Article Text

Abstract
Objectives Pseudomonas aeruginosa is a common nosocomial pathogen responsible for significant morbidity and mortality internationally. Patients may become colonised or infected with P. aeruginosa after exposure to contaminated sources within the hospital environment. The aim of this study was to determine whether whole-genome sequencing (WGS) can be used to determine the source in a cohort of burns patients at high risk of P. aeruginosa acquisition.
Study design An observational prospective cohort study.
Setting Burns care ward and critical care ward in the UK.
Participants Patients with >7% total burns by surface area were recruited into the study.
Methods All patients were screened for P. aeruginosa on admission and samples taken from their immediate environment, including water. Screening patients who subsequently developed a positive P. aeruginosa microbiology result were subject to enhanced environmental surveillance. All isolates of P. aeruginosa were genome sequenced. Sequence analysis looked at similarity and relatedness between isolates.
Results WGS for 141 P. aeruginosa isolates were obtained from patients, hospital water and the ward environment. Phylogenetic analysis revealed eight distinct clades, with a single clade representing the majority of environmental isolates in the burns unit. Isolates from three patients had identical genotypes compared with water isolates from the same room. There was clear clustering of water isolates by room and outlet, allowing the source of acquisitions to be unambiguously identified. Whole-genome shotgun sequencing of biofilm DNA extracted from a thermostatic mixer valve revealed this was the source of a P. aeruginosa subpopulation previously detected in water. In the remaining two cases there was no clear link to the hospital environment.
Conclusions This study reveals that WGS can be used for source tracking of P. aeruginosa in a hospital setting, and that acquisitions can be traced to a specific source within a hospital ward.
- BIOTECHNOLOGY & BIOINFORMATICS
- MICROBIOLOGY
This is an Open Access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/
Statistics from Altmetric.com
Strengths and limitations of this study
-
We have demonstrated that whole-genome sequencing can be used for source tracking of Pseudomonas aeruginosa in a hospital setting.
-
We show convincing evidence that transmission has occurred directly from water to patients, but other routes are as likely.
-
The main limitation of the study was the sample size, which could be attributable to interventions being carried out during the study.
-
Our study focused on a burns unit and critical care unit in a newly built hospital. Modes of P. aeruginosa transmission may be different in hospitals with different styles of plumbing and on other augmented care units.
Introduction
Pseudomonas aeruginosa is a ubiquitous Gram-negative bacterium and an important opportunistic pathogen in the healthcare setting. P. aeruginosa particularly affects those with impaired host or mucosal immunity and has a broad range of presentations including respiratory infections in cystic fibrosis and mechanically ventilated patients, bloodstream infections in premature neonates and wounds in burns injuries. Nosocomial P. aeruginosa outbreaks are frequently reported and associated with water sources such as taps, showers, mixer valves and flow straighteners, sink traps and drains.1–10 Other potential routes of transmission include cross-infection, for example, carriage on the hands of healthcare workers, and through contaminated medical equipment such as endoscopic devices.3 ,5
In the UK, the role of water in the transmission of P. aeruginosa in healthcare settings has become a matter of urgent concern in response to a recent high-profile outbreak affecting a neonatal critical care unit in Belfast in 2012.11 This source was eventually determined to be sink taps.11–13 National guidance is now in place detailing enhanced procedures for routine water sampling on augmented care units, with directed interventions such as disinfection and replacement of high-risk plumbing parts required.14
Historical phenotypic typing methods for P. aeruginosa such as O-antigen serotyping have more recently been replaced by molecular typing methods such as pulsed-field gel electrophoresis (PFGE), variable number tandem repeat analysis, random amplification of polymorphic DNA and multilocus sequencing typing (MLST).15 These methods have been used to investigate outbreaks of P. aeruginosa within hospitals.4 ,16–18 However, such techniques have important limitations for source tracking of infections in hospitals as they sample limited numbers of sites in the genome which may result in false clustering of unrelated strains.19 In the past 5 years, whole-genome sequencing (WGS) has started to be used to investigate outbreaks in hospitals. WGS is attractive because of its digital, sharable format and ultra-high resolution, which is able to discriminate two isolates differing by just a single mutation. WGS has been successfully used to determine likely transmission chains during outbreaks of Staphylococcus aureus, Acinetobacter baumannii and Klebsiella pneumoniae.19–21 Benchtop sequencing instruments now offer a cost-effective approach for bringing bacterial WGS to the clinical environment.22
In this study, we explore the utility of WGS to determine the likely sources of P. aeruginosa in an at-risk population of burns patients. In the UK and US burns patients receive shower cart hydrotherapy as a mainstay of burns treatment.23–26 A previous hospital audit suggested that up to one-third of such patients became colonised with P. aeruginosa. We hypothesised that this high rate of acquisition may relate to transmission from hospital shower water during therapy. We therefore wished to understand the importance of transmission from water compared with alternative routes such as cross-infection and endogenous carriage.
