Article Text

Abstract
Objective To assess the clinical usefulness of measurement of corpus callosum (CC) size in head ultrasound (HUS) to predict short-term neurodevelopmental (ND) outcomes in preterm infants. We hypothesised that including CC measurements in routine HUS will be an additional tool for early identification of infants at risk of adverse short-term ND outcome, over and above the predictive power of perinatal morbidities.
Design Retrospective cohort study.
Setting Level III neonatal intensive care unit (NICU) and outpatient NICU follow-up clinic of an academic medical centre in New York City.
Participants 929 HUS of 502 infants with gestational age of 23–36 weeks in African-American infants were initially studied. Exclusion criteria included those who died, had gross abnormalities in HUS, infants with race other than African-American, infants with suboptimal quality of HUS, late preterm infants and infants who did not participate in ND follow-up. A total of 173 infants completed the study.
Interventions CC size (length and thickness) was measured in a subset of 87 infants who had routine HUS between 23 and 29 weeks (0–6 postnatal weeks). Relevant clinical variables were collected from chart reviews. ND assessments were completed in outpatient follow-up clinics. A statistical model was developed to assess the clinical utility and possible predictive value of CC measurements for adverse short-term ND outcome, while adjusting for perinatal morbidities.
Primary and secondary outcome measures CC size and ND status.
Results Measurements of CC size did not add substantial predictive power to predict short-term ND outcome beyond the information provided by the presence of morbidities related to prematurity.
Conclusions No association was found between morbidities related to prematurity and short-term ND outcome and CC size in preterm infants. CC measurements in HUS early in life did not have an additional value in predicting short-term ND outcome, therefore did not seem to provide further clinical utility.
- Neonatology
This is an open-access article distributed under the terms of the Creative Commons Attribution Non-commercial License, which permits use, distribution, and reproduction in any medium, provided the original work is properly cited, the use is non commercial and is otherwise in compliance with the license. See: http://creativecommons.org/licenses/by-nc/3.0/ and http://creativecommons.org/licenses/by-nc/3.0/legalcode
Statistics from Altmetric.com
Article summary
Article focus
-
Preterm infants are at increased risk for complex morbidities and adverse short-term neurodevelopmental (ND) outcome.
-
Abnormalities in corpus callosum (CC) size in neuroimaging studies in preterm infants have been linked to impaired neurodevelopment.
-
We hypothesised that including CC measurements in routine head sonograms (HUS) studies will be an additional tool for the early identification of infants at risk of adverse short-term ND outcome.
Key message
-
Adding CC measurements to HUS studies does not seem to provide further clinical utility to predict short-term ND outcome.
Strengths and limitations of this study
-
Predicting ND outcome is important for patients, families and health care providers. It is important to determine the most useful and cost-effective methods for evaluating infants at risk for adverse ND outcome.
Introduction
The increasing number and improving survival of preterm infants raises concerns regarding their neurodevelopmental (ND) outcome.1 ,2 Up to 50% of the smallest (extremely low birth weight, ELBW (≤1000 g birth weight)) and very low birth weight infants (VLBW with birth weight of ≤1500 g) may have major disabilities such as cerebral palsy (CP), sensorineural disabilities and developmental delays with behavioural and learning difficulties at a later age.3
Previous studies have shown that in neuroimaging studies, abnormalities in CC size, such as thinning of the CC, have been seen in infants who later developed CP, learning and behavioural difficulties, speech and language delays and cognitive impairment.4–6 Anderson et al7 ,8 reported slower CC growth in ELBW infants compared with their intrauterine growth rate in head ultrasound (HUS) studies. Premature infants also seem to have a slower rate of CC growth,9 ,10 which ultimately may influence CC size.
Morbidities associated with prematurity such as retinopathy of prematurity (ROP), bronchopulmonary dysplasia (BPD), patent ductus arteriosus (PDA) and sepsis may also influence brain development, and are therefore often used to predict short-term ND outcome.1–3 ,11 This study aimed to determine if CC size measurements from routine HUS may be clinically useful to predict short-term ND outcome, over and above the predictive power of perinatal morbidities.
