Article Text

Abstract
Objective To identify factors that have contributed to the systematic development of the Cambodian human resources for health (HRH) system with a focus on midwifery services in response to high maternal mortality in fragile resource-constrained countries.
Design Qualitative case study. Review of the published and grey literature and in-depth interviews with key informants and stakeholders using an HRH system conceptual framework developed by the authors (‘House Model’; Fujita et al, 2011). Interviews focused on the perceptions of respondents regarding their contributions to strengthening midwifery services and the other external influences which may have influenced the HRH system and reduction in the maternal mortality ratio (MMR).
Setting Three rounds of interviews were conducted with senior and mid-level managers of the Ministries of Health (MoH) and Education, educational institutes and development partners.
Participants A total of 49 interviewees, who were identified through a snowball sampling technique.
Main outcome measures Scaling up the availability of 24 h maternal health services at all health centres contributing to MMR reduction.
Results The incremental development of the Cambodian HRH system since 2005 focused on the production, deployment and retention of midwives in rural areas as part of a systematic strategy to reduce maternal mortality. The improved availability and access to midwifery services contributed to significant MMR reduction. Other contributing factors included improved mechanisms for decision-making and implementation; political commitment backed up with necessary resources; leadership from the top along with a growing capacity of mid-level managers; increased MoH capacity to plan and coordinate; and supportive development partners in the context of a conducive external environment.
Conclusions Lessons from this case study point to the importance of a systemic and comprehensive approach to health and HRH system strengthening and of ongoing capacity enhancement and leadership development to ensure effective planning, implementation and monitoring of HRH policies and strategies.
- Public Health
This is an open-access article distributed under the terms of the Creative Commons Attribution Non-commercial License, which permits use, distribution, and reproduction in any medium, provided the original work is properly cited, the use is non commercial and is otherwise in compliance with the license. See: http://creativecommons.org/licenses/by-nc/3.0/ and http://creativecommons.org/licenses/by-nc/3.0/legalcode
Statistics from Altmetric.com
Article summary
Article focus
-
To identify factors that contributed to the systemic development of the Cambodian human resources for health (HRH) system and to derive lessons for HRH system development in fragile resource-constrained countries.
Key messages
-
Lessons derived from this case study point to the importance of a systemic and comprehensive approach to health and HRH system strengthening and of continuous capacity enhancement and leadership development to ensure effective planning, implementation and monitoring of HRH policies and strategies. A conceptual framework ‘House Model’2 developed by the authors formed the backbone for assessing the key variables that impact on the HRH system and the dynamic interrelationships between them.
-
The Cambodian HRH system has developed incrementally to improve the production, deployment and retention of midwives in rural areas as part of a systematic strategy to reduce maternal mortality. The improved availability and access to midwifery services is likely to have contributed significantly to reducing the maternal mortality ratio (MMR).
-
Other factors which contributed to MMR reduction included the development of effective mechanisms for decision-making and implementation; political commitment to reduce MMR and mobilise required resources; leadership from the top, along with a growing capacity of mid-level managers; increased the Ministry of Health (MoH) capacity to plan and coordinate supporting development partners; and conducive changes in external environment.
Strengths and limitations of this study
-
The thrust of this study is based on the logical flows and framework of the ‘House Model’ developed and presented by the authors.2 This study also places particular emphasis on the linkages between the core components and functions of HRH management and on the different jurisdictions of the government. This draws attention to their interface with the HRH system and the requirement for a variety of types of government capacity. Ongoing refinements to such models are of value in fine-tuning our understanding of how systems function and can be strengthened.
-
Study insights were derived from three rounds of interviews with key informants, in-depth analyses of these interviews and associated relevant literature. This approach contributed to identifying and articulating the particular events pertaining to the development of midwifery in Cambodia. The interviews with MOH personnel in particular enabled detailed insights regarding the roles and actions of stakeholders, as well as of the consequences of these actions for the system. These insights underpinned the study team's interpretation of the events which took place and the factors which contributed to them, thus allowing a comprehensive story to be told.
-
Interviews focused largely on the MoH and did not explore the perspectives of other relevant ministries. This may have contributed to a degree of bias in describing the main events contributing to MMR reductions. The perspectives of provincial and district authorities and midwives were beyond the scope of this study as was a detailed exploration of any unintended negative consequences of the policies and processes described and their impact on the day-to-day performance and the ability to provide quality services. These merit further exploration.
