Article Text

Abstract
Introduction Fewer than half of all people at highest risk of a cardiovascular event are receiving and adhering to best practice recommendations to lower their risk. In this project, we examine the role of an e-health-assisted consumer-focused strategy as a means of overcoming these gaps between evidence and practice. Consumer Navigation of Electronic Cardiovascular Tools (CONNECT) aims to test whether a consumer-focused e-health strategy provided to Aboriginal and Torres Strait Islander and non-indigenous adults, recruited through primary care, at moderate-to-high risk of a cardiovascular disease event will improve risk factor control when compared with usual care.
Methods and analysis Randomised controlled trial of 2000 participants with an average of 18 months of follow-up to evaluate the effectiveness of an integrated consumer-directed e-health portal on cardiovascular risk compared with usual care in patients with cardiovascular disease or who are at moderate-to-high cardiovascular disease risk. The trial will be augmented by formal economic and process evaluations to assess acceptability, equity and cost-effectiveness of the intervention. The intervention group will participate in a consumer-directed e-health strategy for cardiovascular risk management. The programme is electronically integrated with the primary care provider's software and will include interactive smart phone and Internet platforms. The primary outcome is a composite endpoint of the proportion of people meeting the Australian guideline-recommended blood pressure (BP) and cholesterol targets. Secondary outcomes include change in mean BP and fasting cholesterol levels, proportion meeting BP and cholesterol targets separately, self-efficacy, health literacy, self-reported point prevalence abstinence in smoking, body mass index and waist circumference, self-reported physical activity and self-reported medication adherence.
Ethics and dissemination Primary ethics approval was received from the University of Sydney Human Research Ethics Committee and the Aboriginal Health and Medical Research Council. Results will be disseminated via the usual scientific forums including peer-reviewed publications and presentations at international conferences
Clinical Trials registration number ACTRN12613000715774.
- Preventive Medicine
- Primary Care
This is an Open Access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 3.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/3.0/
Statistics from Altmetric.com
Strengths and limitations of this study
-
In this project, we will examine the role of an integrated e-health consumer strategy as a means of overcoming such health system inefficiencies.
-
The Consumer Navigation of Electronic Cardiovascular Tools (CONNECT) study will generate rigorously evaluated findings on an issue of national and international importance.
-
The development of a content-rich, consumer-focused e-health intervention that is fully integrated with primary healthcare system will greatly inform the e-health agenda.
-
If effective, the CONNECT e-health strategy could be upscaled and expanded to increase compliance with international e-health strategies. The CONNECT strategy may also have applicability as a standalone strategy where electronic integration with primary care is unavailable.
-
Potential limitations are that this is an Australian study and relies on integration with the Australian personally controlled e-health record. In addition, the intervention is primarily consumer driven.
Introduction
Cardiovascular disease burden
Cardiovascular disease (CVD), including coronary heart disease and stroke, is the leading cause of death and disease burden globally.1 Importantly, in Australia, Aboriginal and Torres Strait Islander peoples experience approximately five times greater CVD burden than other Australians.2 Fewer than 50% of adults who attend Australian general practice or Aboriginal Community Controlled Health Services (ACCHSs) are adequately screened for vascular risk, and for those identified at high risk, only about 40% are receiving best practice care.3–5 Similar findings have been noted in other Australian studies.6–9 Adherence rates to lifestyle modification are around 30%10 and adherence to recommended medicines may be as low as 50% after 6 months of therapy.11 Overall, these studies have demonstrated failure to adequately implement effective interventions (that are also adhered to) to lower CVD risk for those who need it most.
