Article Text

Abstract
Objective α-Linolenic acid (ALA) is considered to be a cardioprotective nutrient; however, some epidemiological studies have suggested that dietary ALA intake increases the risk of prostate cancer. The main objective was to conduct a systematic review and meta-analysis of case–control and prospective studies investigating the association between dietary ALA intake and prostate cancer risk.
Design A systematic review and meta-analysis were conducted by searching MEDLINE and EMBASE for relevant prospective and case–control studies.
Included studies We included all prospective cohort, case–control, nested case-cohort and nested case–control studies that investigated the effect of dietary ALA intake on the incidence (or diagnosis) of prostate cancer and provided relative risk (RR), HR or OR estimates.
Primary outcome measure Data were pooled using the generic inverse variance method with a random effects model from studies that compared the highest ALA quantile with the lowest ALA quantile. Risk estimates were expressed as RR with 95% CIs. Heterogeneity was assessed by χ2 and quantified by I2.
Results Data from five prospective and seven case–control studies were pooled. The overall RR estimate showed ALA intake to be positively but non-significantly associated with prostate cancer risk (1.08 (0.90 to 1.29), p=0.40; I2=85%), but the interpretation was complicated by evidence of heterogeneity not explained by study design. A weak, non-significant protective effect of ALA intake on prostate cancer risk in the prospective studies became significant (0.91 (0.83 to 0.99), p=0.02) without evidence of heterogeneity (I2=8%, p=0.35) on removal of one study during sensitivity analyses.
Conclusions This analysis failed to confirm an association between dietary ALA intake and prostate cancer risk. Larger and longer observational and interventional studies are needed to define the role of ALA and prostate cancer.
- Nutrition & Dietetics
- Preventive Medicine
This is an open-access article distributed under the terms of the Creative Commons Attribution Non-commercial License, which permits use, distribution, and reproduction in any medium, provided the original work is properly cited, the use is non commercial and is otherwise in compliance with the license. See: http://creativecommons.org/licenses/by-nc/3.0/ and http://creativecommons.org/licenses/by-nc/3.0/legalcode
Statistics from Altmetric.com
Article summary
Article focus
-
α-Linolenic acid (ALA) is considered to be a cardioprotective nutrient; however, some epidemiological studies have suggested that dietary ALA intake increases the risk of prostate cancer.
-
A systematic review and meta-analysis of case–control and prospective studies were conducted to investigate the association between dietary ALA intake and prostate cancer risk.
Key messages
-
The present meta-analysis of 12 observational studies (7 case–control and 5 prospective) comparing the highest with the lowest categories of dietary ALA intake demonstrated no significant association between ALA intake and risk of prostate cancer overall.
-
The subgroup analysis of case–control studies alone showed a positive non-significant association, but with substantial heterogeneity. However, after removal of the studies, which reported large ORs, the association became non-significantly protective with decreased heterogeneity. The reasons for this result may be explained by the differing sources of ALA.
-
The subgroup analysis of prospective studies alone showed a protective non-significant association, but with substantial heterogeneity. However, removal of the study by Giovannucci et al21 eliminated heterogeneity and the association became significantly protective.
Strengths and limitations of this study
-
This meta-analysis includes both prospective and case–control studies to determine the effect of ALA on prostate cancer.
-
Possible confounders and sources of heterogeneity were discussed and explored in relation to the results.
-
Interpretation of analyses was complicated by considerable heterogeneity among the studies, which may be due to the lack of randomised controlled trials, variation in ALA sources and dietary patterns, variation in ALA exposure levels, differences in FFQs and food databases, variation in adjustment factors, follow-up duration and study design.
