Article Text

Abstract
Introduction Acute myocardial infarction (AMI) is a major cause of death and disability in the UK and worldwide. Presently, timely and effective reperfusion with primary percutaneous coronary intervention (PPCI) remains the most effective treatment strategy for limiting infarct size, preserving left ventricular ejection fraction (LVEF) and improving clinical outcomes. However, the process of reperfusion can itself induce cardiomyocyte death, known as myocardial reperfusion injury, for which there is currently no effective therapy. Extensive preclinical evidence exists to suggest that sodium nitrite (as a source of endogenous nitric oxide) is an effective therapeutic strategy for preventing myocardial reperfusion injury. The purpose of NITRITE-AMI is to test whether sodium nitrite reduces reperfusion injury and subsequent infarct size in patients undergoing PPCI for MI.
Methods and design NITRITE-AMI is a double-blind, randomised, single-centre, placebo-controlled trial to determine whether intracoronary nitrite injection reduces infarct size in patients with myocardial infarction undergoing primary angioplasty. The study will enrol 80 patients presenting with ST-elevation myocardial infarction. Patients will be randomised to receive either a bolus of intracoronary sodium nitrite or placebo (sodium chloride) at the time of PPCI. The primary outcome is infarct size assessed by creatine kinase area under the curve (AUC) over 48 h. Secondary endpoints include troponin T AUC and infarct size, LV dimensions and myocardial salvage index assessed by cardiac MR (CMR), markers of platelet reactivity and inflammation, the safety and tolerability of intracoronary nitrite, and 1 year major adverse cardiac events.
Ethics and dissemination The study is approved by the local ethics committee (NRES Committee London West London: 11/LO/1500) and by the Medicines and Healthcare Products Regulatory Agency (MHRA) (EudraCT nr. 2010-022460-12). The results of the trial will be published according to the CONSORT statement and will be presented at conferences and reported in peer-reviewed journals.
Trial registration United Kingdom Clinical Research Network (Study ID 12117), http://clinicaltrials.gov (NCT01584453) and Current Controlled Trials (ISRCTN:38736987).
This is an open-access article distributed under the terms of the Creative Commons Attribution Non-commercial License, which permits use, distribution, and reproduction in any medium, provided the original work is properly cited, the use is non commercial and is otherwise in compliance with the license. See: http://creativecommons.org/licenses/by-nc/3.0/ and http://creativecommons.org/licenses/by-nc/3.0/legalcode
Statistics from Altmetric.com
Article summary
Article focus
-
This article describes the study protocol of the first-in-man study assessing the safety and efficacy of intracoronary nitrite infusion during primary percutaneous coronary intervention (PPCI) for acute myocardial infarction (AMI) in a randomised double-blind placebo-controlled trial.
Key messages
-
Despite the introduction of PPCI for treatment of AMI significant morbidity and mortality rates remain, mainly because of reperfusion injury contributing to infarct size.
-
Reducing reperfusion injury is a major target in improving these outcomes.
-
There is extensive preclinical data demonstrating efficacy of sodium nitrite (delivered locally) in reducing reperfusion injury and subsequent infarct size.
Strengths and limitations of the study
-
This is the first randomised-controlled trial assessing the use of intracoronary nitrite to reduce infarct size during PPCI for ST-elevation myocardial infarction.
-
It is a single-centre study, which can affect applicability of the results to other units.
Introduction
Coronary heart disease is the commonest cause of death in the UK, as a consequence of acute myocardial infarction (AMI) causing 1 in 5 and 1 in 7 deaths in men and women, respectively (http://www.heartstats.org). Presently, timely and effective reperfusion with primary percutaneous coronary intervention (PPCI) for ST-elevation myocardial infarction (STEMI) remains the most effective treatment strategy for reducing myocardial infarct (MI) size, preserving left ventricular ejection fraction (LVEF) and preventing the onset of heart failure.1–4 However, despite the introduction of PPCI, and other advances such as the introduction of antiplatelet therapies, resulting in a reduction in mortality of ∼50% at 30 days, substantial mortality and morbidity rates still persist.5,6 The mortality of STEMI patients at 30 days undergoing PPCI in Europe remains significant (3–7% in-hospital mortality depending on the country)7 and 15–20% of patients progress to develop heart failure.8 One of the main determinants of prognosis after AMI is the size of the infarct,9–11 and importantly increased infarct size is associated with an increased incidence of heart failure and arrhythmias.12–14 Thus, there is a clear need for identification of additional strategies that might decrease infarct size and improve outcome.
