Article Text

Abstract
Objectives To determine maternal and neonatal specific antibody levels to selected vaccine-preventable infections (pertussis, Haemophilus influenzae type b (Hib), tetanus and pneumococcus).
Design Prospective cohort study.
Setting A UK secondary care maternity unit (March 2011–January 2012).
Participants Mothers and infants within 72 h of delivery were eligible. Unwell individuals, mothers less than 18 years of age, and infants born at less than 36 weeks gestation, or weighing less than 2500 g, were excluded. HIV-infected mothers were included. 112 mother–infant pairs were recruited. Samples from 111 mothers and 109 infants (108 pairs) were available for analysis.
Outcome measures Specific antibody levels were determined using standard commercial ELISAs. Specific antibody to pertussis antigens (PT and FHA) of >50 IU/ml, defined as ‘positive’ by the test manufacturer, were interpreted as protective. Antitetanus antibody titres >0.1 IU/ml and anti-Hib antibody titres >1 mg/l were regarded as protective.
Results Only 17% (19/111) of women exhibited a protective antibody response against pertussis. 50% (56/111) of women had levels of antibody protective against Hib and 79% (88/111) against tetanus. There was a strong positive correlation between maternal-specific and infant-specific antibodies’ responses against pertussis (rs=0.71, p<0.001), Hib (rs=0.80, p<0.001), tetanus (rs=0.90, p<0.001) and pneumococcal capsular polysaccharide (rs=0.85, p<0.001). Only 30% (33/109) and 42% (46/109) of infants showed a protective antibody response to pertussis and Hib, respectively. Placental transfer (infant:mother ratio) of specific IgG to pertussis, Hib, pneumococcus and tetanus was significantly reduced from HIV-infected mothers to their HIV-exposed, uninfected infants (n=12 pairs) compared with HIV-uninfected mothers with HIV-unexposed infants (n=96 pairs) by 58% (<0.001), 61% (<0.001), 28% (p=0.034) and 32% (p=0.035), respectively.
Conclusions Low baseline antibody levels against pertussis in this cohort suggest the recently implemented UK maternal pertussis immunisation programme has potential to be effective.
- pertussis
This is an open-access article distributed under the terms of the Creative Commons Attribution Non-commercial License, which permits use, distribution, and reproduction in any medium, provided the original work is properly cited, the use is non commercial and is otherwise in compliance with the license. See: http://creativecommons.org/licenses/by-nc/3.0/ and http://creativecommons.org/licenses/by-nc/3.0/legalcode
Statistics from Altmetric.com
Article summary
Article focus
-
Despite renewed interest in maternal immunisation worldwide, and the recent introduction of a national maternal pertussis immunisation programme in the UK, baseline data on maternal and infant specific antibody levels to pertussis and other vaccine-preventable infections are limited.
-
Placental transfer of specific antibody from mother to infant is of key importance to antibody-mediated immunity in the first few months of life. Low maternal antibody, or reduced placental transfer, may result in suboptimal infant antibody levels, increasing vulnerability to infection in the period before primary vaccination is complete.
-
This article reports maternal and neonatal specific antibody levels to selected vaccine-preventable infections (pertussis, Haemophilus Influenzae type b (Hib), tetanus and pneumococcus) in a UK mother–infant cohort.
Key messages
-
Maternal and infant specific antibody levels against pertussis are very low in this UK cohort; this suggests the new UK maternal pertussis immunisation programme has the potential to be effective.
-
Maternal HIV infection is associated with a significant reduction in placental transfer of IgG to pertussis, Hib, pneumococcus and tetanus even in women receiving highly active antiretroviral therapy.
Strengths and limitations of this study
-
This study provides recent data on baseline levels of specific antibody in mothers and newborns to vaccine-preventable infections in a UK cohort. Our results support the recently introduced maternal pertussis immunisation programme in the UK.
-
The main limitation of our study is enrolment of a modest number of mother–infant pairs at a single centre.