Introduction
Prostate cancer is the second most common cancer in men worldwide.1 Prostate cancer incidence rates vary widely among countries, populations and races. The incidence rates vary by more than 25-fold worldwide, with the highest rates documented in the developed countries of North America, Europe and Oceania, which may be largely due to the wide utilisation of prostate-specific antigen (PSA) testing that detects clinically important tumours that might otherwise escape diagnosis.2 In contrast, men of African descent in the Caribbean region have the highest prostate cancer death rates in the world,2 which is thought to reflect partly a difference in genetic susceptibility.3 ,4 The large differences in prostate cancer incidence rates have led to many migration and ecological studies, which have provided strong evidence for the role of environmental factors, such as diet, in the aetiology of prostate cancer.5–14 Armstrong and Doll12 first hypothesised that there was an association between dietary fat and death from prostate cancer, and many studies have examined this connection,15–18 but in recent years more attention has been focused on specific fatty acids. Several studies have examined the association between polyunsaturated fatty acids (PUFAs) and the risk of prostate cancer.19–25 There has been particular interest in α-linolenic acid (ALA), the parent fatty acid for the ω-3 PUFAs, since increased consumption of ω-3 fatty acids is advised for cardiovascular disease risk reduction26–29 despite a possible association with prostate cancer.30
Dietary ALA occurs mainly in plants and vegetable oils with certain seed oils (flaxseed, perilla, chia seed and canola), beans (soya beans and navy beans) and nuts (walnuts) singled out as examples of healthy foods due to their high ALA content.31 However, in the USA, the important sources of ALA are animal-based foods high in saturated fats, such as red meat, beef, pork and lamb, rather than ALA-rich vegetable sources, such as walnuts.25 The largest proportion of ALA (53.8%) comes from red meat in Uruguay,32 but from margarine (25%) in the Netherlands.33 Furthermore, foods such as bread, eggs and margarine are now being enriched with ALA to increase their healthfulness.
There are currently divergent health views on ALA. Numerous epidemiological34–39 and clinical studies40–42 have shown that ALA is associated with a reduction in coronary heart disease (CHD) incidence and heart disease mortality. However, since ALA has also been associated with an increased risk of prostate cancer,25 ,30 ,32 ,43–47 the seriousness of this potential association requires that any favourable effects of ALA on CHD be weighed against its possibly adverse effects on prostate cancer. Numerous prospective cohort19–22 ,24 and case–control studies32 ,45 ,48–52 have investigated the association between ALA and prostate cancer risk. While previous meta-analyses30 ,53 ,54 have been conducted to determine whether a relationship exists, there has been no meta-analysis since 2010 that has examined the specific effect of dietary ALA on prostate cancer risk and none since 2009 that included both prospective cohort and case-control studies. Therefore, it appears timely to determine whether there are associations between dietary ALA from ω-3 fatty acid-rich foods, generally believed to be healthy, and prostate cancer risk.
Methods
We followed the Cochrane handbook for systematic reviews of interventions V.5.1.0 (updated March 2011) for the planning and conduct of this meta-analysis.55 The reporting followed the QUOROM (Quality of Reporting of Meta-analyses) guidelines.56
Study selection
We first conducted a search of MEDLINE (1948 to 17 April 2009) and EMBASE (1974 to 17 April 2009) using the following search terms and Boolean operators: prostate AND (cancer OR adenoma OR adenocarcinoma OR neoplasia OR gleason score) AND (alpha-linolenic acid OR n-3 fatty acids OR omega-3 fatty acids) and this literature search was last updated on 28 August 2012. The search was restricted to human research studies. No limit was placed on language. Manual searches of references cited by the published original studies and review articles supplemented the database search strategy. We included all prospective cohort, retrospective case–control, nested case-cohort and nested case–control studies that investigated the effect of dietary ALA intake on the incidence (or diagnosis) of prostate cancer and provided relative risk (RR), HR, or OR estimates. No randomised controlled trials were identified. No lone abstracts or unpublished studies were identified. In cases where multiple publications existed for the same study, the article with the most recent information was included.
Data extraction
Two investigators (AJC, JLS) independently extracted relevant data on study characteristics and outcomes using a standardised pro forma. These data included information about study design (prospective cohort, case–control, etc), sample size and participant characteristics (nationality, race, named cohort, country of residence, gender, age, disease status and pre-existing medical conditions), follow-up duration, sources of ALA, method of ALA status assessment, end points (incidence of prostate cancer, PSA, Gleason score, etc), endpoint assessment (self-reporting, medical records, biopsy, etc) and number of new incident cases. Bounds of intake categories, quartiles or quintiles were also recorded. The RR, HR or OR with the greatest degree of control for other environmental and dietary risk factors, and their corresponding 95% CIs for incident prostate cancer risk were extracted as the main endpoint. Disagreements were reconciled by consensus and, where necessary, by discussion with another investigator (DJAJ). The authors were not contacted to request any additional information or translation.
