Article Text

Abstract
Objective To resolve uncertainty as to the risk of Sudden Infant Death Syndrome (SIDS) associated with sleeping in bed with your baby if neither parent smokes and the baby is breastfed.
Design Bed sharing was defined as sleeping with a baby in the parents’ bed; room sharing as baby sleeping in the parents’ room. Frequency of bed sharing during last sleep was compared between babies who died of SIDS and living control infants. Five large SIDS case–control datasets were combined. Missing data were imputed. Random effects logistic regression controlled for confounding factors.
Setting Home sleeping arrangements of infants in 19 studies across the UK, Europe and Australasia.
Participants 1472 SIDS cases, and 4679 controls. Each study effectively included all cases, by standard criteria. Controls were randomly selected normal infants of similar age, time and place.
Results In the combined dataset, 22.2% of cases and 9.6% of controls were bed sharing, adjusted OR (AOR) for all ages 2.7; 95% CI (1.4 to 5.3). Bed sharing risk decreased with increasing infant age. When neither parent smoked, and the baby was less than 3 months, breastfed and had no other risk factors, the AOR for bed sharing versus room sharing was 5.1 (2.3 to 11.4) and estimated absolute risk for these room sharing infants was very low (0.08 (0.05 to 0.14)/1000 live-births). This increased to 0.23 (0.11 to 0.43)/1000 when bed sharing. Smoking and alcohol use greatly increased bed sharing risk.
Conclusions Bed sharing for sleep when the parents do not smoke or take alcohol or drugs increases the risk of SIDS. Risks associated with bed sharing are greatly increased when combined with parental smoking, maternal alcohol consumption and/or drug use. A substantial reduction of SIDS rates could be achieved if parents avoided bed sharing.
- Prevention
- Public Health
- Epidemiology
- Sids
- Bed sharing
This is an open-access article distributed under the terms of the Creative Commons Attribution Non-commercial License, which permits use, distribution, and reproduction in any medium, provided the original work is properly cited, the use is non commercial and is otherwise in compliance with the license. See: http://creativecommons.org/licenses/by-nc/3.0/ and http://creativecommons.org/licenses/by-nc/3.0/legalcode
Statistics from Altmetric.com
Article summary
Article focus
-
Is there a risk of Sudden Infant Death Syndrome (SIDS) due to bed sharing when the baby is breastfed, the parents do not smoke, and the mother does not use alcohol or illegal drugs?
-
At what age is it safe to bed share?
-
How is the risk of SIDS associated with bed sharing affected by other factors?
Key messages
-
When the baby is breastfed and under 3 months, there is a fivefold increase in the risk of SIDS when bed sharing with non-smoking parents and the mother has not taken alcohol or drugs.
-
Smoking, alcohol and drugs greatly increase the risk associated with bed sharing.
-
A substantial reduction in SIDS rates could be achieved if parents avoided bed sharing.
Strength and limitations of this study
-
This is the largest ever analysis of individual records of 1472 SIDS cases and 4679 controls from five major case–control studies.
-
Questions on the mother's alcohol use in the last 24 h and illegal drug use were not asked in three of these studies.
-
Imputation of missing data enabled a combined analysis of all the data. The analysis gives unbiased, efficient models that describe the data accurately, especially in key areas.
Background
Despite the marked reduction in Sudden Infant Death Syndrome (SIDS)1 following the advice to place babies to sleep on their back (supine),2 SIDS remains the major cause of infant death in the postneonatal period (28 days through to the first birthday) in high income countries. For instance, in the USA, SIDS remains the leading cause of postneonatal mortality where 2353 babies died from SIDS in 2008, about 0.6/1000 live-births.3
Some countries give advice to parents in their ‘Reduce the Risks’ literature not to bed share with their babies under any circumstances. For example, the Netherlands advises parents not to bed share for the first 3 months of life4 based on their own research findings.5 This is also the case for the USA6 where the American Academy of Pediatrics Task Force on SIDS cited European7 and New Zealand8 data (included in this paper) and made a clear statement advising against bed sharing for sleep. Other countries, notably the UK and Australia, advise only certain groups not to bed share for sleep.9–12 Bed sharing and the risk of SIDS have become controversial, especially as some, while listing when it should be avoided, highlight the benefits of bed sharing.13 ,14
There is general acceptance that sleeping with a baby is a risk factor for SIDS when sleeping on a sofa in any circumstances or in a bed if the mother smokes and/or has taken alcohol.15 ,16 However, authors differ as to whether, in the absence of these risk factors, bed sharing represents a risk.17–22 Mitchell,23 in a recent review, suggests that before embarking on further studies, much could be achieved by combining the information from current studies.
