 25% of the time taken to read slides using the conventional ZN technique-meaning a microscopist can examine four times the number of slides per day with the fluorescence technique.20 ,28 However, the use of mercury vapour or halogen lamp as the source of light in the standard fluorescence microscopy technique (FM) is expensive and requires frequent replacement because of their shorter life span making it economically inefficient for use in resource-constrained settings. The LED-based microscopes (CY and PiLED) on the other hand are structurally built to overcome the hard operational environment of RLS where continuous supply of electricity, sufficient equipment and trained personnel are a frequent challenge. The LED microscopes use lamps that are inexpensive with much longer life span. They are also simple to operate; and no dark room is required.
The scanty-positive findings are more commonly seen with ZN technique and least with the FM. This could be attributed to the low-power objective of the fluorescence techniques that allow the field to be seen larger than in the conventional ZN light microscopy. Some of the samples studied may have come from HIV co-infected patients with low-density bacilli yielding scanty AFBs on the conventional ZN microscopy and earning a grade of 1+ or more when viewed under the fluorescence techniques. However, the fluorescence techniques recorded the highest numbers of false positives compared with the ZN judging from the reported frequencies in the decision matrix table. This is expected because the low-threshold of the fluorescence techniques derived from their low-power objective could allow naturally fluorescent particles present in the sputum, certain spores, fungi to appear AFB positive which may otherwise be negative on ZN microscopy. These and the fact that a significant proportion of the samples studied may have come from patients co-infected with HIV could also explain the particularly low specificity of the PiLED technique. Associated HIV infection was believed to account for low specificity of LED-FM microscopy compared with the conventional ZN microscopy in two previous studies in settings with high burden of the disease29 ,30
As expected, the digestion and decontamination with NALC–sodium hydroxide (NaOH) produces the highest yield of AFB in the sputum exposed to the reagent for 15 min. This shows that the manufacturer's recommended exposure time of 15 min works well in the hard operational environment of a RLS. The 10 min alternative yielded a little less AFB than the 15 min duration probably because the time is not enough to allow complete digestion of the thick sputum which allows the release of mycobacteria and their subsequent concentration by centrifugation. The 20 min exposure on the other hand might have been prolonged beyond the optimal duration necessary and the toxic effect of the reagent kills not only the contaminating normal flora that may overgrow in cultures making it hard to detect the presence of the mycobacteria but also the mycobacteria itself. The success of this process is dependent on the concentration of the reagent, the exposure time, centrifugation and the temperature selected. In this case all other factors were kept constant and only the exposure time was altered.
Some of the reasons for the unusually high proportion of AFB positive, culture negative specimen could possibly be that some of the patients contrary to their claim have actually been on TB treatment at presentation. This may have adversely hindered the bacilli ability to grow, or more importantly in this case, the bacilli may have been killed by the excessive decontamination in the samples decontaminated for up to 20 min especially among cases with paucibacillary disease due to HIV co-infection. These patients may likely test positive to both smear microscopy and culture in repeat examinations with optimal decontamination time. Fungal infections are also not uncommon in the study area and together with some artefacts may have added to the high frequency of the smear positive, culture negative findings.
The design of this study allows test performance assessment under routine (real) resource constrain settings. The point estimates obtained are more likely to represent the expected outcomes in similar settings with high prevalence of TB. Blinding the readers on the clinical or laboratory diagnosis associated with the samples examined minimised bias in the interpretation of the direct smear results. However, our study had a few limitations: we did not obtain participants’ HIV status and therefore were unable to measure its impact on the performance of the techniques and the culture outcomes at different decontamination exposures. The time taken to read slides was also not reflected in the analysis because only estimates of the time taken to read the slides were recorded since the different technicians who read the slides had different proficiency levels and some accurately read the slides much faster than others.
In summary, the high sensitivity for AFB detection shown by the inexpensive light-emitting diode based Primo Star iLED FM in the hard operational conditions of a RLS underscores the potentials for its scalability to remote clinics in similar settings. This will increase TB detection and improve TB treatment uptakes in high burden settings with scarce resources. The optimal exposure duration for decontamination of sputum samples prior to examination and culture using the NALC)–sodium hydroxide (NaOH) reagent in this setting is 15 min.
Acknowledgments
The authors thank the management and staff of the Zankli Medical Centre and the National Tuberculosis and Leprosy Training Centre for their support in the conduct of this study.
References
Footnotes
-
Contributors AA conceived and designed the study, was involved in data collection, revised the article's intellectual content and approved the final version for publication. She is the guarantor of this paper. LL designed tools for data collection, monitored data collection, revised and approved the draft paper. AN collected, cleaned, analysed and wrote the initial draft of the paper. GA designed the analysis plan, cleaned, analysed the data, drafted and revised the paper. OO, PM, TJ, MI, EN and OnO, implemented the study, collected and cleaned the data and wrote the method section of the paper. PD contributed in the conception and design of data collection, supervised data collection and revised the draft paper.
-
Funding This research received no specific grant from any funding agency in the public, commercial or not-for-profit sectors.
-
Competing interests None.
-
Ethics approval Ethic review committee at the Zankli Medical Centre.
-
Provenance and peer review Not commissioned; externally peer reviewed.
-
Data sharing statement No additional data are available.