Introduction
Poor health outcomes are often associated with a shortage and/or maldistribution of health professionals.1 Piecemeal approaches to human resources for health (HRH) that focus on one issue, such as production or deployment, while neglecting other aspects of the HRH system are ineffective, particularly in fragile countries where the health system, infrastructure and social services are underdeveloped.2 Improving maternal, newborn and child health and reducing maternal mortality requires a comprehensive approach, involving competent and committed midwives to ensure 24 h service delivery and a strong focus on equity of access to maternity care by a skilled birth attendant.3 ,4
Cambodia has been identified as one of the poorest countries in South East Asia. Most (80%) of the population of 13.4 million lived in rural areas in 2008.5 The health status of Cambodians ranked low compared with other countries in the region; the infant mortality rate was assessed in 2010 as 45 per 1000 live births and maternal mortality ratio (MMR) as 206 per 100 000 live births.6
Midwives in Cambodia are the main workforce dealing with reproductive, maternal and newborn care in hospitals and health centres. Their work includes basic emergency obstetric care as defined in the standard package of activities for each level of facilities.7 They are classified into two categories (primary and secondary) according to the duration of professional education. Although both work at all levels of the health system, the original intention was that primary midwives would work at health centres and in a supportive role to secondary midwives.7
Cambodia has focused on HRH in the ‘post’-conflicti period since the 1990s. Incremental efforts to scale up the quantity and quality of HRH focused on the production of midwives from 2000 and intensified production of both primary and secondary midwives after 2005. These efforts resulted in an increased number of midwives working at health centres and significant improvements in the coverage of maternal health services (figures 1 and 2). Recent international analyses of maternal mortality highlight the significant improvements in Cambodia (figure 2).6 ,9 Despite financial constraints, the Cambodian government health expenditure has steadily increased (figure 3), reflecting the national commitment and leadership. The ‘story behind this story’ (ABZ) of achievement deserves to be analysed and documented.

Number of midwives 1996–2011 (public sector). MoH, Ministries of Health.

Coverage of maternal health services and maternal mortality ratio.

Health expenditure per capita 1995–2010 at exchange rate (US$).
This paper aims to:
-
Present insights and evidence of the achievements resulting from the investment in midwives and the systems in which they operate;
-
Describe and analyse the factors related to extending and supporting midwifery; and
-
Assess the broader implications for HRH systems development, policy and practice.
