Article Text

Abstract
Objectives To demonstrate the survival benefit from sustained virological response (SVR) in a safety net hospital population with limited resources for hepatitis C virus (HCV) therapy.
Design and setting We conducted a retrospective study at an urban safety net hospital in the USA.
Participants and intervention 242 patients receiving standard HCV therapy between 2001 and 2006.
Primary and secondary outcome measures Response rates, including SVR, were recorded for each patient. Univariate and multivariate analyses were performed to identify predictors of SVR and 5-year survival.
Results A total of 242 eligible patients were treated. Treatment was completed in 197 (81%) patients, with 43 patients discontinuing therapy early—32 due to adverse events and 11 due to non-compliance. Complications on treatment were frequent, including three deaths. SVR was achieved in 83 patients (34%). On multivariate analysis, independent predictors of a decreased likelihood of achieving SVR included African–American race (OR 0.20, 95% CI 0.07 to 0.54), genotype 1 HCV infection (OR 0.25, 95% CI 0.13 to 0.50) and the presence of cirrhosis (OR 0.26, 95% CI 0.12 to 0.58). Survival was 98% in those achieving SVR (median follow-up 72 months) and 71% in non-responders and those discontinuing therapy (n=91, median known follow-up 65 and 36 months, respectively). On multivariate analysis, the only independent predictor of improved survival was SVR (HR 0.12, 95% CI 0.03 to 0.52). Both cirrhosis and hypoalbuminaemia were independent predictors of increased mortality.
Conclusions Treatment before histological cirrhosis develops, in combination with careful selection, may improve long-term outcomes without compromising other healthcare endeavours in safety net hospitals and areas with financial limitations.
- INFECTIOUS DISEASES
- HEALTH ECONOMICS
- PUBLIC HEALTH
This is an Open Access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 3.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/3.0/
Statistics from Altmetric.com
Article summary
Article focus
-
Chronic hepatitis C is common in urban populations with limited financial resources.
-
Individual patient characteristics can limit success.
Key messages
-
Selection process identifies candidates with greater likelihood of better compliance.
-
Survival benefit from successful treatment can be achieved with less expensive, older therapies.
Strengths and limitations of this study
-
Clear demonstration of long-term survival benefit in a high-risk population.
-
Single institution retrospective study.
Introduction
For many years, standard of care for patients with chronic hepatitis C virus (HCV) included treatment with pegylated interferon and ribavirin1 based on evidence from randomised controlled trials (RCTs).2–4 Conditions in RCTs are often very different than those of clinical practice. Given this potential discrepancy between an intervention's efficacy (the effect under carefully controlled conditions) and effectiveness (the effect when implemented in real-world settings), there is increasing emphasis on comparative effectiveness research to improve delivery of care.5 ,6 Accordingly, the National Institute of Health recently included the evaluation of real-world outcomes of healthcare interventions in liver disease as a priority area for future research.
Prior studies evaluating HCV therapy have primarily included well-insured, Caucasian patients followed in academic centres. However, HCV therapy is less well described among the underinsured, urban, minority patients. Some have concluded that current HCV therapy may be ineffective for these patients, warranting new strategies.7 However, we hypothesised that improved HCV outcomes are possible among this difficult-to-treat population with the aid of careful patient selection.
Screening for infection in the birth cohort with the highest prevalence of chronic HCV infection, that is, those born between 1945 and 1965, was controversial. While the Centers for Disease Control and Prevention have made a strong recommendation for this approach,8 the USA Public Service Task Force (USPSTF) was initially less enthusiastic (Grade C).9 However, USPSTF now supports screening in those at high risk (Grade B), previously considered optional, and also birth cohort screening.10 The primary aim of our study was to report the long-term benefit of HCV therapy in an American urban population with a high proportion of difficult-to-treat patients who were followed in a safety net hospital.
