Article Text

Abstract
Objective To investigate Candida species and Staphylococcus aureus and the development of ‘nipple and breast thrush’ among breastfeeding women.
Design Prospective longitudinal cohort study.
Setting Two hospitals in Melbourne, Australia (one public, one private) with follow-up in the community.
Participants 360 nulliparous women recruited at ≥36 weeks’ gestation from November 2009 to June 2011. Participants were followed up six times: in hospital, at home weekly until 4 weeks postpartum and by telephone at 8 weeks.
Main outcome measures Case definition ‘nipple and breast thrush’: burning nipple pain and breast pain (not related to mastitis); detection of Candida spp (using culture and PCR) in the mother's vagina, nipple or breast milk or in the baby's mouth; detection of S aureus in the mother's nipple or breast milk.
Results Women with the case definition of nipple/breast thrush were more likely to have Candida spp in nipple/breast milk/baby oral samples (54%) compared to other women (36%, p=0.014). S aureus was common in nipple/breast milk/baby samples of women with these symptoms as well as women without these symptoms (82% vs 79%) (p=0.597). Time-to-event analysis examined predictors of nipple/breast thrush up to and including the time of data collection. Candida in nipple/breast milk/baby predicted incidence of the case definition (rate ratio (RR) 1.87 (95% CI 1.10 to 3.16, p=0.018). We do not have evidence that S aureus colonisation was a predictor of these symptoms (RR 1.53, 95% CI 0.88 to 2.64, p=0.13). Nipple damage was also a predictor of these symptoms, RR 2.30 (95% CI 1.19 to 4.43, p=0.012). In the multivariate model, with all three predictors, the RRs were very similar to the univariate RRs. This indicates that Candida and nipple damage are independent predictors of our case definition.
- Primary Care
this is an open-access article distributed under the terms of the creative commons attribution non-commercial license, which permits use, distribution, and reproduction in any medium, provided the original work is properly cited, the use is non commercial and is otherwise in compliance with the license. see: http://creativecommons.org/licenses/by-nc/2.0/ and http://creativecommons.org/licenses/by-nc/2.0/legalcode.
Statistics from Altmetric.com
Article summary
Article focus
-
Controversy about the condition known as ‘breast thrush’ or breast candidiasis in lactating women has led to confusion among clinicians and the community.
-
Previous studies have been cross-sectional.
-
This is the first prospective longitudinal study to examine simultaneously both Staphylococcus aureus and Candida spp in breast infections and was designed to resolve the current controversy surrounding the primary organism responsible for the condition known as ‘breast thrush’: Candida spp or S aureus?
Key messages
-
Candida spp is associated with burning nipple pain and breast pain.
-
Colonisation with S aureus is common; at least 50% of women were colonised with S aureus in nipple or milk samples by 4 weeks postpartum.
Strengths and limitation of this study
-
The evidence of microbiological data from this large cohort of women over 4 weeks postpartum is stronger than previous smaller cross-sectional studies.
-
Candida spp were more commonly identified using more sensitive molecular techniques (real-time PCR) than by using standard microbiological culture techniques.
-
As these techniques are not used in clinical practice currently, clinicians should continue to use their clinical skills to diagnose causes of nipple and breast pain in lactating women.
Background
Controversy about the condition known as ‘breast thrush’ or breast candidiasis in lactating women has led to confusion among clinicians and the community. While some clinicians may diagnose and treat this condition in breastfeeding women with deep, radiating breast pain associated with burning nipple pain,1–6 others doubt the relationship with fungal organisms7–11 and decry ‘the alarming trend towards believing that fungi are important in the aetiology of breast infection and deep breast pain associated with breast feeding, despite a lack of good quality evidence’ (ref. 11, p.485).
Unlike mastitis, which is diagnosed when a breastfeeding woman experiences inflammation of the breast associated with systemic symptoms,12 breast thrush is usually diagnosed when the breast is not erythematous or indurated, and the woman is afebrile and systemically well except for the typical burning pain radiating into the breast and/or the back.4 While some authors use the term ‘candida mastitis’,6 ,11 ,13 we feel this is misleading, as inflammation of the breast is not evident. Although some clinicians attribute the pain to infection with S aureus and treat women with long-term antibiotics,14 this has not been tested in trials.
