Article Text

Abstract
Objective To explore experiences of social support needs among South Asian Muslim patients with life-limiting illness, living in Scotland, who are parents of young children.
Design Secondary analysis of data from a multiperspective, longitudinal Scottish study involving in-depth semistructured interviews with patients, their nominated carers and healthcare professionals. Data were analysed using interpretive phenomenological analysis.
Setting Edinburgh, Scotland.
Participants South-Asian Muslim patients with life-limiting illness with children under the age of 18 (n=8), their carer (n=6) and their healthcare professional.
Main outcome measures Access and provision of social support in palliative care.
Results Open-ended qualitative interviews identified four main themes: (1) parental sadness over being unable to provide tangible support; (2) parental desire to continue to provide emotional support; (3) limited availability of informal social support networks; and (4) differing perspectives between healthcare professionals and patients on patient access to social support sources, with a subtheme being the capacity of male carers to provide social support.
South-Asian parents at the end of life had limited access to extended-network support. Gender roles appeared as challenging for healthcare providers who at times overestimated the amount of support a female carer could provide and underestimated the amount of support male carers provided. Implications for practice include the need for greater awareness by healthcare providers of the social support needs of ethnic minority and migrant parents with life-limiting illnesses and especially an awareness of the importance of the role of male and female carers. Further research is needed to explore how the timing of migration impacts the need for and availability of tangible and emotional informal social support among ethnic minority parents with life-limiting illness.
- Social support
- Qualitative Research
- Supportive Care
- Palliative Care
- Minority Groups
This is an Open Access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 3.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/3.0/
Statistics from Altmetric.com
Strengths and limitations of the study
-
Results were frequently discussed with members of a multidisciplinary team; a large response rate (96%); a diverse and broad range of participants highlighted that further research is needed on the relationship between timing of migration and access to palliative care services; and the use of multiple perspectives (patients, healthcare providers, carers).
-
Diverse and broad range of residency status and acculturation-related factors led to inconsistencies in themes, missing interviews with three out of the five male spouses of patients.
-
The lead researcher did not collect data, and therefore there was considerable distance from the data. However, in the scope of the secondary analysis, the method allowed the data to be viewed from a different perspective soliciting new themes.
Introduction
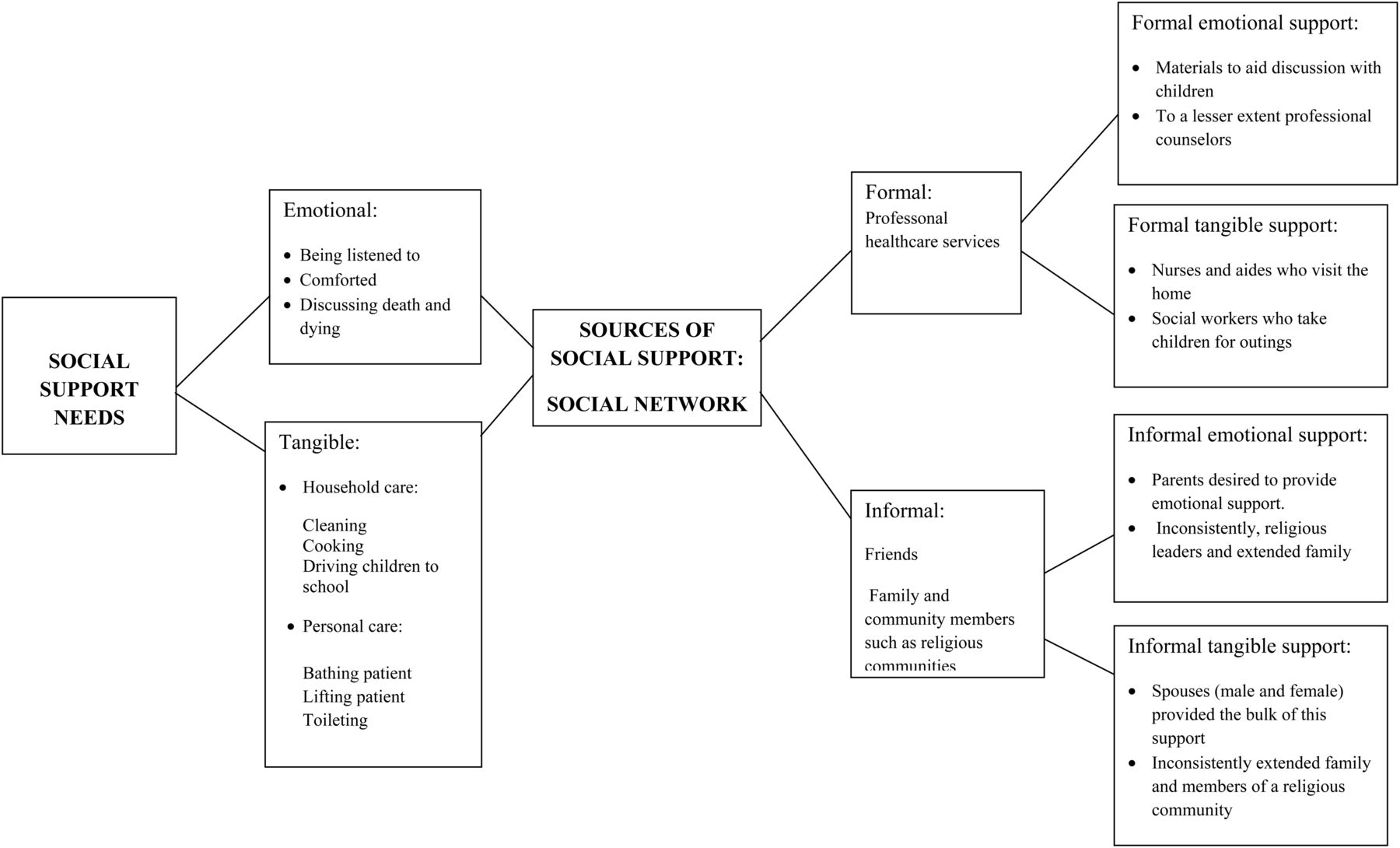
Social support has been found to be associated with an increase in quality of life for patients with life-limiting illness and also for their partners, children and other family members.1–7 Social support consists of addressing tangible needs such as assistance with transportation, home and personal care, as well as emotional support such as being listened to, understood and comforted.5 Tangible and emotional support may be provided through informal and formal social networks. Informal social support is obtained through available family, friends and communities, which may include community and religious networks. Formal social support is obtained through professional service providers such as doctors, nurses and social workers (figure 1).1–4 ,6 ,7
{kind=link}