Methods
Study population
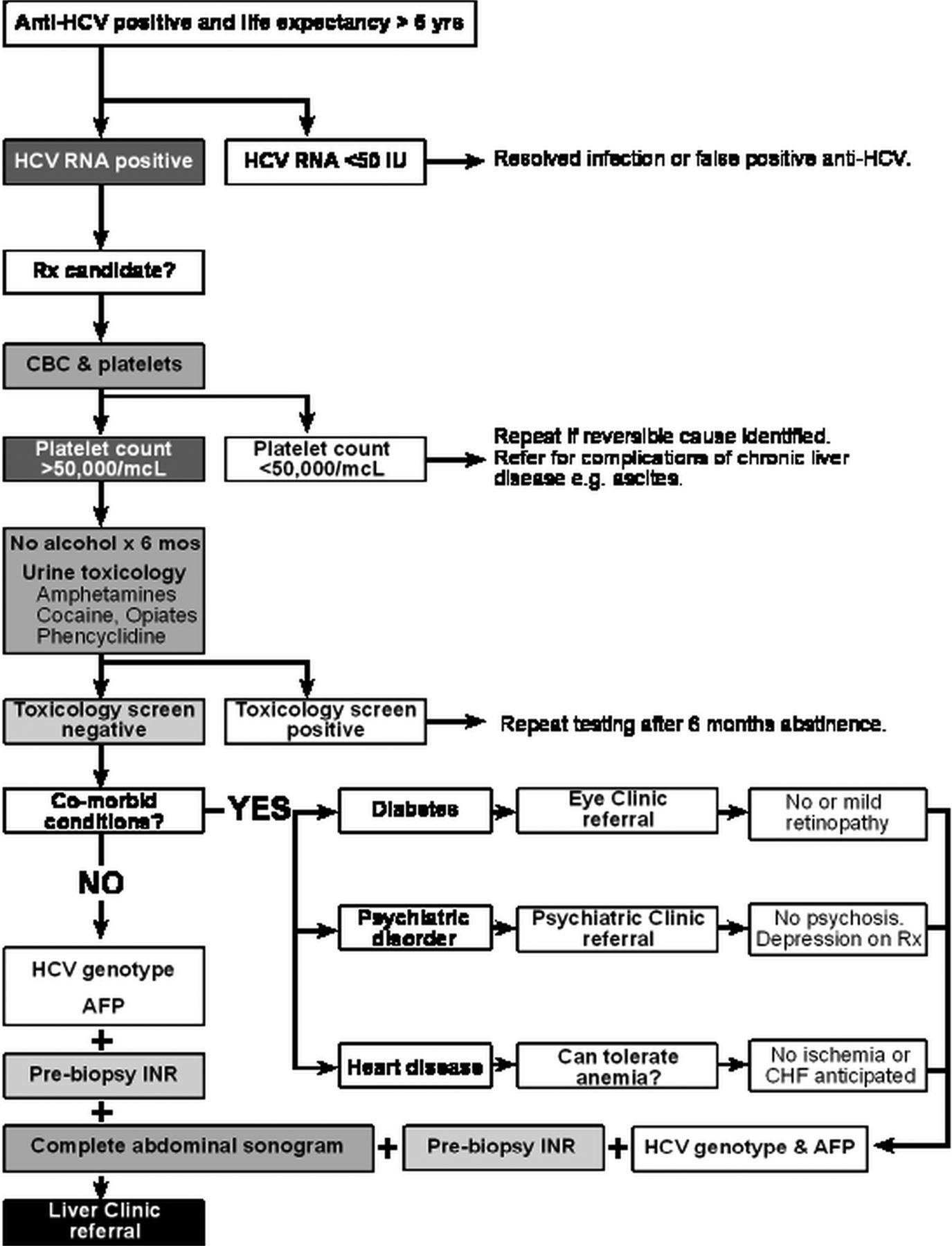
We conducted a chart review of all patients initiated on HCV treatment between November 2001 and October 2006. Eligible patients were seen in the faculty attending supervised Liver Clinic at Parkland Health and Hospital System (PHHS). Clinic patients were evaluated initially by a member of the clinic nursing staff followed by Gastroenterology trainees and/or Internal Medicine residents, under the supervision of Hepatology faculty members (n=6). After patients had fulfilled a list of basic requirements (figure 1), the final decision to initiate treatment for any individual patient was made by the supervising attending physician based on his/her assessment of the patient's candidacy.

Screening algorithm.
Once the treatment decision was made, demographics for all patients were entered into an electronic file maintained by the clinic nursing staff. The electronic file was used for this retrospective medical record review. The clinic nursing staff also saw all patients to provide instructions on medications as well as on interim follow-up visits and offered telephone advice. Patients were regularly seen in the Liver Clinic while on treatment and followed until sustained virological response (SVR) or discontinuation, at which time they returned to primary care or remained in the Liver Clinic, depending on the complications of liver disease experienced. Long-term follow-up was accomplished using the Social Security Death Index (prior to the regulatory 10-year embargo on information and removal of records from the State of Texas) and the combined electronic medical records of PHHS and the University Hospitals of UT Southwestern.