Statistical analysis
Data were analysed using Review Manager (RevMan) V.5.1 (The Nordic Cochrane Centre, The Cochrane Collaboration, Copenhagen, Denmark) and STATA V. 11.2 (StataCorp, College Station, Texas, USA). We used the reported RR or OR of the highest versus lowest intake category as the measure of the relation between ALA intake and prostate cancer risk. The primary pooled analysis of all the reports was conducted using the Generic Inverse Variance method using random effects weighting57 where the log RRs for cohort studies or log ORs for case–control studies were weighted by the inverse of the variance to obtain a pooled RR estimate. Since nested case-cohort and nested case–control studies are temporally prospective, we analysed data from these studies with the prospective studies. As in other meta-analyses that have examined prostate cancer,30 ,54 ,58 ORs were considered as approximations of RRs. Since prostate cancer is a rare disease, ORs were treated as unbiased approximations of RRs.59 Interstudy heterogeneity was assessed by Cochrane's Q (χ2 p<0.10) and quantified by I2. An I²≥50% indicated ‘substantial’ heterogeneity and ≥75% indicated ‘considerable’ heterogeneity.60 Sources of heterogeneity were explored by sensitivity analyses whereby the influence of individual studies was investigated by systematic removal of each study followed by recalculation of the pooled effect estimate and heterogeneity, as well as removal of outlier studies with risk estimates larger than 2 SDs from the mean risk estimate and recalculation of the pooled effect estimate and heterogeneity. We also performed a priori subgroup analyses to assess effect modification by study design (prospective vs case–control). The effect modification by study characteristics was explored using meta-regression. Publication bias was formally tested using Begg's and Egger's tests.
Results
Search results
Figure 1 shows the flow of the literature selection applying the systematic search and selection strategies to identify eligible reports. Two hundred and forty-three reports were identified by the search and two reports were manually included after a database search. Of these, 233 were determined to be irrelevant on a review of the titles and abstracts, and 4 additional reports were then manually included. The remaining 16 reports were retrieved and reviewed in full, of which 4 were excluded. Results for The Health Professionals’ Follow-up Study were published in three separate publications at different times of follow-up.21 ,23 ,25 Only the most recent publication of the results, by Giovannucci et al21, was included in the analyses as representing the cumulative experience of the earlier assessments of this cohort. A total of 12 reports, 5 prospective and 7 case–control studies, were included in the pooled analyses.

Flow of the literature.
Study characteristics
Table 1 shows the characteristics of the 12 included studies, which were composed of 7 case–control studies32 ,45 ,48–52 and 5 prospective studies19–22 ,24 that used 3 designs: cohort, nested case-cohort and nested case–control. Five studies were conducted in North America, one in South America and six in Europe. The 12 included studies contained a total of 14 795 cases of prostate cancer and 231 143 controls. All studies obtained dietary data using food frequency questionnaires (FFQs). Individual and average dietary ALA intake in these studies ranged from ≈0.05 to 4.16 g/day) and the reported RR or OR of the highest versus the lowest intake category ranged from 0.7 to 3.91.
Characteristics of studies included in the meta-analysis of α-linolenic acid intake and prostate cancer
Primary analysis
The overall analysis of the 12 studies examined prostate cancer, comparing the highest ALA intake category with the lowest. Seven studies reported a protective effect of ALA intake on prostate cancer, one of which was significant, and the remaining five studies reported a positive association, of which three were significant. Overall, high exposure to ALA was not associated with increased risk of prostate cancer (pooled RR 1.08; 95% CI 0.90 to 1.29, p=0.40; figure 2). However, there was evidence of considerable interstudy heterogeneity (I2=85%, p<0.00001). The systematic removal of each study, and recalculation of the pooled effect during sensitivity analyses did not identify an influential outlier.

Pooled effect of dietary ALA intake on prostate cancer risk in case–control, nested case–control, nested case-cohort and cohort studies. Relative risk with 95% CI, study weights and pooled effect estimates were generated using the general inverse variance method with random effects models (RevMan V.5.1, Cochrane Library software, Oxford, UK). Interstudy heterogeneity was tested by Cochrane's Q (χ2) at a significance level of p<0.10 and quantified by I2, where I2≥50% is considered to be evidence of substantial heterogeneity and ≥75%, considerable heterogeneity.55 ALA, α-linolenic acid.