Patient population
Clinical data and HUS imaging studies were analysed in 502 preterm infants (with 929 sonograms, 1–6 sonograms per patient) born at our institution and admitted to the neonatal intensive care unit (NICU) between 2007 and 2009, with gestational age (GA) 23–36 weeks and BW between 545 and 3150 g.
Exclusion criteria included the following patient-related issues: (A) those who died (23 infants with 65 HUS); (B) infants with race other than African-American (10 infants with 23 HUS); and (C) preterm infants >32 weeks of GA (125 infants with 139 HUS). Exclusion criteria related to methodology issues included (A) infants with suboptimal quality of HUS (43 infants with 83 HUS) and (B) infants who had gross abnormalities in the HUS, including developmental anomalies of the brain, grades III and IV intraventricular haemorrhage (IVH) and periventricular leukomalacia (17 infants with 57 HUS). This latter group of infants was excluded because the CC could not be clearly visualised and measured, and their pathologies carry their own risk for adverse short-term ND outcome. For the purpose of this study, only those with early HUS (between 23 and 29 weeks of GA or 0–6 postnatal weeks) were analysed, being 87 of the remaining 173 infants. The final study group included 173 infants <32 weeks of GA with their 304 HUS. From this cohort, a statistical model was created including a subset of 87 infants, with BW range of 545–1490 g, who had early HUS with CC measurements between 23 and 29 weeks (0–6 postnatal weeks).
Methods
The institutional review board at the State University of New York Downstate Medical Center approved this study.
The timing of HUS studies was decided by the neonatologist attending the service. HUS studies were routinely conducted between the first postnatal week of life and term (40+ weeks) age and/or prior to discharge from the NICU as part of the standard of care.
All HUS studies were performed at bedside in the NICU using an ATL 3500 ultrasound machine. The length and thickness of the body of the CC were measured in midline sagittal images by two investigators (AP and JA). The CC length was measured between the extreme margins of the genu and splenium. CC thickness was measured at one-third of this distance, as previously described by Anderson et al.7 For intra-rater reliability, both the investigators repeated CC measurements within a 2-week interval on all HUS. The investigator, AP, performed all CC measurements of 502 infants (929 HUS). For inter-rater reliability, every fourth infant’s CC measurements were performed by one of the investigators (JA), which included 247 CC measurements of 125 infants.
Clinical data including infant morbidities, results of HUS studies and ND follow-up were collected from chart reviews. Morbidities related to prematurity included BPD (need for supplemental O2 >35 weeks of GA), PDA (treated with medication and/or surgery), sepsis proven by positive culture results and ROP diagnosed by paediatric ophthalmologist. All infants’ mothers received antenatal steroid treatment, and 26 infants were from multiple births.
ND follow-up assessments were conducted in our outpatient clinic between 18 and 22 months of corrected age and included standard neurological examination, the Denver II Developmental Screening Test (DDST)12 and the Cognitive Adaptive Test/Clinical Linguistic and Auditory Milestone Scale (CAT/CLAMS)13 according to our standard of care with classification of neurodevelopmental outcome (normal vs adverse outcome) as published previously.14 Standard neurological examination was used to assess muscle tone, reflexes and central nervous system integrity. The DDST was used to assess gross motor developmental milestones, whereas the CAT/CLAMS assessed visual/fine motor problem solving and speech and language development.
Statistical analysis
Inter-rater and intra-rater agreement for the CC length and thickness were determined by intraclass correlation. We investigated if these measurements provide additional predictive power beyond a set of easily available clinical variables. Logistic regression was used to determine if CC length and thickness were associated with short-term ND outcome when adjusted for four perinatal morbidities—ROP, PDA, BPD and sepsis. In addition, all analyses were also adjusted for GA, postnatal time of HUS and gender.
The area under the curve (AUC) (area under the receiver operating characteristic (ROC) curve), as a measure of predictive performance, was used to assess the clinical usefulness of measuring CC length and thickness, beyond the information provided by GA, gender, postnatal time of the sonogram and the presence of morbidities described above. We used the method of DeLong et al15 to determine whether the improvement of the AUC after including CC measurements was statistically significant. Mann-Whitney and χ2 tests were used to compare the infants for whom the short-term ND outcome was recorded to those with missing outcome on several clinical measurements. All statistical analyses were performed with SAS V.9.2 (SAS Institute, Cary, North Carolina, USA). In all the analyses, p<0.05 was considered significant.
