Article Text

Abstract
Objective To compare mortality in chronic kidney disease (CKD) stages 4 and 5 (estimated glomerular filtration rate <30 mL/min/1.73 m2), peritoneal dialysis, haemodialysis and transplanted patients.
Design Population-based cohort study.
Setting Swedish national healthcare system.
Participants Swedish adult patients with CKD stages 4 and 5 (n=3040; mean age 66 years), peritoneal dialysis (n=725; 60 years), haemodialysis (n=1791; 62 years) and renal transplantation (n=606; 48 years) were identified in Stockholm County clinical quality registers for renal disease between 1999 and 2010. Five general population controls were matched to each patient by age, sex and index year.
Exposure CKD status (stage 4 or 5/peritoneal dialysis/haemodialysis/transplanted).
Primary outcome All-cause mortality was ascertained from the Swedish Causes of Death Register. Mortality HRs were estimated using Cox regression conditioned on age, sex, diabetes status, education level and index year.
Results During 6553 person-years, 766 patients with CKD stages 4 and 5 died (deaths/100 person-years 12, 95% CI 11 to 13) compared with 186 deaths during 1113 person-years in peritoneal dialysis (17, 95% CI 15 to 19), 924 deaths during 3680 person-years in haemodialysis (25, 95% CI 23 to 27) and 53 deaths during 2935 person-years in transplanted patients (1.8, 95% CI 1.4 to 2.4). Against matched general population controls, the mortality HR was 3.6 (95% CI 3.2 to 4.0) for CKD, 5.6 (95% CI 3.5 to 8.9) for transplanted patients, 9.2 (95% CI 6.6 to 12.7) for peritoneal dialysis and 12.6 (95% CI 10.8 to 14.6) for haemodialysis. In direct comparison versus CKD, the mortality HR was 1.7 (95% CI 1.4 to 2.1) for peritoneal dialysis, 2.6 (95% CI 2.3 to 2.9) for haemodialysis and 0.5 (95% CI 0.3 to 0.7) for transplanted patients.
Conclusions We did not find support for mortality in CKD to be similar to dialysis mortality. The patients with CKD stages 4 and 5 had considerably lower mortality risk than dialysis patients, and considerably higher risk than transplanted patients and matched general population controls.
- chronic kidney disease
- mortality
- renal replacement therapy
- transplantation
This is an Open Access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 3.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/3.0/
Statistics from Altmetric.com
Strengths and limitations of this study
-
This study was population based with no restrictions regarding age or comorbidities, and the data were collected from routine clinical care centres to which there is universal access in Sweden.
-
Using the unique personal identity number of each Swedish resident, follow-up was complete regarding mortality.
-
Although all renal replacement therapy patients in the catchment area were included, an unknown number of patients with chronic kidney disease stages 4 and 5 were missed, as the condition is underdiagnosed.
-
Direct comparison of mortality across different health states is complicated by channelling issues, as patients in renal replacement therapy are required to have survived the chronic kidney disease health state.
Introduction
Mortality is substantially elevated in patients with chronic kidney disease (CKD) and dialysis,1–3 with some studies describing patients with CKD in stages 4 and 5 (estimated glomerular filtration rate (eGFR) 15–29 and <15 mL/min/1.73 m2, respectively) as having mortality rates approaching the rates in dialysis.1 However, there are no studies directly quantifying the relative mortality in CKD, dialysis (separating peritoneal and haemodialysis) and transplanted patients.
An analysis of an insured US population found patients in CKD stages 4 and 5 to approach dialysis mortality rates with a threefold and sixfold higher mortality risk, respectively, than patients with eGFR ≥60.1 This can be compared with a standardised mortality ratio of 8 reported in Swedish incident patients with CKD stages 4 and 5 followed for up to almost 7 years,2 and with HRs ranging from 3.7 to 7.0 for stage 4 patients (eGFR 15–29) with varying levels of albumin-to-creatinine ratio in a meta-analysis of more than 100 000 patients, using patients with an eGFR of 90–104 as reference.4
Regarding dialysis mortality, a large European study showed an eightfold higher age-standardised mortality due to cardiovascular and non-cardiovascular death compared with the general population.3 The study did not distinguish between peritoneal dialysis and haemodialysis.