However, these risks, specifically for non-smokers when breastfeeding, cannot be quantified directly from published data by standard meta-analysis due to the different ways risks are reported.5 ,17 ,19 ,24 ,25 The limited assessment of interactions, for instance between bed sharing and breastfeeding, due to the lack of individual data to analyse was highlighted in the recent meta-analysis of case control studies of SIDS.26 Therefore, the leading authors of five major recent case–control studies agreed to combine the individual data to estimate the risk associated with bed sharing in relation to breastfeeding, smoking, mother's recent alcohol consumption and illegal drug use, after controlling for the other most important risk predictors, namely whether the baby slept in the parents’ room or elsewhere, position in which the baby is put to sleep, mother single, mother's age and parity and baby's birth weight. These five datasets included all cases that some might now classify as ‘unascertained’ or ‘asphyxia’ because they were found to be bed sharing or sleeping face down.
Material and methods
Study population
Data from the European case control studies 1992–1996, that is, The European Concerted Action on SIDS, ECAS,7 the Scottish 1996–2000,27 the New Zealand 1987–1990,8 the Irish 1994–200328 and the German GeSID 1998–200129 datasets were combined. Cases and controls over 1 year of age were excluded. The combined dataset comprised 1472 cases and 4679 normal controls of similar age. For details on how the controls were selected, see online supplementary appendix.
Notes on explanatory variables
The explanatory variables were defined as follows:
-
Bed sharing was defined as when one or both parents slept with the baby in their bed so that they woke to find the baby dead in bed with them. Controls were bed sharing if the baby was in bed with them when they awoke on the day of interview.
-
Room sharing—sleeping in the parents’ room but not in the parents’ bed.
-
Breastfed—infant was being partially or completely breastfed at the time of death or interview.
-
Bottle fed—the infant was not breastfed at this time.
-
Parents—the mother and her current partner.
-
Age—the infant's age at death or at interview for controls.
-
AOR—multivariate adjusted OR (AOR). AORs and rates are followed by the 95% CI in parentheses.
All datasets enabled the identification of cases found sleeping in the parents’ room or elsewhere and whether or not they were bed sharing, together with comparable control data. Cases and controls cosleeping on a sofa or elsewhere were included but grouped with those not bed sharing and not sleeping in the parents’ room. Whether or not the mother or partner smoked, together with the infant's age, sex, race, birth weight, mother's age, parity, whether single or with a partner, and position the infant was last placed to sleep and how the baby was being fed at the time of death/interview were available for all datasets. In addition, data on the mother's alcohol consumption in the last 24 h and mother's illegal drug use after birth were available in two datasets. In total, all the variables shown in table 1, together with age at the time of death or interview, and studyi were used in the analyses.
The number and percent of cases and controls for each factor, percent missing data, univariate ORs and Cls based on complete data. Also, univariate ORs and multivariate AORs and Cls based on the imputed data sets.
Statistical analysis
All variables, other than case or control, age and study, included some missing data. Missing data were imputed as described in the online supplementary appendix. ORs were calculated by logit regression. Univariate analyses were adjusted for age and study because controls were on average 3 weeks older than cases, and the number of controls per case varied between studies. For multivariate AORs, a multilevel logit regression model was used with ‘bed sharing’ random across studies. The fraction of bed sharing deaths attributable to bed sharing, that is the fraction of bed sharing deaths that would not have occurred had the babies not been bed sharing but placed supine on a cot in the parents’ room, all other things being unchanged, was computed as described by Bruzzi et al30 Death rates were computed using the same multivariate model by omitting the trend of bed sharing with age. Rates are given for all infants computed by a weighted combination of the rates for boys and girls. The base rate for girls was the SIDS rate when none of the model risk factors were present. To obtain average AOR for infants <3 months and for infants aged 3 months or more, a logistic form of the rates model confined to records under 3 months and 3 months or more was fitted.
Full details of the statistical methods are given in the online supplementary appendix.
