Article Text

Abstract
Objective Dabigatran was recently approved for anticoagulation in patients with atrial fibrillation (AF); data regarding real-world use, comparative effectiveness and safety are sparse.
Design Pharmacoepidemiological cohort study.
Methods/settings From nationwide registers, we identified patients with an in-hospital or outpatient-clinic AF diagnosis who claimed a prescription of dabigatran 110 or 150 mg, or vitamin K antagonist (VKA), between 22 August and 31 December 2011. HRs of thromboembolic events (ischaemic stroke, transitory ischaemic attack and peripheral artery embolism) and bleedings were estimated using Cox regression analyses in all patients and stratified by previous VKA use.
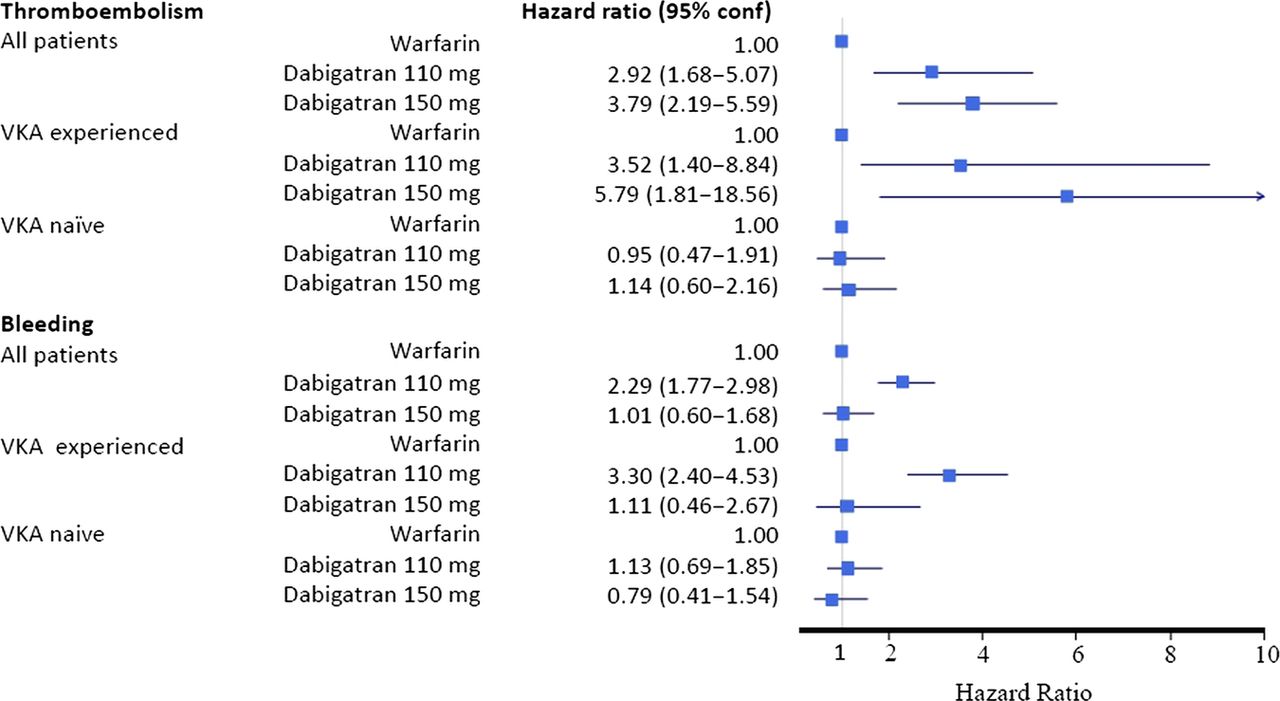
Results Overall, 1612 (3.1%) and 1114 (2.1%) patients claimed a prescription of dabigatran 110 and 150 mg, and 49640 (94.8%) of VKA. Patients treated with dabigatran 150 mg were younger with less comorbidity than those treated with dabigatran 110 mg and VKA, as were VKA naïve patients compared with previous VKA users. Recommendations set by the European Medicine Agency (EMA) for dabigatran were met in 90.3% and 55.5% of patients treated with 110 and 150 mg. Patients treated with 150 mg dabigatran, who did not fulfil the recommendations by EMA, were >80 years, patients with liver or kidney disease, patients with previous bleeding. Compared with VKA, the thromboembolic risk associated with dabigatran 110 and 150 mg was HR 3.52 (1.40 to 8.84) and 5.79 (1.81 to 18.56) in previous VKA users, and HR 0.95(0.47 to 1.91) and 1.14(0.60 to 2.16) in VKA naïve patients. Bleeding risk was increased in previous VKA users receiving dabigatran 110 mg, but not in patients with 150 mg dabigatran, nor in the VKA naïve users.