Definition of social support and examples of application in analysis. Social support was divided into tangible and emotional support. Social support comes from social networks and from either formal or informal providers. Meaning units were selected based on the informant's discussions of formal and informal social support in relation to being a parent.
Having a parent with life-limiting illness or who has died has been linked to stress, anxiety and poor psychological health in children and adolescents.3 ,4 ,8–10 Disability, pain, emotional distress and the need to attend long-term treatment and/or palliative care make it hard for parents to provide the same level of support as before they became ill. Moreover, parents with life-limiting illnesses struggle to maintain normality for their children in helping them with their daily activities such as going to school or for outings.11–18 Social support allows children to engage in important coping processes such as discussing their feelings, developing enjoyable memories with their parents and being able to temporarily take a break from stresses in the home.3 In order to maintain this role, parents often desire the help of formal social support services in order for their children to be able to live as normal daily lives as possible in the context of life-limiting illness.11–18
Concerns have been expressed that ethnic minorities in the UK are less likely to use formal supportive care services than the ethnic majority population.19–23 There has been a debate whether this is due to less need of services, partially due to the healthy migrant effect whereby economic migrants move for work and tend to be healthier and/or younger compared with the ethnic majority population, or due to inequalities in access and acceptability of healthcare.20–23
Factors found to be associated with the lack of uptake of palliative care services among ethnic minorities include socioeconomic status, attitudes towards palliative care, lack of knowledge of available services, mistrust of healthcare providers, lack of referrals and dissatisfaction with healthcare providers.7 ,22 Referrals or lack thereof may be associated with healthcare providers’ perceptions that ethnic minority patients have large networks of extended family members to rely on for support, a stereotype that has now been largely refuted in the literature.24–27
Public health policies in the UK during the 1990s, particularly those directed at South Asian communities, focused on the development of social support services stemming from the community. Many of these policies failed to reflect shifting patterns and laws regarding migration, changing household structures towards a nuclear family structure and women's changing role in the workplace. More recent research has shown that ethnic minorities and migrants in particular have a more fragile social support system than was previously thought and that, even for those with large extended social networks, these networks may not provide adequate social support.5 ,25–29
The majority of existing studies on South Asian experiences of palliative care in the UK focus on the experience of care for elderly patients or care of ill children.30 There is, however, little previous work investigating the social support needs of South Asian parents living in the UK who are severely ill and have young children who may face complex challenges in coping with the physical, mental and social consequences of life-limiting illness and at the same time provide care to their young children. More insight into the experience of reconciling parenthood with life-limiting illness is needed since this will enable the identification of ways to provide support and specifically to meet parents' desire for social support services which allow them to maintain their roles as parents. Moreover, children who have a parent with life-limiting illness require social support in order to engage in important coping processes, such as going on outings and maintaining normalcy in their lives. We therefore sought to explore the experiences of social support among South Asian Muslim patients with life-limiting illness in Scotland who are parents to young children.