Results
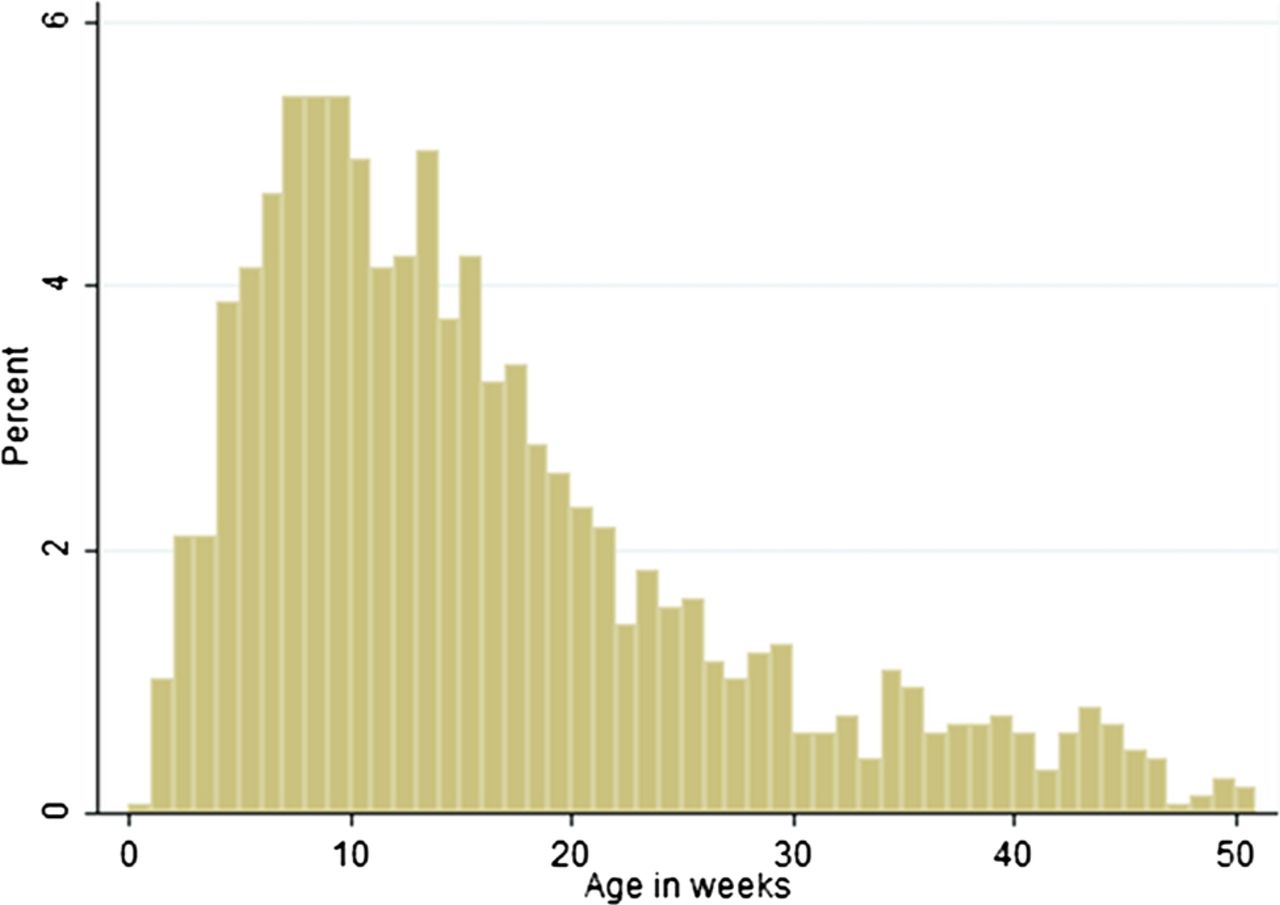
The age distribution of the 1472 cases is shown in figure 1. The peak incidence rate is between 7 and 10 weeks.

The age distribution of the cases in the combined study.
Univariate and multivariate analyses
The data for each variable are tabulated for cases and controls in table 1 together with the percentage of missing data and the single factor ORs adjusted for age and study, together with the corresponding OR derived from analysis of the imputed datasets. Corresponding multivariate adjusted AORs from the overall rates model are also reported. For variables that interact with bed sharing, and consequently age, AORs reported in table 1 are those for infants room sharing but not bed sharing.
Feeding
Table 1 shows that bottle feeding increases the risk of SIDS. When analysed as a single factor, the OR for bottle feeding is 2.9 (2.5 to 3.3); however, the multivariate AOR is 1.5 (1.2 to 1.8).
Multivariate analyses for interactions between age, bed sharing and other variables
The baseline in the multivariate analysis is a breast-fed baby placed on his/her back to sleep on a cot in the parents’ room neither of whom smokes nor has any other risk factors.