Subgroup analyses
Case–control studies
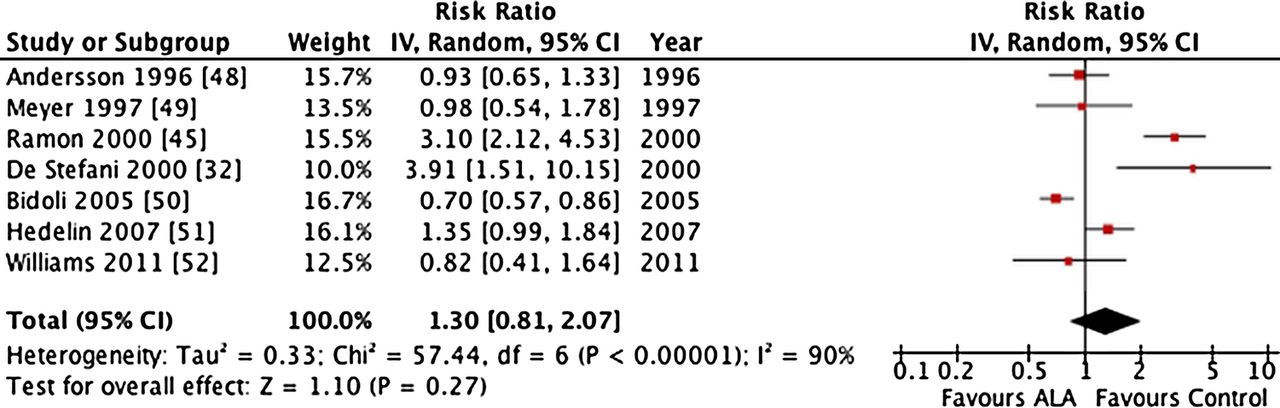
In an a priori meta-regression, we found no evidence of effect measure modification according to study design (p=0.331). There remained significant unexplained heterogeneity within each type of study design. In case–control studies (n=7; 4047 cases and 4762 controls), the summary RR was 1.30 (95% CI 0.81 to 2.07, p=0.27), with considerable interstudy heterogeneity (I2=90%, p<0.00001; figure 3). The systematic removal of each individual study during sensitivity analyses did not explain the heterogeneity. Removal of the two case–control studies by Ramon et al45 and De Stefani et al32 that reported risk estimates larger than 2 SDs from the pooled RR estimate reduced interstudy heterogeneity (I2=68%, p=0.01) but did not eliminate it. The overall association became protective, but was not significant (RR 0.93; 95% CI 0.69 to 1.25, p=0.64).

Pooled effect of dietary ALA intake on prostate cancer risk in case–control studies. Relative risk with 95% CI, study weights and pooled effect estimates were generated using the general inverse variance method with random effects models (RevMan V.5.1, Cochrane Library software, Oxford, UK). Interstudy heterogeneity was tested by Cochrane's Q (χ2) at a significance level of p<0.10 and quantified by I2, where I2≥50% is considered to be evidence of substantial heterogeneity and ≥75%, considerable heterogeneity.55 ALA, α-linolenic acid.
Prospective studies
In prospective studies alone (n=5; 10 748 cases and 207 752 controls), no association between ALA intake and prostate cancer risk was found (RR 0.95; 95% CI 0.84 to 1.09, p=0.48; figure 4) but there existed substantial interstudy heterogeneity (I2=69%, p=0.01). Sensitivity analyses showed that removal of the study by Giovannucci et al21 eliminated heterogeneity with prospective studies (I2=8%, p=0.35) and made the protective effect significant (RR 0.91; 95% CI 0.83 to 0.99, p=0.02; figure 5).

Pooled effect of dietary ALA intake on prostate cancer risk in prospective studies. Relative risk with 95% CI, study weights and pooled effect estimates were generated using the general inverse variance method with random effects models (RevMan V.5.1, Cochrane Library software, Oxford, UK). Interstudy heterogeneity was tested by Cochrane's Q (χ2) at a significance level of p<0.10 and quantified by I2, where I2≥50% is considered to be evidence of substantial heterogeneity and ≥75%, considerable heterogeneity.55 ALA, α-linolenic acid.