These US and European studies indicate that mortality in CKD stages 4 and 5 may be as high as in dialysis. However, control groups differed between the studies (patients with normal kidney function defined as eGFR ≥601 or 90–1044; aggregated Swedish2 or European life tables3), and mortality may differ between modes of dialysis.5
The aim of this population-based cohort study was to examine mortality in CKD stages 4 and 5, peritoneal dialysis, haemodialysis and transplanted patients in relation to matched general population controls, and directly with each other.
Methods
This population-based cohort study was performed in the Swedish healthcare system using patients’ data from clinical quality registers kept for quality of care evaluation in Stockholm County. These data sources were combined with matched general population controls, and enriched with outcome and exposure data via linkage to nationwide health registers kept by the National Board of Health and Welfare and demographic registers at Statistics Sweden. Register linkage was performed using the unique personal identity number assigned to each Swedish resident.6 Ethical approval was granted by the regional ethics committee at Karolinska Institutet, Stockholm, Sweden.
CKD and the Swedish National Health Service
Sweden had a population of 9.4 million on 31 December 2010 (http://www.scb.se), and comprised 21 counties. Stockholm County was the biggest with 2.1 million inhabitants, accounting for 22% of the population. The Swedish healthcare system was tax funded and offered universal access, and patients with renal replacement therapy were treated by nephrologists in inpatient and outpatient hospital care.7 Care for patients with CKD was a mix of mainly outpatient hospital and primary care. The decision to initiate renal replacement therapy was made by nephrologists from clinical evaluations based on the Swedish guidelines8 originating from the National Kidney Foundation-Kidney Disease Outcomes Quality Initiative (NKF-K/DOQI) guidelines9 and the corresponding European guidelines.10
Quality register sources
Patients with CKD
Data from the Stockholm County CKD Register were used, including adult patients with CKD in stages 4 and 5 and not on dialysis registered at Karolinska and Danderyd University Hospital from 1999 to 2010 in the outpatient setting. This does not include all patients with CKD stages 4 and 5 in the county, as some get care elsewhere and some remain undetected. Stages 4 and 5 were defined as an eGFR of 15–29 and <15, respectively. GFR was estimated using the abbreviated Modification of Diet in Renal Disease equation (mL/min/1.73 m2) using serum creatinine levels.11 Data on albuminuria were incomplete and, therefore, no analyses by albuminuria status were performed.
The National Patient Register
Data on inpatient and outpatient hospital care were retrieved from the Swedish National Patient Register.14 This register contains the personal identity number, visit/admission date (and discharge date for inpatients) and main as well as contributory diagnoses coded according to the International Classification of Diseases V.10 (ICD-10). The register reached national coverage in 1987 for inpatient care, and the outpatient component was added in 2001.
From inpatient and outpatient care registered in the National Patient Register, data on hospital visits listing diabetes, malignancies, circulatory disease and chronic obstructive pulmonary disease were gathered. Visits listing these diagnoses were searched for during the past 10 years (ICD-9 and ICD-10 codes provided in see online supplementary eTable 1).
Matched general population control cohort
From the Register of the Total Population at Statistics Sweden, up to five general population controls were matched to each patient at the time of inclusion into the CKD register, and renal replacement therapy initiation, using age (±1 year), sex and index year as matching factors. Data on emigration status and highest attained education were also retrieved from Statistics Sweden.
Outcome and follow-up
The primary outcome was all-cause mortality. Secondary outcomes for patients with CKD included initiation of renal replacement therapy and the composite outcome death or dialysis.
Dates and causes of death were retrieved from the Causes of Death Register kept by the National Board of Health and Welfare. Dates of death were available until 31 July 2010, while main and contributory death causes were available until 31 December 2008.
