Article Text

Abstract
Objective Improved drug labelling for chronic pill-form medications has been shown to promote patient comprehension, adherence and safety. We extended health literacy principles and included patients' perspectives to improve instructions for: (1) non-pill form, (2) short term, (3) ‘as needed,’ (4) tapered and (5) escalating dose medications.
Setting Participants were recruited via convenience sampling from primary care clinics in Chicago, Illinois and San Francisco, California, USA.
Participants 40 adult, English-speaking participants who reported taking at least one prescription drug in the past 12 months were enrolled in the study.
Primary and secondary outcomes Participant opinions, preferences and comprehension of standard and improved medication instructions were assessed during four iterative waves of discussion groups. Brief interviews preceding the discussion groups measured individuals’ literacy skills, sociodemographic and health characteristics.
Results On average, participants were 46 years old, took four medications and reported two chronic health conditions. Patients varied sociodemographically; 40% were men and 33% had limited literacy skills. Patients agreed on the need for simpler terminology and specificity in instructions. Discussions addressed optimal ways of presenting numeric information, indication and duration of use information to promote comprehension and safe medication use. Consensus was reached on how to improve most of the instructions.
Conclusions Through this patient-centred approach, we developed a set of health literacy-informed instructions for more challenging medications. Findings can inform current drug labelling initiatives and promote safe and appropriate medication use.
- GENERAL MEDICINE (see Internal Medicine)
- PRIMARY CARE
- THERAPEUTICS
This is an Open Access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 3.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/3.0/
Statistics from Altmetric.com
Strengths and limitations of this study
-
This study was conducted in two distinct geographical regions, incorporated diverse viewpoints and used health literacy ‘best practices’ to improve drug labelling.
-
While rigorous, our study relied upon a relatively small sample of English-speaking adults and focused only on developmental activities.
-
Additional research will be needed to replicate the findings, develop Rx instructions in other languages and comprehensively evaluate the proposed instructions against the current standards.
Introduction
Approximately 4.5 million outpatient visits each year are related to adverse drug events (ADEs) and recent estimates indicate that preventable, outpatient ADEs cost the US healthcare system more than US$8 billion/year.1–4 While the underlying factors leading to outpatient medication errors vary, patient's misunderstanding of prescription (Rx) medication instructions is likely to be a major root cause.2 ,5 ,6 This is not surprising, as current Rx labelling practices frequently fail to support patient's understanding or safe use of prescribed drugs. Evidence indicates that Rx labelling is highly variable and Rx instructions are often vague and unnecessarily complex.7 ,8 As a result, patients may misinterpret seemingly simple directions for use. A 2006 study found that nearly half (46%) of patients misinterpreted at least one of five common Rx instructions.9
In response to this patient safety and healthcare quality concern, the 2008 Institute of Medicine (IOM) report Standardizing Medication Labels called for setting labelling standards to help patients easily understand Rx directions for use.10 The ‘Universal Medication Schedule’ (UMS) was proposed in this report to promote safe medication use. The UMS uses ‘best practices’ from the fields of health literacy, medicine and education to explicitly describe how to take daily use, pill-form medications.10 Specifically, the UMS grounds medication-taking to four time periods (morning, noon, evening, bedtime) and uses simplified language and formatting to promote understanding (ie, ‘take 1 pill in the morning and 1 pill at bedtime’ instead of ‘take one tablet twice daily’). An efficacy trial of the UMS instructions found that patients were 33% more likely to correctly interpret these instructions compared with a current standard, with overall comprehension rates of the UMS instructions exceeding 90%.11 Despite these findings and high levels of support from government agencies, the UMS has not been universally adopted by pharmacies and healthcare organisations.
While the current UMS framework is a promising first step towards promoting safe and appropriate medication use, to date, it has only been applied to daily use, solid-form medications. To address this shortcoming, our team sought to apply UMS principles to instructions for: (1) non-pill form (ie, injections, inhalers and liquids); (2) short term (ie, antibiotics); (3) ‘as needed’ (ie, pain relievers) and (4) tapered and escalating dose medications (ie, steroids and antidepressants). These medications account for a sizeable proportion of the short-term and chronic care medications currently prescribed and are often the most confusing and difficult for patients to self-administer.2 ,12 To accomplish our objective, we first developed a draft set of instructions incorporating health literacy best practices with the assistance of a Scientific Advisory Board (SAB). We then conducted an iterative series of discussion groups with patients to further refine and develop these instructions from a patient's perspective.