Consumer-focused e-health interventions
During the past decade, there has been rapid development in consumer e-health. Several studies have shown the benefits of interactive Internet portals for managing chronic conditions (asthma,12–14 type 2 diabetes,15 arthritis,16 hypertension17 and mental health18 ,19), for health behaviour change20 ,21 and lifestyle risk factors (physical activity,22 smoking cessation23 and weight loss).24 A Cochrane review of 124 studies concluded that computer-based ‘Interactive Health Communication Applications’ can also improve cognitive and social outcomes of patients with chronic conditions.25 The emerging evidence on text message interventions also appears promising. Five randomised controlled trials (RCTs) have demonstrated the effectiveness of mobile phone text messaging to promote smoking cessation,26 ,27 and a number of small RCTs have shown improved outcomes related to weight loss,28 physical activity,29 asthma medication adherence,30 glycaemic control in diabetes,31 blood pressure (BP) lowering,32 liver transplantation33 and HIV treatment.34 Other studies looking at text messaging systems to improve adherence to lifestyle and medication recommendations for people with established coronary artery disease are ongoing.35 ,36
Although the evidence for consumer-focused interventions is promising, there are few randomised evaluations of personally controlled e-health records (PCEHRs).37 The PCEHR is the Australian secure online summary of an individual's health information. This e-health record allows people, their doctors, hospitals and other healthcare providers to view and share health information and ideally improve care. Most studies investigating online personal health records have had small sample sizes and short follow-up periods (<12 months). This raises concerns about their external validity and sustainability. One Australian system which features a personal health record, tools to assist with making decisions, organising tasks and a social networking feature has been shown in a community-based trial to promote improved uptake of influenza vaccination among university students.38 We are not aware of any RCTs that have incorporated multiple e-health components as part of a multifaceted, complex intervention for chronic disease management and prevention. Critically, there are no trials involving Aboriginal and Torres Strait Islander peoples, and attempts to integrate consumer strategies with Australian primary healthcare electronic health records are at a very early stage.
Digital technologies and access
Equitable digital access is critical to implementation of the national e-health strategy. Digital access is growing exponentially in Australia. In 2010–2011, 79% of Australian households had access to the Internet in their home and 77% of these used the Internet daily.39 Among Aboriginal and Torres Strait Islander adults, in 2008, 59% had Internet access (up from 41% in 2002).40 Mobile phone use has been dramatically rising and now outstrips computer access. In 2006–2007, 81% of Australian consumers reported owning a mobile phone. Although growth was originally driven by the younger market, the largest annual increase in mobile phone ownership is among people aged 65+ years.41 Data on mobile phone access for Aboriginal and Torres Strait Islander people are unclear; however, in 2008, 67% of non-remote and 61% of remote households had access to a prepaid mobile phone, and 41% and 19% of non-remote and remote households, respectively, had mobile access via a contract.41 ‘Smart phones’, characterised by multimedia and Internet connectivity, are the biggest growth area. In 2010–2011, around 25% (3.9 million people) of Australians accessing the Internet did so via their phone (up 63% on the previous year).42
HealthTracker e-health system
An electronic patient care system called HealthTracker has been previously developed and tested by our research team.43 This e-health system is essentially a clinical decision support system for CVD risk management in primary care. HealthTracker is fully integrated with the primary healthcare electronic health record and provides: (1) point of care decision support related to CVD prevention and management; (2) a graphical patient counselling tool; (3) a computerised audit tool that provides rapid snapshots on health service performance combined with a recall and reminder system and (4) access to a quality improvement web-based portal where health services can view monthly peer-ranked performance and access tools and resources to support quality care. HealthTracker has undergone significant proof of concept testing and validation,43–45 and is currently being implemented in a large-scale cluster RCT (TORPEDO) in Australia.42 The trial is funded by the Australian National Health and Medical Research Council and involves 20 ACCHSs, 40 general practices and over 50 000 patients (Grant ID #1010547, ACTRN12611000478910). However, HealthTracker is a provider-directed strategy and the added value of a consumer or patient-focused interface remains unknown. Therefore, the Consumer Navigation of Electronic Cardiovascular Tools (CONNECT) study aims to enhance the existing HealthTracker system and utilise the growing e-health environment to scientifically test whether a consumer-focused e-health strategy provided to Aboriginal and Torres Strait Islander as well as non-indigenous people at moderate-to-high risk of a CVD event will improve risk factor control when compared with usual healthcare. The study also aims to determine the acceptability, equity and cost-effectiveness of such a strategy. We hypothesise that access to an integrated and patient-centred e-health strategy will improve risk factor control when compared with usual healthcare.
Methods and analysis
Study design
CONNECT is a single blind, RCT involving 2000 regular adult health service attendees at General Practices and ACCHSs with an average follow-up of 18 months (figure 1). Written and informed consent will be obtained from all participants.
