Article Text

Abstract
Objective To synthesise existing knowledge of the efficacy and safety of long-acting versus short-acting methylphenidate for paediatric attention deficit hyperactivity disorder (ADHD).
Design Systematic review and meta-analysis.
Data sources Electronic literature search of CENTRAL, MEDLINE, PreMEDLINE, CINAHL, EMBASE, PsychINFO, Scopus and Web of Science for articles published in the English language between 1950 and 2012. Reference lists of included studies were checked for additional studies.
Study selection Randomised controlled trials of paediatric ADHD patients (<18 years), comparing a long-acting methylphenidate form to a short-acting methylphenidate form.
Data extraction Two authors independently selected trials, extracted data and assessed risk of bias. Continuous outcomes were compared using standardised mean differences (SMDs) between treatment groups. Adverse events were compared using risk differences between treatment groups. Heterogeneity was explored by subgroup analysis based on the type of long-acting formulation used.
Results Thirteen RCTs were included; data from 882 participants contributed to the analysis. Meta-analysis of three studies which used parent ratings to report on hyperactivity/impulsivity had an SMD of −0.30 (95% CI −0.51 to −0.08) favouring the long-acting forms. In contrast, three studies used teacher ratings to report on hyperactivity and had an SMD of 0.29 (95% CI 0.05 to 0.52) favouring the short-acting methylphenidate. In addition, subgroup analysis of three studies which used parent ratings to report on inattention/overactivity indicate that the osmotic release oral system generation long-acting formulation was favoured with an SMD of −0.35 (95% CI −0.52 to −0.17), while the second generation showed less efficacy than the short-acting formulation with an SMD of 0.42 (95% CI 0.17 to 0.68). The long-acting formulations presented with slightly more total reported adverse events (n=578) as compared with the short-acting formulation (n=566).
Conclusions The findings from this systematic review indicate that the long-acting forms have a modest effect on the severity of inattention/overactivity and hyperactivity/impulsivity according to parent reports, whereas the short-acting methylphenidate was preferred according to teacher reports for hyperactivity.
- Attention deficit/hyperactivity disorder
This is an open-access article distributed under the terms of the creative commons attribution non-commercial license, which permits use, distribution, and reproduction in any medium, provided the original work is properly cited, the use is non commercial and is otherwise in compliance with the license. see: http://creativecommons.org/licenses/by-nc/2.0/ and http://creativecommons.org/licenses/by-nc/2.0/legalcode.
Statistics from Altmetric.com
Article summary
Article focus
-
To systematically review and meta-analyse existing knowledge of the efficacy of long-acting versus short-acting methylphenidate for paediatric attention deficit hyperactivity disorder (ADHD).
-
To systematically review existing knowledge of the safety of long-acting versus short-acting methylphenidate for paediatric ADHD.
-
To help better inform clinical practice when treating children with ADHD.
Key messages
-
Despite costing up to 15 times as much, long-acting methylphenidate preparations have modest effect on core symptoms based on parent reports, in comparison to short-acting preparations.
-
Short-acting methylphenidate was slightly more favourable to core symptoms according to teacher reports.
-
Both formulations present with similar adverse events.
Strengths and limitations of this study
Strengths
-
Systematically reviewed a question that has never been reviewed and is clinically relevant.
-
Search methods, data extraction and risk of bias assessment were thorough.
Limitations
-
Only included studies published in English.
-
Excluded grey literature.
-
Did not include qualitative outcomes.