Materials and methods
Hospital setting
An observational, prospective study design was employed in a burns centre serving approximately 13.7 million people across the Midlands region of England with 300 admissions annually. Opened in June 2010, the burns centre comprises a purpose built 15-bed ward with 11 side-rooms and 2 dual-bedded rooms. Patients requiring mechanical ventilation and organ support are usually treated in two self-contained burns cubicles located within the trauma critical care unit. Despite the observational nature of the study, sampling was carried out during implementation of interim national guidance on control of P. aeruginosa issued by the Department of Health. These guidelines were issued in draft form March 2012, and subsequently revised in March 2013. This meant that parallel water sampling and engineering interventions were being undertaken during the period of study. In addition, some enhanced infection prevention measures were also introduced in response to an outbreak of a multidrug-resistant A. baumannii.
Study design and patient selection
Patients admitted to the burns unit were eligible for the screening phase of the study if they had burns injuries covering greater than 7% total body surface area (TBSA). Patients were screened as soon as possible after admission after they had given written informed consent. When appropriate, legal consultee advice was sought for patients lacking capacity due to emergency treatment. On admission, recruited patients were screened for carriage of P. aeruginosa (wounds, urine and stool) using standard microbiology techniques. Samples were then taken as part of routine microbiology service during the patients stay. Environmental and water samples were taken after the patient was admitted to the burns centre. If during the period of stay P. aeruginosa was isolated from a patient sample the patient was recruited into the second phase of the study. In this phase, patients had wound swabs taken at each dressing change as well as twice-weekly urine samples. The patient's environment and water from outlets in their bed space were sampled weekly for the duration of their stay, and after discharge (post-cleaning). Termination of the study was planned after 30 screening patient admissions, or a year, whichever came soonest, after which 10 patients were expected to acquire P. aeruginosa. This prediction was based on a previous local audit which suggested about one-thirds of burns patients became colonised with P. aeruginosa.
Microbiological and molecular methods
P. aeruginosa isolates were obtained from wound swab, urine, stool, environmental and water samples. P. aeruginosa was isolated from wound swabs, urine and stool by inoculation onto cysteine lactose electrolyte deficient agar (CLED) and cetrimide agar and incubation for 24 h at 37°C. Stool samples were cultured overnight in a cetrimide enrichment broth before subculture onto CLED. Identification was confirmed by resistance to C-390 and the VITEK 2 GN identification card. Antibiotic sensitivity assays were performed using the VITEK 2 AST N-210 card (bioMérieux, Basingstoke, UK).
The patient's environment (shower head rosette, drain, shower chair or trolley, bedside table, patient chair, instruments in contact with the patient) was sampled over a 10 cm2 area by a Polywipe sponge. The sponge was placed in tryptic soy broth incubated for 24 h at 37°C then subcultured onto CLED and cetrimide agar. During water sampling, water was taken from the patient's shower, or tap if a shower was not present. Shower heads were not removed for water sampling. At least 200 mL of water was collected into a vessel containing sodium thiosulfate as a neutraliser. In duplicate, 100 mL of water was filtered through a 0.45 µ filter and the filters placed onto CLED plates and cetrimide agar. Plates were incubated at 37°C for 48 h and the number of organisms per 100 mL quantified.
For storage and DNA extraction a single colony was purified from the primary culture plate. When different colony morphologies were observed, a single colony from each type was purified. Additionally, for a randomly selected water sample, 24 colonies were individually picked from one water-filter primary microbiological plate for sequencing. Isolates were stored on Biobank beads at −20°C prior to DNA extraction. Organisms were resuscitated on CLED agar plates and genome DNA either extracted directly using the MOBIO UltraClean Microbial DNA Kit, or from overnight LB broth culture using a Qiagen Genomic-Tip 100G.
