Article Text

Abstract
Objectives The aim of this systematic review is to appraise the evidence for the use of anti-VEGF drugs and steroids in diabetic macular oedema (DMO) as assessed by change in best corrected visual acuity (BCVA), central macular thickness and adverse events
Data source MEDLINE, EMBASE, Web of Science with Conference Proceedings and the Cochrane Library (inception to July 2012). Certain conference abstracts and drug regulatory web sites were also searched.
Study eligibility criteria, participants and interventions Randomised controlled trials were used to assess clinical effectiveness and observational trials were used for safety. Trials which assessed triamcinolone, dexamethasone, fluocinolone, bevacizumab, ranibizumab, pegaptanib or aflibercept in patients with DMO were included.
Study appraisal and synthesis methods Risk of bias was assessed using the Cochrane risk of bias tool. Study results are narratively described and, where appropriate, data were pooled using random effects meta-analysis.
Results Anti-VEGF drugs are effective compared to both laser and placebo and seem to be more effective than steroids in improving BCVA. They have been shown to be safe in the short term but require frequent injections. Studies assessing steroids (triamcinolone, dexamethasone and fluocinolone) have reported mixed results when compared with laser or placebo. Steroids have been associated with increased incidence of cataracts and intraocular pressure rise but require fewer injections, especially when steroid implants are used.
Limitations The quality of included studies varied considerably. Five of 14 meta-analyses had moderate or high statistical heterogeneity.
Conclusions and implications of key findings The anti-VEGFs ranibizumab and bevacizumab have consistently shown good clinical effectiveness without major unwanted side effects. Steroid results have been mixed and are usually associated with cataract formation and intraocular pressure increase. Despite the current wider spectrum of treatments for DMO, only a small proportion of patients recover good vision (≥20/40), and thus the search for new therapies needs to continue.
- Ophthalmology
this is an open-access article distributed under the terms of the creative commons attribution non-commercial license, which permits use, distribution, and reproduction in any medium, provided the original work is properly cited, the use is non commercial and is otherwise in compliance with the license. see: http://creativecommons.org/licenses/by-nc/2.0/ and http://creativecommons.org/licenses/by-nc/2.0/legalcode.
Statistics from Altmetric.com
Article summary
Article focus
-
To review the evidence for triamcinolone, dexamethasone, fluocinolone, bevacizumab, ranibizumab, pegaptanib and aflibercept in the treatment of diabetic macular oedema.
Key messages
-
The anti-VEGFs ranibizumab and bevacizumab have consistently shown good clinical effectiveness in the short term without major unwanted side effects.
-
Steroid results have been mixed and are usually associated with cataract formation and IOP increase.
Strengths and limitations of this study
-
A robust, detailed review of the literature has been undertaken and, when appropriate, data have been combined in meta-analysis.
-
The quality of studies included varied considerably.
Introduction
Diabetic macular oedema (DMO) is a complication of diabetic retinopathy and a leading cause of blindness. The prevalence of DMO is likely to increase with more people suffering from diabetes.1 Increasing DMO has significant implications for patients, healthcare providers and wider society. Laser has been the mainstay of treatment, but recently antivascular endothelial growth factor (anti-VEGF) drugs and steroids have been introduced as potential alternatives to laser photocoagulation.
Burden of disease
Diabetic retinopathy is present at the time of diagnosis of diabetes mellitus in 0–30% of individuals.2 The incidence is estimated to be 2.3/100 person-years for the overall diabetic population and 4.5 for patients on insulin therapy.3 There is good evidence that progression to DMO is associated with duration of disease,4–7 poor glycaemic control8 and, in type 2 diabetes, the need for insulin,9 though the need for insulin therapy is more a marker for duration and poor control.