Methods
Developing ‘improved’ instructions
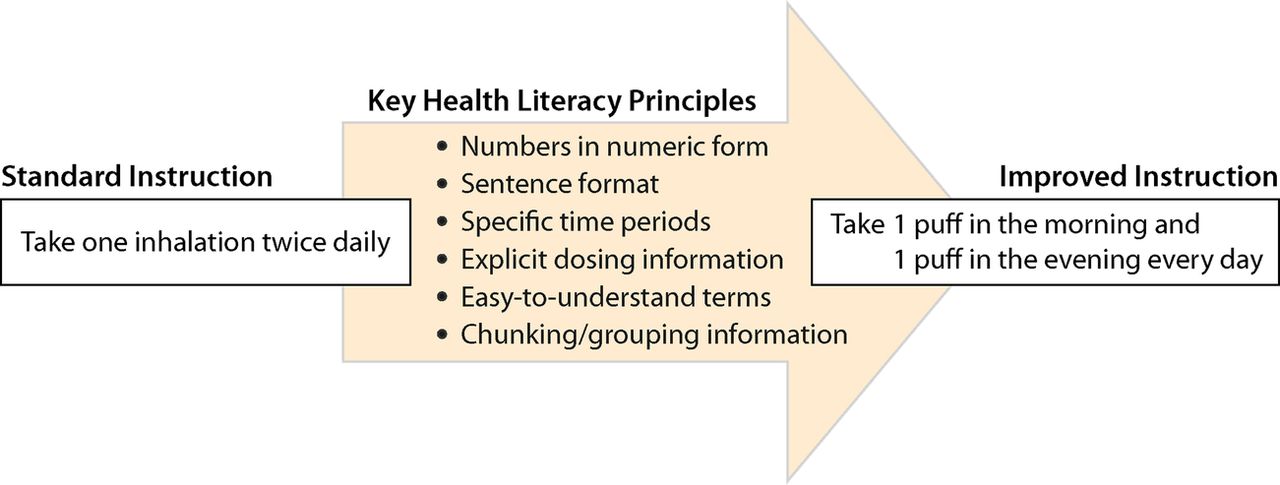
As the first step in the development process, the study team drafted an initial set of ‘improved’ medication instructions for non-pill form, short term, ‘as needed,’ tapered and escalating dose medications. Instructions incorporated the UMS and health literacy best practices whenever possible.10 The SAB, comprised three health literacy and drug labelling experts (2 physicians, 1 psychologist), assisted the study team in this process. Figure 1 provides an overview of key health literacy principles and an explanation of how they were incorporated into the design of the ‘improved’ draft instructions developed by the study team.
{kind=link}
Applying health literacy practices to prescription medication labelling.
Study participants
To incorporate a patient's perspective into the development of improved instructions, a series of brief interviews and discussion groups were then conducted. Study participants included adult patients who were recruited via convenience sampling from clinics in Chicago, Illinois and San Francisco, California, USA. Eligibility criteria were purposively broad and included: (1) age 18 or older, (2) English-speaking, (3) taken at least one prescription medication in the past year and (4) no severe cognitive or visual impairment that would preclude their informed consent or study participation. Study flyers briefly described the research study and asked interested individuals to call a research assistant (RA) to learn more about the study. Trained RAs spoke to interested participants by phone, assessed eligibility and scheduled focus groups around participant availability. The Institutional Review Boards (IRBs) of the University of California at San Francisco and Northwestern University approved the study.
Individual interviews
All participants completed a brief, individual interview prior to the discussion group. The individual interview was administered by RAs in a private area and included assessments of the participant's sociodemographics (age, sex, education, income, insurance coverage, employment status) and health characteristics (health status, prescription medication use, chronic health conditions). Literacy skills were measured through the Rapid Estimate of Adult Literacy in Medicine (REALM), a short screening test designed to identify individuals with reading difficulties.13
Discussion groups
Discussion groups were held immediately following the individual interviews. A total of four focus groups were conducted (n=2 in each location), each lasting approximately 1 h. All groups were moderated by two study team members (SCB and MSW) to ensure consistency. During these discussion groups, participants were shown a series of ‘standard’ and ‘improved’ medication instructions for non-pill form, short term, ‘as needed,’ tapered and escalating dose medications. For each type of medication, participants were asked to consider how the terminology and phrasing of instructions could be improved to promote comprehension. Discussions were iterative in nature; suggestions made during initial focus groups were reviewed in later discussion groups. The study team refined the set of ‘improved’ instructions periodically based on discussion group feedback. The study participants were compensated US$40 cash for their time and effort.