DNA extraction and sequencing
Genomic DNA was prepared from single colony picks using the MOBIO Ultraclean microbial kit (MOBIO, Carlsbad, USA). 1 ng input DNA, as quantified by Qubit (Life Technologies, Carlsbad, USA) was used to prepare genomic libraries for sequencing using the Illumina Nextera XT DNA sample kit as per manufacturer's protocol (Illumina, San Diego, USA). Libraries were sequenced on the Illumina MiSeq using a paired-end protocol resulting in read lengths between 150 and 300 bases. A single additional sample, isolate 910, was chosen as a representative member of Clade 5 for long-read sequencing. DNA from this sample was fragmented using a Hydroshear (Digilab, Marlborough, Massachusetts, USA) using the recommended protocol for 10 kb fragments and further size-selected on a BluePippin instrument (Sage Science, Massachusetts, USA) with a 7 kb minimum size cut-off. The library was sequenced on two SMRT Cells using the Pacific Biosciences RS II instrument at the Norwegian Sequencing Centre, Oslo. C4-P2 chemistry was chosen because it favours long, more accurate reads for de novo assembly.
Stool PCR
For simple presence/absence detection of P. aeruginosa in stool samples using PCR, a stool sample was collected into a stool collection tube containing stool DNA stabiliser. Total DNA was extracted using the PSP Spin Stool DNA Plus kit (Stratec Molecular). PCR amplification of species specific regions of the 16S rDNA gene was carried out using primers PA-SS-F: GGGGGATCTTCG GACCTCA and PA-SS-R: TCCTTAGAGTGCCCACCCG 12 in the following conditions: 0.5 µM of each primer, 1.5 mM MgCl2, 0.2 mM dNTP's using BIOTAQ DNA Polymerase and buffer set. After initial denaturation at 96°C for 2 min, 30 cycles of 96°C for 30 s, 62°C for 30 s and 72°C for 30 s were completed with a final extension of 72°C for 5 min. Products were visualised for size on an 1.5% agarose gel.
Bioinformatics methods
Illumina MiSeq reads from each isolate were adapter and quality trimmed before use with Trimmomatic.27 Phylogenetic reconstruction of isolates sequenced in this study were combined with data from a global collection of 55 P. aeruginosa strains collected world-wide which have been previously analysed by Stewart et al.28 For each of the published strains, 600 000 paired-end reads of length 250 bases were simulated using wgsim (https://github.com/lh3/wgsim) from the complete or draft genome assembly deposited in Genbank. Read sets were mapped against the P. aeruginosa PAO1 reference genome using BWA-MEM 0.7.5a-r405 using default settings.29 Single nucleotide polymorphisms were called using VarScan 2.3.6 and filtered for regions with an excessive number of variants. These may represent regions of recombination, misalignments or strong Darwinian selection.30 FastTree (V2.1.7) was used for phylogenetic reconstruction. This software estimates an approximate maximum-likelihood tree under the Jukes-Cantor model of nucleotide evolution with a single rate for each site (CAT).31 Trees were drawn in FigTree (http://tree.bio.ed.ac.uk/software/figtree/).
For in silico MLST prediction, trimmed reads were assembled de novo using Velvet 32 with a k-mer size of 81 and searched using nucleotide BLAST against the multilocus sequence database downloaded from the pubMLST website on 5 August 2013 (http://pubmlst.org/paeruginosa/).33 For Clade E isolates, in order to exhaustively search for discriminatory mutations, a nearly complete reference genome was generated by de novo assembly using Pacific Biosciences sequencing data. Reads were assembled using the ‘RS_HGAP_Assembly.3’ pipeline within SMRT Portal V2.2.0. Illumina reads from the same sample were mapped to this draft genome assembly in order to correct remaining indel errors in the assembly using Pilon (http://www.broadinstitute.org/software/pilon/). Isolates belonging to each clade were mapped individually against either the PacBio reference (Clade E) or P. aeruginosa PAO1 (NC_002516; Clades C, D and G).