Introduction
The UK is currently experiencing a dramatic increase in the numbers of cases of pertussis (whooping cough). In 2012, there were 9741 laboratory-confirmed cases of pertussis in England and Wales, almost 10 times more than in 2011 (1119 cases) or in 2008 (902 cases), the last peak year.1 The highest incidence of disease has been observed among infants less than 3 months of age, with all 14 pertussis-related deaths in 2012 observed in this age group. These infants, too young to benefit from the protection provided by routine infant vaccination, died from a potentially preventable infectious disease. In response, in September 2012, the UK Department of Health announced the introduction of a temporary maternal pertussis immunisation programme in order to protect young infants.2
A window of vulnerability, before primary vaccination is complete, is not just associated with pertussis, but equally exists for other vaccine-preventable infections where maternal antibody levels are low. The underlying principle of maternal immunisation is to boost maternal antibody levels and therefore increase the placental transfer of antibody from mother to child, potentially benefitting both mother and infant. The concept of maternal immunisation is not new; maternal tetanus immunisation, for example, has been successfully implemented in resource-limited settings for over 40 years. It has proved to be a highly effective strategy that can reduce the risk of neonatal tetanus mortality by over 90%.3
To predict the potential efficacy of any new maternal immunisation programme, it is necessary to determine population baseline levels of protective antibody in mothers and newborns. The aim of our study, undertaken prior to the new maternal pertussis immunisation programme, was to examine levels of maternal and neonatal specific antibody levels to pertussis, Haemophilus influenzae type b (Hib), pneumococcus and tetanus in a cohort of mother–infant pairs in a UK setting.
Methods
Study population and study procedures
The study was conducted between March 2011 and January 2012 at the Imperial College Healthcare NHS Trust, London, UK. The study was approved by the National Research Ethics Service, reference: 07/H0720/178. The study was funded by the National Institute for Health Research (NIHR) Biomedical Research Centre based at the Imperial College Healthcare NHS Trust and Imperial College London. Information was available to mothers in the antenatal clinic and consenting eligible women were recruited from the postnatal wards. All mothers gave written informed consent to participation for themselves and their infants. Mother–infant pairs were eligible for the study if the mother had delivered a live-born infant in the previous 72 h. Mother–infant pairs were excluded if the mother was less than 18 years of age, unwell or intending to leave the study area within the next 5 months. Infants were excluded if they were born at less than 36 weeks gestation, weighed less than 2500 g or were unwell. Maternal HIV infection was not an exclusion criterion. Consecutive eligible women were enrolled in the study, irrespective of HIV infection status.
Up to 5 ml of maternal peripheral venous blood and 1 ml of infant capillary blood were collected. All samples were collected within 72 h of delivery. Serum was separated and stored at −80°C until analysis by standard commercial ELISAs.
Laboratory assays
Specific IgG to Bordetella pertussis antigens pertussis toxin (PT) and filamentous haemagglutinin (FHA) were measured using SERION ELISA classic kits (ESR 120G, Serion Immundiagnostica GmbH, Würzburg, Germany). This assay measures antibody response to the antigens PT and FHA. Results are reported as a collective IgG response to these pertussis antigens. Limits of quantification for this assay were 10–1000 IU/ml. There is no established correlate of protection for pertussis, for either an antibody response to multiple or single antigens; however, low levels of antibody are highly correlated with susceptibility to infection.4–7 It is established in the literature that a ‘positive’ or detectable diagnostic test may be consistent with some measure of protection.8 Pertussis titres of >50 IU/ml were regarded as a positive response by the manufacturer: a pertussis IgG response >50 IU/ml was therefore interpreted as protective.