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Pooled effect of dietary ALA intake on prostate cancer risk in prospective studies after the systematic removal of the study by Giovannucci et al21 following a sensitivity analysis. Relative risk with 95% CI, study weights and pooled effect estimates were generated using the general inverse variance method with random effects models (RevMan V.5.1, Cochrane Library software, Oxford, UK). Interstudy heterogeneity was tested by Cochrane's Q (χ2) at a significance level of p<0.10 and quantified by I2, where I2≥50% is considered to be evidence of substantial heterogeneity and ≥75%, considerable heterogeneity.55 ALA, α-linolenic acid.
Publication bias
Neither Begg’s test (p>0.165) nor Egger’s test (p>0.527) revealed evidence of publication bias; however, one study by Ramon et al45 had an unusually large effect with a small SE.
Discussion
Summary of results
The present meta-analysis of 12 observational studies (7 case–control and 5 prospective) comparing the highest with the lowest categories of dietary ALA intake demonstrated non-significant heterogeneous effects of ALA on prostate cancer risk. Overall, there was no significant association between ALA intake and risk of prostate cancer. The subgroup analysis of case–control studies alone showed a positive non-significant association, but with substantial heterogeneity. However, after removal of the studies by De Stefani et al32 and Ramon et al,45 which reported large ORs greater than 3 but were still within 2 SDs of the mean effect, the association became non-significantly protective with decreased heterogeneity. When examining the prospective studies alone, the association between ALA intake and prostate cancer risk was non-significantly protective and, after removal of the study by Giovannucci et al,21 became weakly but significantly protective with no heterogeneity.
The results from the prospective studies are similar to those of previously published findings that examined only prospective studies.53 Our study additionally investigated the association between dietary ALA intake and prostate cancer risk among case–control studies and reached the conclusion of non-significantly increased risk with high heterogeneity, particularly because of the inclusion of two studies with very high ORs. We explore whether these heterogeneous results can be explained by a number of factors, such as the variation in ALA consumption, sources or population dietary patterns. However, this heterogeneity among the case–control studies may serve to highlight the less reliable nature of case–control study design as it inherently involves recall bias since dietary information is collected after disease development.
Heterogeneity and the effect of ALA between studies
In our study, different findings were reviewed and interstudy heterogeneity may be explained by a number of factors: variation in ALA consumption and sources of ALA as a result of the population's dietary patterns, variation in ALA exposure levels, use of different FFQs and food databases, variation in adjustment factors, and difference in follow-up times among prospective studies.
Variation in ALA consumption and sources, and population dietary patterns
In the Netherlands, the chief sources of ALA include margarine (25% of daily intake), meat (11%), bread (10%) and vegetables (8%),33 whereas in the USA, major sources of ALA come from mayonnaise, creamy salad dressings, margarine, butter, beef, pork, lamb and oil and vinegar-based dressings.25 Interestingly, the prospective study from the Netherlands reported a weak protective effect of ALA intake on prostate cancer risk,20 but the most recent study from the USA reported a 25% increase in risk.21 This difference may be due to the nature of the foods that contain ALA since, in the USA, the sources of ALA are not the ‘healthy’ sources where ALA is naturally found (eg, flaxseed, walnuts and canola oil), but rather profile an unhealthy diet (eg, canola oil in the form of mayonnaise and creamy salad dressings), which may be indicative of a less healthy lifestyle, and this in itself may contribute to an increased risk of prostate cancer independent of ALA intake levels.61 ,62
In addition, case–control studies from Uruguay32 and Spain,45 which showed the largest increases in prostate cancer risk, demonstrated that meat, and not vegetable, was the major source of ALA. When these two studies were removed from the analysis of the case–control studies, the effect of ALA intake on prostate cancer changed from a non-significantly positive effect to a non-significantly protective effect. Compared with the other studies from Europe and the USA, there is a much higher consumption of meat in Spain63 and Uruguay, with Uruguay having the highest meat consumption per capita in the world.64 An earlier analysis of the Health Professionals Follow-up Study cohort25 supports this positive association between red meat consumption and prostate cancer risk. Furthermore, the two studies from Spanish-speaking countries also investigated the effect of animal fat on prostate cancer and both found significant positive associations. The Uruguayan study32 observed that the highest level of ALA intake derived from animal sources, which resulted in almost three times the risk of developing prostate cancer, and the Spanish study45 revealed that the highest level of animal fat intake was associated with two times the risk. These findings indicate that high meat intake rather than high ALA may explain ALA's apparently adverse effect on prostate cancer. In further support of this idea, the study by Bidoli et al50 demonstrated a significant protective association between ALA and prostate cancer risk in an Italian population where ALA is mainly derived from olive oil65 and the diet is rich in raw vegetables50 rather than meat, profiling a more ‘healthy’ diet overall.