Variants (single nucleotide polymorphisms and short insertion-deletions) were called using SAMtools mpileup and VarScan with an allele frequency threshold of 80%.30 Non-informative positions and regions of putative recombination were removed, the later with a variant density filter of more than 3 SNPs every 1000 nucleotides. Analysing samples in each clade individually maximised the number of variants detected by reducing the likelihood of the position being uncovered by a subset of samples. From these variants fine-grained phylogenetic trees were reconstructed for each clade using FastTree. The scripts used to perform this analysis are available at http://www.github.com/joshquick/snp_calling_scripts. Approximate-maximum-likelihood phylogenetic trees were generated using FastTree and visualised in FigTree. For whole-genome shotgun metagenomics analysis, reads were analysed using the Kraken taxonomic classifier software with the supplied minikraken database.34 Reads from the metagenomics data set were aligned to P. aeruginosa Clade E as in the previous section and phylogenetic placement was carried out using pplacer in conjunction with FastTree.35 Sequence data is available from the European Nucleotide Archive for the Illumina data (ERP006056) and the corrected Pacific Biosciences assembly (ERP006058).
Results
Study results
Recruitment lasted a period of 300 days, ending according to protocol after the enrolment of 30 screening patients. In total, we detected P. aeruginosa in five patients. Of these patients, three had P. aeruginosa detected only in burns wound swabs, one had P. aeruginosa detected in their burns wound and in their urine, and one had P. aeruginosa in their sputum. One additional eligible patient did not consent to enter the study and was excluded. The average age in the study group was 41 years. Males predominated with a male-to-female ration of 2.3:1. Flame burns were the most common mechanism of injury, followed by scalds and mixed flame/flash injuries. The average burn size of the study group was 12.5% of the TBSA and 27% of patients sustained an inhalation injury. Eight patients required admission to intensive trauma unit (ITU) and the majority required surgical treatment of their burns with excision and skin grafting (80%). A large majority of the study group (83%) received shower cart hydrotherapy as a routine part of their wound management to encourage healing through wound debridement and decontamination. The average length of hospital stay (LOS) was 17 days and taking into account burn size, the average was 1.4 days per % TBSA.
The water and environment in burns and critical care units are frequently colonised by P. aeruginosa
A total of 282 water and environmental samples were screened for P. aeruginosa of which 39/78 (50%) were positive in water samples, 25/96 (26%) were positive from the wet environment and 7/108 (6%) were positive from the dry environment. A total of 86 genome sequences were generated from the 71 positives, as in some cases multiple colony picks were sequenced. Seventy-eight patient samples were screened for P. aeruginosa of which 39 (50%) were positive. A total of 55 genome sequences were generated, as in some cases multiple colony picks were sequenced. In total, 141 genomes were sequenced; water and environmental (n=86) and patient (n=55). Genomes were sequenced to a mean coverage of 24.4×, with the minimum coverage of a sample being 14× and highest 64.7×.
When placed in the context of a global collection of P. aeruginosa strains, phylogenetic reconstruction demonstrated isolates in our study fell into eight clades (figure 1A). As has been reported previously, there was no strong association between ecological context and position in the phylogenetic tree.28 Isolates in this study are most closely related to strains from a variety of settings. The majority of isolates (52%) belong to Clade E (figure 1B), whose nearest sequenced relative is the Liverpool Epidemic Strain, a clone often isolated from patients in the UK and Canada with cystic fibrosis. 36 ,37 Isolates from Clade E were found in the burns unit's water and the ward environment, as well as from two patient's wounds. However it was never detected in the critical care unit. Clade E was detected throughout the study in a total of 10 different rooms (figure 2).