Patients with CKD and renal replacement therapy included from 1 January 1999 were analysed. Follow-up started at date of inclusion into the Stockholm CKD Register, dialysis initiation or transplantation. Patients accrued person-time in a specific health state until death, transition to another health state, emigration or 31 July 2010, whichever came first.
Statistical analysis
Unadjusted incidence rates and Kaplan-Meier curves were used to present absolute risks. For patients with CKD, a Cox proportional hazards model was used to model time to dialysis, and the composite outcome death or dialysis. The models were adjusted for age, sex, education level (≤9, 10–12, >12 years, missing), baseline eGFR (stage 4 vs 5), comorbidity status and index year.
Comparison versus the general population
In mortality analyses versus matched general population controls, Cox models conditioned on age, sex, education level, diabetes status and index year were used. Some patients did not have a full five controls, but were still included in the analyses, while patients with no controls were excluded. For dialysis and transplanted patients, the Andersen-Gill15 method was applied allowing for patients to re-enter a health state after exiting.
In order to investigate whether potential differences in all-cause mortality were driven by cardiovascular mortality, sensitivity analyses were performed for cardiovascular as well as non-cardiovascular deaths. An analysis was also performed to compare mortality by education level.
Direct comparison of CKD versus renal replacement therapy
To directly compare mortality in the different health states, a Cox model conditioned on age, sex, education level, diabetes status and index year was used with health state as the primary predictor.
Missing data on education level were handled using the missing indicator method. Data were complete on age, sex and register-determined comorbidity status. Missing baseline eGFR resulted in exclusion from CKD analyses.
Statistical analyses were performed using SAS (V.9.3) and Stata (V.11). All p values are two-sided and p values <0.05 were considered statistically significant.
Results
A total of 4249 patients were included. Follow-up of mortality was complete and all patients were analysed, except for 19 patients with CKD who were excluded due to missing baseline eGFR.
Patients’ characteristics at inclusion, dialysis initiation and transplantation are shown in table 1. Patients with CKD were, on average, 66 years old at inclusion, while dialysis patients were younger, and transplanted patients considerably younger: 48% of patients with CKD were more than 70 years old, compared with 37% of haemodialysis, 28% of peritoneal dialysis and 0% of the transplanted patients. All groups were predominantly men, and the education level was broadly similar to that in the general population.
Participant characteristics at chronic kidney disease register inclusion, start of dialysis or transplantation
Regarding selected register-identified comorbidities, the patients with CKD and dialysis were similar, while the younger transplanted group displayed a lower prevalence. More than 30% of patients (except the transplanted group) had diabetes, compared with 3–7% in the matched general population (see online supplementary eTable 2). Approximately 80% of patients had circulatory disease history at inclusion, with about 10% having had myocardial infarction and 10% stroke (except transplanted patients). In patients with CKD and dialysis, malignancies were also more common than in the general population.
In the CKD cohort at inclusion, the mean eGFR was 18 (SD 6; median 18; range 4.1–29.9). A third (n=999) had values <15, while 67% (n=2041) had values between 15 and 29 (full distribution shown in see online supplementary eFigure).