Treatment regimen
On the basis of consensus guidelines, patients were treated with weekly pegylated interferon α-2b 1.5 µg/kg and daily ribavirin 800–1200 mg. A combination of growth factors and dose reductions were used for patients with haemoglobin <10 g/dL, granulocyte count <500/µL or platelet counts <50 000/µL according to a standard protocol. The intended duration of therapy for genotypes 1, 4 and 6 was 48 weeks, and the intended duration of therapy for genotypes 2 and 3 was 24 weeks. All patients were scheduled to be seen at regular intervals during treatment, as deemed necessary based on treatment tolerance, and were followed for an additional 24 weeks after completion of therapy to determine the presence or absence of SVR.
Data collection
The patient demographics, clinical history, laboratory data and imaging results were obtained through review of computerised and paper medical records. Demographics, date of HCV therapy initiation, medication starting doses, medication dose reductions, use of growth factors, date of treatment discontinuation and response rates while on therapy were documented. Response rates included early virological response, end-of-treatment response and/or SVR rates. We also recorded complication rates, including any hospitalisations and/or deaths. Laboratory data recorded included HCV genotype, baseline HCV viral load, white cell count, haemoglobin, platelet count, creatinine, aspartate aminotransferase, alanine aminotransferase, bilirubin, albumin, international normalised ratio and α fetoprotein. Imaging and liver biopsy data were reviewed to determine the presence or absence of cirrhosis. The presence of cirrhosis was based on histology or imaging showing a cirrhotic appearing liver with associated signs of portal hypertension including splenomegaly, varices or thrombocytopenia. Date of death for patients was ascertained using the PHHS electronic medical record and Social Security Death Files.
Statistical analysis
For continuous variables, we summarised the data by mean and SD, and compared groups using a two-sample Student's t test. For categorical variables, we computed percentages and compared groups using Fisher's exact test. We used a multivariate logistic regression model, with stepwise variable selection, to determine predictors for SVR. Statistical significance was defined as a p value <0.05 on univariate and multivariate analyses. All analyses were performed using SAS V.9.2 (SAS Institute, Cary, North Carolina, USA).
Results
Eligibility for therapy
The study participants comprised all patients in the Liver Clinic meeting selection criteria and undergoing antiviral treatment for chronic HCV infection between November 2001 and October 2006. Every patient with chronic HCV being followed in the Liver Clinic or newly referred by a primary care provider was considered for treatment once pegylated interferon was approved by the Pharmacy and Therapeutics Committee in 2001. Between 2001 and 2006, 1966 patients accounted for 2370 new referrals; of these 126 received at least one dose of pegylated interferon and ribavirin. The remaining patients never became eligible or were deemed unsuitable. In an electronic look-back over new patient referrals from a 2-year period (2004 and 2005, n=989), 366 referrals (37%) were for patients ineligible for clinic appointments at that time (see algorithm, figure 1). Clinic appointments were offered to 597 individuals (623 referrals), of whom 389 attended the clinic at least once (ie, 35% did not keep the clinic appointment). A total of 57 individuals were started on treatment (15% of those keeping at least one appointment).
Common reasons for initial exclusion after electronic medical record review, that followed referral from a primary care provider, included severe thrombocytopenia (defined as platelet count <50 000/µL), uncontrolled diabetes (defined as HbA1C>9%), uncontrolled depression and positive urine toxicology screen (figure 1). Reasons for not initiating patients on therapy after physician evaluation in the clinic included comorbid conditions (autoimmune disease, heart disease, lung disease and psychiatric disease), continued alcohol consumption, early-stage histology and/or socioeconomic barriers that would prevent regular follow-up during treatment.
Patient characteristics
Demographic and clinical characteristics of the study population are shown in table 1 and the online supplemental table. The study participants included 166 (68%) patients with genotype 1 infection, 64 (27%) with genotype 2 or 3 and 12 (5%) patients with other genotypes. The median age of the patients was 48 years (range 20–68 years), 72% were in the birth cohort 1945–1965 and 51% (n=123) were men. The patients were racially and ethnically diverse with 31% African-American, 14% Hispanic and 47% non-Hispanic white. Common comorbid conditions included depression or other psychiatric disease (74 patients, 31%), hypertension (68 patients, 28%) and diabetes mellitus (40 patients, 17%). Comorbid conditions potentially associated with decreased response rates included morbid obesity (body mass index (BMI)>40; 22 patients, 9%) and HIV (7 patients, 3%). Cirrhosis was present histologically in 31%, 36 patients biopsied before treatment initiation and another 40 patients by clinical criteria.
Study population characteristics*
Newly referred patients (n=126 patients, with 164 separate referrals) were largely similar to patients entering the clinic through other processes (see online supplemental table). The latter group included patients seen in the clinic while meeting selection criteria, being followed awaiting formulary approval and those referred after an inpatient hospitalisation. The significant differences were the higher prevalence of diabetes (p=0.003) and the higher viral load (p=0.02) in the newly referred patients. The referral patient population had trends towards more African-Americans, higher BMI and fewer deaths in follow-up.