The number of people with DMO is likely to increase as diabetes becomes more common. Some reports have suggested a decrease in progression to severe visual loss between 1975–1985 and 1986–2008 in a combined population of types 1 and 2.10 Regular screening for retinopathy and better glycaemic control are thought to have reduced the progression to severe visual loss. Diabetic retinopathy is associated with a reduced quality of life. Compared with all diabetic complications, blindness was perceived to be the third worst health state after a major stroke and amputation.11
In the USA, the presence of DMO at diagnosis is associated with 29% additional costs within the first 3 years compared with individuals without retinopathy at diagnosis.12 In 2010, the estimated healthcare costs for DMO in England were £92 million, with £65.6 million being spent on hospital treatment and related costs.13
Visual impairment results in increased welfare costs, early retirement and costs of home help and carers.14 In England in 2010 (total population 52.23 million), the estimated population with diabetes was 2.34 million; the above social costs were estimated to be £11.6 million for DMO.13
Overview of pathophysiology
DMO is caused mainly by disruption of the blood-retinal barrier. The complex pathway that leads to this disruption has been previously described in this journal.15 Sustained hyperglycaemia causes a multifactorial cascade of physiological processes, involving increased permeability, cytokine activation, altered blood flow, hypoxia and inflammation. Vascular endothelial growth factor-A (VEGF-A) is a major contributor to the inflammatory process and, in particular, to angiogenesis and permeability.16 Hypoxia caused by microvascular disease stimulates the release of VEGF-A to aid perfusion. There are six major isoforms of VEGF-A: 121, 145, 165, 183, 189 and 206. In addition to causing widespread microvascular injury, there is now evidence that hyperglycaemia results in preceding neuronal dysfunction, which may contribute to visual loss.17
Overview of current treatments
Laser photocoagulation has been the mainstay of treatment for DMO. The landmark Diabetic Retinopathy Study18 and the Early Treatment Diabetic Retinopathy Study (ETDRS)19 ,20 demonstrated its clinical effectiveness. However, although laser photocoagulation was clearly effective in preserving vision, it was less successful in restoring it, once lost. Furthermore, patients with perifoveal ischaemia are not amenable to this form of therapy. In EDTRS, although laser was shown to reduce the risk of moderate visual loss (a loss of three ETDRS lines) by 50%, visual acuity improved in only 3% of patients.20 However, in some recent trials, laser has improved the proportion of patients with more than or equal to 10 letters by 7–31%.21–24 In addition, laser is not without side effects. Foveal burns, visual field defects, retinal fibrosis and laser scars have been reported.25 Over the following decade it became apparent that certain patients suffered severe visual loss despite aggressive treatment.26
Steroids and anti-VEGF drugs are newer treatments in DMO. Intravitreal corticosteroids have potent anti-inflammatory effects. Triamcinolone (Kenalog) is not licensed for eye use but has been used to treat DMO for over 10 years. Triamcinolone (Trivaris), recently, was licensed for eye use. The development of intravitreal implants has allowed sustained release formulations. Fluocinolone acetonide (Iluvien, Alimera Sciences) and dexamethasone (Ozudex, Allergan) are implants that have been introduced recently.
Anti-VEGF agents have shown efficacy compared with laser. Bevacizumab (Avastin, Genenetch/Roche) is a monoclonal antibody that targets all VEGF isoforms. Although being developed for colorectal cancer, it is widely used off-label, as an intravitreal treatment for macular oedema of different aetiologies. Ranibizumab (Lucentis, Genentech/Roche) is a fragment of the bevacizumab antibody (molecular weight of ranibizumab 48.4 KDa compared with 149 KDa for bevacizumab). It was designed specifically for use in the eye. Ranibizumab is considerably more expensive than bevacizumab (the estimated cost of ranibizumab is $2000/dose compared with $50 for bevacizumab).27 Pegaptanib (Macugen, Eyetech Pharmaceuticals/Pfizer) is a PEGylated aptamer, with a high affinity to the VEGF isoform 165, and was approved for the treatment of exudative AMD in 2004. Aflibercept (Regeneron/Bayer HealthCare) is a recent addition to the anti-VEGF class that targets all forms of VEGF-A and placental growth factor.