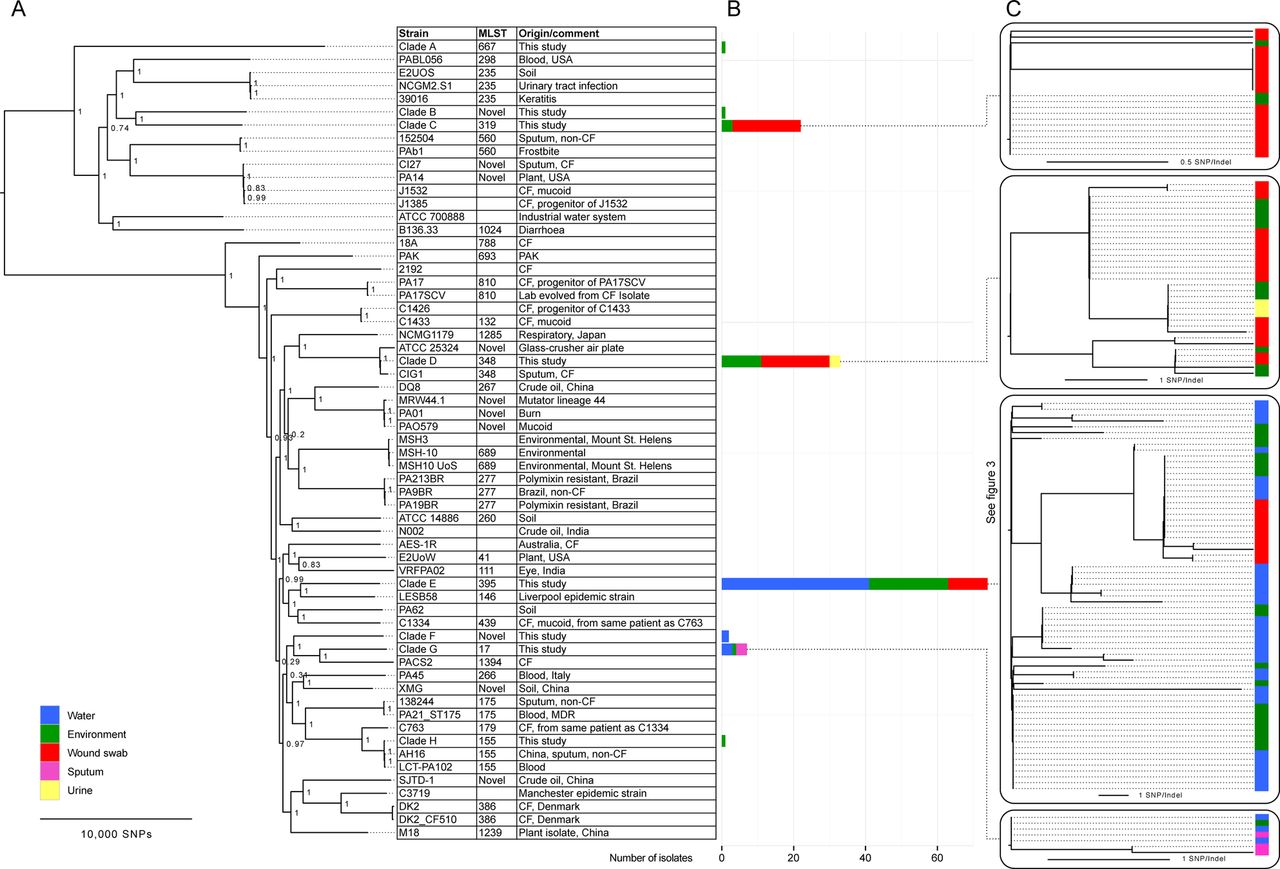
An overview of all samples collected during the study in global phylogenetic context with other sequenced strains of Pseudomonas aeruginosa from the set of Stewart et al.28 Samples collected in this study are widely dispersed in the tree, which contains isolates from different environments (A). Bar plots indicate the numbers of each type of sample collected (B). Microdiversity within each clade is shown, with the colour bar indicating the source of each sample (C).

A schematic view of the 300-day study of Pseudomonas aeruginosa in a burns centre and critical care unit. Time in days is shown along the x axis with bed numbers in the critical care unit and burns unit along the y axis. Each circular icon indicates a positive isolate of P. aeruginosa. The icon's logotype indicates which environment it originated from (wound, urine/sputum, environment or water). The filled colour of the icon indicates the clade it belongs to. Patient icons represent the enrolment of a screening patient into the study and their location. Patient movements around the hospital are noted by dotted lines. The five patients infected with P. aeruginosa are denoted by rounded boxes. Boxes are coloured according to the patient number. In the event two or more isolates of the same source and clade were collected on the same day, these have been collapsed into a single circular icon.
Inferring potential transmission events by WGS
Microevolutionary changes occurring over rapid time-scales (ie, days to months) have been used to detect potential chains of transmission in hospital and community outbreaks.19–21 ,38 ,39 The number of distinct mutations between given isolates has been used to infer whether transmission events are likely to have occurred. Such inferences are aided by prior knowledge of mutation rates in similar populations. Two patients (1 and 4) in our study both had P. aeruginosa from Clade E isolated from their wounds. These isolates had an indistinguishable genotype from those present in water and the environment of the room they were nursed within (figures 1C and 3). This genotype was detected in the patient's shower water after initial patient screening, during screening of the second patient admission, twice during the second patient's stay and then 127 days later (days 27, 65, 89 and 216, respectively). When water isolates were positive, the genotype was also detected in wet environment sites (shower drain, shower rosette and patient's trolley) on the same days.