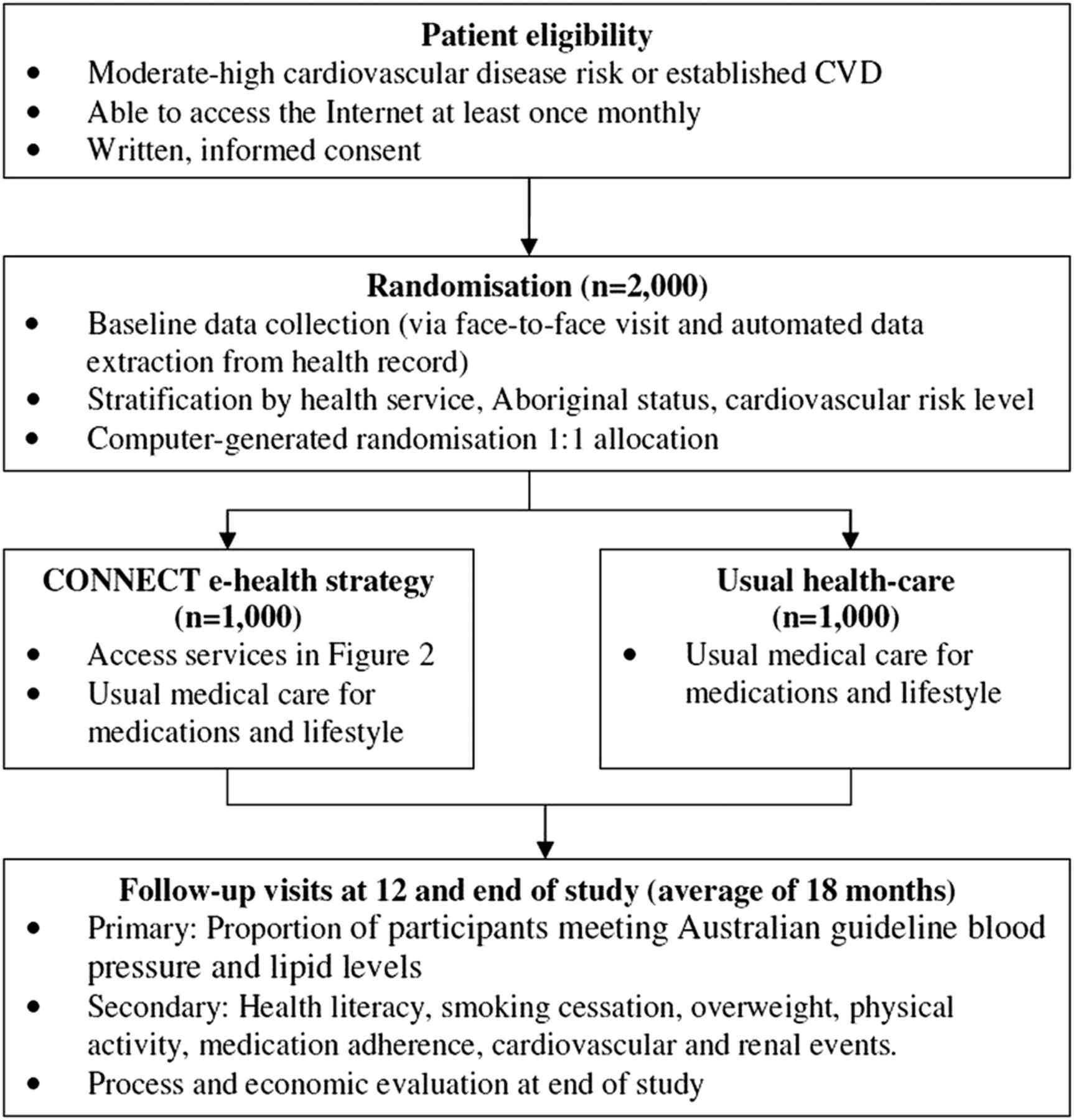
The Consumer Navigation of Electronic Cardiovascular Tools (CONNECT) study schema.
The study will be conducted across approximately 65 Australian General Practices and ACCHSs. Participants with a diagnosis of CVD or who are at high risk of CVD will be randomly allocated to either the control or intervention group. The control group will continue to participate in usual healthcare, supported by HealthTracker; the intervention group will participate in the CONNECT programme which is a consumer-directed e-health strategy for cardiovascular risk management. The programme is electronically integrated with the primary care provider's software and will include access to interactive smart phone and Internet platforms. Control arm participants will not have access to the portal. However, at the end of study, all participants (control and intervention) will be offered portal access for a maximum of 12 months. Participants will be assessed by personnel blinded to treatment allocation at face-to-face appointments at baseline and 12 months and at the end of study.
Randomisation
Eligible consenting participants will be randomly assigned to the e-health strategy or provision of usual care for an average of 18 months (minimum 12 months and maximum 24 months). In both groups, any advice and/or other interventions provided by the general practitioner (GP)/health service will continue at their health provider's discretion. Randomisation will be conducted independently using a central computer-based randomisation service with equal allocation to intervention versus control. A permuted block sequence will be used and will be stratified by level of CVD risk, study centre and Aboriginal and/or Torres Strait Islander status. Study personnel taking follow-up assessments will also be blinded to parallel group assignments.