Bed sharing
The log-linear downward trend in the OR for bed sharing in the first 6 months of life is shown in figure 2, when neither parent smoked and when both smoked. These values are predicted by the overall model of the whole dataset. Checks show that the predicted risks closely fit the data, especially when neither parent smoked and the mother had taken neither alcohol nor drugs and the baby was breastfed and bed sharing (see online supplementary appendix).

{kind=link}
{kind=link}
Adjusted ORs (AORs; log scale) for Sudden Infant Death Syndrome by age for bed sharing breast-fed infants, when neither parent smokes and both smoke versus comparable infants sleeping supine in the parents’ room. AORs are also adjusted for feeding, sleeping position when last left, where last slept, sex, race, and birth weight, mother's age, parity, marital status, alcohol and drug use.
The analysis showed that only the position last left, parental smoking, maternal alcohol consumption in the last 24 h and illegal drug use interact with bed sharing, and consequently the associated risks when bed sharing also decline with increasing age. Table 2 summarises the adjusted AORs for each of these factors, first when room sharing and second when bed sharing at 2, 10 and 20 weeks of age. Three ages are used to illustrate the reduction in risks associated with bed sharing, as the baby gets older. Table 2 confirms that the OR for bed sharing is 8.3 (3.7–18.6) at 2 weeks, and figure 2 shows that bed sharing is a significant risk factor for the first 15 weeks of life in the absence of smoking, alcohol, drugs and all other risk factors.
The AORs for avoidable factors that interact with bed sharing, adjusted for all other factors. Therefore, they relate to the baseline corresponding to babies of non-smoking mothers who do not use drugs, and taking <2 units of alcohol in the last 24 hours, having a non-smoking partner, and no other risk factors
Position last left
When sleeping in a cot, there is a significant risk associated with placing the baby on its side and a substantial risk when it is placed prone. In contrast, when bed sharing, being placed on the side is not associated with an increased risk and analysis shows that when the baby is placed prone, there is little and no significant increase in risk for the first 3 months, table 2.
Parental smoking
Table 2 also highlights the strength of the very significant interaction between smoking and bed sharing. Infants who bed share at 2 weeks of age and whose parents both smoke are at 65-fold increased risk of SIDS compared with infants room sharing with parents who do not smoke. There is a ‘dose response’ effect, univariately, when room sharing, and when bed sharing at 2, 10 and 20 weeks related to whether just the partner smokes, just the mother smokes or both smoke. However, when the parents do not sleep with the infant, the risks associated with parental smoking are comparatively small.
Alcohol and drugs
Table 2 also shows the AORs associated with the mother having had 2 or more units of alcohol in the last 24 h. If the baby does not bed share, having 2 or more units increases the risk nearly fivefold in contrast to a very substantial increase in risk when bed sharing, especially in the first weeks of life (AOR at 2 weeks of age=89.7). The use of any illegal drugs by the mother, including cannabis, increases the risk 11-fold even when the baby is room sharing. The risks associated with a drug using mother bed sharing are unquantifiably large.
Average ORs for the first 3 months and after
In view of the trends in the AORs associated with bed sharing and age, table 3 tabulates the average under and over 3 months AORs for two key factors, smoking and alcohol, when room sharing and bed sharing. These adjusted ORs apply when no other risk factors are present and the baseline risk group is breast-fed baby girls placed on their back for sleep by the bed of non-smoking parents having no other risk factors. Table 3 shows that if this group with a baseline risk bed share, their average risk for the first 3 months, AOR is 5.1 (2.3 to 11.4). After the infant is 3 months old, the corresponding average AOR is 1.0 (0.3 to 3.0).
Average AORs for smoking and maternal alcohol when room sharing and bed sharing with the multiplicative increase in risk due to bed sharing, for infants aged under 3 months and 3 months up to a year
The multipliers shown in the last column show the ratio of the AORs when bed sharing to the corresponding AOR when room sharing. Insofar as these multipliers are >5.1 for the under 3 months, and >1 after that age, they show that the interaction, first of smoking and then of parental smoking plus maternal alcohol with bed sharing, greatly enhances the risk associated with bed sharing. The data are too sparse to give meaningful AORs when the mother is a drug user. It will also be noted that the second largest increase in risk associated with bed sharing occurs when the baby is under 3 months and the mother smoked.