Methods
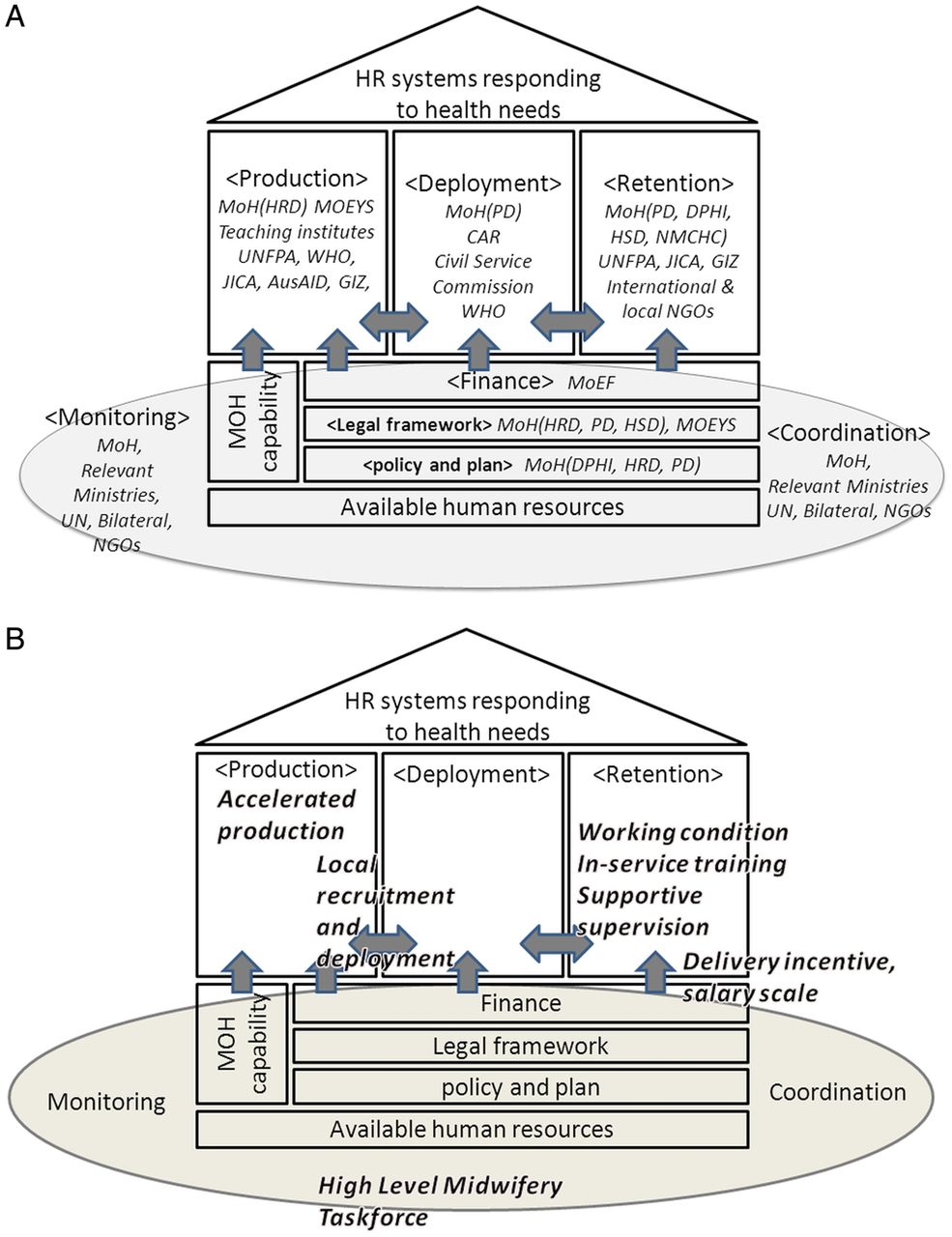
Policy documents and reports, both in the published and grey literature in four languages (English, Khmer, Japanese and French), were reviewed and the database was searched (PubMed and Science Direct) with key words (Cambodia, midwife, midwifery health system, health workers, HRH, and words similar to these words). The literature identified through these searches was assessed by all authors with reference to the ‘House Model’ (figure 4),2 which highlights 11 closely linked and interdependent elements of the HRH system. It includes additional components and functions of the HRH system which were not independently recognised within the WHO framework but which appear significant in the light of this study, including the legal and regulatory frameworks. We examined the events and processes which contributed to and/or impeded the development of the HRH system, with an emphasis on the particular attention given to midwives as a key component of the strategy to address maternal and child health (MCH).

{kind=link}
{kind=link}
{kind=link}
{kind=link}
(A) Stakeholder mapping (House model). (B) Key interventions. Aus AID, Australian Agency for International Development; CAR, Council for Administrative Reform; DPHI, Department of Planning and Health Information, Ministry of Health; GIZ, Deutsche Gesellschaft für Internationale Zusammenarbeit; HRD, Human Resource Development Department, Ministry of Health; HSD, Hospital Service Department, Ministry of Health; MOEYS, Ministry of Education, Youth and Sport; MOEF, Ministry of Economy and Finance; MOH, Ministry of Health; NGO, Non-governmental Organization; NMCHC, National Maternal and Child Health Center; PD, Personnel Department, Ministry of Health; JICA:,Japan International Cooperation Agency; UN, United Nations; UNFPA, United Nations Population Fund; WHO, World Health Organization.
The decision to conduct interviews with individual stakeholders rather than groups was based on a consideration of the cultural context and the readiness of stakeholders to offer critical views of their superiors and their organisations. Data collection occurred in three complementary stages. The first and second rounds of interviews sought to describe HRH system development, issues and opportunities. The first focused more on the role of stakeholders and their views on the present HRH system while the second enquired about HRH system development, future priorities and sustainability. A third round of interviews focused on midwifery in Cambodia since 1980 and explored key midwifery issues identified from both the literature and the earlier interviews, with a focus on the roles of stakeholders and external influences. The approach emphasised a strengths-based approach, seeking to identify and explore in greater detail those factors which contributed to, rather than hindered, system development.