Participant eligibility
Consenting adult patients (>18 years) with access to the Internet at least once a month via mobile phone, tablet or computer who are at moderate-to-high risk of a CVD event will be included. Potential participants will be excluded if they have a severe intellectual disability or if they have insufficient English knowledge to provide written informed consent. Moderate-to-high CVD risk is defined as any of the following:
-
Five-year CVD risk ≥10% using the Framingham risk equation;
-
A clinically high risk condition (Aboriginal/Torres Strait Islander and age >75 years, diabetes and age >60 years, diabetes and albuminuria, epidermal growth factor receptor <45 mL/min, systolic BP ≥180 mm Hg, diastolic BP ≥110 mm Hg and total cholesterol >7.5 mmol)46;
-
An established CVD diagnosis (ischaemic heart disease, stroke/transient ischaemic attack and peripheral vascular disease).
Recruitment
We will aim to recruit approximately 30 participants from each of a total of 65 general practices and ACCHSs. Eligible patients will be identified by clinic staff using a customised electronic data extraction facility in the practice software system47 which was successfully used in the TORPEDO trial.43 Potential participants will receive an invitation letter from their GP. Eligibility will then be confirmed during a telephone call from a study research assistant. The interested individuals will be invited to a face-to-face registration visit at the practice from which they were identified. At the initial visit, written informed consent will be obtained and the baseline assessment will be completed by a CONNECT research assistant. Practices will be reimbursed a small fee (in line with a standard consultation fee) for the time required to assist with recruitment if the minimum of 25 patients per practice are recruited. All software license costs and technical support associated with the HealthTracker system will be provided free for the duration of the trial.