Reperfusion injury and infarct size
In the setting of STEMI the immediate reopening of acutely occluded coronary arteries via PPCI is the treatment of choice to salvage the ischaemic myocardium. However, the sudden reinitiation of blood flow leads to a local acute inflammatory response with further endothelial and myocardial damage. This phenomenon, described as ‘reperfusion injury’15 may explain why, despite optimum myocardial reperfusion, the short-term mortality after AMI approaches 7%6 and the incidence of heart failure approaches 15–20%.1 ,14 Experimental in vivo models suggest that while 50% of the final infarct size is because of the ischaemic insult the remaining 50% is because of reperfusion injury.16 Although, the process of myocardial reperfusion continues to be optimised with recent advances in PPCI technology (thrombus aspiration, novel stents),17 antiplatelet (prasugrel, ticagrelor)18 and antithrombotic therapy (bivalirudin),19 there is currently no effective therapy for reducing myocardial ischaemia-reperfusion (I/R) injury per se.
Reducing reperfusion injury
Disappointingly, while several strategies are effective in reducing I/R injury in preclinical models the majority of these approaches have not translated to the clinical setting, with the notable exception of cyclosporine.20 However, more recently a potential solution to the problem of reperfusion injury has been proposed in the form of inorganic nitrite (NO2−). Over the last decade evidence has accumulated supporting the view that NO2−, which is abundant in blood and tissues,21–24 represents a significant stable intravascular endocrine reservoir and tissue storage form of nitric oxide (NO) that exerts a number of beneficial effects.25
Inorganic nitrite
Under normal conditions, basal endogenously generated NO, produced via the conventional l-arginine/NO synthase (NOS) pathway is essential for maintaining homeostasis, particularly, by sustaining normal healthy cardiac function, perfusion and cardioprotection.26 ,27 However, during ischaemia the activity of the predominant isoform that underlies this NO synthesis, that is, endothelial nitric oxide synthase (eNOS), is severely attenuated as a result of inadequate delivery of oxygen and cofactors.28 In addition, reperfusion generates oxidative stress, which also further reduces the bioavailability of NO,29 ,30 thereby removing its cardioprotective effects. The cardioprotective effects of NO have been proposed to relate to a number of actions that combine to provide an overall beneficial profile. First, NO exerts potent vasodilator effects in the ischaemic myocardium,31 which allows for essential perfusion of injured tissue. In addition NO exerts antiinflammatory effects inhibiting leucocyte recruitment32 ,33 and thus suppressing the inflammatory cell-driven injury to the endothelium and perivascular myocardium that plays a major role in determining infarct size postmyocardial I/R injury.34 NO also exerts antiplatelet effects, which together with the antileukocyte actions of NO attenuates capillary plugging.35 Finally, deficient NO generation contributes to the delay in reendothelialisation following PPCI, enhances cardiomyocyte death and apoptosis during I/R injury, and in the long term contributes to cardiomyocyte hypertrophy postinfarct and decreases the impact of strategies that might facilitate new cardiomyocyte generation.36 ,37 Together, such preclinical observations are consistent with a protective role for NO35 and support the concept of pharmacotherapy focused on replacing the protective NO ‘lost’ during myocardial I/R injury.