Results
Interobserver agreement was 0.89 and intra-rater reliability was 0.78 for measurements of CC length and thickness.
Table 1 shows the clinical variables of the 87 infants included in the study. The results of Mann-Whitney and χ2 tests showed no statistical difference between infants included and those who were excluded with regard to gender (p=0.36) and the occurrence of main morbidities was examined (BPD, p=0.26; PDA, p=0.62; sepsis, p=0.65; ROP, p=1.0). Adverse short-term ND outcome was found in 32 cases (36%) including CP (3), mild global developmental delay (4), gross motor delay (4), speech and language delay (9) and moderate/severe global developmental delay without CP (12). There was no significant difference (p=0.82) between CC measurements of those with or without adverse short-term ND outcome.
Clinical variables of infants included in the study (N=87)*
The ROC curves for the two models (with and without CC measurements) adjusted for GA, gender, postnatal age of the sonogram and the clinical variables (BPD, PDA, ROP and sepsis) are presented in figure 1. AUCs are reported by each curve. No significant difference was found between the AUCs (p=0.39).
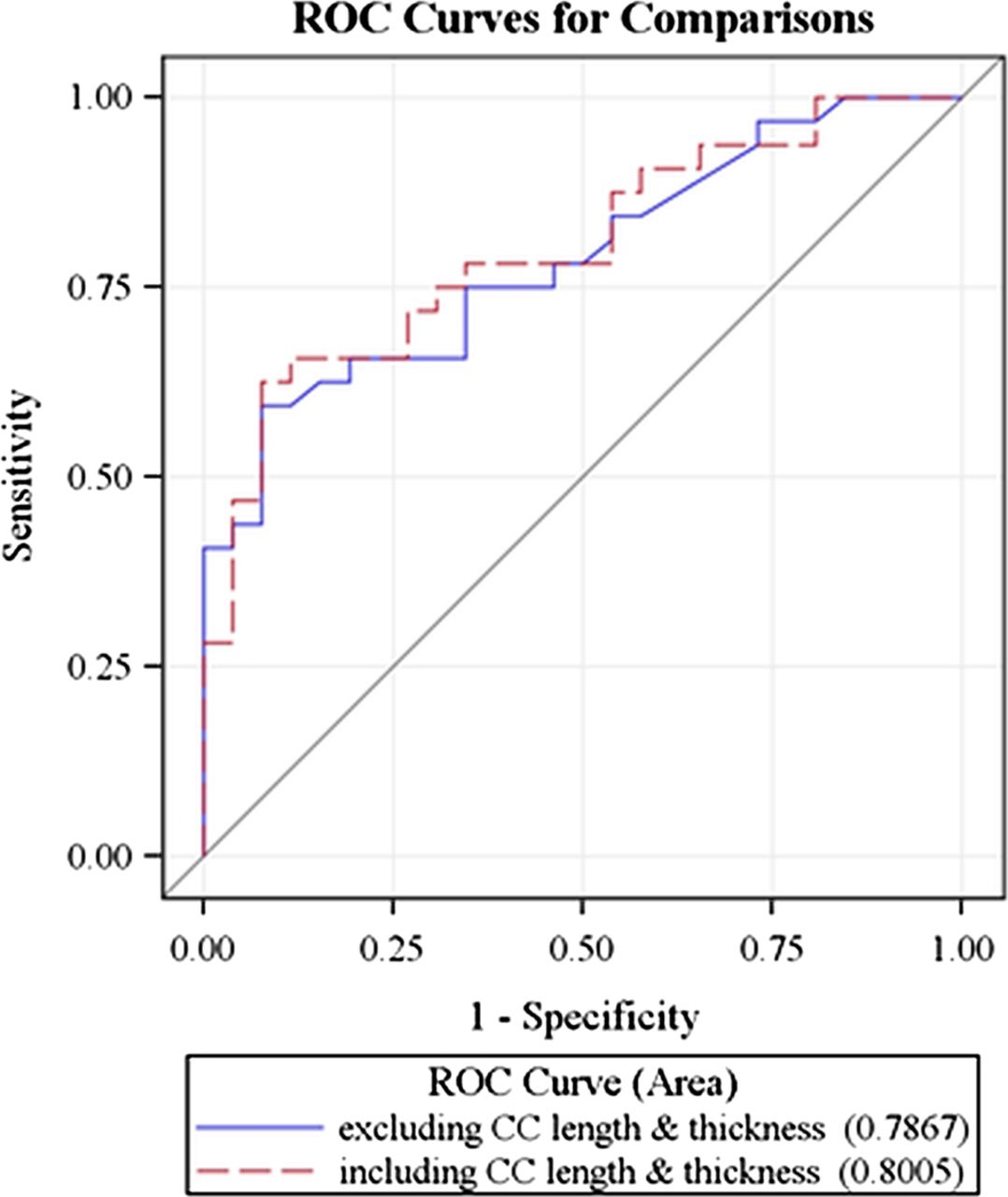
{kind=link}
Receiver operator characteristic curves, with and without corpus callosum measurements. Area under the curve (AUC) reported for each curve; no significant difference (p=0.39) between the AUCs.