Treatment response
Therapy was completed in 197 (81%) patients, with 43 patients discontinuing treatment prematurely (figure 2). Therapy was discontinued for adverse events in 32 patients including three deaths and another 11 patients were non-compliant with the follow-up appointments. There was a trend towards higher treatment discontinuation rates for genotype 1 than genotype 2/3 patients but this did not reach statistical significance (p=0.16). Of the seven patients with HIV (6 Caucasian and genotype 1, 1 Hispanic and genotype 3), four discontinued therapy after side effects, none achieved SVR.

Results of patient evaluation and treatment. RNA negative=hepatitis C virus RNA negative at last measurement, on treatment (n=19) or less than 6 months off-treatment (n=6).
Overall, SVR was achieved in 83 (34%) patients, including 39 (24%) of those with genotype 1 and 39 (61%) with genotype 2/3 infection (p<0.001). There was no significant difference in rates of SVR between patients newly referred to the clinic (46/126, 37%) and patients in the clinic awaiting formulary approval or referred after an inpatient hospitalisation (36/116, 32%). Of note, 10 of 22 patients with morbid obesity (BMI range 41–50) were treated successfully; seven had genotype 1 infection, two of whom were African-American women.
SVR was obtained in only 11% of African-American patients, compared with 44% of non-Hispanic whites (p<0.001) and 38% of Hispanic patients (p=0.001). This difference in SVR rates was primarily seen among those with genotype 1 infection. SVR was achieved in only 7% of African-Americans with genotype 1 infection, compared with 40% of non-Hispanic whites (p<0.001) and 24% Hispanics (p=0.03). SVR rates did not significantly differ by race/ethnicity among patients with genotype 2/3 infection. African-Americans with genotype 2/3 infection had SVR in 60% of cases, compared with 55% of non-Hispanic whites (p=0.82) and 78% Hispanics (p=0.48).
Cirrhosis was associated with significantly lower rates of SVR, only 10 (13%) cirrhotic patients achieved SVR. Among genotype 1 patients, SVR was achieved in 34 (31%) of 108 patients without cirrhosis compared with only 5 (9%) of 57 patient with cirrhosis. Similarly, SVR rates were significantly higher among non-cirrhotic genotype 2/3 patients than those with cirrhosis (70% vs 35%, p=0.01).
In small numbers of patients (n=14), having three or more comorbid conditions reduced the likelihood of achieving SVR (3/14, 21%). Patients with diabetes were less likely to respond favourably (7/40, 18% SVR) as were those with hypertension (15/68, 22% SVR). Psychiatric disease (depression or schizophrenia) did not affect SVR rates (26/66, 39%).
Negative predictors of SVR on univariate analysis included HCV genotype 1 infection (p<0.001), African-American race (p<0.001), presence of cirrhosis (p=0.001), thrombocytopenia (p=0.005) and diabetes (p=0.02). Neither Hispanic ethnicity nor anaemia (Hb <12 g/dL) was a significant predictor of response. On multivariate analysis (table 2), independent predictors of failure to achieve SVR included African–American race (OR 0.20, 95% CI 0.07 to 0.54), genotype 1 HCV infection (OR 0.25, 95% CI 0.13 to 0.50) and the presence of cirrhosis (OR 0.26, 95% CI 0.12 to 0.58). These three factors were highly predictive of failure to achieve SVR, with a c-statistic of 0.77 (data not shown).
Factors predicting sustained virological response (SVR)*
From long-term follow-up after the start of treatment, we found that a total of 43 (18%) patients died, including 34 (20%) with genotype 1 infection and 9 (14%) with genotype 2/3. Survival was significantly more likely among patients who achieved SVR than non-responders (98% vs 71%, p<0.001) and those who discontinued therapy (98% vs 71%, p<0.001). Of the patients with cirrhosis achieving SVR, 90% (9/10) were presumed or known to be alive at least 5 years later. In contrast, 28 of the 43 patients known to have died had cirrhosis at the time of treatment (65%). Both diabetes and hypertension were associated with an increased risk of dying. Complete follow-up and survival analysis are shown in figure 3 and table 3. On multivariate analysis, cirrhosis and hypoalbuminaemia independently increased mortality, whereas SVR decreased mortality.
Factors predicting mortality

{kind=link}
{kind=link}
{kind=link}
Kaplan-Meier survival plot.