Patient 5 was nursed on the critical care unit due to concomitant medical problems. P. aeruginosa belonging to Clade G was isolated from sputum during this time. Identical genotypes were detected contemporaneously in the water from the associated sink and sink tap handle (see online supplementary appendix 4).
Two further patients (patients 2 and 3) were positive for P. aeruginosa. Isolates from these patients belonged to Clade C and D, respectively. Neither clade was ever isolated from hospital water. In both cases, identical genotypes were detectable in the environment associated with the patient but these were not detected before or after the patients’ stay, indicating that the environment was not persistently contaminated. During the course of patient 3's stay, the dry environment such as the bedside table was contaminated, as was the patient's door handle and shower chair. However, after patient discharge, the strain associated with this patient was never seen again during the course of the study in any location.
WGS permits source tracking of P. aeruginosa to individual water outlets
WGS has been reported previously for source tracking, but never for the detection of transmission events from hospital water.40 Phylogenetic reconstruction within Clade E, the most commonly detected water clone demonstrated additional diversity within this clone, with a total of 46 mutations detected an average genetic distance between isolates of 4.1 mutations (figure 3). The reconstruction demonstrated clear evidence of clustering of genotypes both by room and outlet (figure 3). When P. aeruginosa was detected in the wet environment (eg, shower rosettes and drains) these genotypes were most often identical to those found in water, indicating that the water was likely the ultimate source of that clone. Genotypic variation was seen between outlets within the same room. For example, tap water sampled from room 11 had a distinct genotype from that sampled from shower water in the same room and this was consistently found over multiple samplings. Notably, isolates from two patients fell within the cluster originating from shower water, indicating that shower hydrotherapy was the most likely source of infection. Two plasmids (designated pBURNS1 and pBURNS2) were detected in this study set, which both demonstrated geographical clustering, with pBURNS1 only being detectable in isolates from room 8 and pBURNS2 only being detectable in isolates from the shower water in room 9.

{kind=link}
{kind=link}
{kind=link}
The high-resolution phylogenetic reconstruction of Clade E isolates. This demonstrates the clustering of genotypes by bed space. Patient associated samples are contained within a room 11 clade. This clade contains water samples from the shower and environmental samples from the shower, drain and trolley. The water samples from the room 11 tap are in a distinct clade, indicating the biofilm within the tap has a distinct genotype to the shower. This suggests environmental contamination was more likely to arise from contaminated shower water than tap water. Details of sampling site, days since start of study and presence of pBURNS plasmids are also shown. The likely phylogenetic position of Pseudomonas aeruginosa detected in a biofilm from a thermostatic mixer valve is shown in the clade associated with room 9 and indicated ‘TMV’.
Rapid evolution of antibiotic resistance associated with treatment
P. aeruginosa is commonly associated with antibiotic resistance due to a number of predisposing features including intrinsic resistance, a repertoire of efflux pumps and antibiotic-inactivating enzymes including β-lactamases.41 Three infected patients (2, 3 and 5) received antibiotic therapy, and in each case this was associated with the development of resistance to at least one therapeutic agent. Associated mutations were detected that were either partially or fully explanatory of the phenotype (online supplementary appendix 12).
Patient 2 was treated with ciprofloxacin, nitrofurantoin and vancomycin (see online supplementary appendix 11 for full details). Eight of 21 (38%) tested isolates from this patient were ciprofloxacin resistant. Seven of eight isolates (88%) of the ciprofloxacin-resistant strains were distinguishable from the other isolates by a single SNP in mexS (annotated as PA2491 in P. aeruginosa PAO1; see online supplementary appendix 1 and 7). This SNP was predicted to result in a non-synonymous amino acid substitution. Disruption of this gene has been shown to cause increased expression of the mexEF-oprN multidrug efflux pump, associated with resistance to quinolones.42
Patient 3 was not treated with antibiotics, but isolates associated with this patient demonstrated differences in resistance to timentin and piperacillin-tazobactam. These changes were associated with non-synonymous mutations in gacA, the response regulator of the GacA/GacS two-component system and in lasR, a transcriptional activator required for transcription of elastase and LasA protease (online supplementary appendices 2 and 8).