Levels of specific IgG antibodies against tetanus toxoid were determined using SERION ELISA classic kits (ESR 108G, Serion Immundiagnostica GmbH, Würzburg, Germany). Limits of quantification of the assay were 0.05–5.00 IU/ml. Tetanus antibody levels were classified as providing sufficient protection if >0.1 IU/ml.9
Hib capsular polysaccharide-specific IgG present in serum was measured using the VaccZyme Human Anti-Hib Enzyme Immunoassay kit (MK016, The Binding Site Ltd, Birmingham, England). Limits of quantification for the assay were 0.11–9.00 mg/dl. Anti-Hib antibody titres of >0.15 and >1.0 mg/l have been correlated with minimum and long-term protective immunity, respectively. Analysis was made using the higher threshold.10 ,11
Pneumococcal capsular polysaccharide (PCP)-specific IgG was measured using VaccZyme Anti-PCP Enzyme Immunoassay kits (MK012, The Binding Site Ltd). Microwells in the pneumococcal assay were supplied pre-coated with 23 polysaccharide antigens, accounting for 80% of virulent serotypes (PCP antigens 1–5, 6B, 7F, 8, 9N, 9V, 10A, 11A, 12F, 14, 15B, 17F, 18C, 19A, 19F, 20, 22F, 23F, 33F) and incorporated C-polysaccharide antibody absorption. Limits of quantification for the assay were 3.3–270.0 mg/dl. No level of protective immunity has been established for a collective response to multiple pneumococcal serotypes. A threshold value was therefore not used, but results were compared to published age-based ranges using the same assay.12
Data management and statistical analysis
Where assay results were below the lower limit of quantification an arbitrary value of half the lower limit was assigned: anti-pertussis IgG 5 IU/ml,; anti-tetanus IgG 0.025 IU/ml; anti-Hib IgG 0.05 mg/dl; anti-PCP IgG 1.65 mg/dl.
Where assay results were above the upper limit of quantification samples were retested with serial dilutions until a measurable value was obtained. This value was then multiplied according to the dilution factor to obtain the antibody level.
Statistical analyses were completed using IBM SPSS V.20 (SPSS Inc, Chicago, Illinois, USA) and GraphPad Prism V.5.04 (GraphPad Software Inc, La Jolla, California, USA). Two-sided p<0.05 was considered significant. All comparisons were prespecified. The Mann-Whitney test was used to compare geometric mean concentration (GMC) of specific IgG between groups, Spearman's Rank Order was used to assess correlations, Wilcoxon Signed-Rank test was used to compare paired samples and proportions were compared using Fisher's exact test.