Methodology
This study is a secondary analysis of qualitative data constructed as part of a large multiperspective, longitudinal study aimed at understanding the experiences of South Asian Sikh and Muslim patients at the end of life (titled ‘Developing services to meet the end-of-life care needs of South Asian Sikh and Muslim patients and their families in Scotland’). A secondary analysis was conducted in order to explore in depth the social support needs of a subset of Muslim patients who were parents with young children. We present here a brief summary of the methodology since a more detailed description of the recruitment process, data generation and ethical considerations has been presented elsewhere.31
In the original study, purposive sampling was used and patients were approached through healthcare and social care professionals, religious leaders, community leaders and personal contacts. Patients were selected on the basis that they were given a diagnosis of cancer or another life-limiting illness and that they had a prognosis of living less than 1 year. Once patients were contacted and expressed interest to take part in the study, they were asked to nominate and give consent to contact their primary carer and healthcare provider. Maximum variation sampling was used to recruit a diverse range of informants with varying socioeconomic status, gender, age, malignant and non-malignant life-limiting illnesses, educational background and country of birth.31
In-depth semistructured interviews were conducted with a total of 25 patients and their nominated carers and healthcare professionals, yielding a total of 92 interviews.31 Interviews with patients and carers were conducted by a trilingual researcher in Punjabi, English and/or Urdu. The interviews were then transcribed and translated by the trilingual researcher and a trilingual secretary. Healthcare professional interviews were performed by either the trilingual researcher or another member of the research team. Up to three interviews were conducted with patients and when necessary, bereavement interviews with carers were conducted at 8–12 weeks after the patient's death. Interviews were conducted in stages; stage 1 was the initial interview, stage 2 took place approximately 8 weeks after the initial interview and stage 3 took place 18 weeks after the initial interview. Data were collected in 2004. Interviews were undertaken until saturation was reached
Secondary data analysis
In this secondary analysis, only interviews of Muslim patients with children under the age of 18 (n=8) were analysed. A total of 36 interviews were analysed that is, from eight patients, their carers (n=6) and healthcare professionals (n=9; table 1). For one patient, two healthcare providers were included in the study. Only interviews of patients with children under the age of 18 were analysed. We decided to include only Muslim patients in this secondary analysis because there was only one Sikh participant with a child under the age of 18 and this child was not residing in the UK.
Participant characteristics
The topics discussed in the interviews relating to being a parent at the end of life varied between patients, carers and healthcare providers. Specifically, discussions with patients included their perceived needs for palliative care services, their experiences of formal care services, the impact of the illness and their relationship with healthcare providers and decision-making within the family. Relevant topics discussed with the primary carer included the impact of the patient's illness on the family, the carer's needs, the history of the illness from the carer's perspective and the patient's preferences for social support from the carer's perspective. Topics discussed with the nominated healthcare provider included their perspective on the social support needs of the patients and their family and what the healthcare provider provided in contrast to others.31
Data were analysed using interpretative phenomenological analysis (IPA) as described by Griffin and May32 as well as an analysis of multiperspective interviews as described by Kendall et al.33 According to Griffin and May,32 IPA draws on the philosophy that experience is formed based on the perceptions of the participants of the world around them through daily tasks, their perceived geographical or societal location and their interaction with those around them. In addition, in order to operationalise the meaning of social support, this analysis draws on surrounding the meaning of care and the perception of who is available to care as a defining element of understanding experience. Multiple-perspective interviews were conducted across time to contextualise the social support experiences of patients, and to contrast varying perceptions of the patient, carer and healthcare provider. According to Kendall et al,33 in the presentation of results citations can be integrated and/or compared in order to explore the aim. In this secondary analysis, multiple perspectives were integrated to explore commonly expressed needs of social support and compared to explore different perspectives of need between patients, carers and healthcare providers.