The primary cause of nipple pain or damage is often the process of breastfeeding itself: trauma due to the incorrect attachment of the infant's mouth, anatomy of the mouth or dysfunctional suck.15 Nipple thrush is usually diagnosed when the nipple/areola is slightly pink, sensitive to touch and the pain described is out of proportion to the damage seen on clinical examination.4 When the areola is described as itchy and appears red and/or crusty, the diagnosis is dermatitis/eczema rather than fungal infection.16 A nipple with obvious damage is almost certainly colonised with S aureus.17 Nipple/breast pain associated with nipple blanching persisting for longer than a few seconds is likely to be nipple vasospasm; this condition is commonly confused with breast thrush because of the burning, radiating nature of the pain.18 ,19 The pain due to vasospasm is often secondary to nipple damage or infection, exacerbated by cold and relieved by heat or nifedipine.20 In practice, more than one cause of nipple or breast pain is commonly present,6 which makes it difficult to construct a case definition for ‘breast thrush’ for research purposes.
Previous breastfeeding studies have been largely cross-sectional,1 ,7 ,9 ,10 with one longitudinal study collecting microbiological data but no clinical information.21 This is the first prospective longitudinal study to examine both S aureus and Candida spp in breast infections and was designed to resolve the current controversy surrounding the primary organism responsible for the condition known as ‘breast thrush’: Candida spp or S aureus?
Methods
The CASTLE (Candida and Staphylococcus Transmission: Longitudinal Evaluation) study was a prospective longitudinal descriptive study; details have been published in the study protocol.22 A cohort of 360 nulliparous women planning to breastfeed for at least 2 months were recruited at ≥36 weeks’ gestation from two hospitals in Melbourne, Australia (November 2009–June 2011). At recruitment, nasal, nipple (both breasts) and vaginal swabs were collected and participants completed a questionnaire asking about previous Staphylococcus and Candida infections. Participants were followed up six times: face-to-face in hospital, then weekly at home until 4 weeks postpartum. The participants filled out a questionnaire at each time point to collect information about breastfeeding problems and postpartum health problems. At each visit, maternal nasal, and nipple swabs and breast milk samples (both breasts) and infant oral and nasal swabs were collected. In a final telephone interview 8 weeks postpartum, information about breastfeeding problems and postpartum health was collected.
Specimens were collected by research assistants. Fresh gloves were worn for each specimen. After sanitising their hands, research assistants collected nipple swabs, then washed the nipple/areola region twice using sterile water wipes. Midstream milk was collected in a sterile container; the first drops of breast milk were expressed and discarded. Two nipple swabs were obtained from each nipple: a standard charcoal swab for microbiological analysis (Copan Diagnostics Inc, California, USA) and a flocked swab for molecular analysis (Copan Diagnostics Inc). After first moistening in sterile saline, both the standard and flocked nipple swabs were rolled over the nipple and areola together using a 10-point swabbing technique,23 paying particular attention to any cracks/fissures present. Oral and vaginal swabs were collected for culture of S aureus and Candida spp. Breast milk samples were also cultured for S aureus, coagulase-negative staphylococci (CoNS) and Candida spp; nasal swabs were collected for culture of S aureus only.