Introduction
Attention deficit hyperactivity disorder (ADHD) is the most common neurodevelopmental disorder in childhood, occurring in approximately 5.29% of children worldwide.1 The core symptoms of ADHD (i.e, inattention, impulsivity and hyperactivity) can result in multiple areas of dysfunction relating to a child’'s performance in the home, school and community (American Academy of Pediatrics 2001). Furthermore, the core symptoms can be expressed to various degrees in different children, breaking ADHD into three subtypes: the predominantly inattentive type, the predominantly hyperactive-impulsive type and the combined type (ie, children displaying both inattention and hyperactivity).2 The symptoms of ADHD have been shown to have long-term effects on a child's academic performance and social development. It has been estimated that up to 50–60% of childhood ADHD cases will persist into adulthood, making it a lifetime condition for many.3 ,4
Stimulant medication is recommended as a first-line modality for treating ADHD.5 Evidence has suggested that ADHD may be the result of insufficient production of norepinephrine and dopamine in the prefrontal cortex,6 resulting in forgetfulness, distractibility, impulsivity and inappropriate social behaviours.7 By increasing the levels of norepinephrine and dopamine in the prefrontal cortex, stimulants are thought to restore executive functioning.6
Methylphenidate is the most commonly prescribed stimulant for children with ADHD. Numerous studies have shown that methylphenidate improves the core symptoms of ADHD as reflected in parent and teacher ratings.8 In the multimodality treatment study of ADHD 9 a three-times daily regimen of immediate-release methylphenidate was selected as the gold standard pharmacological treatment of ADHD. Despite this, problems remain that are inherent to the multiple daily dosing including issues with adherence. As a result, a number of more expensive, extended-release formulations have been introduced into the market. First generation extended-release formulations utilise a wax-matrix to provide slow, continual release of methylphenidate;10 however, they have been found to have a slow onset of action. The second generation forms contain both immediate-release and extended-release coated particles, designed to have two phases of drug release resulting in rapid onset and longer durations (t1/2=6.8 h). The final type of extended-release methylphenidate is the osmotic release oral system (OROS) methylphenidate, which is a controlled-release formulation that uses osmotic pressure to deliver methylphenidate at a controlled rate throughout the day (t1/2=6.4 h).11
To our knowledge, a systematic review comparing short-acting versus long-acting methylphenidate has never been conducted. As the long-acting formulations cost up to 15 times as much as the short-acting preparations,12 we believe that establishing comparative efficacy and safety between the two forms is imperative. Thus, we conducted a systematic review and meta-analysis which includes a synthesis of all English published randomised controlled trials assessing the efficacy and safety of short-acting versus long-acting methylphenidate formulations to manage the core symptoms of paediatric ADHD.
Methods
Search strategy
We searched the Cochrane Central Register of Controlled Trials (CENTRAL), MEDLINE, PreMEDLINE, CINAHL, EMBASE and PsychINFO from 1950 to 1 August 2012. Relevant, published RCTs were identified using the key terms: attention deficit with hyperactivity disorder, child/adolescent/paediatric, and methylphenidate. English language restriction was applied. The reference lists of included studies identify additional studies.
Selection of studies
Selection of studies was based on a screening of titles and/or abstracts independently by two authors (SP and LZ). Both reviewers independently assessed the full-text articles of those studies whose inclusion was unclear, based on abstracts alone. Final decisions were reached by consensus, with disagreements being resolved by discussion.
Inclusion criteria
English published randomised controlled trials were selected if they met the following criteria: (1) participants were <18 years of age, with a clinical diagnosis of ADHD as determined by Diagnostic and Statistical Manual of Mental Disorders (DSM-III) (American Psychological Association (APA) 1987) or DSM-IV (APA 2000) criteria or equivalent (2) the trial compared a long-acting methylphenidate form with a short-acting methylphenidate form; and (3) the study measured either (a) efficacy defined as improvement of the core symptoms of ADHD (inattention, impulsivity, hyperactivity) measured by either parent and/or teacher rating scales; or (b) adverse events.
Data extraction
Two authors (SP and LZ) independently extracted data from the selected studies using data extraction forms. Extracted data included patient demographics, interventions used, outcomes and trial design. Discrepancies were resolved by discussion; however, there were no major differences in extraction between the review authors.
Missing data
Authors were contacted up to three times to obtain missing data. Clarification was required by one of the authors as to who had filled out the ADHD symptom questionnaire, but no response was provided.