In September 2011, the first series of interviews was conducted with 30 stakeholders (14 Ministry of Health (MoH), 1 non-health Ministry, 5 educational institutes, 2 professional councils and 10 development partner agencies). The second set in June 2012 included 5 MoH personnel and 2 development partner agencies. The third round, in August 2012, included 12 stakeholders (9 MoH senior level and middle-level managers, 3 development partner agencies). Key informants were identified through the earlier interviews and a snowball technique (figure 4A). The first two rounds of interviews identified the strong top-down approach to decision-making (illustrated in the findings below) that limited the participation in decision-making and policy-making to a narrow range. As a result, the key informants in the third round of interviews were those working for the MoH and development partners despite seeking, through snowball sampling, to widen the identification of those participating in these processes. Educational institutions had limited participation and influence in the policy-making and decision-making processes and the professional councils also had limited influence as they were in early stages of development.
Interviews were conducted in English by two researchers (KA and NF), who had working experiences in health technical cooperation projects and health studies in the country for over a decade. An interpreter assisted with four non-English speaking interviewees in the first round of interviews.
Transcripts were analysed through inductive coding performed separately by KA and NF using Nvivo 9. The two sets of coding were compared and combined after discussing any differences. Core concepts were discussed and refined in consultation with ABZ and ArR. Key contributing factors were derived from concepts referring to each component and linkages between the core components of the ‘House Model’ and different jurisdictions of the government (policy and planning, finance, legal). The linkages incorporate HRH management (production–deployment–retention)
Findings
In this section, we first present the chronology of HRH system development (Otable 1) focusing on midwifery issues from 1980 onwards, corresponding to the period covered by this study. The chronology (table 1) draws in new findings from the archival review which took 1946 as the start-date. We present key events in the evolution of a more comprehensive approach to reducing maternal mortality which covers the components of the House Model. We also present stakeholder perspectives on HRH issues and identify those factors which contributed to increases in midwifery service coverage.
Evolution and chronology of health system, human resource system and midwifery-related issues in Cambodia (1946–2012)
Chronology of HRH system development, focused on midwifery from 1980 to 2005 (table 1)
The following subsections depict chronologically the main issues, responses and developments concerning HRH in midwifery (1980–2005). The areas covered include policies and plans, production, deployment, and retention, organisations, and partnership with development partners.
Accelerated production after the Khmer Rouge genocide
Since very few health professionals survived the Khmer Rouge regime (1975–1979), Cambodia needed to reconstruct its health system to provide basic services and accelerate the production of health personnel (Lanjouw S, Macrae J, Zwi A. The role of external support for health services rehabilitation in ‘post’-conflict Cambodia. Unpublished report, 1998). The MoH standardised curricula for nursing and midwifery schools for two types of midwife: primary and secondary.10 Agencies working in the Thai-border refugee camps continued to produce health workers with varying abilities (Lanjouw S, Macrae J, Zwi A. The role of external support for health services rehabilitation in ‘post’-conflict Cambodia. Unpublished report, 1998).
Development of MoH institutional capacity and organisational evolution for HRH
From the 1990s, the MoH started to develop institutional capacity with international community support. In 1995, as part of the health sector reforms, the MoH established the Department of Human Resources Development (HRD, in charge of production and continuous education), the Personnel Department (PD, deployment and personnel management) and the National Maternal and Child Health Center (NMCHC, maternal and child health national programmes) (Lanjouw S, Macrae J, Zwi A. The role of external support for health services rehabilitation in ‘post’-conflict Cambodia. Unpublished report, 1998). Some core MoH staff were sent abroad to study public health with the support of development partners.
Policies and plans: shifting from quantity to quality, suspension of production of midwives
The MoH developed HRH policy with external technical assistance and formulated a health workforce plan, rationalised professional categories and shifted the focus from producing large numbers of basic health workers to ensuring availability of better qualified staff.11 This change, influenced by the development partners, resulted in the suspension of midwifery training between 1997 and 2003,12 resulting in a 10% decrease in numbers. This hindered the capacity to attain staffing standards for midwives especially in rural areas13 (figure 1):
…It was a big mistake, big, big mistake. I think at that time, the international standard was not consistent with the real situation of Cambodia. (MoH1)
Accelerated production to respond to acute shortages
The shortage of midwives became apparent early in the 2000s.13 The MoH responded promptly to address the shortage and accelerated production through a 1-year primary midwife (PMW) course.12 Following a situation analysis by HRD, the PMW course started in 2003 in four provinces. It was delivered by provincial health departments (PHDs) with provincial trainers, adapting arrangements from the 1980s, emphasising local recruitment, establishing workplace contracts and providing student allowances.14
Around the same time (2002), the First Health Strategic Plan (HSP1) 2003–2008 was formulated and provided MoH staff with clear directions for human resource development.