Patient 4 was treated with meropenem, piperacillin/tazobactam, flucloxacillin and colistin. Five isolates collected 10–18 days after initiation of meropenem showed resistance to imipenem and intermediate resistance to meropenem (see online supplementary appendix 3 and 9). The most likely mutation responsible for this phenotype was detectable in two isolates, both of which had a frame-shift mutation in the gene coding for the membrane porin OprD.43
Patient 5 had a prolonged stay in ITU and had multiple medical problems including A. baumannii infection and was treated with nine antibiotic agents including ciprofloxacin, meropenem and piperacillin-tazobactam. Serial isolates from this patient demonstrated the stepwise acquisition of two mutations (online supplementary appendix 4). The first was in nalC, a probable repressor of the TetR/AcrR family (online supplementary appendix 10).44 On inspection of the sequence alignment in this region, a large deletion of 196 nucleotide bases was seen compared to the reference PAO1 strain. This mutation was seen in association with full resistance to piperacillin-tazobactam, ceftazidine, aztreonam, meropenem and intermediate resistance to ciprofloxacin. This deletion is likely to result in over-expression of efflux pumps involving the mexAB-oprM operon.44 ,45 Ciprofloxacin resistance in a later isolate corresponded to the stepwise acquisition of a second mutation. This mutation is predicted to affect the well-studied DNA gyrase subunit A gene (gyrA) which is strongly associated with ciprofloxacin resistance.46
Confirmation of P. aeruginosa genotypes in biofilms by whole-genome metagenomic shotgun sequencing
P. aeruginosa is able to produce and survive in biofilms. Plumbing parts such as flow straighteners, shower rosettes, flexible hoses, solenoid valves and thermostatic mixer valves (TMV) are particularly at risk of biofilm formation due to factors including surface areas, convoluted designs and inadequate pasteurisation.47 To confirm the presence of P. aeruginosa in water fittings associated with rooms on the burns unit, we obtained a TMV removed by the hospital estates team from the shower in room nine as part of compliance with UK guidelines for managing P. aeruginosa in hospitals. On visual inspection, a biofilm was present which was scraped from the surface with a sterile scalpel. DNA from this biofilm was extracted for whole-genome shotgun sequencing. The majority of reads did not map to any known bacterial taxa. The most abundant taxon identified was P. aeruginosa (3%). Subsequent alignment to the P. aeruginosa Clade E reference covered 94% of the 6.3 million base reference genome at a median coverage of 5×, confirming that reads were correctly classified to this species and not other environmental Pseudomonas species. Alignment to the P. aeruginosa Clade E reference genome followed by phylogenetic placement of reads demonstrated that it fell into the same clade as previously recovered isolates from the shower or tap in room 9 (indicated on figure 3, and in online supplementary appendix 6).
Discussion
The hospital environment has been intimately linked with P. aeruginosa infection for over 50 years yet hospital acquisitions, clusters and outbreaks remain a common occurrence and understanding precise routes of transmission can be difficult.47 ,48 Our results demonstrate that, even in a new hospital, P. aeruginosa can become rapidly endemic in hospital plumbing. Furthermore, by linking P. aeruginosa genotypes recovered from patients to specific individual water outlets, we offer compelling evidence of unidirectional transmission from water to patients. Further, by sequencing of a biofilm identified in a TMV from a hospital water system, we can identify the likely common source of genotypes found in water and in the hospital environment.
Our results suggest that use of WGS can reduce ambiguity about potential transmission events in hospitals and consequently inform infection prevention efforts about the direction and sequence of transmission. Typing schemes such as MLST and PFGE are much lower resolution methods and would not be able to provide sufficient information to permit such inferences to be made. It is notable that the burns unit was colonised by a single clone, meaning that it was very unlikely that water outlets at each bed space were colonised as a result of transmissions from the patient or environment. For this to happen would require multiple transmission events from separate patients with the same clone, for which there is no evidence. Instead we speculate that this clone was introduced to the hospital associated with its commissioning. One hypothesis is that particular plumbing fittings, that is, the TMV may have been colonised simultaneously by a clone circulating in water. Clade E (ST395) has been frequently reported associated with water, so this remains a possibility. 49 ,50 However, it is possible that plumbing fittings are installed ‘pre-seeded’ with P. aeruginosa as has already been proposed by Kelsey.3 ,5 ,47 Investigation of an outbreak in Wales implicated new plumbing parts as a potential source of P. aeruginosa. New plumbing components are often tested by companies prior to their supply and it is possible they were contaminated prior to distribution. The limited amount of diversity (average 4 SNPs) seen within this clade is consistent with a single founding genotype coinciding with the opening of the burns unit, based on estimates from a previous study using WGS which reported that mutations accumulate at a rate of approximately one every 3–4 months in a hospital-associated clone.51 However, our results suggest that our isolates accumulate mutations even more slowly. This may be due to reduced growth rates in nutritionally-poor biofilms.52
It is notable that antibiotic resistance to multiple first-line agents developed rapidly in response to therapy. These results underline the importance of selecting appropriate antibiotic therapy in P. aeruginosa infections. It is reassuring however that antibiotic resistance genotypes selected in vivo did not show evidence of persistence in the ward environment or transmission to other patients.