Risk of bias assessment
Two authors (SP and LZ) independently assessed the risk of bias of each trial, following the domain-based evaluation as described in the Cochrane Handbook for Systematic Reviews of Interventions 5.0.0.13 Six domains were assessed: randomisation, allocation concealment, blinding, incomplete outcome data, selective outcome reporting, and other sources of bias. Disagreements between the authors were resolved by discussion.
Outcomes
T`he outcomes of interest included efficacy and adverse events. Efficacy was defined as improvement of the core symptoms of ADHD (inattention, impulsivity, hyperactivity) measured by parent and/or teacher rating scales. Secondary outcomes included adverse events.
Statistical analysis
Continuous outcomes (ie, change in core symptoms) were recorded as the mean relative changes from baseline (where possible) or mean end-point values and SD. Meta-analysis was conducted for each core symptom that was reported in more than one study. Since the scales differed across the studies, the effect size was calculated using standard mean differences (SMD) and 95% CI. We employed a random-effects model for all analyses.
For crossover trials, endpoints of both periods were combined for each treatment arm. For studies with multiple treatment arms, only the relevant intervention arms were taken into consideration.
We measured the inconsistency of study results using the I2 heterogeneity statistic to determine if the variation in outcomes across trials was due to study heterogeneity rather than chance (Higgins 2011). I2 values of 25% indicate low heterogeneity, 50% indicate moderate heterogeneity and 75% indicate high heterogeneity.13 Heterogeneity was further explored by subgroup analysis (discussed below).
Subgroup analyses
Where I2 was found to be >50%, we performed subgroup analyses based on the type of long-acting formulation used.
Sensitivity analysis
A sensitivity analysis based on risk of bias using only studies rated with a low-risk of bias in all six domains of the risk of bias tool was planned; however, since no study met this requirement, this analysis was not conducted.
All calculations were performed using the Cochrane Collaboration's Review Manager Software (RevMan 2008).
Results
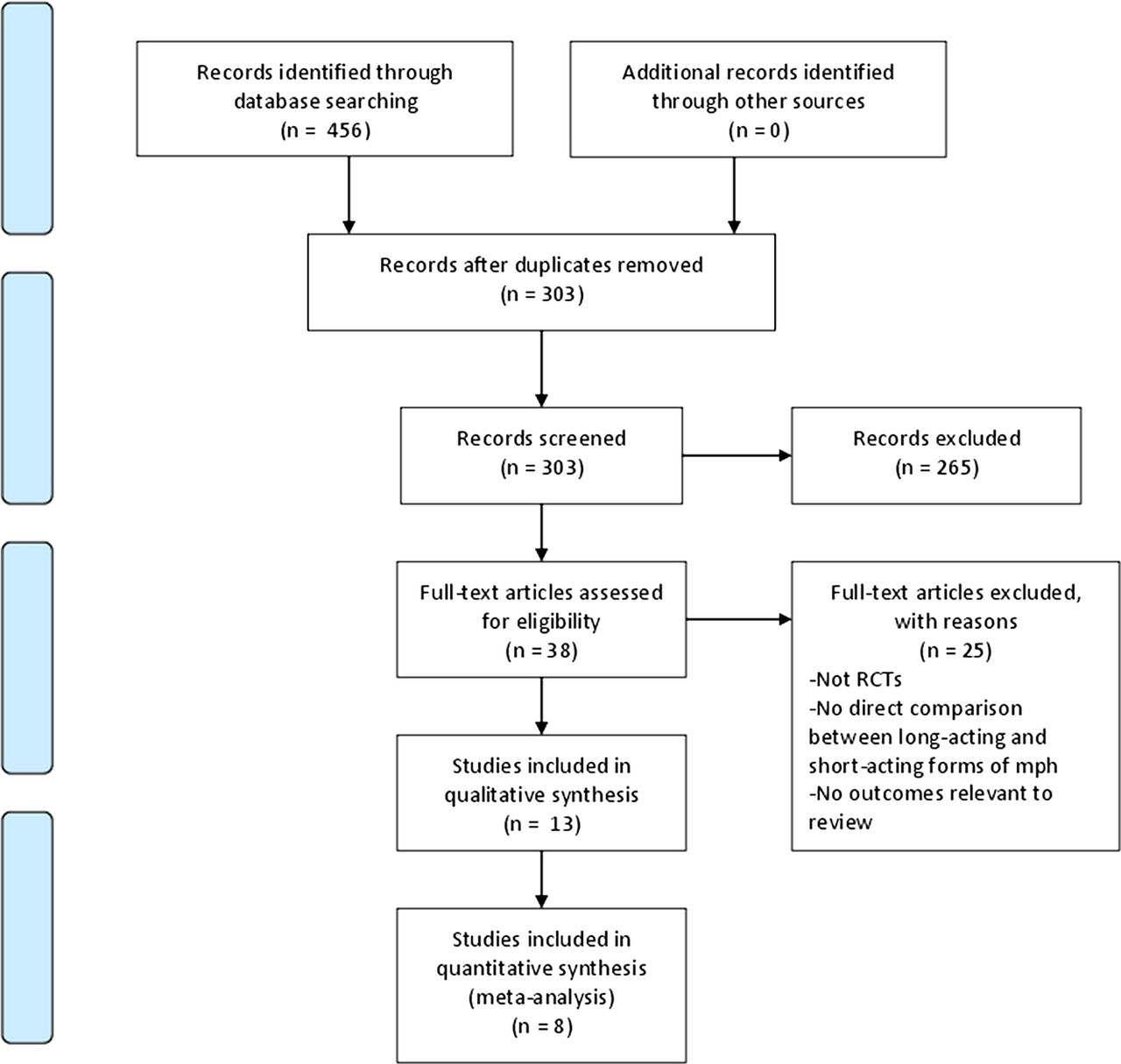