Results
Study population
A total of 112 mother–infant pairs were enrolled in the study. A further 275 women were invited to participate, but declined. Reasons for non-participation were as follows: not interested in participating in any research (n=199); maternal blood sampling required (n=34); infant blood sampling required (n=34) and involvement in other research studies (n=7). There were 40 women who were unable to provide informed consent and 58 women who fulfilled the stated exclusion criteria.
A blood sample was unobtainable for one mother and three infants. The final analysis was therefore based on samples from 111 mothers and 109 infants (108 mother–infant pairs). Characteristics of the study cohort are shown in table 1.
Subject characteristics
Maternal antibodies specific for pertussis, Hib, tetanus and PCP
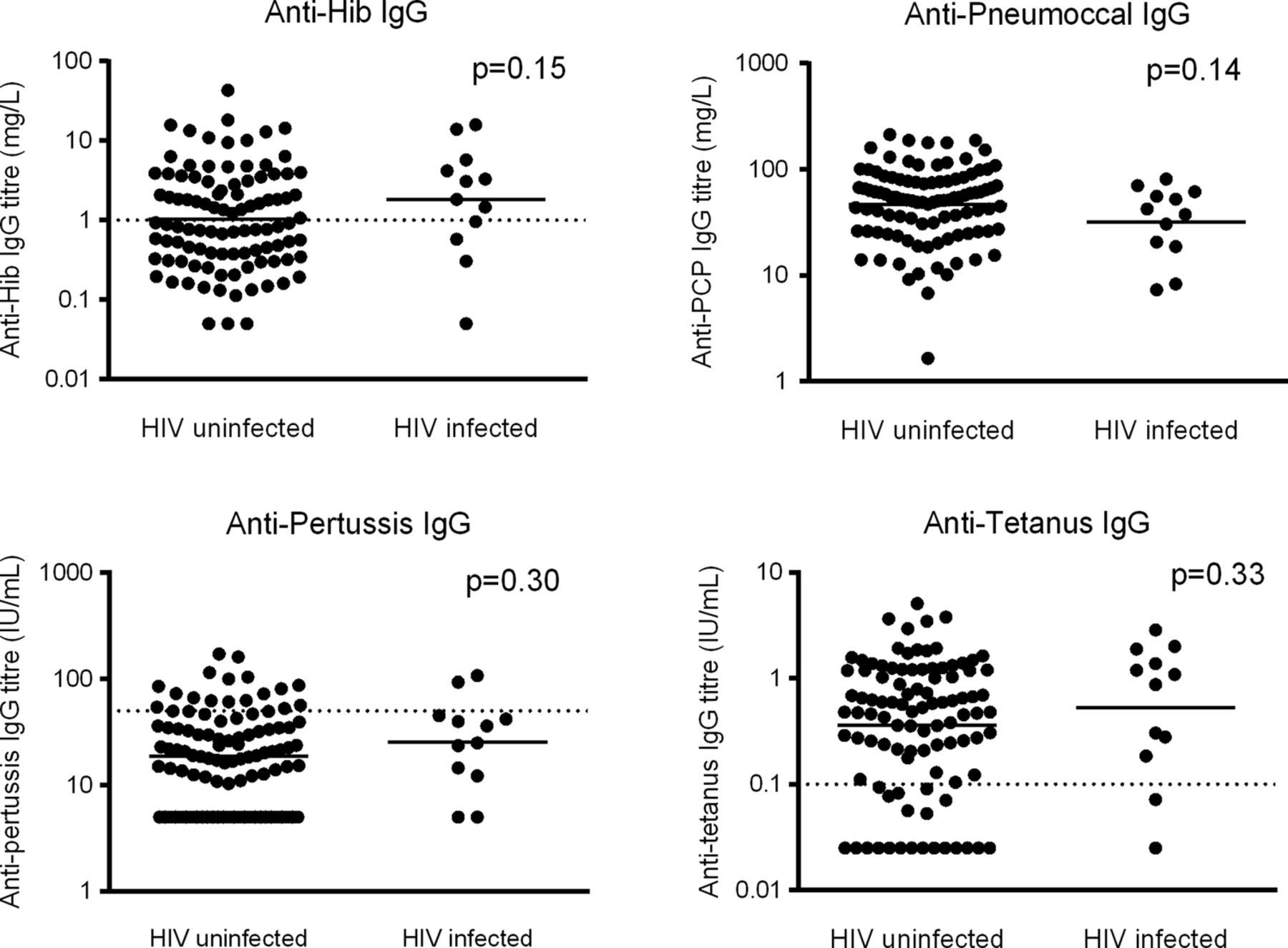
Figure 1 represents maternal specific antibodies titres. The GMC of maternal specific antibody to pertussis was 19.19 IU/ml (95% CI 15.74 to 23.41 IU/ml); only 17% (19/111) of women had a response regarded as protective. The GMC of specific IgG to Hib was 1.10 mg/l (95% CI 0.83 to 1.45 mg/l); only 50% (56/111) of women had levels of antibody likely to be associated with long-term protection. High maternal levels of anti-tetanus-specific antibody (GMC 0.38 IU/ml, 95% CI 0.29 to 0.49 IU/ml) were observed and the majority of women had levels of antibody likely to be associated with protection against tetanus (79%, 88/111). The GMC of specific antibody to PCP (23 serotypes) among mothers was 44.54 mg/l (95% CI 38.10 to 52.08 mg/l). This is within the normal adult range.12 There was no significant difference in specific antibody titres between HIV-infected and HIV uninfected women in this cohort (figure 1) and inclusion of the data from HIV-infected women in the overall analysis did not significantly alter the results (see online supplementary table S1).

Maternal specific antibody titres at time of delivery. HIV-uninfected women n=99. HIV-infected women n=12. Solid horizontal line indicates geometric mean concentration. Dotted horizontal line indicates antibody level associated with protection (where applicable). Groups compared using Mann-Whitney U test.