In the studies conducted on women with vulvovaginal symptoms, molecular microbiological techniques have been useful in detecting Candida in women who were found to be negative with standard microbiology techniques.24 ,25 Therefore, we planned to use molecular techniques to increase detection of Candida spp in nipple specimens.22 Owing to cost constraints, we did not plan to use molecular techniques for the milk specimens (up to 4000 specimens). As participants only had one or two vaginal specimens, we extracted DNA from vaginal as well as nipple swabs for molecular identification of Candida spp using real-time PCR.22
At each contact, women were asked about their nipple pain (In the last 48 h, have you experienced nipple pain/discomfort?) and whether it was burning in quality (If yes, would you describe your nipple pain as burning?), clinical signs and symptoms of mastitis as used in previous research (ie, redness, fever, etc),26 and other types of breast pain (Have you had other breast pain in the last 2 days? No/I have had stabbing (radiating or shooting) breast pain only/I have had non-stabbing breast pain only/I have had both stabbing and non-stabbing breast pain). We also asked, ‘Do you have nipple vasospasm? (Nipple blanches or goes white in the cold or during/after feeds) No/Yes, for less than 5 min/Yes, for more than 5 min/Not sure’. Researchers also collected clinical observations of the nipple/areola and breast at each visit (weeks 1–4), including the colour of the nipple/areola. Our case definition of ‘nipple and breast thrush’ used a combination of burning nipple pain and breast pain (non-mastitis). Francis-Morrill et al found nipple appearance (‘shiny’ or ‘flaky’ nipple or with pink colour) to be predictive of Candida.27 However, in our study, very few women were described as having these appearances (shiny, n=4, flaky, n=17), while 140 women were described as having ‘pink’ nipple/s. Adding the appearance identifiers to our case definition was not helpful. Clinically, the symptoms of nipple and breast thrush develop in the first week postpartum, and since most pain in the first week postpartum in first-time mothers is likely to be due to adjustment of the body to breastfeeding, we examined the case definition at weeks 1–8, and weeks 2–8 separately.
Statistical analysis was conducted using Stata V.12. Hypothesis 1—women with nipple/breast thrush are more likely to have Candida spp isolated from culture than other women; hypothesis 2—women with nipple/breast thrush are more likely to have S aureus isolated than other women. A sample of 318 women was estimated to provide adequate power.22 χ2 tests were used for comparing categorical variables. We investigated the incidence of nipple/breast thrush using a multivariable discrete version of the proportional hazards regression model.28 Outcome variable was the incidence of new cases of our nipple and breast thrush definitions; time-varying predictors were: the presence of Candida spp, presence of S aureus and mother-reported nipple damage. We present crude rate ratios (RR), and multivariate analysis, adjusting for the presence of Candida spp, S aureus and nipple damage.
Results relating to mastitis, other breastfeeding and postpartum problems will be published separately (papers in preparation).
Results
Fourteen women withdrew from the study after giving birth, leaving 346 (96%) women available for data collection at subsequent visits; 340 (94%) women completed the study at 8 weeks postpartum. Women who participated in the study were highly educated (77% had a tertiary degree or higher) and most were married or lived with their partner (96%) (table 1). Just over half gave birth in a private hospital (56%), 45% by Caesarean section.
Characteristics of nulliparous women recruited in late pregnancy
Burning nipple pain was reported by 42% of women (146/346) during weeks 1–8, or 32% women (111/346) during weeks 2–8. Radiating or non-radiating breast pain (not related to engorgement/mastitis) was reported by 54% of women (186/346) during weeks 1–8, or 47% of women (162/346) during weeks 2–8. Combining these symptoms to estimate the number of women with both burning nipple pain and non-mastitis breast pain (at the same time), there were 19% of women in weeks 1–8 (65/346), or 15% in weeks 2–8 (50/346).
Candida albicans was the most commonly isolated Candida spp in culture with Candida glabrata only isolated in one nipple specimen and one milk sample (table 2). Although ‘other Candida spp.’ were found, none speciated as Candida krusei or Candida kefyr. Candida PCR of the nipple was positive for Candida spp in 33% of women (115/346), in contrast to culture of only 3% of women (9/346) being positive for Candida spp. Candida spp were isolated from the culture of breast milk samples from 5% of the women (18/346), but no molecular analyses were conducted on these samples. Table 3 shows Candida isolated from the culture and by PCR on each visit. S aureus was isolated from the culture of the nipple and/or breast milk in 67% of women (231/346), and from the nose and/or mouth of 73% of infants (253/346) at some point during follow-up. There were 22 milk samples positive for Candida, of which 10 were only milk, and 12 were positive for nipple and milk. For S aureus, 425 milk samples were positive, of which 89 were positive in milk only.