Our study has certain limitations. Based on a previous audit, we expected around one-third of patients screened for P. aeruginosa would develop colonisation or clinical infection. In fact, only 5 out of 30 of patients were colonised. This may have been related to guidance and engineering interventions being put in place during the study as detailed in national guidance issued while this study was on-going. In addition, infection control policies were revised to address control of an outbreak of a multidrug resistant A. baumannii in this same burns unit. Following these interventions, only 1 of the last 20 patients recruited was infected with P. aeruginosa which may demonstrate the importance of national guidance in reducing transmissions.
By focusing on burns patients who receive hydrotherapy, our study population were at extremely high risk of waterborne infection. In other patient groups it may be that alternative routes of transmission including cross-infection or endogenous carriage play a more important role. Our results suggest that our burns unit is endemically colonised with a distinct clone of P. aeruginosa that may have been imported coinciding with the opening of the hospital. Other intensive care units, particularly those which have been open for longer may harbour a greater diversity of P. aeruginosa as a result of increased opportunities for clones to be imported.
One potential application for WGS in infection control would be to determine whether cases are as a result of water transmission, or represent sporadic clones originating from the wider environment. Despite improved guidance concerning improved engineering infection control practices and the introduction of the water safety group in the UK, it may not be realistic to eliminate P. aeruginosa from hospitals entirely. In augmented care units such as ITUs, burns units and neonatal wards where P. aeruginosa poses a significant risk to vulnerable patients, the increased resolution offered by WGS will justify its use, particularly as the costs continue to fall.
In conclusion, we have identified through WGS clear evidence for transmission of P. aeruginosa from specific water outlets to burns patients and offer a forensic-level framework for dealing with outbreaks linked to hospital water. We expect WGS will continue to make inroads into clinical microbiology and become a vital tool for tracking P. aeruginosa in the hospital environment, helping inform targeted control measures to help protect patients at risk of infection.
Acknowledgments
The authors are grateful to Mark Webber for discussions on antibiotic resistance and to Paul Keim for discussion on phylogenetic placement of metagenomics samples. The authors thank Lex Nederbragt, Ave Tooming-Klunderud and the staff of the Norwegian Sequencing Centre, Oslo for Pacific Biosciences sequencing. The authors thank Matthew Smith-Banks for laboratory assistance with processing samples. The authors also thank Jimmy Walker for critical reading of the manuscript. The authors also thank Drs David Baltrus, Thomas Connor, Jennifer Gardy and Alan McNally for their helpful comments and suggestions to help improve the manuscript made during the open peer review process.
References
Supplementary materials
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
Files in this Data Supplement:
- Data supplement 1 - Online appendix
Footnotes
JQ and NC contributed equally.
-
Contributors MJP, NSM and BO conceived the study. CMW and AB enrolled patients into study and collected samples. NC collected environmental and water samples. NC, CC and MN processed samples and performed microbiology. NC, CC and JQ did sequencing. JQ, NC, CMT and NJL analysed the data. NJL, NC, JQ, MJP and BO wrote the paper. All authors commented on the manuscript draft.
-
Funding This paper presents independent research funded by the National Institute for Health research (NIHR). The views expressed are those of the author(s) and not necessarily those of the NHS, the NIHR or the Department of Health. NJL is funded by a Medical Research Council Special Training Fellowship in Biomedical Informatics.
-
Competing interests None.
-
Ethics approval The study protocol received approval from National Research Ethics Service committee in the West Midlands (reference number 12/WM/0181).
-
Provenance and peer review Not commissioned; externally peer reviewed.
-
Data sharing statement Pacific Biosciences raw data files are available from the corresponding author (Nicholas J Loman, n.j.loman@bham.ac.uk).