[Formulation of] policy and health strategic plan was an achievement. Before [it was] not clear, no guidelines. (MoH7)
In 2005, given the dissatisfaction with the quality of the PMW graduates, the MoH decided to shift the responsibility for training from the PHDs to the regional training institutes that were expected to offer better quality programmes.12 ,14
Changes associated with partnership with development partners
In the process of expanding the sector-wide approach (SWAP), a group of development partners established a pooled fund as a new funding modality.16 This modality provided MoH departments with more flexible and accessible microlevel budgeting based on their self-designed plans.
Key events in the evolution of a comprehensive approach to reducing maternal mortality and stakeholder perspectives on HRH issues (table 1)
First midwifery forum (2005)
The high MMR (472 per 100 000 live births) identified through the Demographic and Health Survey (DHS) 2005 evoked major concerns17 and propelled the MoH to take urgent action:
Everyone woke up. All felt ashamed… We talked that we have to do something. (DP2)
The first Midwifery Forum convened in December 2005 was a high profile national event which promoted political commitment to systematically and comprehensively tackle maternal mortality.28 Relevant stakeholders from the Deputy Prime Minister to field midwives were involved and represented every component of the HRH system (figure 4B). Final recommendations included concrete multidimensional and multisectoral interventions: increasing the number of midwives at health centres, motivating midwives through increasing salaries and performance incentives, improving working and living conditions in rural areas, and supporting midwifery education and students.28
The top-level decision to reward performance for a live birth (‘delivery incentive’) at hospitals and health centres had a great impact on the reduction of MMR. The government-funded delivery incentive (US $10–15) was successfully implemented in 2007, and involved the provincial treasury and commune council.20
Recommendations from the Forum were very positive and effective for reducing MMR. ….It was a starting point to promote midwives. (MoH1)
Stakeholder involvement was evident with contributions from development partners. The Secretary of State set the agenda, involved key stakeholders and engaged mid-level managers from MoH departments (HRD, PD and NMCHC) in decision-making, drawing on relevant data.
High-level midwifery taskforce
Following the first national Midwifery Forum, a comprehensive situation analysis supported by development partners identified effective interventions in 2006.7 This led to the development partners and Secretary of State establishing in 2007 a High Level Midwifery Taskforce chaired by the Secretary of State. This event can be seen as the beginning of a sustained systemic approach with participation of mid-level managers from departments for planning, production, deployment and maternal health service delivery.18 The strong leadership enhanced by delegation from the Health Minister promoted coordination with other ministries.
…the terms of reference [of HLMWTF] … [appeared] in the top-down form... [suddenly] 1 day, a notice of the TOR was put on the wall, delivered’ (DP1)
The High-Level Midwifery Taskforce (HLMWTF) developed a multiyear plan focusing on the quantity and quality of midwives and maternal health services.19 Agreed objectives (increased coverage of midwifery services for the reduction of MMR) and a clear role for Taskforce members provided an opportunity for collaborative planning and implementation of strategic interventions. Monitoring indicators were reported to MoH and Annual Health Review meetings provided a platform for broad participation by development partners.19 Within the Taskforce, the development partners contributed skills and knowledge and worked closely with relevant MoH departments. Their Cambodian national staff played a role as mediators.