Calculation of AORs for other risk groups
Because AORs multiply in the absence of interaction, tables 1–3 enable approximateii AORs to be calculated for almost all other risk groups. Thus, at 2 weeks, if the baby is not breastfed but bottle fed, table 1 shows that the AOR is multiplied by 1.5; if the baby's birth weight is between 2000 and 2499 g, the AOR is scaled up by 4.2, and so on. Thus, at 2 weeks, for a bottle-fed baby boy with birth weight 2140 g who bed shares with a cohabiting 21-year-old mother with one previous child and both parents smoke, the
 Using table 2, if we replace 65.1 with 2.9, we find that this alarming figure drops to 202 for parents who did not bed share. By changing the first AOR from 65.1 to 21.8, we find the average AOR for this child for the first 3 months to be approximately 1516, again reducing to an average of 202 if the baby did not bed share but is placed supine for sleep on a cot in the parents’ room.
Using table 2, if we replace 65.1 with 2.9, we find that this alarming figure drops to 202 for parents who did not bed share. By changing the first AOR from 65.1 to 21.8, we find the average AOR for this child for the first 3 months to be approximately 1516, again reducing to an average of 202 if the baby did not bed share but is placed supine for sleep on a cot in the parents’ room.
These alarming AORs show how the effect of multiple risk factors builds up, and indicates that infants with multiple risk factors are likely to be at a far greater risk than is generally supposed.
Fraction of deaths while bed sharing attributable to bed sharing
In this combined dataset, 22% (n=323) of the deaths occurred while bed sharing; 66% (n = 212) of these were under the age of 3 months. Overall, 87.7% (86.3% to 89.2%) were attributable to bed sharing, assuming that they would otherwise have been placed on their back on a cot in the parents’ room. This rises to 89.5% (88.8% to 90.3%) for bed sharing deaths under 3 months of age.
Comparison of SIDS rates
To get an overview of the absolute risks and increases in risk associated with bed sharing, SIDS death rates for infants (ie, ages 0 up to 1 year) when room sharing or bed sharing are estimated and tabulated in table 4 for six combinations of risk factors. In addition, table 4 also shows the ratio of SIDS rates for bed sharing compared with room sharing. These SIDS rates have been calculated by assuming that the population SIDS rate is 0.5/1000 live births and apply to a typical cohabiting white mother aged 26–30 having a second normal weight baby with birth weight between 2.5 and 3.5 kg—the most common situation of a mother completing her family.
Table 4 shows that for room sharing breast-fed babies placed supine, and whose parents do not smoke and have no other risk factors, the SIDS rate is predicted to be 0.08 (0.05 to 0.14)/1000 live-births. This rate is predicted to increase by 2.7 times (1.4 to 5.3) to 0.23 (0.11 to 0.49)/1000 when bed sharing. For all combinations of risk factors, the predicted increases in risk associated with bed sharing are statistically significant. These rates may be scaled up or down depending on the population SIDS rate, and other factors present; see online supplementary appendix for details. For example, from tables 1 and 4, we find that a 2.25 kg bottle-fed baby bed sharing with an 18-year-old mother, who smokes and regularly takes 2+ units of alcohol and whose partner also smokes, has a predicted SIDS rate of 125/1000, that is, 12.5% (see online supplementary table b) in online supplementary appendix.
Predicted SIDS Infant death rates for normal women*
Discussion
Mitchell21 recently reviewed the risks and benefits of bed sharing; he concluded that the postulated benefits and guidelines for bed sharing safely are not evidence based. He also found that there is only one small group with no increased risk of SIDS when bed sharing, namely breast-fed infants over 3 months whose parents do not smoke, and whose mother does not take 2 or more units of alcohol or drugs and does not cosleep on a sofa. Mitchell urged that parents had a right to know the risks they are exposing their infants to when bed sharing, but was unable to quantify these risks.
This study combines five major SIDS case–control studies. It includes 1472 cases and 4679 controls, making it the largest study of SIDS risk factors with individual level data. By combining individual data, this design allows the interaction of risk factors such as breastfeeding, infant age and smoking to be examined in relation to bed sharing and SIDS. Accordingly, it is able to examine the interplay of the risk factors related to bed sharing in depth as never before. Our findings confirm Mitchell's conclusions and quantify the relative risks and predicted SIDS rates associated with bed sharing in a variety of circumstances.