Analysis plan
Quantitative analyses were performed using STATA, V.11.0. Specifically, descriptive statistics were calculated for variables measuring the participants’ sociodemographic and health characteristics. REALM scores were dichotomised; participants were classified as having either adequate or low/marginal literacy skills. A qualitative descriptive approach was utilised for discussion groups, which were recorded using a separate note-taker at each session. Investigators utilised a content analysis approach, where the patient comments and discussions were broadly categorised and classified to discern participants’ preferences for optimal wording, phrasing and content of medication instructions.14 ,15 Final wording and phrasing choices were determined based on suggestions that were endorsed by the majority of discussion groups.
Results
A total of 40 participants were enrolled in the study across four discussion groups (n=20 per location). Discussion groups were held from December 2012 to April 2013; two discussion groups were conducted at each of the study locations. Table 1 describes the sociodemographic and health characteristics of the study sample. Overall, participants varied greatly in terms of their educational attainment, age and income. The mean age of participants was 46 (range 21–67) and the majority were female (60%) with low income. On an average, participants took four prescription medications and reported having two chronic health conditions. Almost all participants (92.5%) had taken a non-pill form, short term, as needed, escalating or tapered dose medication in the previous year; half of them had used three or more of these types of medications. One-third of participants (33%) were classified as having inadequate literacy skills; according to REALM criteria, these participants were reading on less than a 9th grade level. The participants’ sociodemographic attributes, health characteristics and literacy skills were similar between the study locations.
Characteristics of study sample
Discussion group findings
Results from the discussion groups indicated that most of the standard instructions could be enhanced to promote patient's understanding. Overall, participants found most of the standard instructions to be unnecessarily confusing and complicated. One participant summarised these feelings by stating: “You need medication just to use the label.” The findings are displayed by topic area below. Table 2 displays examples of standard instructions and improved instructions developed based on group discussions.
Standard and Improved Rx Instructions
Use of terminology
Participants suggested using clear, concise wording and phrasing whenever possible. Certain words, such as ‘subcutaneously’ and ‘inhalation,’ were viewed as unnecessarily difficult, and often confusing, by many participants. One participant in Chicago explained: “When you read ‘subcutaneously’ you think, what in the world are they talking about?” Potential alternatives were discussed; most of the participants ultimately supported using ‘under your skin’ and ‘puff ’, respectively.
Greater disagreement was expressed over measurement terminology for liquid medications. Participants were informed about standards supporting the use of ‘mL’ as a unit of measurement instead of ‘teaspoon’ or ‘teaspoonful’; these recommendations were developed due to dosing errors that commonly occur when patients or caregivers use household teaspoons, which are often highly variable, to dose medications.16 ,17 Some participants believed that mL should be used on the label due to these dosing concerns. One participant summarised this point of view by stating: “If you don't want us to use a teaspoon, then don't put that on the label.” In contrast, other participants were against using mL as it was an unfamiliar term. One participant stated: “5mL? I have no idea what that is.” There was concern that using this unfamiliar term might lead to even greater dosing errors. Some participants suggested using illustrations to support the measurement of liquid medications. They also emphasised the importance of always providing patients or caregivers with the appropriate dosing instruments (ie, cups, syringes) if an unfamiliar term like mL was included on the Rx label.
Presentation of numbers
Consistent with health literacy best practices, improved instructions contained numeric instead of alphanumeric presentations of numbers (ie, 1 vs ‘one’). However, to our knowledge, prior research has not examined how to best present fractions on Rx labels. Fractions may be common, particularly for medications requiring a tapered or escalating dose. Participants were shown various options for half a pill, including 0.5, 1/2, ½ and the word ‘half.’ Participants overwhelmingly preferred ‘half,’ and believed that the fraction and decimal options could cause greater confusion. One participant explained this viewpoint by saying: “Half is universal, ½ could be too small and not everyone will be able to see it.” When asked their preference for one and a half, most participants preferred to have the entire phrase written out as opposed to 1 ½, 1 1/2, 1.5 or 1 and a half for similar reasons.