We collaborate(d) with transparency and accountability [about our work] within a [specified] timeframe. So that our plan is not an ambitious plan but effective with limited resources. (MoH5)
The mid-level managers facilitated the consecutive implementation of effective interventions (figure 4B):
The advantage [of the HLMWTF] was that Directors of MoH departments actually met. There had not been many opportunities….Without having communication, each department…acted inconsistently…like a typical Cambodian way (DP1)
Fast track initiative
The Second Health Strategic Plan (HSP2) 2008–2015 was developed in 2008.22 The MoH contributed much more actively than to earlier efforts, which had been donor-driven. The strategy prioritised midwifery including staffing at health facilities, revision of training content, increasing student intake, raising the quality of training and trainers, and salary reform.22
In 2008, the new Health Minister declared a ‘Fast track initiative to reduce maternal and newborn mortality’ with a target of ‘midwives in all health centers’. It signalled strong leadership from the top, reinforcing the high-level commitment seen earlier. The mid-level managers, including provincial officials, were committed to reaching the target.23 Through the reallocation of midwives from hospitals to health centres,24 and accelerated production and deployment, the target of ensuring 24 h delivery service in all health centres was achieved by having at least one midwife in 2009, although 463 health centres (48%) had only PMWs at present (figure 1):
Slogan [Place midwives in all health centers] is easy to understand for everyone.(DP1)
In 2009, a second midwifery forum reviewed progress.25 The Forum itself was becoming routine, no longer a tool for innovation in tackling midwifery issues.
Reproductive, maternal, newborn and child health taskforce
The Reproductive, Maternal, Newborn and Child Health (RMNCH) taskforce was created in 2009 as one of four taskforces under the HSP2. Unlike HLMWTF, midwifery issues were integrated into the broader RMNCH issues. A mid-level manager with a long-time career and field experience developed the terms of reference and served as chair. Taskforce members were drawn from across the MoH, development partners, and non-governmental organisations.
This Taskforce identified priority areas and interventions, mobilised financial resources, guided implementation and provided an enabling environment.26 The Taskforce institutionalised collaboration within the MoH and offered a roadmap for the Fast Track Initiatives.26
Mid term review of the Health Workforce Development Plan 2006–2015
The MoH requested development partners to facilitate the review of the Health Workforce Development Plan 2006–2015. The Minister of Health established a Human Resource for Health Committee to initially guide the Review and then oversee the implementation of its recommendations. The HRH Committee comprised the Human Resource and MCH leaders and was chaired by the same Secretary of State as HLMWTF.27
Stakeholder perspectives on current and future HRH issues
Stakeholder views of HRH issues were consistent with those in MoH reports.27 Future concerns included the quality of production; regulation of private institutions; retention in rural areas; shortage of capable staff at MoH and the sustainability of development partner support. Recognition of the issues and their causes were shared by many stakeholders, potentially reflecting the MoH communication.
Factors contributing to increasing the coverage of midwifery services
Comprehensive approach to decision-making and effective implementation
A comprehensive approach covering all components of the HRH system framework (‘House Model’) and involving the necessary stakeholders inside and outside the MoH, both at the central and peripheral levels, promoted midwifery services. These contributed to the achievement of quantitative and qualitative HRH targets, although the interventions were primarily related to the supply side. HLMWTF was seen as a successful platform and provided a venue for open-discussion, planning and implementation of strategic interventions. Held in a culturally appropriate setting, this prioritised activities with synergistic effects, given the resource limitations. The Taskforce presented a coherent voice to the outside. The MoH applied this model and experience to the working of the RMNCH Taskforce in the area of RMNCH services and Human Resource for Health Committee in HRH system development.
HRD produce, PD absorb, and NMCHC support and monitor in-service training. A comprehensive and continuous process. We improved step by step. Like a spiral, I think we can call it ‘spiral improvement’. (MOH4)
Political commitment to address high MMR
Political commitment was strong, at a high level and continuous. Key factors for the success in obtaining such commitment were lobbying by the MoH leadership using survey and other data.17,15 Development partners, who were influential to the core ministries, increased awareness of the growing political commitment.
It (involvement of other ministries) did not happen before, but I think, the idea for promoting midwives existed in the Council of Administrative Reform, Secretary of Public Function, and Deputy Prime Minister. So we could involve them. (MoH1)
Delivering it as a clear slogan in the Fast track Initiative (‘Place midwives in all health centers’) accelerated this strategic intervention.26
Leadership from the top for decision-making and effective implementation
Strong top-down leadership is acceptable in Cambodia and is taken seriously by subordinates. A capable and experienced Secretary of State negotiated and coordinated with stakeholders including other ministries, mobilised resources and monitored activities carefully. He created, chaired and led HLMWTF. The Secretary's position and high capacity for donor coordination had been effective.