The search of the electronic databases retrieved 456 publications. After eliminating duplicates, 303 publications were identified for further consideration. After screening the titles and available abstracts, 38 studies were considered for possible inclusion. Of those 38 studies, 13 met criteria for inclusion in the view.10 ,14–25 The flow of studies through the screening process of the review is shown in figure 1 and are reported based on the PRISMA guidelines.26 The 13 eligible studies included 8 crossover RCTs and 5 parallel RCTs. The number of participants per study ranged between 13 and 272, with a total of 1031 participants. The average age of the participants of the included studies ranged from 8.25 to 11.3 years. Four studies used first generation long-acting methylphenidate, five studies used the second generation formulation and four studies assessed OROS methylphenidate. Characteristics of the included studies can be found in table 1.
Characteristics of included studies

PRISMA flow diagram.
Risk of bias
Trials consistently failed to describe sequence generation and allocation concealment, resulting in a mostly unclear risk of bias assessment with respect to those domains. Most trials sufficiently described their blinding methods and addressed their incomplete data. It was not possible to assess for selective reporting, as protocols were not made available for any of the studies. The area where the majority of trials were assessed as having a high risk of bias was in the ‘other sources of bias’ domain, owing to sources of funding. Ten studies reported that they were affiliated with or funded by industry.10 ,15 ,17–21).
Meta-analysis
Primary outcomes
Ten studies reported on the core symptoms of ADHD.14 ,16–22 ,24 ,25 Most studies used both parent and teacher reports to assess symptoms, except Steele et al, who used only parent reports, and Dopfner et al, who used only teacher reports (figure 2).19 ,22 The study results of Dopfner et al could not be included in the meta-analysis since the study was conducted over a single day. The study results of Schachar et al could not be included in the meta-analysis because the study did not specify who had completed the questionnaire.

{kind=link}
{kind=link}
(A) Teacher reports: inattention/overactivity meta-analysis. (B) Parent reports: inattention/overactivity meta-analysis. (C) Teacher reports: inattention meta-analysis. (D) Parent reports: inattention meta-analysis. (E) Teacher reports: hyperactivity meta-analysis. (F) Parent reports: hyperactivity meta-analysis. (G) Teacher reports: hyperactivity/impulsivity meta-analysis. (H) Parent reports: hyperactivity/impulsivity meta-analysis.