Preclinical evidence for beneficial effects of nitrite
NO2− has now been shown to mediate a number of beneficial effects on the cardiovascular system. Perhaps the most potent and reproducible effect of NO2− being its ability to mediate cytoprotection after I/R in a number of organs and species.38–42 The activity of nitrite resides in its propensity for conversion to NO: the optimal conditions for which are low p2 and low pH conditions which prevail during ischaemic episodes and coincide with substantial reduction of NOS function.28 Studies from our own lab38 and those of others have demonstrated nitrite-derived NO production in the heart and blood vessels.22––24
The beneficial effects of inorganic nitrite on the heart were first demonstrated in 200438 when administration of NO2− either prior to or at reperfusion in the isolated rat Langendorff heart preparation improved both left ventricular function and coronary perfusion pressure as well as decreasing infarct size following an I/R insult. Several studies followed confirming these beneficial effects on the heart demonstrating the protective effects of nitrite administered intraventricular or intracoronary in rodent models of AMI in vitro and in vivo.38 ,39 ,43 ,44 Importantly, studies have confirmed that ischaemia-dependent conversion of NO2− to protective NO is also a property shared by human heart tissue ex vivo.38 The functional benefits of NO2− have been translated to larger species in vivo, where the intravenous administration of NO2− in just the last 5 min of a 2 h period of ischaemia in the heart, reduced infarct size by ∼50% as in dogs.45 Although, the largest body of evidence demonstrating the cytoprotective properties of NO2− has accumulated in models of MI, similar protective effects have been evidenced in other organs subject to I/R injury including the liver,39 brain40 and kidney.42 In all of these studies the beneficial effects were shown to be because of the activity of NO and were specifically associated with the local application into or on the organ of interest.
These observations clearly support investigation of the potential of NO2− in the treatment of acute STEMI, particularly where NO2− could be delivered locally before balloon inflation at the time of PPCI. The design of this study seeks to determine whether a significant improvement in infarct size and clinical outcomes can be achieved by the intracoronary injection of nitrite during PPCI.
Methods and analysis
Study design
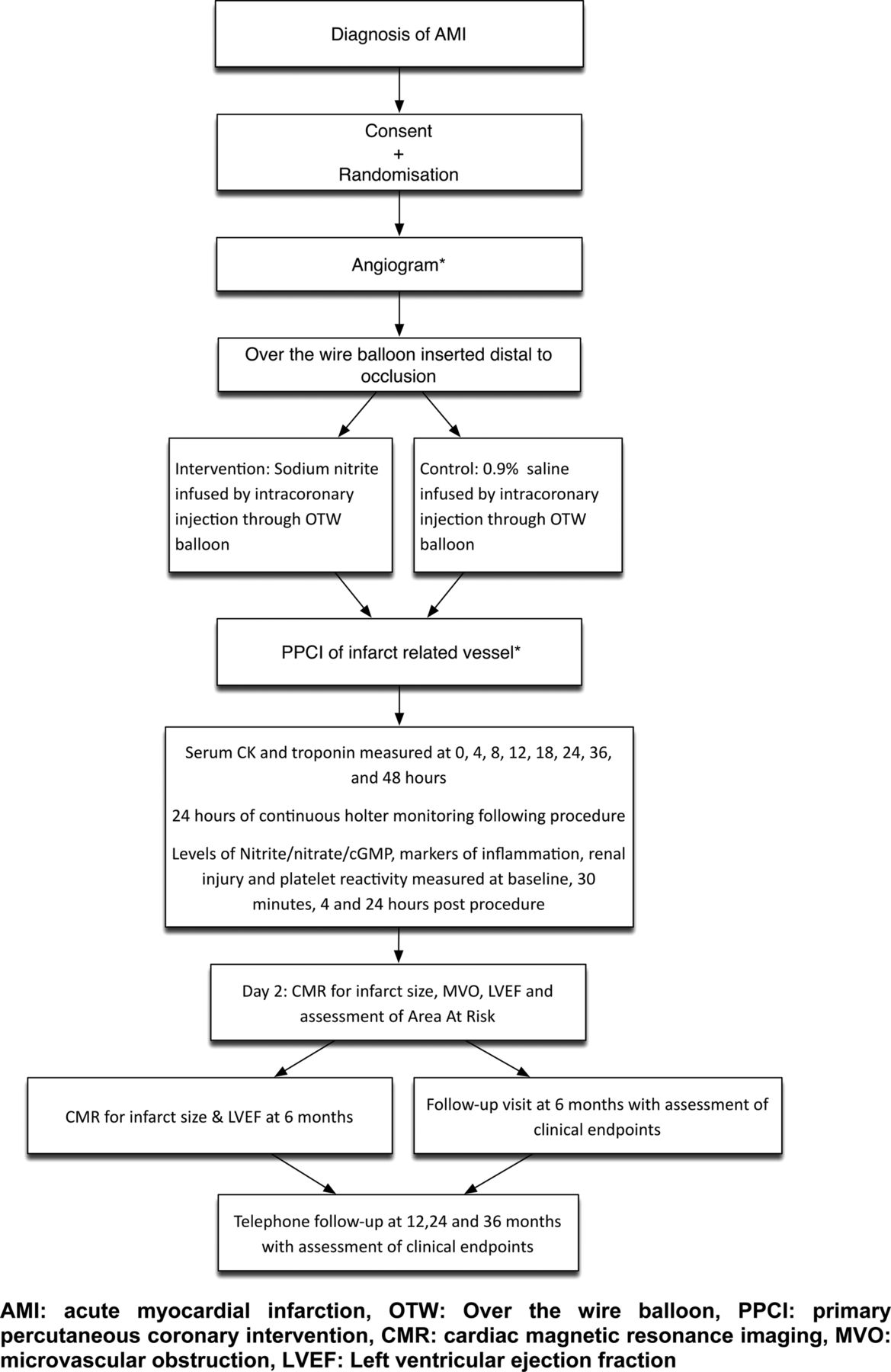
NITRITE-AMI is a double-blind, randomised, single-centre, placebo-controlled trial to determine whether nitrite injection reduces infarct size in patients with myocardial infarction undergoing primary angioplasty (figure 1).

{kind=link}
Flow diagram of study design.
Aims
-
To assess whether intracoronary nitrite is safe, tolerable and reduces infarct size during PPCI in patients with AMI.
-
To understand the effect of intracoronary nitrite on inflammatory load and platelet function during PPCI for AMI.
Hypothesis: In patients with STEMI undergoing PPCI, an intracoronary injection of nitrite initiated prior to establishment of full reperfusion reduces infarct size through prevention of I/R injury.
Study participants