Association between maternal-specific and infant-specific antibody titres
There was a strong positive correlation between maternal and infant specific antibody responses for pertussis (rs=0.71, p<0.001), Hib (rs=0.80, p<0.001), tetanus (rs=0.90, p<0.001) and pneumococcus (rs=0.85, p<0.001).
Passively acquired infant specific antibodies to pertussis, Hib, tetanus and PCP at birth
In line with the correlation between maternal and infant antibody levels, newborn infants also had low levels of specific antibodies to pertussis (GMC 28.40 IU/ml, 95% CI 23.15 to 34.83 IU/ml) and Hib (GMC 0.65 mg/l, 95% CI 0.49 to 0.87; figure 2). Consequently, only 30% (33/109) and 42% (46/109) of infants had protective antibody levels to pertussis and Hib, respectively. Infant GMC of specific antibody to tetanus was 0.41 IU/ml (95% CI 0.29 to 0.57 IU/ml) and 82% (89/109) of infants had protective levels of antibody. Infant GMC of specific antibody to PCP was 42.85 mg/l (95% CI 36.63 to 50.13 mg/l), similar to the observed maternal GMC. There was a significant difference in specific antibody to pneumococcus between HIV-exposed, uninfected infants and HIV-unexposed infants, but no significant difference in any of the other specific antibodies tested (figure 2, see online supplementary table S2).

{kind=link}
{kind=link}
Infant specific antibody titres at birth. HIV-unexposed infants n=96. HIV-exposed, uninfected infants n=13. Solid horizontal line indicates geometric mean concentration. Dotted horizontal line indicates antibody level associated with protection (where applicable). Groups compared using Mann-Whitney U test. *p<0.05.
Maternal HIV-infection and specific antibody responses
Within our study cohort, we identified a group of women and infants who may be particularly vulnerable to vaccine-preventable infections by nature of maternal HIV-infection. We compared the placental transfer of antibody from HIV-infected women and their HIV-exposed, uninfected infants with placental transfer of antibody from HIV-uninfected women and their infants. All HIV-infected women had received tailored prevention of mother to child transmission (PMTCT) interventions as part of their routine care and none of their infants were vertically infected with HIV. The placental transfer of specific IgG to pertussis, Hib, pneumococcus and tetanus was significantly reduced from HIV-infected mothers to their HIV-exposed, uninfected infants (n=12 pairs) compared with HIV-uninfected mothers and HIV-unexposed infants (n=96 pairs) by 58% (p<0.001), 61% (p<0.001), 28% (p=0.034) and 32% (p=0.035), respectively (table 2). When the total placental transfer ratio (based on the ratio of the total infant population GMC to the total maternal population GMC was analysed, a similar reduction in placental transfer was observed in the context of maternal HIV infection (see online supplementary table S3).
Influence of maternal HIV status on placental transfer of specific antibody
Uninfected infants born to HIV-infected mothers (n=13) had significantly lower levels of antibody to PCP antigen compared with that of HIV-unexposed infants (n=96) (24.2 mg/ml, 95% CI 17.1 to 34.3 mg/l, vs 46.3 mg/l, 95% CI 39.2 to 54.8 mg/ml, p=0.005), despite similar levels of antibody between HIV-infected and uninfected mothers (figure 1). Antibody levels against Hib, pertussis and tetanus were similar between HIV-exposed and HIV-unexposed infants (figure 2, see online supplementary table S2).