We need someone strong, behind the scene, and [who can] work for long time. (MoH4)
…MCH Sub COCOM (Coordination Committee) in 1992 or 1993. I was the chair. .. there was a rumor that I became crazy with lots of development partners… We have a proverb in Khmer, ‘two cows at the same time, many cows at the same time, we need to gather them’. So I did. I need to respect (my) role of coordinator, not blame development partners, but create coordination. (MoH1)
‘Staff behind the scene’: growing capacity and confidence of mid-level individual managers
The mid-level managers comprised the right persons from the necessary departments who had knowledge and experience of practice and evidence-based decision-making and monitoring; substantial experience in the MoH; and working experience with development partners. These mid-level managers, often responsible for the technical aspects of programming, prepared the data and documentation that assisted the lobbying and negotiations of the senior MoH leaders:
Not only people at high positions, but people behind the scene are important…the people at the departments who prepare documents are important, they work as a team. (MoH4)
Increased MoH capacity in planning and coordination
Throughout the processes studied, we found evidence of increasing capacity of MoH departments in planning and coordination. For example, the HRD reviewed the quality of PMW production and immediately revised the production mechanisms.14 The PD collaborated with other ministries and implemented smoothly and strategically the recruitment (figure 1), deployment and increased the salary scale of midwives.20 In addition, the Cambodian MoH increased its capacity as demonstrated by its role in formulating HSP2 and establishing the RMNCH Taskforce. This increased MoH capacity facilitated policy implementation around midwifery.
The improved quality of MoH data through the introduction of a workforce projection tool convinced the Council of Ministers to give special treatment to the MoH, which increased civil servant allocations to the MoH by 58% annually for the previous 2 years (figure 1). While not specifically for midwives, many of the positions allocated have been for midwifery; remarkable given that Cambodian government administrative reforms have led to a reduction in civil servant positions overall.
Supportive development partners took actions for human resource crisis and MDG goal
The development partners continued to offer technical and financial support. In addition, they brought new perspectives through working closely with MoH departments for a sustained period. These contributed to capacity development of the MoH and are particularly important in ‘post’-conflict and fragile states where resources are so limited. These partners were able to draw on their national staff to integrate external perspectives with understanding of the cultural and political sensitivities present.
External environment surrounding the health sector
Rapid changes in the external environment after 2000 were also favourable to the health sector in Cambodia. Owing to the political stability and security, Cambodia enjoyed economic growth with dramatic improvements in infrastructure, communication, transportation and the educational level of community members. These improvements facilitated the recruitment of PMW and deployment and retention in remote health centres, which in turn promoted broader HRH system development:
In the late 90's, only for 40km it took all morning. Now we have clean health facilities,…. Start(ed) production (in 2003),… when they (the students) graduate(d) and start(ed) working, infrastructure was improved. Timing was perfect. (DP2)
Discussion
The Cambodian case is encouraging, although the degree of political stability over the last decade is uncharacteristic for ‘post’-conflict countries.8 A comprehensive and systemic approach focused on midwifery consolidated efforts and rapidly achieved the goal of implementing effective interventions to reduce MMR; this built on the incremental development of the health and HRH systems underpinned by economic growth. A similar comprehensive and systemic approach in Liberia, another ‘post’-conflict state, focused on nurses and proved to be effective in expanding service coverage.29
Cambodian Taskforces strengthened coordination at the decision-making level and collaboration at the implementation level. The approach enhanced linkages between the components of the ‘House Model’ contributing to HRH system development. Ongoing HRH system development and those focused on midwives reinforced one another. The high level political commitment to promote achievement of the MDGs propelled the system by ensuring resource availability and more speedy decision-making, documented also in a Sierra Leonian case study.30
Even when a comprehensive approach is taken, a narrow focus on one cadre (in this case, midwives) brought advantages for rapid resource mobilisation, but risked delaying attention and efforts to addressing other issues. This may undermine the needed systemic HRH development. Monitoring progress and adjusting decisions accordingly may help shift the focus as needed for future priorities. This ongoing set of responses, including adjustments based on evidence from previous interventions, enabled the HRH system to cope with the changing and emerging issues for midwifery. These issues changed from a focus on the availability of personnel to an emphasis on the quality of services and the retention of competent and motivated midwives in rural health centres.31 These issues were manifest as shared perspectives of the stakeholders.