This is a single-centre trial with 80 patients to be recruited at The Barts Health Heart Attack Centre, based at The London Chest Hospital. This centre runs a 24/7 heart attack care service covering a population of almost two million from the City of London to the M25 and performed 755 primary angioplasties in 2012. Haemodynamically stable patients aged between 18 and 80, presenting with STEMI, with a single culprit vessel will be recruited. Potentially eligible patients will be approached at their acute admission (box 1 for inclusion criteria and box 2 for exclusion criteria).
Inclusion criteria
-
Patients aged between 18 and 80 years
-
Acute ST-elevation myocardial infarction with ECG showing ST-segment elevation of 1 mm or more in two adjacent limb leads or 2 mm or more in at least two contiguous precordial leads or new left bundle branch block
-
Haemodynamically stable
-
Estimated symptom to balloon or aspiration time <6 h
-
Angiographically
-
Primary percutaneous coronary intervention indicated for revascularisation
-
Single epicardial artery to be treated
-
Expected ability to use over the wire balloon
-
Exclusion criteria
-
Inability to consent (including inability to speak English)
-
Patients on organic nitrate treatment (nicorandil, isosorbide mononitrate)
-
Previous history of acute myocardial infarction, systolic dysfunction or CABG
-
Patients presenting with cardiogenic shock (systolic blood pressure <80 mm Hg for >30 min, or requiring inotropes or emergency intra aortic balloon pump for hypotension treatment) or cardiopulmonary resuscitation
-
Current diagnosis of or treatment for malignancy, other than non-melanoma skin cancer
-
Current life-threatening condition other than vascular disease that may prevent a patient from completing the study
-
Use of an investigational device or investigational drug within 30 days or five half-lives (whichever is the longer) preceding the first dose of study medication
-
Patients considered unsuitable to participate by the research team (eg, owing to medical reasons, laboratory abnormalities, or patient's unwillingness to comply with all study-related procedures)
-
Severe acute infection, or significant trauma (burns, fractures)
-
Pregnancy
-
Contraindications to cardiac MR scanning
-
Pacemakers, intracranial clips or other metal implants
-
Claustrophobia
-
Renal failure (eGFR, epidermal growth factor receptor <30 m/min)
-
-
History of alcohol or drug abuse within the past 6 months
-
History of congenital methaemoglobinaemia
-
Angiographically
-
Severe vessel tortuosity, diffuse disease or severe calcification is present which may impede successful delivery of the over the wire balloon
-
Randomisation and study blinding
Patients will be randomised to receive sodium nitrite or matching placebo (in a 1:1 allocation) with both the patient and treating clinicians blinded to the assignment (double-blind). Manufacture of the investigational medicinal product, blinding, coding and randomisation will be carried out by the pharmacy manufacturing unit at Ipswich hospital prior to transfer of stock to the London Chest Hospital pharmacy. The randomisation list will be a computer-generated randomisation table (http://www.randomisation.com) based on blocks of ten to assign patients to treatment group or placebo group. Eighty indistinguishable vials of sodium nitrite and placebo will be provided and delivered to patients in a sequential fashion. Only the pharmacy at the London Chest Hospital and the manufacturing unit in Ipswich will be aware of the identity of the solution.