Observation time and deaths
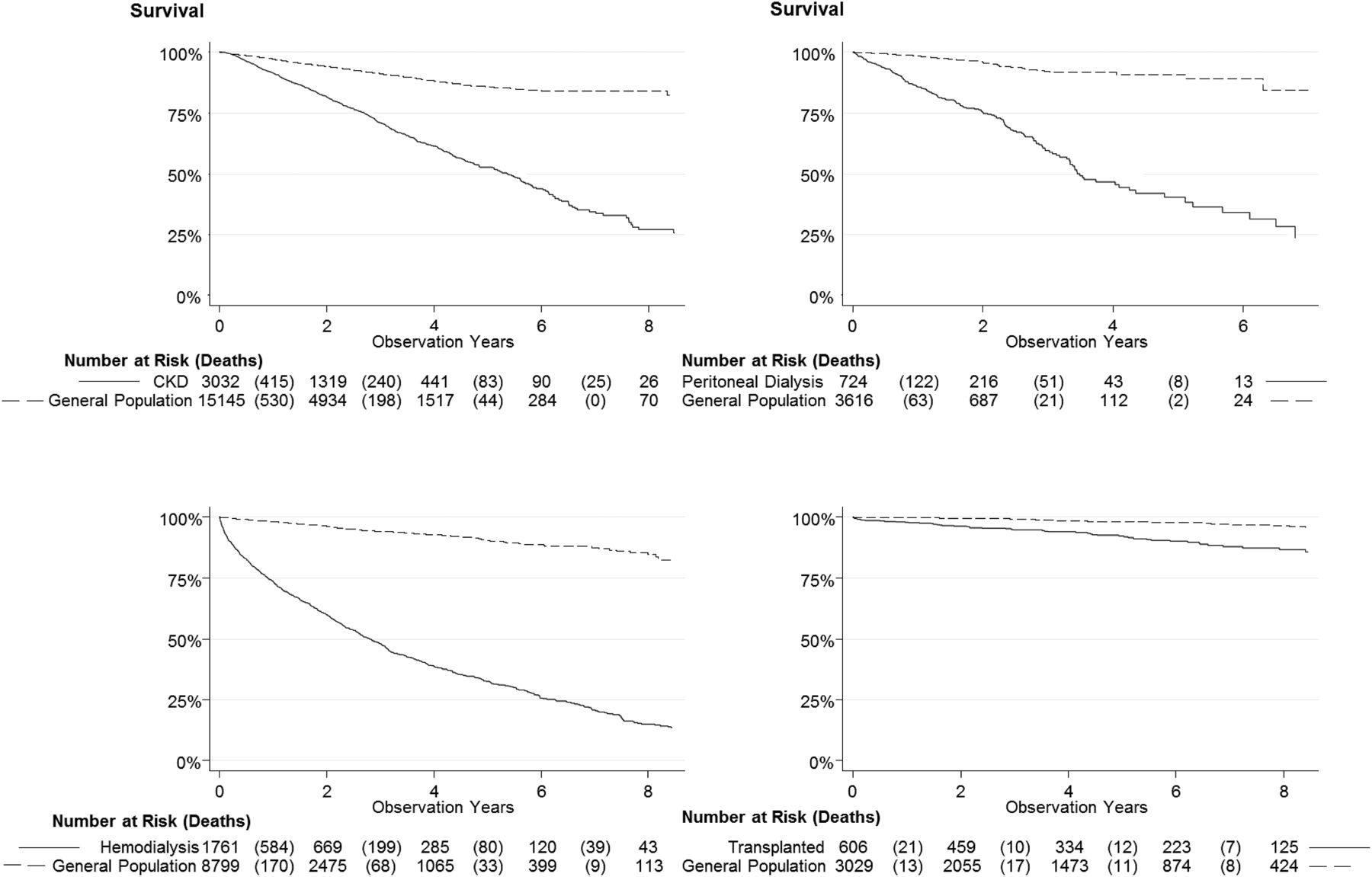
Crude death rates were highest in haemodialysis and lowest in transplanted patients (table 2; figure 1). When stratified by age, crude mortality rates were considerably lower in patients with CKD compared with dialysis patients, but remained higher than in transplanted patients (figure 2).
Mortality and accumulated person-years by health state

Survival curves describing time to death for patients with chronic kidney disease, peritoneal dialysis, haemodialysis and transplanted patients, as well as matched general population controls.

Crude mortality rates by health state and age.
Risk of dialysis and death in CKD
In patients with CKD, the analysis of time to death and time to dialysis was affected by the concurrent risk of starting dialysis or dying, respectively: older age was associated with an increased risk of death, but a decreased risk of dialysis progression (table 3). When analysing death and dialysis as a composite outcome, age displayed a borderline association. Having an eGFR of <15 compared with 15–29 at inclusion was associated with an almost threefold increased risk of death or dialysis, while male sex was associated with a smaller risk increase, as was low compared with high education and presence of comorbidity.