IPA is a method that lends itself well to analysing the lived experience of social support. This is because with IPA the researcher takes what an informant sees as a daily experience, such as homecare or driving children to school, and places them into a larger theoretical framework.32 IPA allows the researcher to explore the different perceptions of how the participants relate to their life-world and how they experience social support. This method is important since much of the current literature on palliative care experiences of ethnic minorities refers to the lack of referral by healthcare professionals and the prevailing assumption that ethnic minorities have available large social support networks.
As described by Griffen and May,32 the analysis was conducted in four steps. First, a close reading of the selected interviews was performed and initial thoughts were recorded. For this stage, Open Code software34 was utilised in order to record initial codes and select meaning units. In identifying meaning units, the definition of social support was divided into emotional and tangible support as well as awareness of the source of the support, formal or informal (see figure 1). The next step was the interpretative phase where more abstract ideas are generated about the lived experiences of social support. Finally, themes were identified and grouped into clusters under superordinate themes. Negative data or disconfirming cases were continuously sought.
Ethical approval
Care was taken in order to ensure that participants understood the study and could give informed consent. Special consideration was taken in gaining consent from participants who were illiterate in any language. In reporting the data, participants’ identities were disguised in order to maintain confidentiality. Researchers were sensitive in their discussions of death and dying, especially if the participants were unaware of their prognosis or diagnosis.
Results
Four themes were developed in relation to experiences of social support needs among South Asian Muslim parents with life-limiting illness. These are described below together with supporting illustrative data.
Sadness over being unable to provide tangible support: I cannot do anything for my children
In general, patients expressed sadness over no longer being able to provide tangible support and perceived this as a loss of an important part of their parenting role. As one patient described when asked about the overall experience of having a life-limiting illness,
R: What is the most difficult thing for you?
P: I cannot do anything for my children…[crying].
(Patient 1, Male, Stage 1 interview)
Often, the experience of multiple losses caused by life-limiting illness was expressed in the context of family life, which for these South Asian patients it was important to maintain actively. Patients struggled to uphold their responsibilities within the immediate and extended family. They particularly grieved at being unable to provide social support for their children.
The most important expressed need for tangible support was transportation. Patients and their carers frequently discussed the importance of availability of transportation, particularly in relation to picking up and dropping off children from school, taking outings and attending doctor's appointments,
Sometimes [I] had to make [my] son take a day off school when I needed to go and see him [patient] in the hospital. Even now, when I take him [patient] to see the doctor, my son will need a half day off school.
(Carer, Patient 2, Female, Stage 1 interview)
Patients described children's desire to go on outings with their parents. However, ill parents and some carers, particularly female carers, were often unable to drive. Patients reported a longing to be able to take outings with their children, which they perceived to be important elements of a happy, carefree childhood,
My eldest son did say to me once those other children's mums take them out and I would like to do that [crying]. Hence I started to drive to the shopping centre and sit in the car. I couldn't go in because I was feeling so tired…
(Patient 25, Female, Stage 1 interview)
The need for transportation was most acute when participants had arrived recently in Scotland and did not have resources such as cars, driving licenses or a support network to help in picking up and dropping off children from school or engaging in enjoyable activities.
Desire to provide emotional support: by God's grace I still have that power
Patients desired to provide emotional support for their children, very often because they could only provide limited tangible support. In one parent's words,
See if I had, I don't know how to put it so it sounds politically right, if I had suffered any mental problems, then it would be different. Because I would not be able to keep my family together, whereas, through God's grace, I have still got the power. I have still got that ability to step in and help my children when they have a problem. Or if we have a problem, to sit and talk like an ordinary family. Only thing is that I can't do anything for them.
(Patient 4, Female, Stage 3 interview)
The same patient added that at one point in time her daughter was offered an opportunity to join a support group for young persons with parents who suffered from life-limiting illness. The daughter refused this offer. The patient explained that she respected her daughter's decisions, stating she wanted her daughter to experience as much normalcy as possible,
Yes, at one point, they did offer support for my children, joining a group or something like that. And my daughter said no, ‘I don't want it’. And I said, well, I don't want them to feel any different, I just want them to grow up. Have, as much as possible, a normal up-bringing. The choice was given to her and she refused, so that's fine.
(Patient 4, Female, Stage 1 interview)
Some parents were happy to receive tangible and emotional support services, though there were cultural differences which sometimes prevented full access to these services. For example, in regard to emotional support services for patient 5, the healthcare provider reported that children, despite parents’ interest, had never attended the offered group therapy session due to a scheduling conflict. This conflict was due to the children needing to attend the mosque at the same time as the group therapy session. Children's participation in religious activities was perceived by many patients as important both for their children's upbringing and for their present and future emotional well-being. Culture—and more specifically religious—aspects shaped experiences and priorities among patients as exemplified by the emphasis bestowed on religious learning for their children. However, the patient and carer were happy to receive materials such as a children's book to discuss with their children,
I first met them and told them a bit about the leaflets and the resources that are around for children to help adults talk to children about cancer […] they were quite happy with it in English…em there's a book I did give to them which was one was called Mummy's ill…and kind of explains about cancer and what that is and what chemotherapy is and what is radiotherapy, all that sort of things.