Conclusions Deviations from the recommended use of dabigatran were frequent among patients treated with 150 mg. With cautious interpretation, dabigatran use in VKA naïve patients seems safe. Increased risk of thromboembolism and bleeding with dabigatran among previous VKA users was unexpected and may reflect patient selection and ‘drug switching’ practices.
This is an open-access article distributed under the terms of the Creative Commons Attribution Non-commercial License, which permits use, distribution, and reproduction in any medium, provided the original work is properly cited, the use is non commercial and is otherwise in compliance with the license. See: http://creativecommons.org/licenses/by-nc/3.0/ and http://creativecommons.org/licenses/by-nc/3.0/legalcode
Statistics from Altmetric.com
Article summary
Article focus
-
To describe dabigatran use in atrial fibrillation (AF) patients and compare it with vitamin K antagonist (VKA) use.
-
To describe if dabigatran is prescribed according to the recommendations set by authorities.
-
To estimate initial risk of thrombosis and bleedings related to dabigatran and VKA use among all patients, and stratified by previous use of VKA.
Key messages
-
Dabigatran was prescribed in approximately 5% of AF patients with oral anticoagulation during the initial 4 months after approval.
-
Recommendations set by the European Medicine Agency for dabigatran were met in 90.3% and 55.5% of patients treated with 110 and 150 mg, respectively.
-
Compared with VKA, the thromboembolic risk associated with dabigatran 110 and 150 mg was higher in previous VKA users, but comparable in VKA naive patients. Bleeding risk was increased in previous VKA users (D110 mg). Increased risk of thromboembolism and bleeding with dabigatran among previous VKA users may reflect patient selection and ‘drug switching’ practices.
Strengths and limitations of this study
-
The main strength is the nationwide complete dataset of unselected AF patients and the use of validated pharmacoepidemiological methods.
-
The main limitation is the short follow-up time.
Introduction
Stroke is a serious complication of atrial fibrillation (AF), and prevention with antithrombotic medication has high priority.1 ,2 Until recently, vitamin K antagonists (VKA) have been the drug of first choice in high-risk patients with AF,3 but food and drug interactions and the need for frequent monitoring within a narrow therapeutic range makes VKA unattractive to many patients.4
The novel oral anticoagulant dabigatran etexilate has been compared with VKA in patients with non-valvular AF in a large phase 3 randomised trial; it has been shown to be non-inferior to VKA with a comparable or lower risk of strokes, and with a more favourable side-effect profile concerning serious bleedings.4 Dabigatran has fewer interactions with food and drugs than VKA and does not need monitoring of its anticoagulant effect.5 Moreover, dabigatran 150 mg twice daily was superior to VKA in preventing stroke, with an additional overall reduction of cardiovascular mortality, and without increasing the risk of major bleeding.4 In patients with a clear indication for oral anticoagulation and without contraindications for therapy, the 2012 focused update of the European Society of Cardiology AF guidelines recommends one of the novel anticoagulants (dabigatran, rivaroxaban or apixaban) as a first-line choice of anticoagulation.2 ,6 ,7
Dabigatran was the first drug to be approved by the authorities for patients with non-valvular AF; however, the approval was followed by several concerns including case reports of serious bleedings8 ,9 as well as concerns about poor adherence to therapy.10 Consequently, the Food and Drug Administration (FDA) in the USA, and European Medicine Agency (EMA) brought a safety announcement of serious bleedings.11 ,12 EMA has approved the use of dabigatran in AF patients if one of the following risk factors are present: previous stroke, transient ischaemic attack, age ≥75 years, left-ventricular ejection fraction <40% or age ≥65 years with one of the following: diabetes, coronary heart disease or hypertension. A dose of 150 mg twice daily is recommended unless the patients are ≥80 years, or with an increased risk of bleeding where a dose of 110 mg twice daily is preferred/should be considered.2 The 2012 European Society of Cardiology guidelines on AF management state that dabigatran 150 mg twice daily is the default dose, with the 110 mg twice daily dose being recommended in those aged ≥80 years, with high bleeding risk (HAS-BLED ≥3) and concomitant interacting drugs (eg, verapamil).2
Until now, only preliminary real-life postapproval data have reported on the use of dabigatran.13–15 The purpose of this nationwide cohort study was to describe initial postapproval use, comparative effectiveness and safety of treatment with dabigatran 110 and 150 mg twice daily among patients with AF, compared with those with VKA, during the initial 4 months after approval.