Intervention
The experimental intervention is a bolus of sodium nitrite solution, 1.8 μmol in 10 ml (prediluted in 0.9% sodium chloride in a syringe) which will be delivered over 30 s via intracoronary injection initiated during the re-establishment of antegrade epicardial flow with PPCI. The control intervention is a bolus of 0.9% sodium chloride solution (prepared with an identical appearance to the sodium nitrite). The patient, the PPCI operator and the assessor of clinical outcomes will be blinded to the treatment allocation.
After crossing the obstruction of the infarct-related coronary artery with a long guide wire, an over-the-wire balloon will be positioned at the level of the obstruction. The guide wire will then be removed and the sodium nitrite or placebo will be injected manually through the central lumen of the balloon catheter into the distal vascular bed over a period of 30 s. The guide wire will then be reinserted through the balloon catheter and advanced to a distal position. The procedure will then be continued as per standard practice. The intracoronary route allows for the nitrite to be delivered in an adequately high and effective local concentration with negligible effects on systemic levels (owing to its uptake locally into ischaemic myocardium, short half-life of ∼1 min and systemic dilution). The dose of 1.8 μmol is derived from clinical studies in human forearms where this dose resulted in a local concentration between 2.5 and 10 μmol/l, well within the range associated with protection in reperfusion injury.46–48
Study endpoints
Blood samples for troponin-T and creatine kinase (CK) will be taken prior to PPCI and at 4, 8, 12, 18, 24, 36 and 48 h postprocedure. Blood sample for full blood count, urea and electrolytes, liver function tests, glycosylated hemoglobin, glucose, total cholesterol, will be taken at baseline. Arterial blood gases will be taken pre-PPCI and post-PPCI to assess levels of methaemoglobin. N-terminal pro-brain natriuretic peptide will be measured at baseline and 48 h. Blood will be collected for flow cytometry assessment of inflammation and platelet reactivity at baseline, 30 min, 4 and 24 h post-PPCI. Whole blood aggregometry will be used for assessment of platelet reactivity. Plasma nitrite, nitrate and cyclic guanosine monophosphatase (cGMP) (surrogate for NO) levels will be measured at baseline, postprocedure and at 4, and 24 h post-PPCI. Cardiac MR (CMR) will be performed 2 days and 6 months after the index procedure.
The primary endpoint is myocardial infarct size, assessed by 48 h area under the curve (AUC) plasma CK levels. CK AUC is a recognised accurate estimate of infarct size49 ,50 used in multiple previous studies assessing both thrombolytic51 and mechanical reperfusion.20 Secondary endpoints include alternative measures of myocardial infarct size (48 h AUC troponin T, CMR-determined infarct size, myocardial salvage index, LV volumes, mass and ejection fraction and the presence of microvascular obstruction (MVO)), and mechanistic endpoints (plasma nitrite/cGMP) concentrations/and markers of inflammation/platelet reactivity measured at baseline, post-procedure, at 4 h and 24 h post-PPCI). Clinical endpoints include the acute safety and tolerability of intracoronary nitrite in STEMI (haemodyamics and inpatient major adverse cardiac events (MACE)), assessment of ventricular rhythm disturbance for 24 h post-PPCI and an assessment of MACE endpoints at 6 and 12 months (death, heart failure, MI, stroke, need for repeat revascularisation).