Inattention/overactivity (a) Teacher reports: four studies used teacher ratings to report inattention/overactivity.16–18 ,20 The meta-analysis showed no significant differences between the short-acting and long-acting forms (SMD of −0.04 (95% CI −0.31 to 0.23)). (b) Parent reports: five studies used parent ratings to report inattention/overactivity.16–18 ,20 ,22 The meta-analysis revealed no significant differences between the methylphenidate formulations; however, heterogeneity was high at 83%. Subgroup analysis was conducted by the type of long-acting formulation (1st generation vs 2nd generation vs OROS generation) and found significant differences between the short-acting and long-acting forms of methylphenidate in the second and OROS generation subgroups. The second generation subgroup favoured short-acting methylphenidate with an SMD of 0.42 (95% CI 0.17 to 0.68), while the OROS generation subgroup favoured the long-acting form, with an SMD of 0.35 (95% CI −0.52 to 0.17).
Inattention (a) Teacher reports: four studies used teacher ratings to report inattention.14 ,18 ,21 ,24 The meta-analysis revealed no significant differences between formulations (SMD 0.07 (95% CI −0.11 to 0.24)). (b) Parent reports: three studies used parent ratings to report inattention 18 ,21 ,24 and the pooled results showed no significant difference (SMD−0.12 (95% CI− 0.31 to 0.06)).
Hyperactivity (a) Teacher reports: three studies used teacher ratings to report hyperactivity.14 ,16 ,24 The meta-analysis showed significant results in favour of the short-acting form, with an SMD of 0.29 (95% CI 0.05 to 0.52) (figure 2B). (b) Parent reports: two studies used parent ratings to report hyperactivity,16 ,24 and the meta-analysis revealed no significant differences between methylphenidate formulations (SMD −0.01 (95% CI of −0.28 to 0.25).
Hyperactivity/Impulsivity (a) Teacher reports: two studies used teacher ratings to report hyperactivity/impulsivity.18 ,21 The meta-analysis revealed no significant difference between short-acting and long-acting formulations (SMD −0.00 (95% CI −0.24 to 0.24)). (b) Parent reports: three studies used parent ratings to report hyperactivity/impulsivity.14 ,18 ,21 The meta-analysis revealed significant results favouring the long-acting form, with an SMD of −0.31 (95% CI −0.51 to −0.08).
Adverse events
Twelve of the 13 included studies reported on adverse events;14–18 20–25 however, one of these studies did not provide clear numbers of adverse events.14 Forty-two adverse events were extracted from 11 studies, of which the most commonly reported adverse events included anorexia, headaches, abdominal pain and insomnia in both formulations (see table 2). The long-acting formulations presented with slightly more total reported adverse events (n=578) as compared with the short-acting formulations (n=566).
Adverse events extracted from each study
Discussion
While the therapeutic effect of short-acting methylphenidate has been well established, the introduction of more expensive, long-acting formulations in the market makes comparative effectiveness and safety paramount. The findings from this systematic review indicate that the long-acting forms have a modest effect on the severity of inattention/overactivity and hyperactivity/impulsivity according to parent reports, whereas the short-acting methylphenidate was preferred according to teacher reports for hyperactivity. These discrepancies between parent and teacher ratings may reflect differing demands between home and school environments; therefore, determining the environment in which a child's ADHD symptoms most affect them may help guide appropriate treatment decisions.