Aim of the review
The aim of this review is to provide clinicians with an up-to-date overview of current intraocular drug treatments for DMO. It is hoped that the information contained herein will assist clinicians to present their patients with the best evidence supporting each treatment, including possible complications. In addition, this review may be helpful to policy makers. The review focuses on the current evidence for the use of anti-VEGF drugs and steroids to treat DMO, as assessed by change in best corrected visual acuity (BCVA) (mean and proportion with more than two lines improvement), central macular thickness (CMT), as determined by optical coherence tomography (OCT), and their adverse events.
Evidence acquisition
A systematic literature search was performed. The databases searched included MEDLINE, EMBASE, Web of Science with Conference Proceedings and the Cochrane Library. The dates searched were from the inception of each database until July 2012.
The search terms combined the following key words:
ranibizumab or lucentis or bevacizumab or avastin or pegaptanib or macugen or aflibercept or vegf trap-eye or steroid* or corticosteroid* or dexamethasone or fluocinolone or triamcinolone or anti-VEGF* or anti-vascular endothelial growth factor*
AND
DMO or diabetic macular edema or diabetic retinopathy or diabetic maculopathy
AND
(masked or sham or placebo OR control group or random*) OR (systematic review or meta-analysis) OR (risk or safety or adverse or harm or pharmacovigilance or side-effect* or precaution* or warning* or contraindication* or contra-indication* or tolerability or toxic)
The meeting abstracts of the Association for Research in Vision and Ophthalmology, the American Diabetes Association (2002–2012) and the European Association for the Study of Diabetes were searched from 2002 to 2012.
In addition, the web sites of the European Medicines Agency and the US Food and Drug Association were searched for data on registration status and safety. Clinicaltrials.gov and the EU Clinical Trials Register were searched in July 2012 for data on ongoing research.
Full details of the searches are shown in appendix 1.
Randomised controlled trials (RCT) were used to evaluate clinical effectiveness. Safety was assessed through both RCTs and observational studies.
RCTs were included provided that they (1) addressed the use of triamcinolone, dexamethasone, fluocinolone, bevacizumab, ranibizumab, pegaptanib or aflibercept in patients with DMO, (2) had a minimum follow-up of 6 months and (3) had a minimum of 25 eyes per study arm. Studies were excluded if they (1) evaluated laser only, (2) assessed the effect of the aforementioned treatments in macular oedema due to other retinal diseases (instead of DMO), (3) used only a single dose, (4) were combined with a surgical intervention or (5) published studies in languages other than English. There were no exclusions based on drug dose. Trials were excluded if they evaluated combined drug treatment with surgery or systemic treatment.
Search results were screened by two independent authors (JF and PR/DS). Data were extracted by one author (CC) and checked by a second (JF). Data extracted included inclusion/exclusion criteria, baseline demographics, BCVA expressed as a change in logMAR/ETDRS letters or proportion of participants with more than two or three lines BCVA improvement, CMT and adverse events. Risk of bias was assessed using the Cochrane risk of bias tool.
Studies were assessed for similarity in study population, interventions (dose and frequency), outcomes and time to follow-up, with a view to including similar studies in a meta-analysis. Conference abstracts were excluded from the meta-analysis because their quality and detailed methodology were not clear. A difference of 6 months was allowed between study follow-ups because of the potential heterogeneity from disease progression and differences in the number of doses prescribed. If salient data were not reported, such as SDs, data were sought by personal communication with authors. Data were analysed using Review Manager software. If data from multiple time-points were available, the primary end-point data were used. Data were entered by one author (JF) and double-checked by a second (DS). Mean differences were calculated for change in BCVA and CMT and ORs were calculated for proportion of participants with more than two lines improvement. The 95% CIs were calculated for all outcomes. Statistical heterogeneity was measured through I2 scores. A score of less than 30% was considered as low heterogeneity, a score of more than 70% was considered as high heterogeneity and scores between 30% and 70% were considered as moderate. A random effects model was used throughout. The random effects model assumes variability between studies and therefore models uncertainty into the meta-analysis. Fixed assumes no variability. Generally speaking, the random effects model results in wider CIs.