CMR imaging and analysis
CMR imaging will be performed 2 days and 6 months±2 weeks following study drug administration using a 1.5-T scanner (Philips Medical Systems, Best, the Netherlands). Each examination will use cine-CMR for ventricular volumes and function, and delayed-enhancement CMR (DE-CMR) for infarct size assessment and evaluation of MVO. Myocardial oedema will be assessed at all time points using T2-weighted triple inversion turbo spin echo STIR imaging (TE 80, TR 1667). The inversion time will be optimised to null normal myocardium. Images will be anonymised, batched and analysed in a blinded fashion by two experienced operators. Scar and oedema volumes will be calculated by manually drawing endocardial and epicardial contours followed by semiautomated selection of normal remote myocardium per slice. Myocardial oedema will be described as >2 SD in signal intensity from remote normal myocardium. Infarct size will be calculated using the full-width half maximum method as previously described.52
Myocardial salvage index
When assessing the efficacy of a reperfusion treatment strategy, it is essential to express myocardial infarct size (IS) as a percentage of the area-at-risk (AAR). In this study, the AAR will be quantified using both coronary angiography (modified Bypass Angioplasty Revascularisation Investigation (BARI)53 and modified Alberta Provincial Project for Outcome Assessment in Coronary Heart Disease (APPROACH)54 jeopardy scores) and the acute (2 day) CMR scan (infarct endocardial-surface-area (Infarct-ESA)). As a measure of the AAR, infarct-ESA has been validated against the BARI and modified APPROACH scores54 and T2-weighted imaging of myocardial oedema.55 Myocardial salvage index will be calculated according to (AAR-IS)/AAR.
Adverse events reporting
Safety analyses will summarise all adverse events (AEs), serious AEs and related unexpected serious AEs. The number of events and number of patients with events will be summarised. All serious adverse events (SAEs) that are thought to be related to treatment are subject to expedited reporting and will be reported within 24 h of study team becoming aware. The principal investigator will be responsible for follow-up of all SAEs to ensure all details are available and for reporting to the regulatory authorities.
Statistical analysis
To calculate the target sample size for the trial, we used the available database of the study of myocardial postconditioning by Staat et al56 and a recent study assessing cyclosporine11 for infarct size reduction.49 We hypothesised that nitrite would reduce the AUC for CK release by 30%, the same amount as both cyclosporine and postconditioning. For a statistical power of 80% and a probability of a type I error of 0.05 using a two-sided test, we calculated that the sample size should be 70 patients (35 per group). Since 4–8% of patients will die by the time of the primary endpoint at 6 months and 10% will either not tolerate or fail to attend the MRI at 6 months an additional 10 patients will be needed, giving a total of 80 patients.
Analysis will be based on the intention-to-treat principle. Baseline demographic and clinical variables are summarised for each arm of the study. Descriptive summaries of the distributions of continuous baseline variables will be presented in terms of percentiles (eg, median, 25th and 75th percentile), while discrete variables will be summarised in terms of frequencies and percentages. The statistical comparisons of the treatment arms with respect to the primary endpoint will be performed using the Wilcoxon rank-sum test as the principal analytic tool. All p values will be two-sided. Comparisons will be between the sodium nitrite-treated and placebo control-treated group for the primary and secondary outcomes.
Monitoring
A trial steering committee composed of three independent experts in the fields of: pharmacology, interventional cardiology and clinical trials along with the investigators will monitor the study. This will include a lay member to focus on patient issues. This committee will meet before patient recruitment and then annually to assess safety, feasibility or any other arising problems (eg, with recruitment) and their recommendations will be followed. In addition an independent Data and Safety Monitoring Committee (DSMC) will monitor patients’ safety and treatment efficacy data while the trial is ongoing. This committee is independent of the sponsor and investigators, and has no competing interests. The DSMC will meet prior to initiation of the clinical study, after the recruitment of 10 patients and then at 3 monthly intervals. The DSMC will have access to unblinded patient data. If a serious concern with the safety of the patients in the trial would arise, the DSMC may recommend early termination of the study.