Methods
Data sources
Nationwide administrative registers were linked on an individual level. For this study, we used: (1) The Danish National Patient Register, which holds information on all admissions to Danish hospitals since 1978 with one primary and, if appropriate, one or more secondary diagnoses coded according to the International Classification of Diseases (ICD) 8 and 10. (2) The National Prescription Register holds information on all prescriptions dispensed in Danish pharmacies since 1995 (coded according to the Anatomical Therapeutic Chemical (ATC) classification system), including information on the date of dispensation, strength and number of tablets dispensed. All pharmacies are required by Danish legislation to provide information that ensures complete and accurate registration.16 ,17 (3) The Civil Register holds information of vital status of all citizens.
Study population
We identified all Danish residents registered with a diagnosis of AF (ICD-10 code I48) between 1 January 1995 and 31 December 2011 by the Danish National Patient Register (see online supplementary figure S1). All AF patients admitted to the hospital with AF, managed for AF in an outpatient clinic/ambulatory or seen at an emergency department contact for AF were eligible for the study.
Warfarin and dabigatran therapy
Patients with a prescription claim of VKA (ATC B01AA03) or dabigatran (ATC B01AE07) between 22 August and 31 December 2011 were included. According to their first prescription claim in this period, patients were stratified in three groups: VKA, dabigatran 110 mg twice daily and dabigatran 150 mg twice daily. Prescription claims of VKA from 0 to 180 days prior to baseline stratification were registered and classified as previous VKA therapy. Furthermore, patients were stratified according to previous use of VKA, since risk of bleeding can be higher in VKA naïve patients than in previous VKA users.18 ,19 Use of VKA and dabigatran 110 and 150 mg was included as dichotomous variables since the study period was short.
Comobidities and concomitant medical therapy
Comorbidities of congestive heart failure, hypertension, diabetes mellitus, thromboembolism (ischaemic stroke, transitory ischaemic attack and peripheral artery embolism), vascular disease (myocardial infarction, peripheral artery disease and aortic plaque) and previous bleeding within 180 days prior to index (22 August 2011) were determined, as performed in previous studies.20 ,21 Concomitant medical treatment with digoxin, amiodarone, Class 1C antiarrythmics, sotalol, β-blockers, non-dihydropyridine calcium channel blockers, non-steroidal anti-inflammatory drugs and aspirin was assessed. Criteria for comorbidities, ICD-8 and ICD-10 diagnoses and ATC codes used in the analyses are listed in the online supplementary material, table 1, and have been used in similar analyses previously.18 ,20 CHADS2 (congestive heart failure, hypertension, age ≥75 years, diabetes mellitus, stroke/transient ischaemic attack), CHA2DS2–VASc (ie, CHADS2 and adding vascular disease, age 65–75 and female sex) and HAS-BLED (hypertension, abnormal renal/liver function, stroke, bleeding history or predisposition, labile international normalised ratio(left out due to lack of information, as performed in previous studies), elderly (>65 years), drugs/alcohol concomitantly) scores were calculated. Identification and validation of these scores in similar cohorts have been described previously.18 ,21 ,22
Baseline characteristics
Prescription patterns
Description of the patients prescribed dabigatran 110 and 150 mg twice daily according to recommendations by EMA is presented, as are the baseline differences between previous VKA users and VKA naïve patients.2 ,11
Endpoints: thromboembolism and bleeding
The following two endpoints were assessed: (1) thromboembolism was defined as an admission with a thromboembolic diagnosis (including ischaemic stroke, transitory ischaemic attack and peripheral artery embolism). (2) Bleeding was defined as an admission with a bleeding diagnosis (including cerebral bleedings, bleedings from the respiratory tract, gastrointestinal bleedings and bleedings from the urinary tract). ICD-10 codes used to define the endpoints are listed in online supplementary table S1.