Results
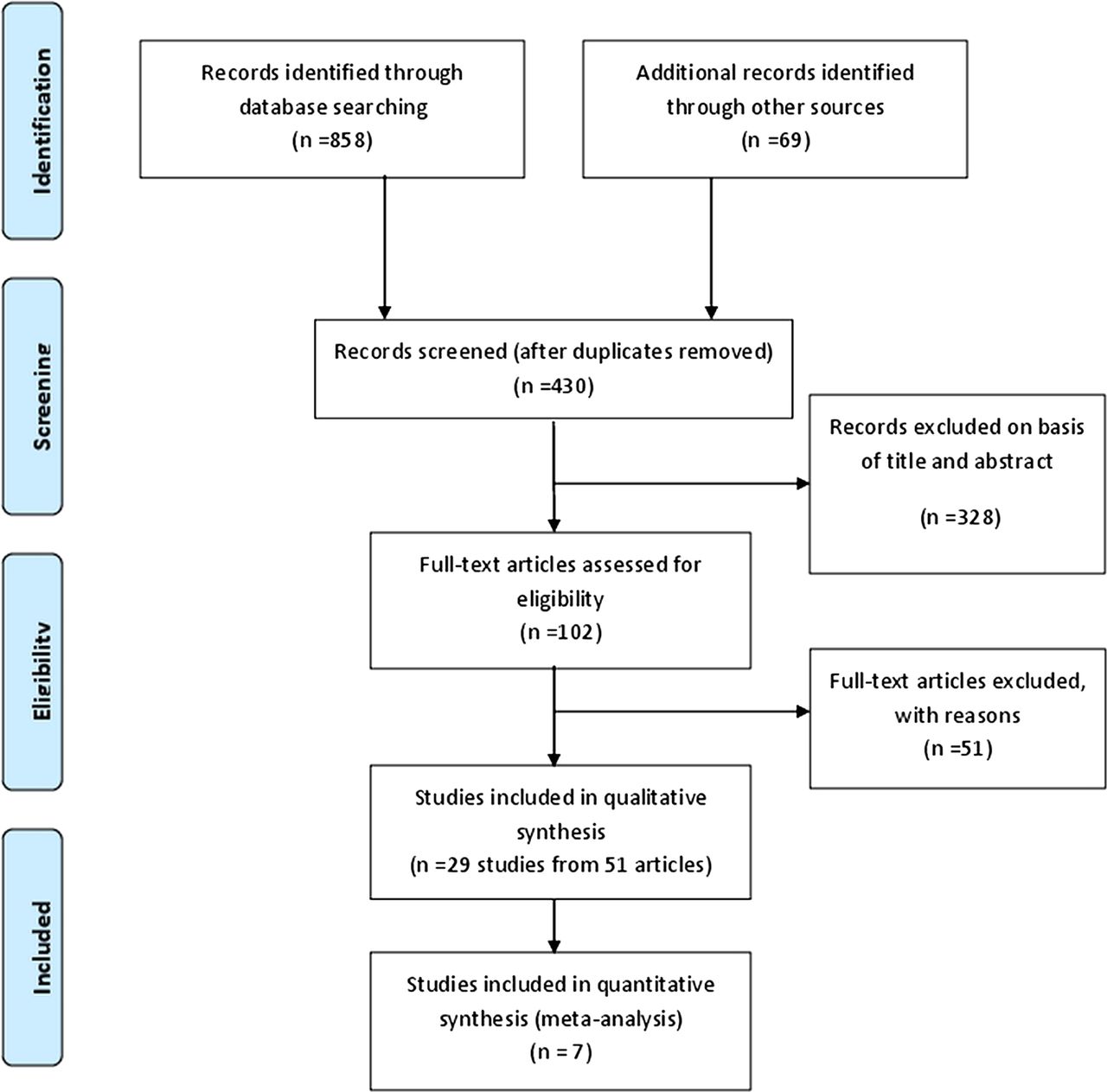
The literature search identified 430 unique articles for possible inclusion, as shown in figure 1. In total, 328 articles were excluded on the basis of title and abstract, leaving 102 full papers to be read. Fifty-one of these articles were excluded; the reasons for their exclusion are summarised in table 1. Fifty-one articles from 29 studies met the inclusion criteria and were included in the review; these are described in tables 3⇓⇓⇓⇓⇓⇓⇓⇓⇓⇓⇓⇓–16. Seven studies were suitable for meta-analysis.