Discussion
In this UK cohort only one in six women had a positive antibody response to pertussis antigens that may be protective against disease. Placental transfer of pertussis IgG was highly efficient; however, in keeping with low maternal antibody levels, less than one-third of newborn infants had a potentially protective level of pertussis antibody. In the context of the current pertussis epidemic, this suggests that a significant number of UK mothers and infants are at risk. Maternal antibody levels against Hib were also low; only 50% of mothers had antibody levels associated with long-term protection. Since placental transfer of anti-Hib IgG was less efficient, the majority of infants (58%) had an anti-Hib response below protective levels. By contrast, placental transfer of anti-tetanus IgG was highly efficient, and maternal antibody levels were high, consequently antibody responses to tetanus in both mothers and infants in this cohort are likely to be sufficient to provide protection against tetanus. The GMC of specific antibody to PCP (23 serotypes) among mothers was 44.54 mg/ml, which is within the normal adult range.12 No specific level of antibody to multiple pneumococcal serotypes has been correlated with a protective response. Maternal specific antibody levels were similar for pertussis, Hib, tetanus and pneumococcus between HIV-infected and HIV-uninfected women. However, the placental transfer of specific IgG to pertussis, Hib, pneumococcus and tetanus was significantly reduced from HIV-infected mothers to their HIV-exposed, uninfected infants compared with HIV-uninfected mothers and HIV-unexposed infants. Despite this finding, only responses to pneumococcus were significantly lower among uninfected infants born to HIV-infected mothers compared with HIV-unexposed infants.
Despite renewed interest in the potential of maternal immunisation to protect infants, data on baseline levels of maternal specific antibody levels, and passively acquired immunity in newborns, remain limited. Given differences in natural exposure to disease, vaccination strategies and genetic variation, baseline maternal and infant antibody levels will vary between different populations. The major strength of our study lies in presenting such data for a recent UK cohort.
This data is in keeping with low levels of maternal and infant pertussis and Hib antibody have also been found in similar-sized cohort studies in the USA, the Netherlands, Italy and South Africa.13–19
Our data also support recent studies which found that placental transfer of IgG to protein antigens, such as tetanus toxoid and pertussis toxin, shows active transport, leading to infant antibody levels greater than maternal levels.16 ,17 By contrast, placental transfer of IgG to polysaccharide antigens, such as Hib and pneumococcal polysaccharide antigens is much less efficient, resulting in equal or lower infant levels. This has been attributed to the active transport of IgG1 subtype antibodies, predominantly elicited by proteins, relative to the less-efficient transport of polysaccharide-elicited IgG2 antibodies.20 Conjugate vaccines are now available to Hib and pneumococcus, which could potentially elicit a greater IgG1 response. Since these vaccines were only introduced in the UK in 1992 and 2006, respectively, we would expect very few of the mothers in our cohort (median age 31.84) to have received these vaccines. Therefore, any maternal antibody response is likely to reflect natural exposure to polysaccharide, resulting in a predominant IgG2 response and consequently reduced placental transfer.
Our finding that maternal HIV-infection was associated with reduced placental transfer is also consistent with previous studies.20–24 Our data are of particular interest since, in contrast to previous studies, all HIV-infected women in this cohort were clinically stable and receiving highly active retroviral therapy. One surprising finding in our study is that, with the exception of lower antibody levels against pneumococcus, reduced placental transfer did not result in significantly lower specific antibody levels in HIV-exposed, uninfected infants compared with HIV-unexposed infants. This is in contrast to our previous work in South Africa.18 Although there were no significant differences in maternal antibody levels, a trend towards higher antibody levels in the HIV-infected mothers for Hib, pertussis and tetanus may have offset the effect of reduced placental transfer. This may reflect population differences between cohorts, different treatment regimes, or the limitations of sample size in our UK HIV-infected subgroup.
It is of particular concern that maternal antibody responses to pertussis antigens in this UK cohort were very low, given the current pertussis epidemic. Pertussis antibody levels decline within 2 years of both vaccination and infection, however protective immunity may last considerably longer.25 Waning vaccine-related immunity is thought to explain a peak prevalence of pertussis infection in adolescence.26 Since natural pertussis immunity is thought to decline over 4–20 years postinfection, and almost half of all infants in the UK are born to mothers aged over 30,27 ,28 it is not unexpected that maternal pertussis immunity in the UK may be suboptimal. In addition, it has been established that passively acquired immunity wanes rapidly in newborn infants, with disappearance of maternal antipertussis IgG by around 6 weeks of age.19 ,29 The new UK maternal pertussis vaccination programme aims to increase maternal and therefore infant antibody levels, extending the period of passive immune protection.8 The low baseline levels of immune response to pertussis shown in our UK cohort suggest that this intervention has the potential to be effective.