Statistical analyses
Baseline variables for patients on warfarin, dabigatran 110 or 150 mg are presented, referring to the patients’ first exposure group, as are the differences in baseline characteristics in previous VKA users and VKA naïve patients. Logistic regression analysis was used to determine variables associated with dabigatran use. Crude incidence rates per 100 person-years and adjusted HRs of thromboembolism and bleeding were assessed in all patients and in previous VKA users and VKA naïve patients.18 ,19 Patients were considered at risk (exposed) from the first date claiming a prescription of warfarin or dabigatran during the study period between 22 August and 31 December 2011. The study period was chosen since the use of dabigatran was approved by 22 August 2011, and follow-up data obtained from the nationwide registries were only available until 31 December 2011. Patients were censored at the first thromboembolic or bleeding event, at death or at the end of the study period. Adjusted risks associated with dabigatran 110 and 150 mg use were estimated using the Cox proportional-hazards models, with warfarin as reference. The analyses were adjusted for age-groups (<65, 65–74 and ≥75), sex, comorbidity and concomitant medical treatment. The models were tested for the absence of interactions, linearity of continuous variables and fulfilment of the proportional hazard assumption, and found to be valid. Calculations were carried out using the SAS statistical software V.9.2 (SAS Institute, Cary, North Carolina, USA). The study was conducted and reported in accordance with the Strengthening and the Reporting of Observational Studies in Epidemiology recommendations.23
Results
Prescription patterns
Between 22 August and 31 December 2011, a total of 52 366 AF patients claimed a prescription for oral anticoagulation. Of these, 1612 (3.1%) and 1114 (2.1%) patients were treated with dabigatran 110 and 150 mg twice daily, and 49 640 (94.8%) were treated with VKA. Compared with VKA and dabigatran 110 mg twice daily, patients treated with dabigatran 150 mg were younger with less comorbidity, as well as lower CHA2DS2VASc and HAS-BLED scores. Among dabigatran users, 782 (48.5%) in the 110 mg group and 349 (31.3%) in the 150 mg group had previously used VKA (p<0.001). Baseline characteristics are presented in table 1. Independent predictors of dabigatran use are presented in table 2. Of note, 171 patients (34 (2.1%) and 137(12.3%) users of dabigatran 110 and 150 mg, respectively) were initiated on dabigatran without the presence of relevant risk factors, while 481 patients only had one ‘moderate’ risk factor (122 (7.6%) and 137 (32.2%) for dabigatran 110 and 150 mg).
Predictors associated with dabigatran use, results from the logistic regression analysis
Compliance with European recommendations
Among patients treated with dabigatran 110 mg, 90.3% fulfilled the labelled recommendations listed by EMA; this applied to 55.5% among users of 150 mg. Details relating to recommended indications and contraindications are presented in table 3.
Indications and contraindication for dabigatran use
Thromboembolism and bleeding events
Duration of follow-up was 4 months and 9 days. Event rates of thromboembolism and bleedings per 100 patient-years and number of events are shown in figure 1 (for all patients, and in VKA experienced and VKA naïve patients). Related adjusted HRs are shown in figure 2.

Event rates and crude incidence rates per 100 patient years.
{kind=link}
{kind=link}
Adjusted risk of thromboembolic events and bleeding (Cox proportional hazard model).
VKA experienced versus VKA naive
VKA experienced and VKA naive patients differed in baseline characteristics (table 4). Unexpectedly, among all patients, the adjusted risk of thromboembolism was higher among users of dabigatran compared with users of warfarin, but when stratified by previous VKA use, the increased risk of thromboembolism was only seen among previous VKA users (for both 110 and 150 mg doses). Among all patients, the adjusted risk of bleeding was increased among users of dabigatran 110 mg with warfarin as reference. Stratified by previous VKA use, this increased risk only persisted among VKA experienced patients.