Results from microbiological analysis of specimens collected from 346 women and their infants (at any time point)
Candida positive on PCR or culture at each visit
Burning nipple pain was very common in week 1, primarily as women adjusted to breastfeeding; therefore, we explored the relationship between Candida spp and S aureus using two case definitions: weeks 1–8 and weeks 2–8 (table 4). There was a statistically significant association between these symptoms in weeks 2–8 and Candida spp in nipple/breast milk/baby (p=0.014); as also for Candida spp in vagina/nipple/breast milk/baby (p=0.047, not shown). S aureus was common in nipple/breast milk/baby samples of women with these symptoms as well as in women without these symptoms (82% vs 79%) (p=0.597, table 4).
Case definition and Candida spp (culture or PCR) and Staphylococcus aureus separately (n=346)
As women with nipple vasospasm described burning, radiating pain, we have also analysed the case definition excluding women with vasospasm (see table 4). Only two women were removed from the analysis (n=48), which made little difference to the results.
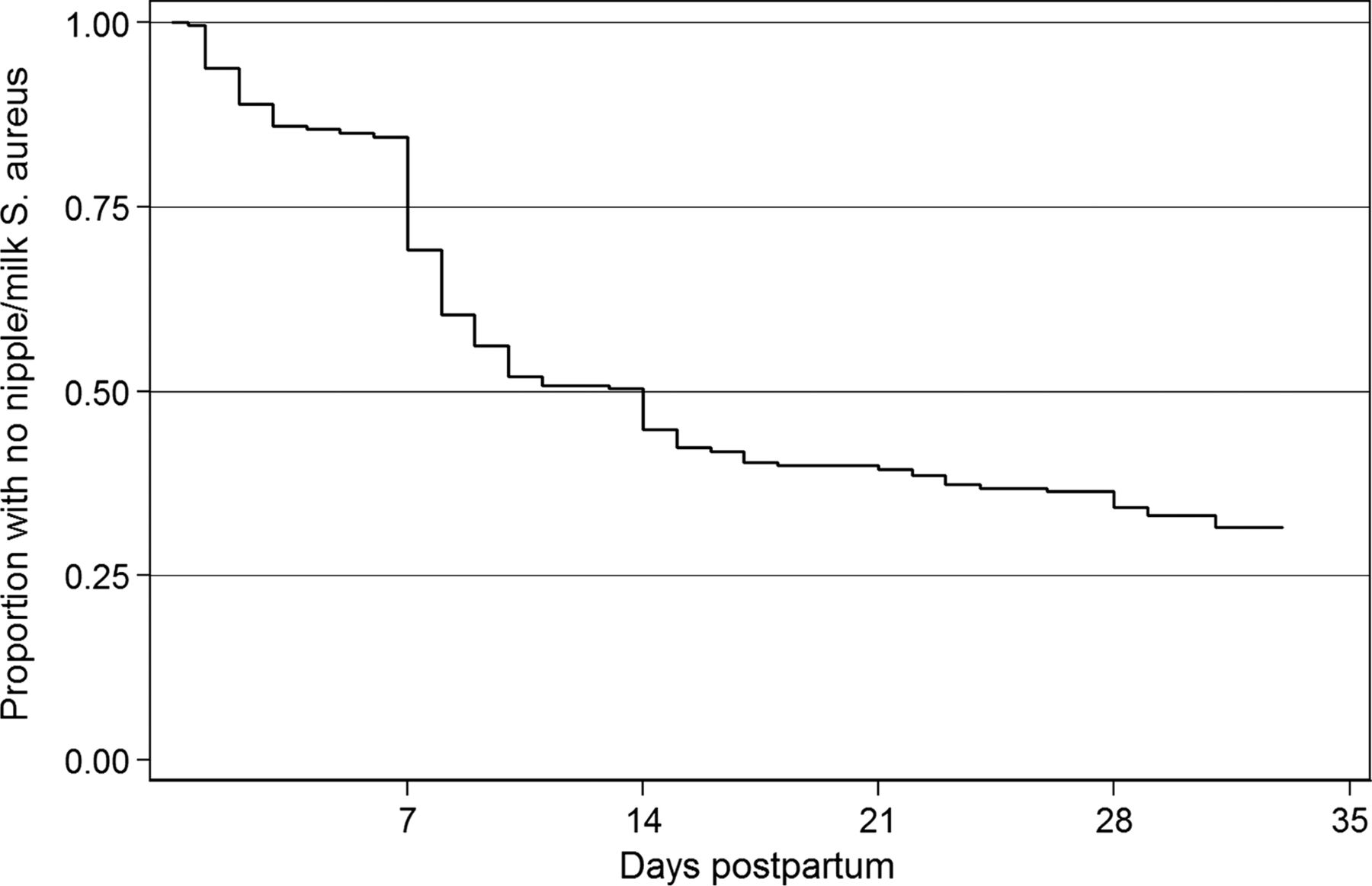
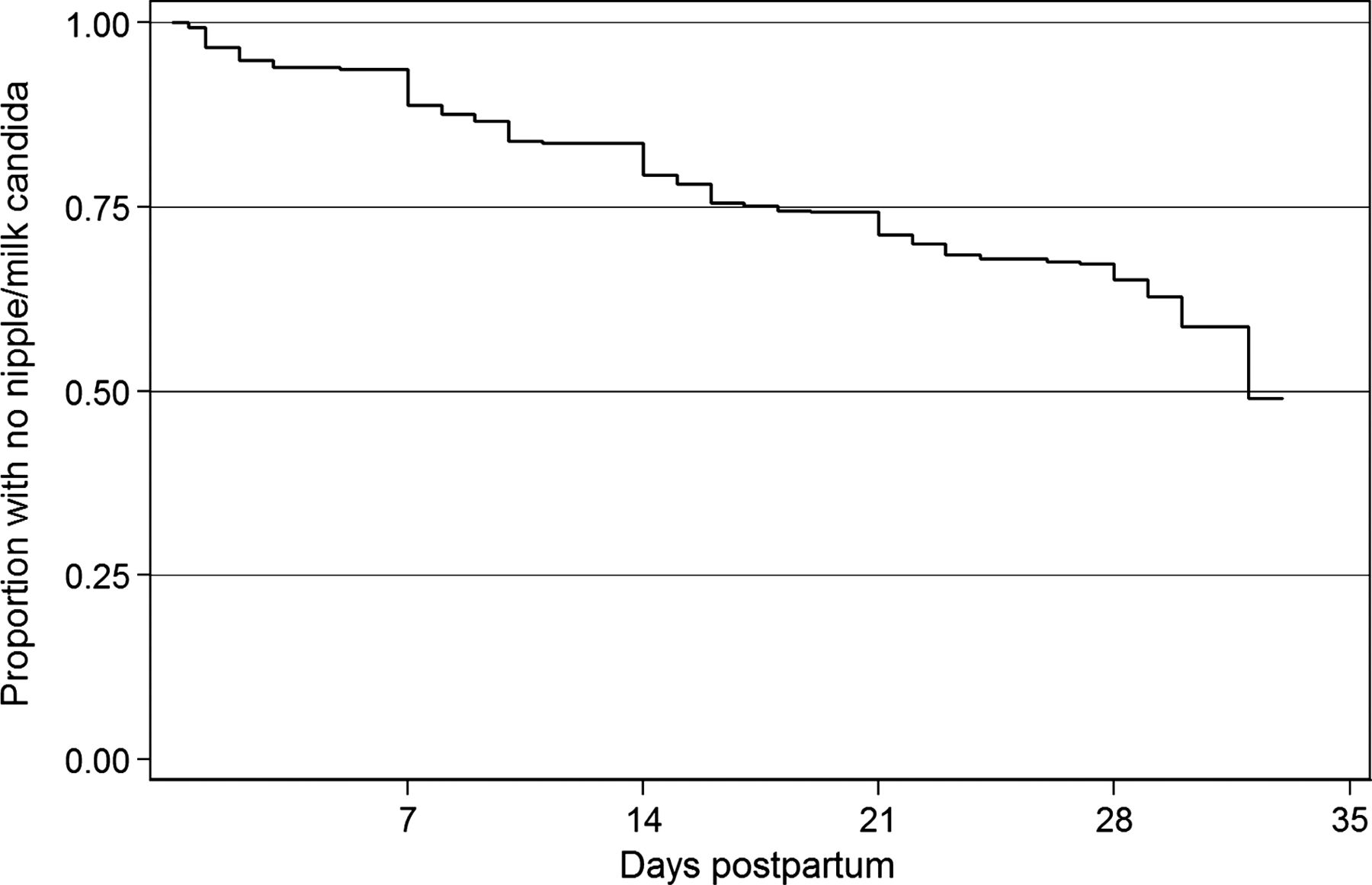
Time-to-event analysis examined predictors of our case definition of nipple/breast thrush (burning nipple and breast pain (non-mastitis)) up to and including the time of data collection in the first 4 weeks. (See unadjusted survival curves: figures 1⇓–3 and table 5). Candida in nipple/breast milk/baby predicted incidence of the case definition (RR 1.87 (95% CI 1.10 to 3.16, p=0.018). Thus, for women with Candida in the nipple/milk/baby at any time point, the rate of subsequently developing the case definition was increased by 87%, compared to women without Candida. The evidence for S aureus colonisation as a predictor of these symptoms was not strong (RR 1.53, 95% CI 0.88 to 2.64, p=0.13). Mothers’ report of nipple