Ethical considerations and dissemination
Ethical considerations
The important ethical considerations concern (1) consent in the acute setting, (2) the risk of the intervention itself and (3) any delay in door to balloon time.
-
Seeking informed consent for clinical research from patients suffering from AMI is an ethical challenge owing to the medical condition of the patients, the emergency situation and the limited time available. There is no obvious solution to the particular difficulties of informed consent in this situation, and so previously patients have been enrolled in AMI trials on the basis of more or less comprehensive consent procedures. We have addressed this by excluding patients who are unconscious, critically unstable (cardiogenic shock) or deemed unable to consent (pain, distress, language) and by also providing a clear and concise summary sheet shown to the patient during the consent process.
-
The risks from the intervention are low. Sodium and nitrite are endogenously occurring ions with no immunological potential therefore there is no risk of an allergic reaction. The small volume of 1.8 μmol in 10 ml of saline given over 30 s is very unlikely to pose any problems.
-
The delivery of the intervention (sodium nitrite) down the coronary artery will lead to a small delay in balloon inflation, however any possible delay has been minimised by
-
the guide wire may have already restored some epicardial flow before the IMP is delivered
-
nitrite will be infused through an over-the-wire balloon which can be inflated immediately after infusion restoring flow, if necessary, otherwise an export catheter will be used to aspirate thrombus first
-
the time of the infusion has been kept to 30 s meaning at most there should be a delay of 1–2 min in the door to balloon time.
-
Potential benefits
If the impressive effect of sodium nitrite on reperfusion injury does translate from animal studies to humans, this would result in smaller infarcts and potentially better functional parameters in patients treated with nitrite. If this positive outcome occurs this would pave the way for the future development of this cheap and easily manufactured substance that could be made readily and widely available to the general population in the future.
Dissemination
The study will be performed in agreement with the Declaration of Helsinki and is approved by the local ethics committee (NRES Committee London West London: 11/LO/1500). The study has also been approved by the Medicines and healthcare products Regulatory Agency (MHRA) (EudraCT nr. 2010-022460-12). Data collection will be completed by mid-2013. Primary and secondary analysis will start immediately after data monitoring is completed, publications will be prepared for submission in late 2013. The results of the trial will be published according to the CONSORT statement. Dissemination of results will focus on publications in peer-reviewed journals, presentations at national/international cardiology meetings and NHS groups. In accordance with recommendations, we have registered NITRITE-AMI with public registries, the UK Clinical Research Network (Study ID 12117), http://clinicaltrials.gov (NCT01584453) and Current Controlled Trials (International Standard Randomised Controlled Trials No: 38736987).
Summary
Experimental studies in myocardial I/R injury have demonstrated a protective effect of sodium nitrite but to date no clinical studies have been performed. The NITRITE-AMI study is a first-in-man study assessing the safety and efficacy of intracoronary nitrite infusion during acute myocardial infarction. The results of the study will set the stage for a larger trial to evaluate the safety and efficacy of sodium nitrite during STEMI.
References
Footnotes
-
Contributors All authors listed above fulfil all three International Committee of Medical Journal Editors (ICMJE) guidelines for authorship which are (1) substantial contributions to conception and design, acquisition of data or analysis and interpretation of data; (2) drafting the article or revising it critically for important intellectual content and (3) final approval of the version to be published. DAJ was responsible for coordinating the contribution of all authors to this paper. All authors made significant contributions to the development and conceptualisation of the protocol. DAJ, MA and SA were responsible for drafting this paper. AJW, RJS, AA and AM were responsible for editing and providing guidance on the paper. All authors were responsible for critically revising the paper. All authors approved the final version of this paper for submission.
-
Funding DAJ and this work are funded by an NIHR Doctoral Fellowship (DRF-2011-04-080).
-
Competing interests None.
-
Ethics approval NRES Committee London West London.
-
Provenance and peer review Not commissioned; internally peer reviewed.