Understanding when medications should be taken
Two of the improved instructions included information on when medication should be taken (ie, when you are short of breath, if you have pain). Participants supported including this information at the beginning of the instruction and removing the term ‘as needed’ to avoid any confusion. Providing clear information on when medications should be taken upfront helped orient participants to the medication-taking process and provided clear guidance on how to link symptoms to the need to take medication. During these discussions, participants also reported the need to describe symptoms that would prompt medication use in the clearest manner possible. For example, while most of the participants understood the phrase ‘short of breath,’ some questioned whether another phrase, such as ‘difficulty breathing’ or ‘trouble breathing,’ should be used instead. Others disliked these alternative phrases as they felt having asthma necessarily meant you had ‘trouble breathing,’ whereas ‘shortness of breath’ occurred on isolated occasions. Overall, ‘short of breath’ was endorsed by the majority of participants.
Timing and duration of use
Overall, participants supported the UMS framework and tying medication use to specific time periods. When medications required taking doses for a specific period of time (ie, for 7 days), participants suggested placing this information at the beginning of the instruction to better orient patients. For short-term medications such as antibiotics, participants suggested adding the phrase ‘until all pills have been taken’ to the end of the instruction. This phrase was preferred over other suggestions, such as ‘until pills are gone’ or ‘until the bottle is empty.’ For pain relievers with a maximum daily dosage, participants approved of adding the statement ‘Do not take more than 6 pills in 24 h.’ Many participants believed there was a benefit to adding the word ‘warning’ or ‘caution’ before this phrase to highlight the importance of the message; between these two terms, ‘warning’ was preferred by the majority of participants. Overall, participants reported wanting very specific, detailed information on how to take medication; discussions also highlighted the need to choose optimal phrasing and wording to promote ease of understanding.
Need for external aids and counselling
While discussion groups were designed to focus on improvements that could be made to Rx labels, participants frequently expressed a need for greater counselling and education to support safe medication use, especially for challenging-to-use medications. This was particularly the case for tapered dose medications (see table 2). While the study team attempted to simplify instructions for these drugs, participants strongly felt that external aids and counselling were necessary to properly educate patients on their use. When viewing the length and complexity of written instructions for a tapered dose medication, one participant commented: “People will feel overwhelmed and get a headache if all this information is on the label.” In terms of external aids, participants thought that a calendar-based tool would support safe and appropriate use; they also approved of blister packs. Otherwise, as one participant noted, “By the time you get to day 10, you don't remember what day you started the medicine.” Overall, discussions highlighted the need to provide additional support to patients to promote safe and consistent medication use; improving labelling alone was seen as an insufficient means of improving medication understanding and use.
General medication-related challenges
It is also important to note that certain key points arose that were not specific to any of the proposed medication instructions. Specifically, participants clearly and repeatedly stated the general and well-known difficulties of consistently remembering to take chronic medications. Moreover, participants expressed their dissatisfaction with long wait times and brief interactions with physicians and pharmacists. Participants routinely voiced their opinion that “Everyone should have the right to talk to the pharmacist” but noted that not all patients were afforded that opportunity. Participants saw the lack of communication between providers and patients as barriers to understanding and using medications properly. These points mirrored other discussions on the need to consider avenues beyond medication labelling to promote safe and appropriate prescription drug use.
Discussion
The instructions developed in this study are for some of the most commonly used medications today, including insulin, antibiotics, corticosteroids and antidepressants.18 Developing easy-to-understand instructions for these medications is essential, as Rx labels are often the most tangible, frequently used source of information for patients on proper medication use.10 Our study findings can help advance the science of optimising drug labelling practices from a patient's perspective.