damage was a predictor of these symptoms, with an RR of 2.30 (95% CI 1.19 to 4.43, p=0.012). In the multivariate model, with all three predictors, the RRs were very similar to the univariate RRs. This indicates that Candida and nipple damage are independent predictors of our case definition.
Time-to-event analysis of predictors of first symptoms of case definition

Survival curve for first time to nipple/milk Candida.
Survival curve for time to first nipple/milk Staphylococcus aureus.

{kind=link}
{kind=link}
{kind=link}
Survival curve for time to first symptoms of case definition of ‘breast thrush’.
Discussion
Principal findings
Unlike some cross-sectional studies which found no relationship between the presence of Candida spp and the condition known as breast thrush,9 ,10 we have shown that Candida spp is associated with burning nipple pain and breast pain—in two analyses (‘at any time’ and ‘time-to-event’). As in previous studies,1 ,7 we uncommonly isolated Candida spp from the nipple using standard microbiological culture techniques. However, Candida spp. were more commonly identified using more sensitive molecular techniques (real-time PCR). This test is not used in routine practice currently, and therefore it is not helpful in making the diagnosis in clinical care at this time. Candida spp were also rarely isolated in breast milk, using standard techniques. It is possible that the isolation rate would have been higher if we had used the technique of Morrill and colleagues,29 who added iron to inactivate milk lactoferrin. However, Hale et al were unable to identify Candida in breast milk of women with ‘Candida mastitis’ using culture and another specific technique (presence of 1→3-β-D-glucan).10 The 16 cases had ‘sore, inflamed, or traumatised nipples, intense stabbing or burning pain that radiated into the axilla often persisting after feeding, and painful feeding without alternate