Baseline differences between VKA naive and VKA experienced
Discussion
This study describes the use of dabigatran and warfarin in a nationwide cohort of AF patients after approval of dabigatran. Our main findings were as follows: (1) dabigatran was prescribed in approximately 5% of patients with oral anticoagulation; (2) users of dabigatran 150 mg twice daily were younger with less comorbidity than users of VKA and dabigatran 110 mg. A higher proportion of previous VKA users was found in patients treated with dabigatran 110 mg compared with 150 mg; (3) European recommendations for dabigatran use were fulfilled in 90.3% and 55.5% of patients with dabigatran 110 mg and 150 mg, respectively, and (4) the adjusted risk of thromboembolism in VKA naive dabigatran users were comparable to that in VKA (both doses of dabigatran) users, but increased in previous VKA users. The adjusted risk of bleeding was comparable to VKA in VKA naive patients but increased among previous VKA users prescribed dabigatran 110 mg.
Prescription patterns
Our study shows that dabigatran uptake has been rapid, as it already constitutes 5.2% of oral anticoagulant therapy prescribed to AF patients during the initial 4 months after approval. Slightly higher numbers have been seen in the USA after approval, where the market share of dabigatran was 7%, 12% and 28% during the first, second and fifth quarters.24 In the present study, 51.5% and 68.7% of dabigatran users were VKA naive patients (110 and 150 mg, respectively), indicating that the novel oral anticoagulants such as dabigatran are relevantly considered as first-line oral anticoagulant therapy.2
Compliance with European recommendations
EMA and FDA approved dabigatran use in AF patients with at least one of the following risk factors: previous stroke, transient ischaemic attack or systemic embolism; left-ventricular ejection fraction <40%, symptomatic heart failure, and age ≥75 or ≥65 years with one of the following: diabetes, coronary artery disease or hypertension. In the USA, off-label use of dabigatran has commonly been shown.24 In our population, 90.3% and 55.5% of the patients treated with dabigatran 110 and 150 mg, respectively, met the EMA recommendations.2 ,11 Thus, off-label use with dabigatran 150 mg was also common in our cohort.
In the present study, few patients ≥80 years were treated with 150 mg dabigatran, compared with more than half of the patients on 110 mg dabigatran. This is reassurring as there is an increased risk of bleeding among older patients; thus, 110 mg dabigatran is being recommended in those aged >80 years.4 ,25 In addition,we found that one-fourth of the patients treated with dabigtran 150 mg had a high bleeding risk (as reflected by HAS-BLED score ≥2), and some were diagnosed with liver or renal disease. In those at high bleeding risk, 110 mg twice daily is recommended.2 ,26
Thromboembolism and bleedings, with or without previous VKA use
The duration of follow-up was approximately 4 months, since the registry data were only available for the period until the end of 2011. In the overall cohort, we unexpectedly found that the adjusted risk of thromboembolic events was increased among users of both doses of dabigatran.4 Among VKA naive subjects, the risk of thromboembolic events was comparable with VKA with both doses of dabigatran, but increased in dabigatran users who had previously used VKA. This is in contrast to results from the RE-LY study, where thromboembolic events among previous VKA users and VKA naive patients were similar between groups.27 The interpretation of this is that dabigatran, at least at this point, is being used in clinical settings where VKA have failed. Notably, these results reflect real-life clinical use of a novel anticoagulant that is not necessary but is in accordance with use in a controlled clinical trial. Guidelines recommend a novel oral anticoagulant if warfarin is difficult to keep within therapeutic range, in case of side-effects, or an inability to undertake international normalised ratio (INR) monitoring (class IB).2 The increased thromboembolic risk in previous VKA users prescribed that dabigatran users can plausibly be explained by several unmeasured confounders including poor compliance or unmeasured serious comorbidities. Differences in baseline characteristics between VKA naive and previous VKA users, the latter being associated with more comorbidities, support this assumption.