An explanation for the apparent association of prostate cancer incidence with vegetable sources of ALA may be that those who follow healthy lifestyles with an increased intake of ALA from plant sources, may also undergo more frequent PSA testing and therefore have early prostate cancer detection. In this respect, it has been found that higher whole grain intake was also associated with increased prostate cancer risk. However, when the frequency of PSA screening was accounted for, the association of whole grains with prostate cancer incidence disappeared.66 These studies indicate the importance of not only identifying the dietary sources of ALA, but also taking into account what the nature of the foods may indicate in terms of diet and lifestyle since these may also affect prostate cancer risk.
Variation in ALA exposure levels
Another important aspect to consider is the differing exposure levels between the studies. Each study had different cut offs for each quantile, which makes a true comparison of ALA intake exposure difficult since some studies had higher levels of ALA in their highest intake quantile than others. Further, some studies did not adequately define the absolute upper and/or lower limits of ALA intake21 ,32 ,50 and one study did not report numerical exposure levels.49 Two studies, one from Spain45 and one from the Netherlands,20 with the largest adequately defined upper and lower limits of ALA exposure ranges, paradoxically reported the second highest and the second lowest risk of developing prostate cancer, respectively. Since the studies with the greatest range of exposure do not necessarily show the greatest effects, dietary variation in the levels of exposure does not appear to explain differences among the studies, thereby making differences in dietary sources of ALA of more importance especially in relation to meat consumption in Western countries.
Variation in FFQs and food databases
In terms of utilising different FFQs and food databases, each study used a different dietary FFQ. The ALA content of processed food can vary, which can be of concern when using food databases to translate food intake into fatty acid intake. For example, the ALA content of 12 margarines available in Australia range from 0.2% to 5.9%.67
Variation in adjustment factors
Although all the studies reported adjusted RRs or ORs, the adjustment factors were not consistent among the studies. Some of the adjustment factors in these studies included age, smoking history, physical activity level, body mass index (BMI), family history of prostate cancer, history of diabetes mellitus, race, education, socioeconomic status, area of residence and intakes of total calories, fat, processed meat, fish, lycopene and vitamin E supplements. Currently, the most well-established risk factors for prostate cancer are age, family history of the disease and race/ethnicity,68 and consequently are the most important adjustment factors. Only 420–22 ,52 of the 12 included studies adjusted for all of these three factors. The studies conducted by Park et al19 and Mannisto et al24 did not adjust for age, which is by far the strongest predictor of prostate cancer incidence and death.68 A family history of prostate cancer has been shown to increase the risk of diagnosis and death, and this factor was not adjusted for in studies by Hedelin et al,51 Andersson et al48 and Mannisto et al.24 Race is a prostate cancer risk factor and prognostic factor, with African-American or black men being at increased risk, and this was not adjusted for in the studies by Bidoli et al,50 De Stefani et al,32 Ramon et al45 and Meyer et al49 The differences in adjustment among the included studies, particularly with respect to the important factors of age, family history of prostate cancer and race, could result in differences in risk estimates, thereby contributing to interstudy heterogeneity.
Variation in follow-up duration
Follow-up time may also have an effect on heterogeneity, especially since the study by Giovannucci et al21 had the longest follow-up duration (16 years). A comparison of previous prospective studies following the same cohort23 ,25 with this most recent study21 demonstrates a shift over time (total of 12 years) from a non-significant association to a significant positive association between ALA intake and prostate cancer. So it can be hypothesised that the heterogeneity induced by this study may indicate that follow-up duration is positively related to the strength of the association between ALA and prostate cancer risk. This association may relate to the development of cancer over a longer period of time and, therefore, a stronger association in the cohort between agents that may cause cancer and tumour occurrence. Alternatively, this relationship may reflect changes in diagnostic effectiveness over time.