It has been suggested that we should have taken into account the partner's alcohol consumption in the last 24 h and his drug use. We did not include the former factor because, in the analysis of the ECAS study, it was found that the partner's consumption of alcohol was correlated with that of the mother and did not add further to the risk of SIDS.7 To check on this possibility, we have gone back to the original records for the key subgroup, namely babies <3 months who were breastfed and whose parents did not smoke and whose mother took less than 2 units of alcohol in the last 24 h and did not use drugs, who either bed shared or room shared. We find that in both the bed sharing and room sharing groups, the control partners had taken slightly more alcohol in the last 24 h than the partners of cases. Consequently, if we adjusted for this factor, it would increase the OR for bed sharing. We also note that the subgroup OR based on the complete data is 5.6 (1.6 to 20.3), which is almost identical to the adjusted AOR for this group 5.1 (2.3 to 11.4: table 3).
To respond to the criticism that the missing data in relation to alcohol and drug use in three of the five datasets make any attempt to exclude the contribution of these factors to the risks associated with bed sharing completely unreliable, we have gone back to the original records for bed sharing cases in the key subgroup. Most of these records include pertinent questions on alcohol use, but not maternal use, in the last 24 h. This enabled us to establish that neither alcohol nor drug use contributed in any way to any of these deaths.
Also, as discussed in more detail in the online supplementary appendix, because missing data are primarily determined by the study; by including a ‘study’ when modelling the subset of complete data and modelling the imputed data, the results of both will be essentially unbiased. In this setting, multiple imputations are expected primarily to recover information by including the partially observed records in the analysis, which is what we found. Consequently, we can be confident of our estimate of the adjusted effect of bed sharing from the imputed data.
Importantly, the combined data have enabled the demonstration of increased relative risk associated with bed sharing when the baby is breastfed and neither parent smokes and no other risk factors are present (see figure 2 and table 2). The average risk is in the first 3 months and is 5.1 (2.3 to 11.4) times greater than if the baby is put to sleep supine on a cot in the parents’ room (table 3). This increased risk is unlikely to be due to chance (p=0.000059). Bias could occur because these estimates are based on models fitted to all the data or to all the data relating to infants under 3 months of age. Moreover, checks show that the models accurately describe the data, especially those relating to cases whose only risk factor is bed sharing; see online supplementary appendix. Bias is also possible due to the selection of the studies. However, the present study incorporates far more data than were included in Vennemann et al's26 recent meta-analysis of the ORs for bed sharing in infants of non-smoking mothers. The meta-analysis produced summary ORs that were very similar to those reported in this study. Furthermore, our findings are very unlikely to be due to confounding since the AORs are adjusted for all the major SIDS risk factors. Although the partner's consumption of alcohol is not included in the dataset, it was found in the ECAS study that this factor was correlated with mother's alcohol consumption (r=0.52) and, after taking account of the mother's alcohol consumption, it did not add further to the prediction of risk.7
Mitchell's21 review of the mechanisms by which bed sharing might cause SIDS shows that a causal pathway is not unreasonable. Box 1 reviews the evidence that the association of bed sharing, when mothers do not smoke, have not taken alcohol or use drugs, with SIDS is causal by Bradford Hill's criteria.31 Clearly, bed sharing in the white European context can be a causal factor for SIDS, especially in the first 3 months in the absence of other factors. It has been argued that because the risk of bed sharing is greatly increased by parental smoking, alcohol and/or drugs, it is the way we bed share rather than bed sharing itself that is important. Parental smoking greatly enhances the risk of SIDS associated with bed sharing, but in what way their pattern of bed sharing differs from that of non-smokers is not obvious. Although breastfeeding is lower among smokers than non-smokers, 46% of cases of bed sharing smokers were breastfeeding and 61% of controls. These figures are lower than for non-smokers, 62% and 73%, respectively, but these differences do not demonstrate that parental smoking results in a different way of bed sharing. For non-smokers and smokers alike, sleeping in a ‘western style’ bed with a baby carries a risk of SIDS. Why the risk is so greatly enhanced by parental smoking is not known.
Assessment of bed sharing, in the absence of parental smoking alcohol and maternal drug use, as a causal risk for SIDS by Bradford Hill's criteria31
-
Strength of association
-
Adjusted Odds Ratio (AOR) for bed sharing=2.7 (95% CI 1.4 to 5.3), p=0.0027, for breastfed infants with no other risk factors. AOR for the first 3 months of life=5.1 (2.3 to 11.4), p=0.00006. These AORs are moderately strong.
-
Consistent
-
Of more than 12 published studies, all but two small ones show, after multivariate adjustment, increased risk of SIDS associated with bed sharing, some combined with sofa sharing.26
-
SPECIFIC × (not an essential criterion)
-
Smoking, alcohol and drug use all have greatly increased risk when bed sharing
-
Bed sharing is associated with other causes of death, eg, Suffocation.