Our study was conducted among a group of participants from two distinct geographic locations; participants varied in terms of age, education and income. Yet, there was a high level of agreement on how to best phrase Rx instructions to promote comprehension. Many health literacy best practices for drug labelling, such as using simpler wording and explicit directions, were readily supported by participants. This is consistent with prior studies, including many conducted by members of our research team.9 ,19 ,20 Some of the most valuable, novel findings from the discussion groups were related to presenting numerical information on Rx labels, selecting measurement terminology for liquid drugs and the need for external aids to support tapered dosing. In terms of presenting fractions, participant feedback suggested that writing out the fraction (ie, half or one and a half) was superior to other formats (ie, ½, 1/2 or 0.5). In general, health literacy research suggests that numeric presentations of numbers are superior to alphanumeric; this finding is therefore unique and somewhat in contrast to accepted health literacy practices.10 ,21 Regarding terminology for measuring liquid medications, many participants were uncomfortable with mL as a unit of measurement, mostly due to a lack of familiarity with the term. This could be one underlying root cause of misunderstanding of liquid medication instructions; previous research has consistently shown that patients have difficulty measuring liquid medications correctly.22 To further complicate the problem, evidence also suggests that Rx instructions and accompanying measurement devices (ie, syringes, cups) often utilise different units of measurement, potentially leading to greater confusion for the patients.23 Participant feedback suggests that if mL is used on Rx labels, additional illustrations and accompanying measurement devices with the same unit of measurement would be necessary to promote safe and appropriate dosing. Additional research will be needed to develop, refine and test tools and counselling strategies to support patient's understanding and use of these medications.
Finally, the discussion groups underscored the necessity of external aids and counselling for tapered dose medications. Their comments about the unmet need for medication counselling and barriers to medication comprehension at the pharmacy are consistent with previous studies.24 ,25 This suggests that policy efforts, for example, legislation requiring patient counselling at pharmacies, have either not been implemented adequately or have not necessarily led to improved patient education.26 Continued efforts are needed to promote patient counselling and support of medication use; innovations in technology and more supportive reimbursement policies may assist in this process.
By incorporating the UMS, health literacy principles and patients' perspectives, our team created a set of Rx instructions that can be adopted by prescribers and pharmacies to support patient's understanding and use of prescribed drugs. This expansion addresses one of the major limitations of the UMS, making it a more universal, widely adoptable framework. While additional barriers exist—such as the need to update labelling software and to educate prescribers and pharmacists on the importance of health literacy-informed labelling—we believe our current efforts are an instrumental first step towards promoting the adoption of the UMS. This is particularly timely and relevant, as the California State Board of Pharmacy recently passed regulations requiring pharmacies throughout the state to generate standardised Rx labels that incorporate health literacy principles; regulations specifically referenced using the UMS as a best practice.27 A number of other states are now considering similar legislation. The Rx instructions developed through this study can help support these initiatives, promoting the adoption and use of patient-centred drug labelling.
This study has limitations that should be noted. It relies on a relatively small sample of English-speaking adults. Additional research will be needed to replicate findings and develop Rx instructions in other languages, which we have carried out with chronic pill-form medications.28 While participants were recruited from two geographically distinct locations, convenience sampling was used, which may limit the generalisability of our findings. Finally, this study focused on the development of Rx instructions. Future comprehension testing is planned to evaluate the proposed Rx instructions against standard instructions using hypothetical medications. If instructions are found to promote understanding, an actual use assessment would be necessary to demonstrate the efficacy.
In conclusion, through this project, our team developed a set of patient-centred, health-literacy informed Rx instructions for use with non-pill form, short term, as needed, tapered and escalating dose medications. These Rx instructions are an essential next step to promoting comprehensive patient-centred labelling in the USA. Given the building evidence in support of the UMS framework, the California State Board of Pharmacy recommended its use to pharmacy practices to fulfil recent regulations promoting patient-centred labelling.27 Others are now considering similar requirements and efforts have been launched across a number of states to advocate for improved Rx labelling. If found to support comprehension, our Rx instructions could provide valuable guidance to legislators, regulatory agencies, prescribers and pharmacists on how to label non-pill form, as needed, short term, tapered and escalating dose medications.
References
Footnotes
-
Contributors SCB, US, MSW, DSr and AHC are study investigators and participated in the design and conduct of the study and the analysis and interpretation of findings. AR and AL are research coordinators who were responsible for data collection, analysis and manuscript development. GM is the programme officer for this project and provided input on manuscript development and interpretation of findings; he also provided guidance on the overall study design.
-
Funding This study was funded by the California HealthCare Foundation.
-
Competing interests None.
-
Ethics approval Northwestern University Institutional Review Board (IRB), University of California at San Francisco IRB.
-
Provenance and peer review Not commissioned; externally peer reviewed.
-
Data sharing statement No additional data are available.