Adverse effects
As summarised above, 43 (18%) patients discontinued treatment prior to completion including 32 patients for adverse events. Of the patients discontinued for adverse events, 26 required hospitalisation. The most common reasons for hospitalisation included infection (n=13), severe cytopenias (n=4), volume depletion (n=3) and chest pain (n=2). There were two patients whose therapy was discontinued after they developed hepatocellular carcinoma. Three (1%) patients died during therapy. One patient, whose course was complicated by depression and another, whose course was complicated by infection (pneumonia and tooth abscess), died out of the hospital from unknown causes. The third patient had gastrointestinal bleeding in the setting of non-steroidal anti-inflammatory drug use and died after developing streptococcal bacteraemia and acute renal failure.
Discussion
While we found that SVR was achieved in only one-third of treated patients, the lower rates among African-American patients and those with underlying cirrhosis explain most of the difference. In addition, patients in safety net hospitals have multiple barriers to therapy initiation, with only a small minority being treatment eligible by the selection criteria used. In our cohort, less than 10% of patients referred for HCV were initiated on treatment. Finally, HCV therapy has potentially severe adverse effects and careful patient selection is crucial. Our study, therefore, highlights several concepts applicable to current-day HCV practice despite the approval of telaprevir and boceprevir for patients with genotype 1 infection.11 ,12 In addition, our findings support early screening and detection of chronic HCV so that therapy can be started before progression to cirrhosis.
HCV infection is particularly common among patients followed in safety net hospitals where resources are limited, making this an important population to study.13 ,14 Patients followed in safety net hospitals tend to be quite different from most clinical trial patients. Safety net hospitals have higher proportions of racial/ethnic minority patients, as well as higher rates of comorbid illnesses and socioeconomic barriers to care.15 Compared with a representative RCT of HCV treatment,2 our population was older, more obese, had a higher proportion of African-Americans and more advanced liver disease at presentation. In a prior study from a safety net hospital in New York City, only 14% of genotype 1 patients achieved SVR, with significantly lower rates among minority patients.7 Our ability to achieve higher SVR rates than that reported by Feuerstadt and colleagues may be related to differences in treatment eligibility. Although both protocols selected for suitable medical candidates, our protocol also selected more compliant patients. Whereas nearly 26% of patients in the study by Feuerstadt and colleagues were non-compliant with clinic visits, this led to therapy discontinuation in only 5% of patients in our study (p<0.001). The importance of adherence cannot be underestimated, with both early and SVRs being dependent on this single factor.16 Compliance will continue to be important in future therapy until regimens are simple and consist of long half-life oral medications with minimal side effects.
Our study has several limitations. It was performed in a single large safety net hospital and may not be generalisable to other practice settings. Not all patients underwent liver biopsy prior to HCV treatment so the presence or absence of cirrhosis was also determined by imaging, which may not be as accurate. However, we believe that the limitations of this study are outweighed by its notable strengths including the size of our cohort, the unique patient population and the length of follow-up.
In conclusion, our study highlights several important lessons to remember even when using new protease inhibitor therapy. Multiple challenges, including socioeconomic barriers precluding compliance and comorbid illnesses, make only a small minority of patients followed in safety net hospitals eligible for HCV therapy. SVR occurs in only one-third of patients, with even lower rates among minority patients and those with underlying cirrhosis. Both early detection and careful patient selection remains crucial, given that severe adverse effects are seen in nearly 15% of patients. Data from long-term benefit studies, such as ours, as well as real-world effectiveness should be taken into account more than efficacy data from clinical trials, when weighing the risks and benefits of screening for chronic HCV and starting HCV therapy among patients followed in safety net hospitals in clinical practice.17
References
Supplementary materials
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
Files in this Data Supplement:
- Data supplement 1 - Online supplement
Footnotes
AGS and TDD equal first authors.
-
Contributors AGS participated in analysis and interpretation of the data; drafting of the manuscript; critical revision of the manuscript for important intellectual content. TDD and JAC participated in study design; acquisition of the data; review of clinical records; analysis and interpretation of the data; drafting of the manuscript; critical revision of the manuscript for important intellectual content. PFM participated in study design; critical revision of the manuscript for important intellectual content. SA participated in critical revision of the manuscript for important intellectual content. SZ participated in analysis and interpretation of the data; critical revision of the manuscript for important intellectual content.
-
Funding This project was supported in part by grants KL2 RR024983-04 and the ACG Junior Faculty Development Award.
-
Competing interests None.
-
Ethics approval University of Texas Southwestern Medical Center Institutional Review Board.
-
Provenance and peer review Not commissioned; externally peer reviewed.
-
Data sharing statement Extra data can be accessed via the Dryad data repository at http://datadryad.org/ with the doi:10.5061/dryad.qc57j.