Natural immunity to Hib relies on recurrent subclinical infection.30 The significant reduction in Hib carriage rates in the community since the introduction of effective immunisation in the UK in 1992 contributes to a protective herd effect for neonates, and may also explain the low level of maternal immunity in our cohort. Numbers of cases of neonatal invasive infection are currently too low to justify a programme of maternal immunisation in the UK31; however, mortality for invasive Hib disease remains high, and our data confirm that the majority of infants will not have protective levels of immunity to Hib until primary vaccination is complete. This supports the Health Protection Agency’s current recommendations for prophylaxis of vulnerable household contacts of confirmed invasive Hib infection.32
While tetanus is now rarely seen in the UK, it remains a significant cause of neonatal mortality worldwide. The high antitetanus antibody levels observed in our cohort may be due to the adolescent booster programme. High maternal antibody levels coupled with efficient placental transfer of antibody ensures protective levels of antibody in the majority of newborns. Universal maternal tetanus immunisation in the UK is therefore unnecessary, however worldwide remains an essential tool in the elimination of neonatal and maternal tetanus and an excellent example of the potential utility of maternal immunisation to reduce infant mortality.3 ,33
Like Hib, invasive pneumococcal disease has become less common in the UK since the addition of pneumococcal conjugate vaccines to the infant immunisation schedule.34 Carriage rates of serotypes included in these vaccines have also reduced, providing some protection through herd immunity for neonates.35 However concerns remain regarding a rise in carriage and invasive disease due to non-vaccine serotypes, with over 100 cases of non-vaccine serotype invasive pneumococcal disease in infants less than 2 years in the UK in 2011–2012.36 While there is no validated correlate of protection for collective response to multiple pneumococcal serotypes, our finding of lower pneumococcal antibody levels in HIV-exposed infants is of some concern. In developing world settings, HIV-exposure, even without HIV-infection, is associated with an increased risk of severe pneumonia.37 While the mortality risk for HIV-exposed, uninfected, infants in a UK setting is likely to be lower, our data suggest that this population remains vulnerable to invasive pneumoccocal disease. Previous studies of maternal immunisation to prevent pneumococcal disease in infants have demonstrated an increased immune response in mothers and infants lasting several months38–42; however, a recent systematic review concluded there was insufficient evidence that maternal pneumococcal immunisation reduced neonatal infection.43 Included trials were limited by small sample size, and all used the (unconjugated) pneumococcal polysaccharide vaccine. While this vaccine offers coverage for a larger number of serotypes, pneumococcal conjugate vaccines could theoretically offer the advantage of producing IgG1 antibodies with more efficient placental transfer. Larger clinical trials are required to assess the potential impact of maternal pneumococcal immunisation in infants, particularly infants exposed to HIV.
Our study has a number of limitations, one of which is enrolment of a modest number of mother–infant pairs at a single centre. Consecutive sampling ensured that our cohort accurately reflected families accessing care in this central London hospital; however this ethnically diverse population, with a high proportion of HIV-infected mothers, may not be representative of all areas in the UK.
Another potential limitation of this study is the use of a mixed pertussis antigen (PT/FHA) ELISA to assess antibody response. This assay was chosen to allow comparison to previously published work18 and because both PT and FHA are vaccine antigens present in all licensed vaccines in Europe. The use of ELISAs that measure these antibodies separately may however have allowed easier comparison to other studies. Another concern is that mixed antigen assays have been found to be less specific in the diagnosis of pertussis.44 Published recommendations for the diagnosis of pertussis infection state that PT-specific antibodies alone should be measured; however, these recommendations acknowledged that measurement of antibodies to other pertussis antigens may be appropriate in immunogenicity studies.45 Although both sensitivity and specificity of the assay used in this study have previously been reported to be 95%,46 a more recent study-reported specificity to be only 56%.44 If the specificity of our pertussis assay is low we may have overestimated maternal-specific pertussis antibody levels, and therefore may have underestimated the proportion of mothers and infants susceptible to pertussis. Our main conclusion, that pertussis antibody levels in this cohort are worryingly low, remains unchanged.