-
SIDS can occur in the absence of bed sharing.
-
Temporally correct
-
Bed sharing always precedes SIDS.
-
Dose response
-
New Zealand study showed risk increased with duration of bed sharing.32 Not otherwise investigated.
-
Biologically plausible
-
Bed sharing risk is greatest to youngest infants who are most vulnerable.
-
Coherence
-
The proposition that bed sharing is causally related to SIDS is coherent with theories that respiratory obstruction, re-breathing expired gases, and thermal stress (or overheating), which may also give rise to the release of lethal toxins,33 are all mechanisms leading to SIDS, in the absence of smoking, alcohol or drugs. Infants placed prone are exposed to similar hazards.
-
Direct experimental evidence ×
-
Not ethically possible.
-
Analogy
-
Overlying is a serious cause of mortality in piglets. Sows are normally separated by a bar from piglets to prevent them being crushed when she turns over, but allowing her piglets to feed.
Recently, there has been a tendency to record unexplained bed sharing infant deaths as due to ‘suffocation-bed’ (ICD code E913/W75)34 ,35 or ‘undetermined’, rather than SIDS when the baby was bed sharing and may have suffocated.36 However, an investigation into deaths certified as SIDS and unascertained by the UK Office of National Statistics found that many of their characteristics were very similar,37 and now ONS reports these deaths together as unexplained deaths in infancy.38 In 2004, Limerick and Bacon,39 in a study of terminology used by pathologists in reporting SIDS, found that when giving the cause of death of an infant found unexpectedly dead while bed sharing, only 1 in 70 said asphyxia. The selection of cases in our studies includes all such deaths. Certifying such deaths under headings other than SIDS does nothing to minimise the tragedy.
Other new findings
The risk of SIDS for an average family with no known modifiable risk factors—table 4 baseline (breast-fed, non-smoking, non-drinking parents who are room sharing and not bed sharing)–was 0.08/1000 live-births. This is the level of SIDS that might be achieved if all known modifiable risk factors were removed. Such a SIDS level may be deemed intrinsic (possibly genetic) and not directly amenable to behaviour modification. This rate is consistent with countries reporting low SIDS rates. National surveys in the Netherlands show that, following an active campaign to discourage bed sharing,4 bed sharing rates have fallen from 13% in 1999, to 10% in 2005, to 1.5% always bed sharing and 3.1% sometimes bed sharing in 2011 (M L'Hoir, Personal communication Apr, 2012). During the same period, as part of a general downward trend in SIDS mortality,40 SIDS rates have fallen by 25% from 0.12 in 2000 to 0.09/1000 in 2010.41 ,42 At the same time, the percentage of infants being breastfed at 3 months of age has risen from 45% to 52%, and at 6 months from 24% to 32%,43 confirming that promotion of bed sharing is not necessary to achieve high rates of prolonged breastfeeding.
A recent study commissioned by UNICEF44 suggests that the promotion of breastfeeding and support of breastfeeding mothers in the UK would reduce the burden of disease on the National Health Service and could thereby be cost-effective. However, if bed sharing is promoted as a means of encouraging breastfeeding, it is likely to increase the number of SIDS because AOR for bed sharing, 2.7, is nearly double that for bottle feeding, 1.5. Consequently, such an approach would be likely to increase the number of SIDS cases. If SIDS deaths are costed at more than £1.5 million each, as in the UNICEF report, the costs resulting from any increase in bed sharing would far outweigh any benefits from the increased breastfeeding rates, quite apart from the disastrous consequences for families associated with the loss of a child. To reap the benefit of increasing the breastfeeding duration and rates, the Dutch recommendations should be followed, namely: ‘To achieve maximal security for the baby and optimal availability of breastfeeding, mothers are advised to take the baby of less than 4 months of age into their bed for feeding during the night, but afterwards to place the baby on its back into his own crib, placed adjacent to the parents’ bed in the parents’ bedroom’.5
Thus, we do not suggest that babies should not be brought into the parent's bed for comfort and feeding. This has been investigated in previous studies and has not been found to be a risk factor, provided the infant is returned to his or her own cot.45 ,46 This study is concerned with the risks associated with sleeping with a baby in bed. Tables 3 and 4 of this report are designed to enable an informed choice to be made by parents as to whether the risks associated with bed sharing outweigh the postulated benefits. However, our models predict that 88% of the deaths that occurred while bed sharing would probably not have occurred had the baby been placed on its back in a cot by the parents’ bed. Even for the very low-risk breast-fed babies under 3 months of age, with no risk factors other than that they slept in their parents’ bed, the model predicts that 81% (78.9% to 82%) of the deaths could have been readily prevented in this way. One has to ask whether it is worth taking the risk, however small, of losing a baby, when it can be so easily avoided.