(Healthcare Provider, Patient 5, Stage 1 interview)
Another form of emotional support parents wanted to provide was through teaching their children religious practice since this was considered an important part of parenting. One patient hoped that teaching her daughter religious practice would give her daughter emotional support both now and in the future,
The other thing that worries me is that she is 13, she does not know namaz [daily prayer] yet, she is still reading the Qur'an. I was saying to her we really need to get on top of that because that is a big obligation as a parent…I say to her that that is really important because I feel that, you know, sometimes you will get comfort from that as well.
(Patient 3, Female, Stage 3 interview)
Parents referred to religion in terms of their own emotional coping, performing an important duty as a parent and also providing emotional support for their children. However, they did not describe themselves as relying on or gaining tangible social support from religious networks.
Patchy informal social support networks: we tried to get my sister over…
The responsibility for tangible support fell largely onto the primary carer, most often the spouse of the patient. One of the carers described taking on the majority of her husband's care, which was even more strenuous because she had a young child,
I did it myself, I still do now…Enough, what else can I do, he needs care. I used to go out to work and I had to leave that about 6 months ago. It was difficult having a young child too.
(Carer, Patient 2, Female, Stage 1 interview)
Extended family, when available, frequently provided support by taking children for overnight visits or watched children while parents were attending doctor's visits or were admitted to hospital. One patient, in the only family where the husband and wife were both born in Scotland, described the role played by extended family,
Sometimes we would need to stay in overnight, and my mum would come up with my brother and take the two of them away. Sometimes her mum and dad would come and take them. So the least you have to worry about…
(Patient 13, Male, Stage 3 interview)
However, the availability of extended family members varied and participants cited that family members had their own families to care for.
In some families, extended family members lived in other cities or countries and grandparents often had their own life-limiting illnesses. Some families applied for visas for their family members to come from abroad and help with daily life, as one carer explained,
We tried to get my sister over from (country) for about six months. She could come and help with the child by picking him up from school.
(Carer, Patient 2, Female, Stage 1 interview)
Visas for healthy family members to come and help with social support needs of those who were ill were sometimes denied, even though healthcare professionals wrote visa support letters.
Insecurity and differing perspectives on social support sources: I've got to leave one healthy parent behind
Patients who received formal support services were quite pleased with the services they received. However, some healthcare providers mentioned that they were sometimes unable to gauge the amount of informal social support patients were receiving from family and community networks which would inform the amount of formal social support services needed. As one healthcare provider mentioned,
R: Is there anything else that you want to say that I haven't asked you about?
P: Em, how much support do people get from Mosque, I mean is it like here? They have to belong to a Church and then the Church rallies round or is it different with the Mosque?
(Healthcare Provider, Patient 1, Stage 1 interview)
The same healthcare provider, in response to a question regarding how to increase social support services for South Asians in Scotland, referred to a breakdown in communication,
I was in Glasgow on Friday and was told there's a man, Muslim man whose looking after his mum single-handedly and washing her, bathing her and you know it's really not the kind of thing you'd expect from a man to do for a female, either he's not getting the support or what he's getting not just good enough for his mother, you know there are issues there, there's a breakdown somewhere.
(Healthcare Provider, Patient 1, Stage 1 interview)
Other patients referred to on-going discussions with their healthcare provider regarding family availability to provide care when requesting access as to services. One patient described an ongoing conflict between herself, the carer and healthcare providers regarding who in her family was available to provide support,
But they [formal social support provider] keep telling me ‘you have family.’ And I say, ‘yes, what do you want me to do? Kill them before their time?’ I'm on my way out; I've got to leave one healthy parent behind.
(Patient 4, Female, Stage 1 interview)
The nominated healthcare provider explained how resource constraints influenced the agency's policy towards provision of support, making it more likely that they would ask family members to provide care,
…our department, Community Care, has changed from the early days—‘we treat this person as an individual, we don't rely on the family’ and all the rest of it—to the complete opposite. If there's family there, they are expected to help because resources are so tight. So initially it was ‘couldn't the children be involved.’