Adjusted HRs for risk of progressing to dialysis, death and death or dialysis for patients with chronic kidney disease stages 4 and 5 (conditioned on index year; n=3040)
Mortality compared with the general population
Against matched general population controls, the mortality HR was 3.6 (95% CI 3.3 to 4.0) for CKD, 5.6 (95% CI 3.5 to 8.9) for transplanted, 9.2 (95% CI 6.6 to 12.7) for peritoneal dialysis and 12.6 (95% CI 10.8 to 14.6) for haemodialysis patients (figure 3). Mortality HRs were statistically significant for cardiovascular as well as non-cardiovascular deaths for all groups.
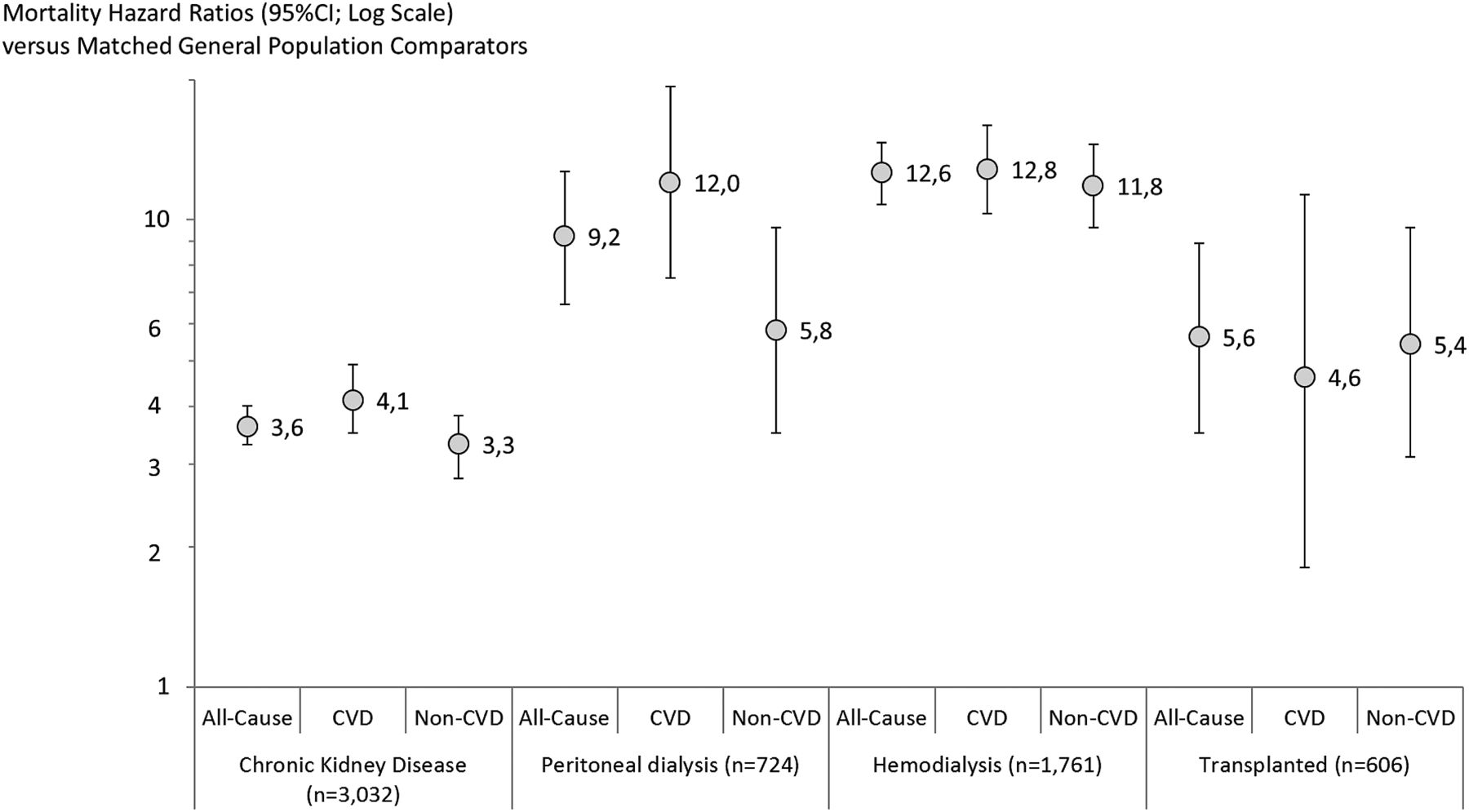
Conditional all-cause, cardiovascular (CVD) and non-cardiovascular (non-CVD) mortality HRs versus matched general population controls.