Broadly comparable patterns were seen concerning bleeding, with an increased risk among previous VKA users treated with dabigatran 110 mg, and a similar risk to warfarin among VKA naive patients with dabigatran. These findings are somewhat surprising, given that VKA naïve patients usually have more bleedings shortly after initiation, at least in some studies18 ,19 ,27 On the other hand, our finding supports current recommendations that patients complying with VKA treatment who are kept within the recommended therapeutic INR range (ie, with high time in therapeutic range) should remain on warfarin treatment rather than ‘switch’. As patients treated with dabigatran 110 mg twice daily in our study were older, with more comobidity and a higher HAS-BLED score (with increased bleeding risk), this could be a product of unmeasured confounders.25 Patients treated with dabigatran 110 mg twice daily had higher CHA2DS2-VASc and HAS-BLED scores than patients treated with dabigatran 150 mg twice daily, as did previous VKA users compared with VKA naive patients. One previous study showed that patients with both high CHA2DS2-VASc and HAS-BLED scores had the most net-clinical benefit from VKA treatment.22 Whether the high-risk patients in our study would have shown a net-clinical benefit from 150 mg twice daily instead of 110 mg dabigatran cannot be concluded from the present analyses. However, it is possible that clinicians may have opted to particularly use dabigatran 110 mg twice daily in patients perceived to be at high risk for bleeding (ie, high HAS-BLED score) as the primary consideration, and given that stroke and bleeding risk parallel each other, the CHA2DS2-VASc score was correspondingly higher.
With cautious interpretation due to the low number of events and short follow-up, dabigatran use in VKA naive patients seems to be a safe option in our study without an increased risk of thromboembolic or bleeding events.27 In addition, our results call for a more cautious approach when shifting high-risk patients from VKA to dabigatran treatment.
Strengths and limitations
The strength of this study is the completeness of data, with a nationwide unselected cohort of AF patients initiated on oral anticoagulation. In Denmark, all citizens regardless of socioeconomic status, healthcare-insurance and geography are covered by a public healthcare system ensuring complete registration of outpatient contacts and hospital admissions. The pharmacies also register all claimed prescriptions. By the use of a unique personal registration number, administrative registers can be linked on an individual level. In this setting, it is possible to describe the initial Danish experience with dabigatran, compared with VKA, and indirectly reveal the doctors’ interpretation of EMA's recommendations for dabigatran use in clinical practice. The register data used have been validated previously,16 ,17 ,28–30 as have the methods used for assessment of comorbidity and risk stratification in patients with AF.18 ,20–22
One limitation is that we had no information of INR values, time in therapeutic range or creatine clearance. To overcome this drawback, methods from previous studies were used.22 In the adjusted analyses, we included known confounders present in our registries, but unmeasured confounders may still have influenced our results. Another major limitation is the short period of follow-up, and thus the low number of events of both thromboembolism and bleeding. Thus, interpretations of these risks should be cautious and seen in the context of an early pattern after approval of dabigatran. In addition, our definition of bleeding varies from the definition used in the RE-LY trial,4 but at least it includes serious bleedings leading to hospitalisation, as has been used previously.18
Conclusion
Deviations from the recommended use of dabigatran were frequent among patients treated with 150 mg twice daily. Dabigatran use in VKA naive patients with AF seems safe. Reasons for the increased risk of thromboembolic events with dabigatran (and bleeding with 110 mg twice daily) among previous VKA users may reflect patient selection and ‘drug switching’ practices that merit a more cautious approach when shifting high-risk patients from VKA to dabigatran treatment. Additional real-life follow-up data of dabigatran use are warranted in the future.
References
Supplementary materials
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
Files in this Data Supplement:
- Data supplement 1 - Online supplement
Footnotes
GYHL and MLH contributed equally.
-
Contributors MLH, GG, CT-P and RS participated in the study design and data analysis. RS wrote the paper. All authors interpreted the results, revised the report and approved the final version.
-
Funding The present study did not receive specific funding. GG is supported by an independent research scholarship from the Novo Nordisk Foundation.
-
Competing interests None.
-
Ethics approval Register studies do not require ethical approval in Denmark. The study was approved by the Danish Data Protection Agency (ref: 2007-41-1667).
-
Provenance and peer review Not commissioned; externally peer reviewed.
-
Data sharing statement No additional data are available.