(Healthcare Provider, Patient 4, Stage 1 interview)
In contrast to the above statement made by a healthcare provider, parents felt very strongly against their children being relied on to provide care.
It is important to note that several healthcare providers mentioned resource constraints in regard to providing culturally sensitive services including translated leaflets and providing a choice of homecare attendants. For example, the carer of patient 5 states, while he was open to services such as homecare and a social worker to take the children for outings, cultural differences, such as the homecare worker refusing to take off her shoes inside the home, made care unacceptable,
A worker comes in she hoovers the place washes the dishes irons things like this, I asked her to take her shoes off and put some slippers on that we had, she didn't say a word, had some tea and went off after doing her work…she went back and complained they told me to take the shoes off this that and the other. I got rude phone call from her boss. “Excuse me, did you tell her to take her shoes off”?
(Carer, Male, Patient 5, Stage 1 interview)
When the carer requested another homecare attendant, he was told there were a limited number of attendants available. Hence, this interview suggests that at times it was difficult for patients to receive culturally sensitive formal social support services.
In summary, patients were open to receiving formal from social support services; however, cultural differences and constrained resources prevented patients and their family members from fully accessing social support services.
Differing perceptions of social support and the role of gender
In discussing the amount of available informal social support, healthcare providers often referred to the gender of the carer, which by some were perceived to be shaped largely by cultural factors. Specifically, some healthcare providers assumed female family members were more involved in providing social support for the patient and the children in the family compared with male family members. Healthcare providers at times referred to their previous experience with South Asian Muslim patients in palliative care settings in the UK, and a few also described that their perspectives stemmed from experiences working in Muslim countries,
It has been my experience with the few other Muslim women I have dealt with as well – they have come on their own without their husbands or their partners have seemed to be very much in the background. Muslim women seem to have a more distant relationship with their husbands…White couples do seem to come as equals – may well be that they are estranged equals – but they are there as equals, it seems that South Asian women are much more submissive. They are more clearly different. Husbands often seem so much more traditional.
(Healthcare Provider, Patient 3, Stage 2 interview)
In some cases, healthcare providers had difficulties in assessing the roles of family members in providing care to the patient. Culturally shaped gender roles and the importance of maintaining care within the context of the family emerged in several cases. In one case, the healthcare provider described her perception that the patient's adolescent daughter had taken a major role in providing care and a family preference that social support came from within the family,
I think (daughter) had helped her mum so much in the earlier stages – helping her managing her menstruation, showering, and everything was so…it's such a lot.
(Healthcare Provider, Patient 4, Stage 1 interview)
However, interviews with the patient showed that she did not think her daughter should take on such responsibilities,
My daughter was only 12 and I was told you've got family. I said for God's sake, my daughter is only 12. What you want me to do tell her to drop out of school and stay with me all the time?
(Patient 4, Female, Stage 2 interview)
One of the largest sources of missing data in this study was from the perspective of male carers. From the perspectives of the patients and those male carers interviewed, it was often mentioned that male carers faced additional stress in regard to maintaining work. However, reportedly few male carers were offered social support services; only one carer (for Patient 4) had attended a support group for carers.
In one family where the male parent was ill, the healthcare provider expressed concern over what she perceived to be his lack of involvement with his children. The patient, however, described how it was very important for him to spend time with his children before he died,
The children love me a lot. I love them a lot too…At night we turn the TV off in the drawing room and they come into my room, (wife) goes upstairs the children are with me and we sit and watch TV together for as long as I will allow them…How involved they are with me, people just can't see, I mean when (wife) goes away for a few hours, they're with me and…But if someone comes, I get busy so how can they tell how involved my children are?
(Patient 1, Male, Stage 2 interview)
In summary, some healthcare providers in this study had assumptions that male carers were less likely to provide support than female carers as a result of traditional gender roles and that male patients were distant from their children. Also, some providers assumed that female children were carers, which the families did not agree with.
Discussion
Parents expressed sadness over being unable to provide tangible support which was perceived to be necessary for their children having a good childhood, despite a parent having a life-limiting illness. Parents with a life-limiting illness also perceived that giving their children emotional support was a way for them to maintain their role as a parent. These two themes correspond with previous studies of parenting and children's experiences when a parent has a serious illness in other countries, settings and populations.11–18 In maintaining their roles as parents and providing emotional support, parents were not as interested in formal support groups for their children as they were in information aiding them to speak themselves to their children about their illness. This is similar to the findings from the study by Turner et al14 which found that parents with advanced cancer desired information and resources regarding how they could speak with their children about cancer because they desired to provide emotional support. However, our study also identified social support themes unique to ethnic minorities who had migrated recently, including concerns regarding visa problems for family members to provide care, and geographically distant family members.