Mortality in CKD versus renal replacement therapy
In a direct comparison of patients in different health states (conditioned on age, sex, diabetes status, education level and index year), all groups differed significantly from each other in terms of mortality hazard: transplanted patients had the lowest risk, followed by patients with CKD stages 4 and 5, peritoneal dialysis and haemodialysis patients (table 4; all p<0.001). Compared with patients with CKD, peritoneal dialysis had a 1.7 (95% CI 1.4 to 2.1) and haemodialysis patients a 2.6 (95% CI 2.3 to 2.9) times greater mortality hazard.
Conditional* mortality HRs for chronic kidney disease stages 4 and 5, peritoneal dialysis, haemodialysis and transplanted patients compared with each other
Education level and mortality
Nine years of education or less, compared with more than 12 years, was associated with an increased mortality hazard overall (HR 1.4, 95% CI 1.2 to 1.7; figure 4). The HR point estimate for ≤9 years of education versus >12 years was elevated in all health states, but did not reach statistical significance in the smaller peritoneal dialysis and transplanted groups.

{kind=link}
{kind=link}
{kind=link}
{kind=link}
Mortality HRs by education level using >12 years of education as reference.
Discussion
Principal findings
In this population-based cohort study, we did not find support for mortality in CKD to be similar to dialysis mortality. Relative age-adjusted mortality was lowest in the transplanted group followed by CKD, peritoneal dialysis and haemodialysis. Compared with dialysis patients, patients with CKD had lower absolute mortality in age-adjusted analyses, lower relative mortality versus the general population and lower relative mortality in direct comparison.
Strengths and weaknesses
This study was population based, and the data were collected from routine clinical care centres to which there is universal access in Sweden. No restrictions were set regarding demography or comorbidities, increasing generalisability. Another strength was that we followed patients from CKD to death directly, or via different forms of renal replacement therapy. We could estimate death rates in CKD stages 4 and 5, as well as in haemodialysis, peritoneal dialysis and transplanted patients during the same calendar period and at the same hospitals.
Using the unique personal identity number of each Swedish resident and linkage to national mortality data, follow-up was complete. Using national registers, we could also collect data on comorbidities, as well as match general population controls to each patient, which is likely to result in more accurate estimates than if using aggregated life-table data.
One limitation was that while all renal replacement therapy patients in Stockholm County were included, an unknown number of patients with CKD were missed: CKD is underdiagnosed and many patients are identified only at dialysis start, or die before identification. Our results should, therefore, only be generalised to patients with CKD in nephrology care.
Second, comparing mortality estimates in the respective health states is complicated by channelling issues, as patients in renal replacement therapy are required to have survived the CKD health state.16 Such channelling of survivors likely decreases the mortality differential between CKD and dialysis patients. To be selected for transplantation, several prognostic factors are also considered, such as age and diabetes (which we adjusted for), but also general frailty (which we did not capture beyond certain comorbidities). Also, the lower mortality in peritoneal dialysis compared with haemodialysis should be interpreted with caution, as patients may transfer to haemodialysis at the end of life, inflating haemodialysis mortality estimates. Prognostic factors may also be worse for haemodialysis patients than in patients selected for peritoneal dialysis, although the groups were similar in terms of comorbidity status and education level. Other channelling variables may still influence relative mortality between the groups. Some observations could also support our finding of lower mortality in peritoneal dialysis than haemodialysis: data indicate that more frequent dialysis is beneficial,17 and peritoneal dialysis does not seem to result in the same degree of myocardial stunning,5 two factors that could contribute to lower mortality rates in peritoneal dialysis than in haemodialysis.