Intervention
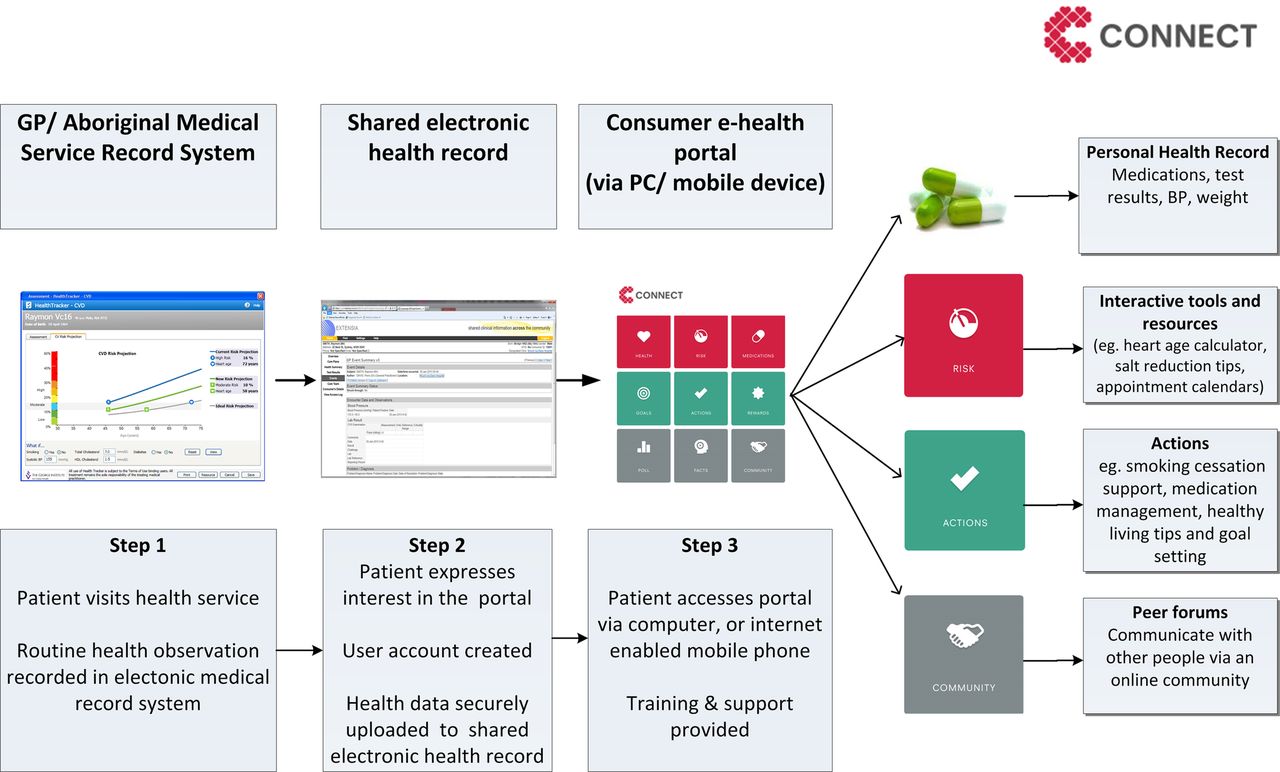
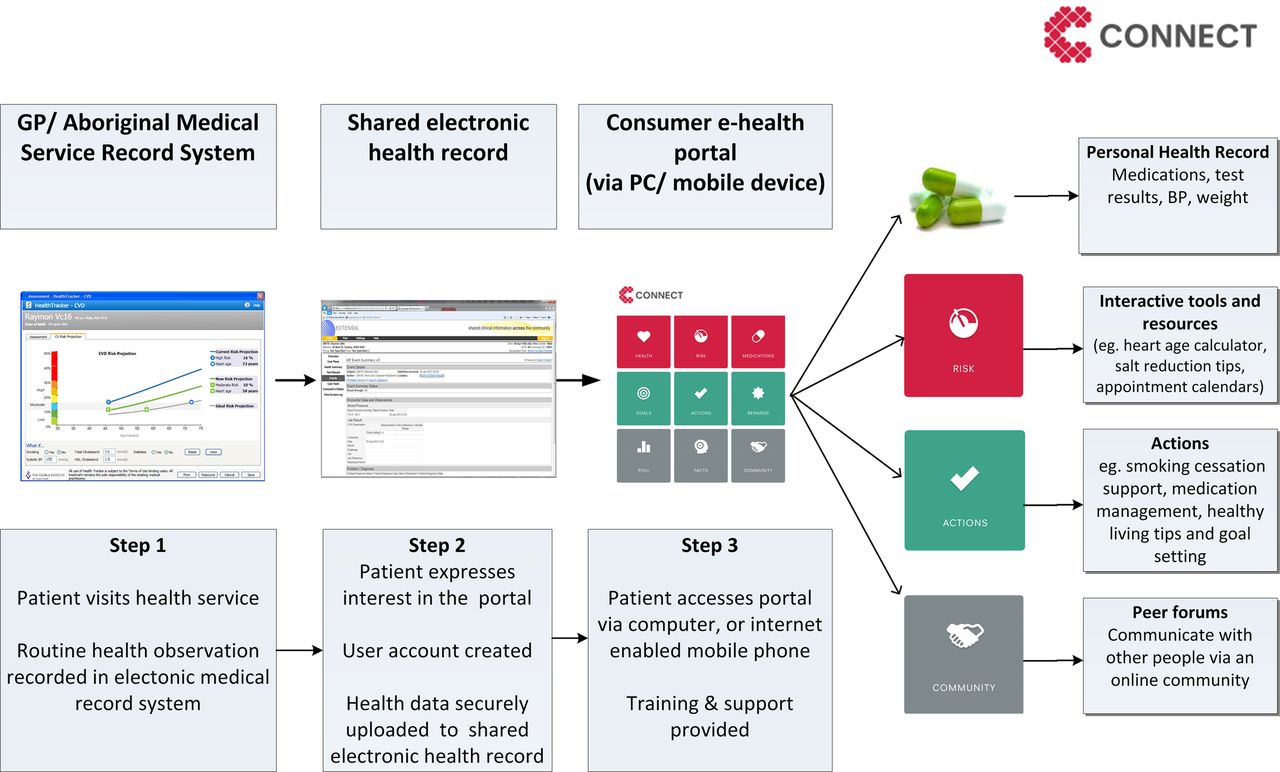
The intervention group will participate in the CONNECT programme, which is a consumer-focused e-health strategy aimed at assisting with the management and prevention of CVD (figure 2). The programme components focus on cardiovascular risk assessment, medication adherence, lifestyle change and seamless patient-provider communication. CONNECT content has been informed by a detailed analysis of factors that drive uptake of Internet-based programmes for CVD secondary prevention.48 HealthTracker assessment data (eg, CVD risk factors and scores, medications and other treatment advice) are uploaded securely to a consumer-focused CVD-specific module built using a e-health record architecture. Patients will then be able to securely register for access to the integrated portal. Throughout the trial, a minimum of one upload from their software to the CONNECT portal will be performed by the GP or an authorised staff member for participants randomised to the intervention. Subsequent uploads to the CONNECT system will be at the discretion of the treating practitioner and will depend on visit frequency and availability of new data (based on changes in patient care and frequency of visits). An alert will be flagged in the application if a new upload has occurred. CONNECT was systematically developed through an iterative process and using user-centred design approach.49 The intervention development process involved collaborative design workshops (including journey mapping and persona building),49 sketching and iterative validation by consumers.