Patients and their families were often open to receiving formal tangible support services and sometimes formal emotional support services. However, there were gaps in cultural understanding between healthcare providers and beneficiaries, such as the lack of understanding of children not being able to attend therapy at times of religious services. Some healthcare providers in this study seemed to have preconceived ideas regarding gender roles within Muslim families and availability of social support, thus overestimating the amount of social support women could provide and underestimating the role of men in the family. Whereas healthcare providers highlighted cultural differences in gender roles and in the importance attached to maintaining care within immediate and extended families, patients often expressed unmet needs for formal social support to supplement the support given within family settings. The actual and potential roles of male carers were difficult to assess in cross-cultural encounters between families and healthcare providers. In addition, some healthcare providers overestimated the amount of social support female children provided or could provide. As previous studies have found, parents wanted to maintain normalcy for their children,11–18 and parents in this study explicitly did not want their children to take on the bulk of their care.
In a similar study conducted in England, Katbamna29 points out that the most vulnerable group to have their support needs neglected is that of young female carers living in nuclear families because healthcare providers and family members may not acknowledge their need for support. A study by Llacer et al35 found that recent arrival may limit the ability of female migrants to develop social support networks and achieve important skills such as language or driving. This study had similar findings; for example, transportation needs were consistently highlighted but were the most limited in families where the female carer had arrived recently in the UK.
Also consistent with the study presented here, another study found that male carers felt that healthcare professionals did not acknowledge their concerns or assumed they were not part of care.25 In this study, male carers often struggled to be both the primary carer and provider for their family. Some male carers greatly reduced their hours at work or took on the role of a full-time carer. However, in our study, only one male carer mentioned being offered formal emotional support services.
It was evident that the availability of informal social support networks was inconsistent, meaning that friends and family members were not consistently available, either time-wise or geographically, to provide support. This was also found in a study conducted by Kristiansen et al5 where social networks of migrants were perceived to be geographically dispersed and thus unavailable in the context of life-limiting illness. Some participants in our study expressed a desire to bring family members from another country to aid with daily life or provide emotional support. Given that informal support networks were inconsistently available, the majority of the social support for the patient fell mostly on the spouse or primary carer.
The ability to provide culturally competent care has become a common requirement for palliative care providers due to increased ethnic diversity in many European countries.36–38 However, providers may at times have a lack of insight into how culture shapes understandings of and responses to death and dying, and how to assess psychosocial needs among different ethnic minority groups.36–39 Moreover, healthcare providers may be in fear of being insulting or insensitive.36 ,37 Overall, it has been found that healthcare providers providing palliative care services often do not have the necessary training to provide culturally competent care for patients or understand the complex relationship between culture and health.36–39
Patients and healthcare providers had differing understandings of the amount of social support provided by family members. For example, it has been observed that healthcare providers often assume that South Asian Muslim families would prefer to ‘look after their own’, whereas when British Muslims where questioned, they felt that the family structure was changing.36 In addition, healthcare providers in our study expressed curiosity regarding the amount of support patients received from religious communities and/or religious leaders. Yet, among the patients, religious community members and/or leaders were not perceived to be sources of social support. As reported in the original study for which these data were gathered, some participants actually withdrew from their religious communities due to perceived stigmatisation.31 While religious beliefs have been reported to serve as an important coping mechanism for South Asian Muslims with life-limiting illness,31 religious leaders, imams, were not described as a consistent source of social support for parents of young children.
Methodological considerations
This analysis is a secondary analysis; while respectability of a secondary analysis of qualitative data is growing,40 it is not without its limitations. In this secondary analysis, the first author did not conduct the interviews and therefore had limited opportunity to gain a sense of the context of participants’ lives. Moreover, the lead researcher is not of the same ethnic background or resides in Scotland. Thus, a large amount of reflexivity in the analysis was required as well as discussion with coauthors who performed the interviews. There are, however, benefits to having an outsider perspective. In IPA, preunderstanding must be bracketed or put aside in order to allow the text to speak for itself.32 The researcher came to this study with limited preunderstanding and therefore was able to perform the analysis solely on the text first and then later oscillating between theories of social support, previous research and the data. While there are limitations to a secondary analysis, there are also strengths. A secondary analysis allows researchers to view the data through different perspectives and allowed the researcher to focus on themes related to social support.