In Cambodia, the Secretary of State played a significant role in establishing appropriate fora, committees, taskforces and initiatives to ensure a systemic and integrated approach. The low turnover of mid-level managers reinforced and consolidated their capacity, further sustaining the momentum for system development. Teamwork linked managers and leadership to promote enhanced processes. The importance of capable senior leadership and mid-level managers working together deserves more attention. Increasing the institutional capacity and resources of MoH departments creates and builds the basis for systemic changes, although this is often neglected. Institutionalising and reinforcing a comprehensive approach, through regular stakeholder engagement and other measures, warrants further attention.
HRH system development in ‘post’-conflict countries takes decades, and needs consistent, long-term support at every level of the health system. Such support is more feasible where critical reflections on the HRH system development have occurred and good capacity exists for MoH personnel to drive forward HRH system change and development. Donor-driven development is often pervasive in such countries, resulting in fragmented, short-sighted and often contradictory policies and interventions, as seen in the earlier disruption of midwifery training in Cambodia.
Strengths and limitations
This study is based around the logical flows and framework of the ‘House Model’ developed and presented by the authors.2 The study places particular emphasis on the linkages between the core components and functions of HRH management (production–deployment–retention) and on the different jurisdictions of the government (policy and planning, finance, legal). This draws attention to their interfaces with the HRH system as well as necessitating different types of government capacity. Ongoing refinements of such models are of value in conceptualising how systems operate and determining how they might be further enhanced or strengthened.
The study insights were derived from three rounds of interviews with key informants, subsequent in-depth analyses of interviews and relevant literature. This approach contributed to identifying and articulating the particular events pertaining to the development of midwifery in Cambodia. Given the profile of informants and the cultural context, individual interviews instead of group interviews were considered more appropriate in eliciting the opinions of stakeholders.
Non-Khmer interviewers were both a strength and a limitation; offering a degree of objectiveness alongside limitations in appreciating cultural nuances. The interviews with MoH personnel in particular enabled detailed insights regarding the roles and actions of stakeholders, as well as of the consequences of such actions for the HRH system. These insights underpinned the study team's interpretation of the events which took place and the factors which contributed to them, thus allowing a comprehensive story to be told.
Although the results of the first and second round interviews defined the focus of interviews on MoH personnel, this may have led to some degree of bias in descriptions of the main events concerning MMR reductions, and in so doing reducing the scope for exploring more comprehensively the perspectives of other relevant ministries. Another limitation is that we were unable to examine the perspectives of provincial and district level personnel, and those of midwives themselves, in relation to interventions to reduce MMR. The unexpected consequences of policy interventions at local levels may not have been fully explored as a result. The perspectives of provincial and district levels, and midwives were, however, not the main focus of our research.
Conclusion
This study examines and documents the key events and underlying factors which contributed to an emphasis on midwifery as part of the response to high maternal mortality and simultaneously to building the HRH system. The well-focused and integrated approach was central to Cambodian achievements. Increased MoH capacity, both at the organisational and individual levels, also contributed. Capable senior and mid-level managers are vital for HRH system development, especially in ‘post’-conflict countries. The systemic approach adopted could well be applied to other existing and emerging priority health issues.
In Cambodia and elsewhere, the HRH systems approach needs to be complemented by consolidating sustainability. Studies of HRH system experiences are little documented but valuable. Such critical but constructive debate offers useful insights for HRH system development.
Footnotes
-
Contributors NF and KA reviewed the literature, designed and conducted the interviews, analysed the results and wrote the first draft. AZ and ArR contributed to the design, conceptualisation, methods, analysis and writing. RT and PK contributed to the literature review and preparation of chronology. AnR contributed to the draft revision. All authors reviewed and agreed with the final version of the paper.
-
Funding The study was funded by a Research Grant for International Health, H22-8, by the Ministry of Health, Welfare and Labor, Japan (http://www.ncgm.go.jp/kaihatsu/). The funders had no role in the study design, data collection and analysis, decision to publish, or preparation of the manuscript.
-
Competing interests None.
-
Ethics approval This study was approved by the Ethical Committee of National Center for Global Health and Medicine, Japan, and by that of the Ministry of Health, Cambodia.
-
Provenance and peer review Not commissioned; externally peer reviewed.
-
Data sharing statement No additional data are available.
-
↵i We use the term ‘post’-conflict in recognition of the fact that in many such countries conflict continues in some areas or recurs.8