diagnosis’.10 Possible explanations for Hale et al's findings are that the women had other causes of pain (from the traumatised nipple, from maternal vasospasm, or infant posterior tongue-tie or other mechanical causes of pain); that Candida was present in the nipple (samples were only collected from the milk), or that Candida is not present in the milk of women with this syndrome. The question as to whether Candida is present in the lactiferous ducts is still open to debate; what we have shown is a link between Candida and nipple/breast pain—independent of the presence of nipple damage or S aureus.
Candida spp are commensal organisms, and therefore the presence of Candida spp does not always imply infection. Recent understanding of vulvovaginitis postulates that the threshold number of organisms for symptomatic vaginitis varies for different groups of women; women with infrequent vaginitis have a higher threshold.30 Furthermore, the symptoms associated with vaginitis may be caused by the host neutrophil response; small numbers of organisms may promote an aggressive inflammatory response in some women.30
Consistent with other studies of mothers and infants,21 ,31–34 colonisation with S aureus is common; at least 50% of women were colonised with S aureus in the nipple or milk samples by 4 weeks postpartum. Therefore in clinical practice, a finding of S aureus in the nipple or breast milk is not evidence that the bacteria are the principal cause of the woman's pain. Our analysis indicates that candida and S aureus are acting independently, despite often coexisting. The case-control study of women with a clinical diagnosis of nipple and breast thrush by Panjaitan et al,35 which only used molecular techniques from nipple swabs and excluded women with clinical signs of bacterial infection (exudate on nipple or inflamed breast), found that S aureus was present in equal numbers of cases and controls.