Participants were identified through health and social care workers, community leaders and personal contacts. These sources, in themselves, are forms of formal social support networks. Hence, some of the most vulnerable or isolated persons are most likely not included in this study. The use of multiple perspectives strengthened the understanding of the individual experience of the patient as well as exploring different perspectives of the patients, the carers (informal social support) and healthcare providers (formal social support).
Study implications
The reasons for and timing of migration may influence the availability of social support.35 Themes such as inconsistent informal social support networks or transportation difficulty were often due to timing of migration as migration often leads to dispersed social networks expanding across national borders. In this study, some participants had been born and raised in Scotland and others had arrived in Scotland within 1–12 years of the study date. Therefore, while the majority of support fell on the spouse as the primary carer, patients had varying amounts of extended family available to provide support. The ability to uphold important aspects of the parenting role is furthermore clearly dependent on the type of illness, its severity and the types of treatments and/or palliative care that patients are offered.41 Further research is needed in order to understand the influence of these factors on the support needs among ethnic minority parents at the end of life. Studies exploring the experiences of children in families affected by life-limiting illness are needed in order to identify the future support needs of children prior to the death of the parent.
Culture is dynamic and changing and migration often accelerates dynamic changes to culture.36 While all patients were of South Asian origin, it is important to acknowledge the diversity within the category of ‘South Asia’, which encompasses a very diverse group of patients and families with varying resources and vulnerabilities.41 Within the patients interviewed, there were patients who had migrated recently and patients who were born and raised in the UK, carers who had migrated to the UK and one carer who was white Scottish. Moreover, participants in the study were from various regions of India and Pakistan. Recognising how this diversity shapes the experiences of support needs in individual patients is important in order to avoid drawing broad generalisations. In addition, some of our findings underscore the commonalities in psychosocial needs at the end of life across different ethnic groups. For example, and as previously discussed, studies have found that parents with life-limiting illness in general desire to provide tangible and emotional support for their children to maintain normalcy for as long as possible. In our study, culture, migration, gender and socioeconomic position were factors that shaped the expression of this desire to maintain parental support roles despite disabling illness, but the importance of holding on to normality and the experience of need for support in doing so are most likely not confined to ethnic minority groups. To further understand how needs for social support are shaped by cultural factors, including expectations tied to gender roles, the role of ethnic minority status and the changes occurring with time spent in the postmigration environment, comparisons between longitudinal studies conducted among different ethnic groups are needed.41 ,42 Having this insight would help in understanding how to adjust care to meet the specific needs among groups at risk of being inadequately supported in palliative care.
Conclusions
South Asian Muslim parents of young children with life-limiting illness experienced informal and formal social support needs in maintaining their role as a parent. Implications for practice include the need for greater awareness by healthcare providers of tangible and emotional social support needs of ethnic minority and migrant parents with life-limiting illnesses. Healthcare providers and other professionals involved in delivery of palliative and supportive care for ethnic diverse populations should more systematically assess support needs and available informal and formal sources of support that may help families inflicted with life-limiting illness. Support for carers is important and should encompass male and female carers. Formal social support services should aim at helping parents to provide services such as transportation for their children and how to talk to children about their illness and death. Finally, future research is needed in order to understand the influence of the timing of migration on the need for and access to social support services among parents with life-limiting illness representing diverse ethnic groups.
Acknowledgments
The authors would like to thank the participants, their family members and the professionals who participated in the study, and the many people who helped with recruitment. Furthermore, they would like to thank Duncan Brown, Elizabeth Grant, Julia Lawton, Raj Bhopal, Scott Murray, Marilyn Kendall, James Adam and Rafik Gardee. They are most grateful to Shahida Shah for secretarial support.
References
Footnotes
-
Contributors AS conceived the study and all grant holders developed the design. TI and AW collected the data. The secondary analysis of the data was conducted by EMG, with support from all authors. This paper was drafted by EMG, and revised and edited by all the authors. EMG and AS were the guarantors.
-
Funding Funding was provided by Chief Scientist Office, Scottish Government Health Department (grant number CZH/4/242). Publication fees were provided by Danish Research Centre for Migration Ethnicity and Health.
-
Competing interests AS is supported by the Commonwealth Fund, a private independent foundation based in New York City. The views presented here are those of the author and not necessarily those of The Commonwealth Fund, its directors, officers, or staff.
-
Ethics approval This study received ethical approval from the Lothian Research Ethics Committee (Scotland).
-
Provenance and peer review Not commissioned; externally peer reviewed.
-
Data sharing statement No additional data are available.