{kind=link}
{kind=link}
The consumer-focused e-health strategy linked to primary healthcare.
The portal will be accessible via the Internet and also via a downloadable application for use on a mobile device. As described in figure 2, participants in the intervention arm will be able to securely access the consumer portal via a secure login process. Patient data will be electronically uploaded from the clinic record to the portal. As part of the intervention, an implementation team of ‘CONNECT coordinators’ will provide face-to-face training to participants on how to use the various features in the portal. Key training features include: (1) viewing personal health record summary including information such as medicines, test results, BP and weight; (2) use of interactive tools and resources (eg, the HealthTracker risk calculator that visually plots CVD risk projections and allows people to perform ‘what if scenarios’ to explore the relative risk reductions (RRRs) from various CVD risk factors); (3) access to simple medication and healthy lifestyle reminders and motivational message prompts depending on their choice and health profile (eg, smokers wanting to quit will be able to receive a series of random messages to assist with cessation) and (4) an interactive goal setting and social media feature where people will be able to set their own goals and receive virtual rewards and also communicate with other users using CONNECT. As part of the intervention, participants will be contacted at months one and two by telephone and additional support will be provided as needed. At any time, assistance will also be available via a helpdesk number or via an online or mobile text help request. A CONNECT coordinator will receive these requests and provide appropriate medical support or arrange technical advice if needed. The CONNECT coordinators will be separate from the recruitment and assessment team so as to maintain blinding of outcome assessments.
Control group
Participants in the intervention and control groups will continue with usual healthcare. Control arm participants will not have access to the portal; however, at the end of study, all participants (control and intervention) will be offered portal access for a maximum of 12 months.
Data collection and study outcomes
Centrally employed CONNECT research assistants (blinded to group allocation) will conduct study visits at baseline, 12 and 24 months and ensure all clinical measures are entered into a purpose-built and secure online database. Clinical and survey data will be collected via face-to-face or phone interviews (if necessary) and entered into a secure central web-based database. During 12-month and 24-month assessments, we will assess the access to CVD management services for both groups such as the frequency of GP and specialist visits (self-report), access to allied health services (eg, dietitian and psychologists) and community groups or activities (eg, local walking group, online smoking cessation programme). In addition, analytic information from the CONNECT portal and smartphone application will be extracted on a monthly basis to determine usage patterns (website and smartphone/tablet application). This study will be monitored and managed centrally with periodic site monitoring visits.
The primary endpoint is the proportion of participants at the end of study whose BP and fasting low-density lipoprotein (LDL) cholesterol are meeting the Australian guideline targets (defined as: ≤130/80 for participants with CVD, diabetes or albuminuria OR ≤140/90 mm Hg for all others participants) and LDL-cholesterol < 2 mmol/L).50 Secondary outcomes include the mean difference from baseline in systolic and diastolic BP and fasting LDL cholesterol levels, proportion meeting BP and LDL targets separately, self-efficacy, health literacy, self-reported point prevalence abstinence in smoking, mean difference from baseline in body mass index and waist circumference, self-reported physical activity and self-reported medication adherence (box 1).
Box 1 Primary and secondary outcomes (measured at baseline, 12 months and end of study)
Primary
Proportion of participants meeting the Australian guideline BP and lipid targets50
-
BP of 140/90 mmHg for all except those with CVD, diabetes or albuminuria for whom the target BP is 130/80 mmHg. BP measurement is conducted via three resting and sitting digital recordings with the mean of the last two readings.
-
LDL of <2.0mmol/L. LDL measurement is via fasting blood sample.
BP is based, on an average, of three resting and sitting digital recordings with the mean of last two readings, and LDL-cholesterol is measured on a fasting blood sample.
Secondary
-
Proportion meeting guideline-recommended BP and LDL-cholesterol targets separately
-
Difference in mean systolic and diastolic BP at the end of study
-
Difference in mean cholesterol levels at the end of study (TC, LDL and HDL)
-
Difference in mean body mass index and waist circumference at the end of study
-
Difference in health literacy scores—HLQ51 and the eHEALS52 at the end of study
-
Cardiovascular and renal events, new onset diabetes—self report and confirmed with medical records
-
Physical activity—WHO Global Physical Activity Questionnaire53
-
Point abstinence in smoking (≤5 cigarettes in the previous 7 days54 or recent smoking according to assessment using carbon monoxide meter)
-
Fruit and vegetable intake, fish, salt and saturated fat intake—self-report portions consumed in 7 days prior and compared with published guidelines recommendations
-
Cardioprotective medication adherence—self-report and verified by medical record and pharmaceutical benefits scheme data
-
All-cause mortality—medical record
-
Hospital readmissions—self-report and verified by medical record
-
Health-related quality of life—EQ5D (version 5L with Australian standardised weights55)
BP, blood pressure; CVD, cardiovascular disease; eHEALS, e-health Literacy Scale; HDL, high-density lipoprotein; HLQ, Health Literacy Questionnaire; LDL, low-density lipoprotein; TC, total cholesterol.