While our study demonstrates a slight preference towards the long-acting or short-acting methylphenidate on certain core symptoms, depending on the environment, we recognise that our results depend on the internal validity of the included studies. Not one of the included primary studies had a low risk of bias rating on all domains of the Cochrane risk of bias tool, which can result in overestimates of treatment effect.27 In addition, we are unable to examine claims regarding the comparative efficacy of long-term use of these formulations (ie, beyond 8 weeks use). Twelve studies were of only 4 weeks duration; only one evaluated treatment effect at 8 weeks. Short trials are particularly problematic in a chronic condition such as ADHD, as children receive stimulant medications for much longer time periods than what was studied in these trials. In addition, the results of our review may have been influenced by the inclusion of several studies affiliated with or funded by pharmaceutical companies. This has been shown to be strongly associated with an overestimate of treatment effect in favour of the sponsor's interest, thereby potentially distorting the true measures of outcome in this review.28
Our review found no difference in the reported adverse events between the two formulations, but this warrants cautious interpretation. The included studies were powered to assess efficacy, not safety, so the lack of statistical difference between groups is not surprising. We also found that adverse event reporting was often unclear among the primary studies. For example, some studies only reported on adverse events that were experienced by a certain percentage of the participants within their trial, thereby ignoring any adverse events reported by less than that fraction. Moreover, studies were unclear about how and when they ascertained adverse events, and whether they were associated with the interventions themselves. Heterogeneous terms used to describe adverse events also limited our ability to meaningfully synthesise the adverse event data, which limits its utility. Finally, as with efficacy data, long-term safety data are not available because of the paucity of long-term trials.
Limitations of our review include not including grey literature in our search, which would exclude unpublished work. Since published trials are known to describe a larger treatment effect than unpublished trials,29 excluding grey literature may result in an over-estimate of treatment effect. We did not report on indirect outcomes, such as quality of life, social functioning, academic achievement or patient preference. While these indirect outcomes are impacted by ADHD,3 our primary interest was the effect of the two medication classes on the core symptoms of ADHD, since this is the reason they are prescribed. We also chose not to include physician or child self-report regarding core symptom assessment, thereby excluding potentially important perspectives on treatment effect. Instead, we chose parents and teachers as guidelines identify their perspective as being the most important to clinicians and researchers regarding a child's naturalistic functioning in relation to peers of the same age and sex.30 ,31
Future trials should assess the long-term comparative effectiveness and safety of ADHD stimulant medications. Although issues with compliance are a primary motivation to use long-acting medications, only three studies reported compliance. While one supports greater compliance in those taking the long-acting formulation (Steele et al), the other two found no difference in compliance between the two formulations (Pelham 2001, Schachar et al). Future studies should report compliance in order to allow determination of the cost-to-benefit ratio of long-acting versus short-acting formulations. It would also be helpful if future studies separated ADHD subtypes in their analyses, in order to note important differences in treatment effects, and reported all adverse events in all participants, to allow for more meaningful data synthesis. Future research should take into account not only symptom management but also global outcomes and patient preference.
Based on the findings of this review, neither long-acting or short-acting forms of methylphenidate alleviate all core symptoms of ADHD across both home and school environments. Long-acting formulations can cost up to 15 times more than the generic short-acting formulation, without evidence of greater compliance. For children whose ADHD symptoms are impacting their school performance, parents and healthcare providers can be confident that short-acting methylphenidate will be found to be effective by teachers. Further research is needed to investigate the long-term costs, benefits, and harms of both formulations of methylphenidate in ADHD patients of all sub-types.
Acknowledgments
The authors would like to thank Ben Vandermeer for his assistance with the statistical analysis.
References
Supplementary materials
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
Files in this Data Supplement:
- Data supplement 1 - Online supplement
Footnotes
-
-
Contributors SP and SV conceived this review. SP led the design and ongoing coordination of this review with oversight from SV. SP developed the additional search strategies and carried out the searches for this review. SP organised the retrieval of papers for this review. SP and LZ screened the retrieved papers against inclusion criteria for this review. SP and LZ settled disagreements regarding the included studies for this review through discussion. SP and LZ independently appraised the quality of papers for this review. SP and LZ independently extracted data from papers for this review. SP wrote to the authors of the included studies for additional information for this review. SP managed data for this review including entering data into RevMan and analysing the data with the assistance of Ben Vandermeer. SP interpreted the data for this review. SP wrote the review. JN, LH, LU, LZ and SV critically read and edited the review prior to submission.
-
Funding This research received no specific grant from any funding agency in the public, commercial or not-for-profit sectors.
-
Competing interests SV receives salary support from Alberta Innovates Health Solutions.
-
Provenance and peer review Not commissioned; externally peer reviewed.
-
Data sharing statement No additional data are available.