Maternal immunisation has a sound theoretical basis and has been proven to increase levels of maternal and infant antibody for a number of infectious diseases, but with the exception of tetanus the efficacy of this strategy in reducing infant mortality needs further study.47 ,48 The introduction of maternal pertussis immunisation in the UK offers an excellent opportunity for a large population-based study to assess impact of this programme on maternal seroprevalence and national rates of infant pertussis infection. In addition, more data is needed to resolve concerns that high levels of maternal antibody diminish infant active immune response to vaccination. While recent studies suggest this does not affect efficacy of the acellular pertussis vaccine,48 ,49 it would be prudent to assess this further by comparing infant immune responses postvaccination in infants of mothers who received the pertussis vaccination to a control group of those who did not.
Finally, a challenge to the introduction of the maternal pertussis vaccination campaign will be achieving acceptability and therefore uptake among pregnant women. Reports suggest initial uptake of the maternal pertussis vaccine in the UK is relatively high at 50%.50 However, such promising early results would only be maintained and improved if pregnant women, and their healthcare providers, were convinced that the benefits are very clear and there were no safety concerns. As has been observed with the influenza vaccination, where uptake among pregnant women in England was only 27.4% in 2011/2012,51 important barriers to implementation of these potentially life-saving interventions exist. Evidence-based strategies to increase public and practitioner acceptability of maternal immunisation are required.47
Infant immunisation remains one of the most successful tools in reducing child morbidity and mortality worldwide. Maternal immunisation offers the potential to extend this success story to protect our youngest and most vulnerable children.
Acknowledgments
We would like to thank the families who participated in the study and our colleagues in Maternity Services at St Mary's Hospital who helped with this project. Dr Sarah Burl, Research Scientist, Imperial College London assisted with laboratory assays and sample processing. Dr Graham Taylor, Consultant in Genito–urinary Medicine/HIV and AIDS and Dr John Smith, Consultant Obstetrician at St Mary's Hospital facilitated patient recruitment.
References
Supplementary materials
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
Files in this Data Supplement:
- Data supplement 1 - Online tables
Footnotes
CJ and LP contributed equally.
-
Contributors CJ co-designed the study, designed data collection tools, contributed to recruitment and data collection, monitored data collection for the whole study, wrote the statistical analysis plan, performed laboratory assays, cleaned and analysed the data, and drafted and revised the paper. She is the guarantor. LP performed laboratory assays, cleaned and analysed the data, and drafted and revised the paper. SMB and AB recruited patients, collected data and revised the draft paper. BK designed the study, advised on data analysis and drafted and revised the paper. All authors had full access to all the data in the study and take responsibility for the integrity of the data and the accuracy of data analysis. All authors have read and approved the final manuscript.
-
Funding This study was funded by the National Institute for Health Research (NIHR) Biomedical Research Centre based at Imperial College Healthcare NHS Trust and Imperial College London (grant number P31436). The views expressed are those of the author(s) and not necessarily those of the NHS, the NIHR or the Department of Health. The funding body had no role in the study design; in the collection, analysis or interpretation of data; in the writing of the report or in the decision to submit the article for publication.
-
Competing interests All authors have completed the Unified Competing Interests form at www.icmje.org/coi_disclosure.pdf (available on request from the corresponding author) and declare: CJ, LP, SMB and AB had no financial relationships with any organisations that might have an interest in the submitted work in the previous 3 years. In the past 2 years BK has acted as a scientific advisor for Pfizer and Novartis and has submitted grant applications for other research in maternal immunisation to the Wellcome Trust and MRC, she also holds a Pfizer Investigator Initiated grant for research assessing the impact of pneumococcal vaccination. The authors declare no other relationships or activities that could appear to have influenced the submitted work.
-
Ethics approval National Research Ethics Service, reference: 07/H0720/178.
-
Provenance and peer review Not commissioned; externally peer reviewed.
-
Data sharing statement No additional data are available.