Statistical considerations
For the primary outcome measure, assumptions used in the sample size and power estimates have been determined from TORPEDO data of 10 181 routinely attending patients at moderate-to-high CVD risk. Calculations assume that 25% of people are meeting guideline-recommended BP and LDL targets (as defined above) at baseline with mean systolic BP 136 mm Hg (SD 17.2) and mean LDL cholesterol 2.5 mmol (SD 0.70). A total sample size of 2000 participants, allowing for a 20% loss to follow-up, would have 90% power to detect an absolute improvement of at least 7.5% in the proportion of people meeting recommended targets using two-sided tests, with p values of less than 0.05 judged as significant. For secondary outcomes, this translates to a 2.8 mm Hg absolute difference in systolic BP and a 0.11 mmol/L absolute difference in LDL cholesterol.
Although there is little literature on effect sizes of e-health interventions for CVD risk factors, we have powered the study on effect estimates that could be considered clinically meaningful for a moderate-to-high risk population. Based on previous work on modelling cardiovascular risk factor reductions, the BP and LDL cholesterol effect sizes mentioned above could each translate to around 5–10% RRR or combined RRR of 10–19% in cardiovascular events.56
Primary analyses will be unadjusted, following an intention-to-treat principle, and conducted blind to treatment allocation. If necessary, multivariate analyses will be performed to adjust for any significant differences between each study arm. Prespecified analyses will be conducted on the following subgroups: established CVD versus high-risk non-CVD; Aboriginal versus non-Aboriginal; proportion meeting/not meeting the primary endpoint at baseline; proportion adherent/not adherent to guideline-recommended BP and lipid medicines at baseline. Characteristics will be compared between groups using independent t tests for continuous variables and χ² tests for categorical variables. Mean risk factor levels will be compared between groups in terms of relative risks, 95% CIs and two-sided p values. Mann-Whitney U tests will be used where data are not normally distributed.
Process evaluation
Process evaluations explore the implementation, receipt and setting of an intervention and help in the interpretation of outcome results.57 Our team has extensive experience in such evaluations.44 ,48 ,58 Analyses will be conducted by the Pawson and Tilley59 realistic evaluation model, which seeks to understand human actors’ choices and actions, within the context of the systems in which these players operate. We will use mixed methods to investigate why the e-health strategy may or may not have been effective and which intervention components were most influential. Four data sources will be used: (1) quantitative data on patient measures described above; (2) usage of data extracted directly from the consumer portal; (3) patient and provider surveys of satisfaction, tool utility and health actions taken and (4) semistructured interviews with participants and care providers (including GPs) toward the end of study.
Multivariate subgroup analyses will assess for any differential impact of the intervention on outcome measures by Aboriginal status, postcode, income, education level, language spoken at home, age, gender and internet and mobile phone access. Qualitative data will explore participant views on benefits, disadvantages and acceptability of the portal. Taking an equity perspective, interviews will seek to understand barriers and enablers to uptake by particular subpopulations, including factors such as Internet/smartphone connectivity and geographical remoteness. To obtain a broad range of views, we will use a maximum variation sampling method based on patient demographics and health service characteristics.60 Sampling will continue until no new themes or categories emerge (‘thematic saturation’). We anticipate, based on our previous experience, around 80 interviews will be required. In ACCHSs, Aboriginal participants will be interviewed by Aboriginal researchers. As with previous research collaborations, support and training will be provided for Aboriginal health researchers in the process evaluation, focusing not only on data collection but also on analysis and reporting. Analyses will be thematic and coding will be carried out inductively based on emergent themes. NVivo V.9 will be used to assist with interview data management. Given the focus of CONNECT on consumer engagement with an e-health strategy, assessment of health literacy (including communication with providers and understanding of information provided) will allow greater understanding and explanation of potential clinical outcomes as well as barriers and enablers that engage with the intervention. The process evaluation will provide important narratives on the role of e-health tools in the patient and care provider experience. These standalone research findings will make a novel contribution to translating findings into policy and practice.