Previous epidemiological studies have shown that being placed on the front, prone, for sleep was a risk factor for SIDS and fulfilled similar criteria as a causal risk for SIDS; in the 1970s, OR was 2.9 (1.2 to 7.5) and in 1986 from five pooled case–control studies, OR was 3.0 (1.7 to 5.3).2 A campaign to reduce prone sleeping effectively halved the number of SIDS cases worldwide between 1990 and 2000, saving thousands of babies in the developed world. Delay in implementing an effective ‘back to sleep’ campaign is estimated to have resulted in the deaths of 10 000 infants in the UK alone.2
Recent case studies indicate that now 50% or more of SIDS cases18 ,47 occur while bed sharing in contrast to 22% in this study, table 1. In the UK, possibly due to the pro bed sharing lobby14 in the 10 years between the two studies by Blair and colleagues,46 ,18 the percentage of cases bed sharing (excluding sofa sharing) doubled and the percentage of controls bed sharing increased by 50% from 14.5% to 21.8%. Meanwhile, the crude unadjusted OR for bed sharing only changed from 2.0 to 2.2. (An adjusted OR for bed sharing is not reported for the latter study.) Our analysis estimates that 88% of bed sharing deaths are attributable to bed sharing, that is, would not have occurred had the baby not been bed sharing. The stability of the crude OR for bed sharing despite the increase in the prevalence of bed sharing suggests that our estimate of attributable risk may reasonably be applied currently. Consequently, our analysis suggests that about 90% of bed sharing SIDS deaths would not occur in the absence of bed sharing.
The current messages saying that bed sharing is dangerous only if you or your partner are smokers, have been drinking alcohol or taking drugs that make you drowsy, are very tired or the baby is premature or of low-birth weight, are not effective because many of the bed sharing deaths involve these factors. Our findings suggest that professionals and the literature should take a more definite stand against bed sharing, especially for babies under 3 months. If parents were made aware of the risks of sleeping with their baby, and room sharing were promoted, as ‘Back to Sleep’ was promoted 20 years ago, a substantial further reduction in SIDS rates could be achieved.
References
Supplementary materials
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
Files in this Data Supplement:
- Data supplement 1 - Online appendix
Footnotes
-
Contributors The first five authors played a major role in the design and analysis of their studies, and submitted data for this combined analysis. JRC and MS were responsible for imputing missing data. RGC combined and analysed the data and drafted the report. EAM advised on the analysis. All authors commented on drafts and have seen and approved the paper as submitted.
-
Funding This combined analysis and report was not grant aided. Original data collection was funded by the European Concerted Action on SIDS—The European Union and the Foundation for the Study of Infant Deaths; Irish SIDS study—Irish Department of Health and Children; New Zealand Cot Death Study—The Health Research Council of New Zealand; Scottish Cot Death Study—Scottish Cot Death Trust; German Study on Sudden Infant Death—Federal Ministry of Education and Research. The authors are indebted to these funding bodies and all those who made those studies possible.
-
Competing interests The first five authors are actively involved in SIDS and/or paediatric research. RGC is a member of the Steering Committee of the Lullaby Trust's Care of Next Infant, CONI, project for which he receives travelling expenses. The last two authors are specialists in the imputation of missing data. Melanie Smuk is funded by a PHD scholarship from the MRC Clinical Trials Unit, London. RGC is grateful to the London School of Hygiene & Tropical Medicine for the loan of a fast computer to facilitate the analysis of the imputed datasets. EAM is supported by Cure Kids. JRC was funded by the Economic and Social Research Council grant RES-063-27-0257, and follow-on funding RES 189-25-0103. We are indebted to the referees for many helpful comments.
-
Ethics approval All studies were ethically approved. Only completely anonymised data were combined for this study.
-
Provenance and peer review Not commissioned; externally peer reviewed.
-
Data sharing statement The original case–control datasets and the imputed data can only be made available to other research workers in this field, with the explicit permission of the person responsible for each dataset.
-
↵i The ECAS data set comprises a set of 20 studies, five of which were excluded due to absence of data on feeding or unwillingness to participate.
-
↵ii The AORs obtained as described here will not be precise but will be well within the CI for the best estimates, see online supplementary appendix.