Discussion
Contrary to the findings in the current study, several neuroimaging modalities including HUS and brain MRI studies described correlations with decreased CC size and adverse short-term ND outcome including gross motor impairment, cognitive skills and speech and language development.16–18 The size of the CC in various studies have been recorded in mm (length and thickness), cm3 (volume), mm2 (surface areas),19 ,20 and/or ratios, both in HUS and in MRI studies.21 ,22 Differences in measuring and imaging methods may make comparison of the results of various studies more complicated.
Alterations of the CC have been addressed by Thompson et al21 who examined VLBW infants’ neuroimaging studies using MRI, including the measurement of CC cross-sectional area at term-equivalent age. This study did not show an association between CC size and ND outcome at 2 years of age.
Cooke et al22 observed no significant correlation between ND outcome and imaging study results in their study, although CC measurements and neurodevelopmental assessment have been performed at a different age (15–19 years; long-term outcome) and by different modality (MRI) than what was found in our study.
We chose to assess CC size in HUS studies because of its portability, easy use, reproducibility of measurements and low cost. A further advantage of HUS studies is that infant sedation is not required. We analysed the data of infants between 23 and 29 weeks of GA as a subgroup in a statistical model. These most immature infants frequently have complex morbidities which influence ND outcome.
We had hypothesised that CC measurements would help to predict short-term impaired neurodevelopment based on several studies4–6 9–10 that indicate that abnormalities in CC size are related to adverse short-term ND outcome. However, using the AUC, a widely used measure of predictive performance, analysing ROC curves for comparisons, we found that early HUS studies of CC size (ie, 0–6 weeks postnatally) were not related to short-term adverse outcome.
A limitation of this study is the inclusion of a homogenous (African-American) patient population, so the results may not be applicable for infants of different race or ethnicity.
In summary, inclusion of early CC measurements in routine HUS study evaluations does not seem to have clinical utility with regard to the prediction of adverse short-term ND outcome in preterm infants. CC growth rate in HUS may be a better predictor of short-term ND outcome rather than early CC measurements as described by Anderson et al.7 ,8 Diagnostic tools other than neuroimaging studies that may predict ND outcome early in life include Prechtl's general movement assessment,23 which is incorporated into the standard of care in our ND follow-up clinic.
Acknowledgments
The authors would like to acknowledge the assistance of Jeremy C Weedon, PhD, Associate Director of the Scientific Computing Center at SUNY Downstate, in the statistical analysis of the results.
References
Footnotes
-
Contributors AP and JA conceived the idea that corpus callosum measurements in routine head sonograms performed in the neonatal intensive care unit may help to improve the identification of infants at increased risk for poor neurodevelopmental outcome. AP and JA were involved with obtaining corpus callosum measurements. JA read all sonograms as the paediatric radiologist. AP and JSK were involved with neurodevelopmental follow-up of patients. DGS as the biostatistician performed all statistical analyses. All four authors participated in the analysis and interpretation of data and drafting and revision of the article. All authors were involved in the final version of the article to be published.
-
Funding This research received no specific grant from any funding agency in the public, commercial or not-for-profit sectors.
-
Competing interests None.
-
Ethics approval State University of New York Downstate Medical Center Institutional Review Board.
-
Provenance and peer review Not commissioned; externally peer reviewed.
-
Data sharing statement No additional data are available.