Clinical implications
Diagnostic skills are needed to make a diagnosis of nipple/breast candidiasis; clinicians should routinely consider all causes of nipple and breast pain, in the same way they consider differential diagnoses when assessing a patient with chest pain.36 Women with nipple damage or with nipple vasospasm describe pain that is burning in quality; in the past, this has often been misdiagnosed as Candida infection.37 The pain clinically associated with Candida infection is persistent, ranges from mild to severe, and is not relieved by the use of nipple shields or expressing/pumping, or applying heat. When the pain is related directly to infant feeding, the cause is likely to be mechanical, and when the pain is relieved by heat, vasospasm is the likely cause.19 We found that nipple damage was associated with burning nipple and radiating breast pain, so clinicians should be cautious about diagnosing infection (whether fungal or bacterial) in every woman with nipple damage.
Strengths and limitations
The strength of this study is that a cohort of healthy women who had not previously breastfed was recruited prior to starting breastfeeding and was followed closely until 2 months postpartum. It is the first prospective longitudinal study to examine simultaneously both S aureus and Candida spp in a cohort of breastfeeding women and their infants.
The main limitation is that we did not have a clinical diagnosis of nipple/breast thrush and had to use a case definition based on two symptoms to estimate this condition. Participants responded to questions about pain and nipple blanching, and research assistants reported nipple appearance, but these measures could not substitute for a clinical assessment. Furthermore, infant oral anatomy was not examined to exclude tongue-tie, and breastfeeds were not observed. We are not implying that all women with burning nipple and breast pain had a clinical diagnosis of nipple/breast thrush. We hypothesise that Candida is associated with nipple/breast pain in some women, in a similar manner to the relationship between Candida and vulvovaginal symptoms: Candida is a commensal in some women, while other women experience significant pain when only small numbers of organisms are present.30
Another limitation is that we only followed the cohort for 8 weeks postpartum—with microbiological data to only 4 weeks postpartum; women who developed problems after this time period were not captured in our data collection.
Conclusions
This large cohort study provides evidence that Candida spp play a role in nipple and breast pain in lactating women; however, burning nipple pain is common in breastfeeding women, and a diagnosis of Candida spp infection should not be made without considering differential diagnoses.4 Further research into the role of staphylococci in breast pain in lactating women with inflammatory symptoms and without is needed. Animal models, as have been used in vulvovaginal candidiasis,30 may be required to fully understand the pathogenesis of this condition. Future researchers may consider the RCTs for treatment or clearance of Candida.
References
Footnotes
-
Contributors LHA conceived the study, which was designed in collaboration with all authors. SMD managed the data and conducted the statistical analyses. SMG, SNT, CMB and MSP provided microbiological expertise into study design, analysis and writing of the paper. MC was the project coordinator and contributed to the questionnaire design. MSP was the research scientist. LHA drafted the manuscript which was critically revised by all authors.
-
Funding This study received financial support from the National Health & Medical Research Council (NHMRC) (project grant 541907, equipment grant, Health Professional Training Fellowship (LHA)), Helen Mcpherson Smith Trust, Faculty Research Grant, Faculty of Health Sciences, La Trobe University.
-
Competing interests None.
-
Ethics approval This study was approved by the La Trobe University Human Ethics Committee (06–078); Human Research Ethics Committee of the Royal Women's Hospital (06/41); Human Research Ethics Committee of the University of Melbourne (1033949); and Medical Advisory Committee at Frances Perry House.
-
Provenance and peer review Not commissioned; externally peer reviewed.
-
Data sharing statement No additional data are available.