Reasons for the lack of effect of ALA
The overall effect of ALA on prostate cancer was found to be non-significant but may result from a number of factors including ALA exposure levels that are within health guidelines, confounding from other PUFAs, and the difference in effect of ALA on prostate cancer mortality versus incidence.
The mean dietary ALA intake levels observed in these studies were all within the dietary reference intake range 1.1–1.6 g/day,69 suggesting that ALA may not increase the risk of cancer more than any other nutrient promoting cell growth. Rather, since ALA is a nutrient deficient in the Western diet,70 it may be that a deficiency inhibits all cell growth, including tumour growth, instead of adequate or excess levels causing prostate cancer growth.
Another issue to consider is confounding from other PUFAs such as ω-6 or other ω-3 fatty acids (eicosapentaenoic and docosahexaenoic fatty acids) that might affect ALA metabolism71 and consequently may introduce bias. The case–control study from the USA52 demonstrated this as there was no significant association between ALA, ω-3 or ω-6 fatty acids and prostate cancer risk individually, but the highest dietary ratio of ω-6/ω-3 fatty acids was significantly associated with increased risk of high-grade prostate cancer.
Finally, our analysis involved cancer incidence rather than mortality and ALA, among other factors such as energy intake, height, BMI, calcium and smoking, which are also associated with cancer mortality.21 The study by De Stefani et al,32 which was the only study that defined cases solely as advanced prostate cancer, had the highest risk estimate of prostate cancer, indicating that ALA may be strongly associated with disease progression rather than incidence. In support of this point, the prospective study by Giovannucci et al21 found that higher ALA intake was more strongly associated with increased risk of fatal prostate cancer than with incident. However, three other prospective studies did not find any difference between the effects of ALA on incident or advanced prostate cancer cases.19 ,20 ,22 From these mixed findings, it is unclear whether ALA is associated with severity of prostate cancer, but determining whether ALA impacts prostate cancer incidence or progression is an important distinction that should be investigated in the future. Furthermore, the picture of ALA's effect on prostate cancer is complicated by the positive association of incident prostate cancer with either serum or adipose tissue ALA levels24 ,43 ,44 ,46 ,47 ,72 despite the in vitro evidence which suggests that ALA may suppress prostate cancer cell growth.73 ,74 However, there appears to be some correlation between ALA intake and serum ALA levels. In terms of intake, Gann et al43 found that plasma ALA levels were significantly positively correlated with meat and dairy product intake, and similar to the prospective analysis from the Health Professionals Follow-up Study,25 they found that red meat was positively associated with advanced prostate cancer, whereas diary foods were not. This corroboration not only suggests a correlation between ALA intake and serum ALA levels, but also enforces the positive association between ALA from red meat and prostate cancer, as seen in the studies from Uruguay32 and Spain,45 rather than from plant foods.
Limitations
The first limitation of the meta-analysis is that all data currently available for inclusion come from epidemiological studies since there are no data from randomised controlled trials due to ethical concerns. Second, interpretation of the analyses was complicated by the evidence of considerable heterogeneity among the studies, which, as discussed above, may have resulted from differences in ALA sources and population dietary patterns, ALA exposure levels, FFQs and food databases, adjustment factors and duration of follow-up. There are also inherent limitations in the studies included based on study design. For example, there is the possibility of recall bias in case–control studies, as dietary intake information is collected after disease development.
Conclusion
In conclusion, these findings provide no clear evidence of an association between dietary ALA intake and prostate cancer risk. Further, since these observational studies can only show association between ALA intake and prostate cancer, possible causation would be difficult to establish. Therefore, additional research from epidemiological, clinical and in vitro studies is required to elucidate whether ALA has a promotional, inhibitory or no effect on prostate cancer risk and development. At present, no significant association has been found and where any support of a positive effect was seen, red meat sources have been strongly implicated. The source of ALA appears to be of importance, particularly identifying whether it is from animal or vegetable sources, as ALA may be a marker for higher meat and fat intake in some countries, both of which have been associated with increased prostate cancer risk. Attention should also be paid to the effect of ALA on prostate cancer progression to address the issues of specific vulnerability identified in the studies of Giovannucci et al21 and De Stefani et al32 However, resolving the relation of dietary ALA to prostate cancer risk through randomised controlled trials will very likely continue to be difficult due to the significant public health implications of reducing/eliminating a dietary fatty acid which is essential and has suggested heart-health benefits. Determination of the sources of fatty acids is probably of greater importance since ALA is associated in the North American diet with meat membranes and creamy salad dressings, which themselves may be markers of a suboptimal dietary pattern and lifestyle.