List of excluded studies
Study quality
Ranibizumab trials
Bevacizumab studies
Pegaptanib and aflibercept studies
Dexamethasone and fluocinolone studies
Triamcinolone studies
Trials assessing more than one drug
Ranibizumab safety data
Bevacizumab safety
Pegaptanib safety
Aflibercept safety
Dexamethasone safety
Fluocinolone safety
Triamcinolone safety
Safety data in trials assessing more than one drug

PRISMA flow diagram.
Study quality
The quality of the included studies was, in general, good as is shown in table 2. (Note that the meeting abstracts were not quality assessed, owing to the lack of details reported on the methods.) Most studies adequately described sequence generation, except in three studies where it was unclear.28–30 However, allocation concealment was poorly described throughout, with only eight reports addressing this issue appropriately.31–38 Reporting of masking also varied. A number of studies masked patients using sham injection or sham laser.21 ,24 ,29 ,31 ,33 ,36 ,38 ,39 ,40 Various studies reported that masking of patients was impossible. Assessors, where reported, were masked. In two studies, incomplete outcomes were not addressed.31 ,41 Baseline characteristics were consistent within study treatment arms. Administration of laser followed the ETDRS protocol, or a modified version, in all studies that described laser administration.21–24 ,28 ,30 ,33 ,34 ,42 ,43 Two studies, both available only as meeting abstracts, did not report the laser administration details.44 ,45
Intravitreal anti-VEGFs
The characteristics of all published studies including design, inclusion/exclusion criteria, intervention, outcomes and their timing are shown in tables 3⇑⇑⇑⇑–8. Safety data for each drug are shown in tables 9⇑⇑⇑⇑⇑⇑–16.
Ranibizumab
Nine RCTs have evaluated ranibizumab as a potential new treatment for patients with DMO (tables 3 and 8); seven were sponsored by industry, and two were led by independent investigators)(table 7).21 ,46 READ-2 was the first large RCT (n=126).28 ,47 It compared ranibizumab (0.5 mg) alone, and ranibizumab in combination with laser and laser alone. At 6 months, BCVA had improved significantly in the ranibizumab alone group compared with laser alone or ranibizumab plus laser. Addition of laser to ranibizumab did not provide additional BCVA gain. REVEAL (n=396) compared ranibizumab (0.5 mg) with ranibizumab plus laser and laser alone.48 At 12 months, both ranibizumab arms resulted in a statistically significantly better improvement in BCVA compared to laser alone. The addition of laser did not confer further benefit.
Within the past 2 years, the results of RESOLVE,36 RESTORE24 and RISE and RIDE38 have been published in peer-reviewed journals. RESTORE (n=345) randomised similar groups as the READ-2 study (ranibizumab (0.5 mg) alone, laser alone and ranibizumab plus laser); outcomes were evaluated at 12 months. Ranibizumab improved mean BCVA, with laser providing no additional benefit. Two-year extended follow-up suggested that these results continued.49 RESOLVE (n=151) compared two doses of ranibizumab (0.3 and 0.5 mg) with sham injection. The greatest improvement in BCVA at 12 months was in the 0.3 mg group (11.8 letter gain) compared to the 0.5 mg group (8.8 letter gain) or sham injection (1.4 letter loss). In this study, rescue laser was allowed after 3 months of treatment, if BCVA had decreased by 10 letters or more, or if the investigator considered the macula not to be flat as assessed by OCT. Only 4.9% of the ranibizumab group required rescue laser, compared with 34.7% in the sham injection group.