Finally, several important potential confounders were taken into account, such as age, sex, diabetes status and education level, but residual confounding due to other risk factors cannot be ruled out. For example, ethnicity may affect mortality through various mechanisms, including access to renal transplantation (depending on blood group and tissue type histocompatibility). We did not have access to ethnicity data and could, therefore, not determine whether there was an imbalance between cases and controls. The analyses were also limited by lack of albuminuria data.
Previous research
Go et al1 analysed 8458 insured patients with CKD stages 4 and 5 with similar mean age as in our study, and similar prevalence of diabetes. Their sample was predominantly female compared with only 35% women in our study. They found age-standardised death rates of 11 and 14/100 person-years in CKD stages 4 and 5, respectively, approaching the levels seen in dialysis. The death rates were standardised to their full study population which was comparatively young (mean age 52 years), complicating comparisons of absolute mortality rates with our study (mean age 66 years). They reported adjusted mortality HRs of 3.2 and 5.9 for the two groups versus insured patients with eGFR≥60.
In a meta-analysis of more than 100 000 patients, Matsushita et al4 used eGFR 90–104 as reference and found mortality HRs for patients with CKD stage 4 between 4 and 7 over a range of urine albumin-to-creatinine ratios. Our findings for CKD stages 4 and 5, versus matched general population controls, seem largely congruent with both these previous studies, but appear lower than the standardised mortality ratio of 8.3 reported by Evans et al2 from Sweden. This discrepancy is most likely explained by their exclusion of patients ≥75 years old (a patient segment making up 33% of our sample in the current study), as relative mortality compared with the general population decreases with age, pushing our estimates downwards compared with that of Evans et al's.
Regarding dialysis mortality, we found cardiovascular and non-cardiovascular mortality to be elevated, similar to findings from a large European analysis of dialysis mortality by de Jager et al.3 They analysed all dialysis patients as a group, while we separated peritoneal dialysis and haemodialysis patients (for which we found differential mortality).
We also found an association between education level and CKD progression, as well as survival in renal replacement therapy. This is in agreement with Swedish findings regarding risk factors for chronic renal failure (unskilled workers vs professionals),18 and a Danish study on risk of renal replacement therapy (low vs high income families, and low vs high education level).19
Implications
As mortality increases after peritoneal and haemodialysis initiation, optimal timing of dialysis start has been debated, particularly as dialysis is initiated at higher eGFR currently than previously: in the USA, in 1996, only 4% started dialysis with eGFR>15, while 15% did in 2005.20 The trend has been similar in Europe.21 A recent randomised controlled trial gave no indication that early start was beneficial for survival.22 Our data showing much higher mortality in peritoneal dialysis and haemodialysis compared with CKD, together with previous findings, indicate that caution should be exercised before initiating dialysis.
References
Supplementary materials
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
Files in this Data Supplement:
- Data supplement 1 - Online supplement
Footnotes
-
Contributors MN, SHJ, C-GE and BH conceived the study hypothesis. MN and JE conducted the statistical analyses. MN wrote the first draft of the manuscript. MN, SHJ, JE, C-GE and BH critically reviewed and contributed to the final draft. All authors are guarantors.
-
Funding This work was supported by Stockholm County Council and Baxter.
-
Competing interests MN has received payment for a lecture from Baxter. C-GE and BH have received a grant to their academic institution from Baxter to support the work with this publication. SHJ has acted on an advisory board for Baxter, and received lecture payments at scientific meetings. BH, SHJ and CGE are employed by Stockholm County Council.
-
Ethics approval Ethical approval was granted by the regional ethics committee at Karolinska Institutet, Stockholm, Sweden (DNR: 2009/1225-31/5).
-
Provenance and peer review Not commissioned; externally peer reviewed.
-
Data sharing statement No additional data are available.