What this Paper Adds
ALA is considered a cardioprotective nutrient, however some epidemiological studies have suggested that dietary ALA intake increases the risk of prostate cancer. Although Carayol et al. conducted a meta-analysis on the effect of dietary ALA on prostate cancer in 2010, only prospective studies were analyzed and case-control studies were not included. Overall, we found no significant association between ALA intake and risk of prostate cancer. The results from the prospective studies were similar to those of previously published findings. However, the subgroup analysis of case control studies alone showed a positive non-significant association, but with substantial heterogeneity. The case control studies suggested an element of increased risk, which was dependent on the inclusion of two studies with very high odds ratios, the reasons for which are difficult to explain. Additional research from epidemiological, clinical, and in vitro studies are required to elucidate whether ALA has a promotional, null, or inhibitory effect on prostate cancer risk and development.
References
Footnotes
-
Contributors AJC was involved in the conception and design, analysis and interpretation of data, drafting the manuscript and revising it critically for important intellectual content, and final approval of the version to be published. JLS was involved in the conception and design, analysis and revising the manuscript critically for important intellectual content. RDS was involved in revising the manuscript critically for important intellectual content. GME was involved in the conception and design and revising the manuscript critically for important intellectual content. DJAJ was involved in the conception and design, revising the manuscript critically for important intellectual content and final approval of the version to be published.
-
Funding DJAJ received research grants from Saskatchewan Pulse Growers, the Agricultural Bioproducts Innovation Program (ABIP) through the Pulse Research Network (PURENet), Advanced Food Materials Network (AFMNet), Loblaw, Unilever, Barilla, Almond Board of California, Coca-Cola, Solae, Haine Celestial, Sanitarium Company, Orafti, International Tree Nut Council Nutrition Research and Education Foundation and the Peanut Institute, the Canola and Flax Councils of Canada, Calorie Control Council, Canadian Institutes of Health Research, Canada Foundation for Innovation, and the Ontario Research Fund; and received travel support to meetings from the Solae, Sanitarium Company, Orafti, AFMNet, Coca-Cola, The Canola and Flax Councils of Canada, Oldways Preservation Trust, Kellogg's, Quaker Oats, Griffin Hospital, Abbott Laboratories, Dean Foods, the California Strawberry Commission, American Peanut Council, Herbal Life International, Nutritional Fundamental for Health, Metagenics, Bayer Consumer Care, AAFC, CAPI, Pepsi, Almond Board of California, Unilever, Alpro Foundation, International Tree Nut Council, Barilla, Pulse Canada, and the Saskatchewan Pulse Growers.
-
Competing interests DJAJ has served on the Scientific Advisory Board of Sanitarium Company, Agri-Culture and Agri-Food Canada (AAFC), Canadian Agriculture Policy Institute (CAPI), California Strawberry Commission, Loblaw Supermarket, Herbal Life International, Nutritional Fundamental for Health, Pacific Health Laboratories, Metagenics, Bayer Consumer Care, Orafti, Dean Foods, Kellogg's, Quaker Oats, Procter & Gamble, Coca-Cola, NuVal Griffin Hospital, Abbott, Pulse Canada, Saskatchewan Pulse Growers, and Canola Council of Canada; received honoraria for scientific advice from Sanitarium Company, Orafti, the Almond Board of California, the American Peanut Council, International Tree Nut Council Nutrition Research and Education Foundation and the Peanut Institute, Herbal Life International, Pacific Health Laboratories, Nutritional Fundamental for Health, Barilla, Metagenics, Bayer Consumer Care, Unilever Canada and Netherlands, Solae, Oldways, Kellogg's, Quaker Oats, Procter & Gamble, Coca-Cola, NuVal Griffin Hospital, Abbott, Canola Council of Canada, Dean Foods, California Strawberry Commission, Haine Celestial, Pepsi, and Alpro Foundation; has been on the speakers panel for the Almond Board of California.
-
Provenance and peer review Not commissioned; externally peer reviewed.
-
Data sharing statement No additional data are available.