Economic evaluation
A cost-effectiveness analysis will be undertaken to compare the e-health strategy with usual care. The economic evaluation will entail two components: a trial-based economic evaluation and a modelled economic evaluation of long-term costs and outcomes. The trial-based economic evaluation will estimate the incremental cost-effectiveness of the e-health strategy in terms of quality-adjusted life years (QALY) as measured over the follow-up period. This will enable an incremental cost per QALY gained to be estimated. The direct costs of the intervention over and above usual care, including training support and software maintenance, will be assessed. Alongside these will be cost offsets, in which the difference between the costs incurred in the utilisation of health services, medications and tests between treatment groups will be assessed. Data for these costs will be drawn from automated extracts of health service records (eg, service utilisation) and from self-reported questionnaires (eg, events, hospitalisations and quality of life). Details on medications, laboratory tests and service utilisation will be costed at prevailing rates. Hospitalisations will be costed using standard Australian National Diagnosis Related Groups (AN-DRG) cost weights.
A modelled economic evaluation will be built onto the trial to enable quality of life and survival to be examined over a longer time frame than the trial follow-up period. Patients in usual care and the e-health strategy would be tracked over this extended period to capture various health states (including death and various cardiovascular events). Transition across these health states will be based on probabilities in relation to long-term treatment effects, safety and disease progression derived from the trial findings and/or literature review. Data on costs and quality of life attached to various health states will also be drawn from literature review and trial data. With appropriate discounting, estimates of long-term costs and outcomes will fold out of the model. Sensitivity analyses will be conducted on variables such as discount rate, uncertainty in outcome estimates and assumptions made in costings. Different pricing scenarios will also be tested to determine threshold values for achieving cost-effectiveness, including cost-effectiveness of different components of the strategy.
Ethics and dissemination
The findings of this study will be disseminated via the usual scientific forums including peer-reviewed publications and presentations at international conferences. The study will be administered by the George Institute for Global Health, with the design and conduct overseen by a Steering Committee. This committee has expertise in large-scale clinical trials and qualitative research, economic analysis, clinical CVD management and healthy policy implementation. This study will adhere to the National Health and Medical Research Council ethical guidelines for human research.
Conclusion
Less than half of all people at highest risk of a CVD event are receiving and adhering to best practice recommendations to lower their risk. In this project, we will examine the role of e-health-assisted consumer strategies as a means of overcoming such health system inefficiencies. With the availability of the PCEHR for all Australians in 2012, consumer-focused e-health is set to become a key component of the health system. Despite the scale of this initiative, uptake has been slow and there is little research on the factors that will support its uptake. Innovative strategies that are practical to implement and support negotiation of care between consumers and care providers are therefore urgently needed.
The CONNECT study will generate rigorously evaluated findings on an issue of national and international importance. The development of a content rich, consumer-focused e-health intervention that is fully integrated with the primary healthcare system will greatly inform the e-health agenda. Equitable access to these emerging technologies is essential, and this study, quantitatively and qualitatively, tests the acceptability and effectiveness of the intervention for Aboriginal and Torres Strait Islander peoples and other socioeconomically disadvantaged groups. The intervention will be compliant with Australian PCEHR specifications, thus allowing for seamless interoperability. This maximises its viability for large-scale implementation across Australia. If found to be successful, the CONNECT e-health strategy could be upscaled and expanded to increase compliance with international e-health strategies. The CONNECT strategy may also have applicability as a standalone strategy where electronic integration with primary care is unavailable.
References
Footnotes
-
Contributors JR and DP conceived the study and intervention, and drafted the protocol. TU, MFH, AR, NH, KP, CC, EH, AP and NZ contributed to the scientific design and protocol development. SJ led the economic analysis aspect of the design. AL, LN, GC and FH contributed to the practical components of the intervention design and delivery. All authors read and approved the final version of the manuscript.
-
Funding This work was supported by the National Health and Medical Research Council (Australia) for (APP1047508). JR is funded by a NHMRC/National Heart Foundation Postdoctoral Fellowship (632933). LN (APP1036763) and DP (APP1054754) are supported by a NHMRC Early Career Fellowships. AP (APP632938) and MH (APP1002600) are supported by an NHMRC Senior Research Fellowship.
-
Competing interests None.
-
Ethics approval University of Sydney Human Research Ethics Committee and the Aboriginal Health and Medical Research Council.
-
Provenance and peer review Not commissioned; peer reviewed for ethical and funding approval prior to submission.