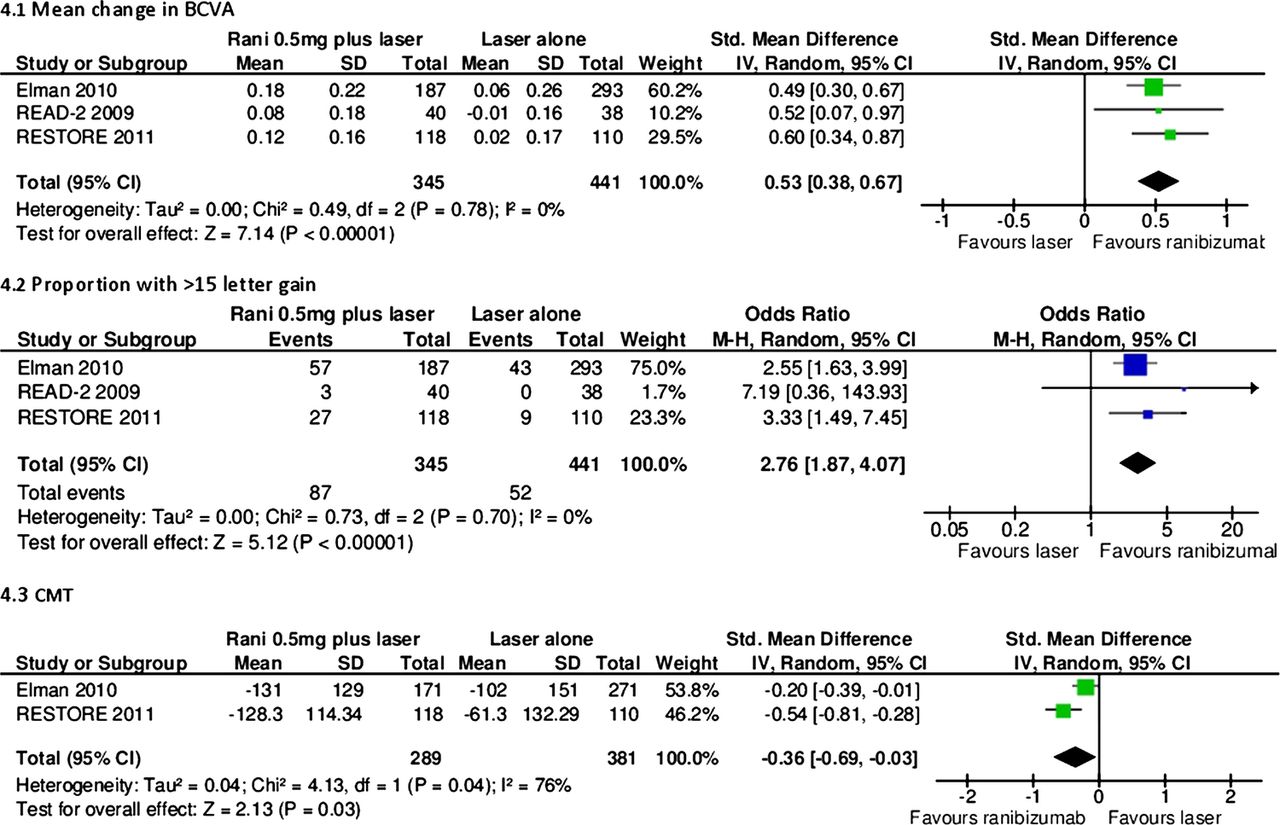
READ-2 and RESTORE were suitable for pooling through meta-analysis and, when doing so, it was found that ranibizumab statistically significantly improved mean BCVA compared with laser (figure 2). In regard to the proportion of patients gaining more than or equal to 15 letters, individual trials showed a statistically significant difference between laser and ranibizumab but when these two trials were pooled using a random effects model, the result was no longer statistically significant. When a fixed effects model was used, the result was statistically significant (figure not shown). Adding laser to ranibizumab did not add any significant benefit (figure 3). In fact, the mean change in BCVA and the proportion of patients with more than 15 letter gain favoured, although not statistically significantly so, ranibizumab alone compared with ranibizumab plus laser. This was probably a chance effect.

Ranibizumab 0.5 mg alone versus laser alone. (A) Mean change in best corrected visual acuity. (B) Proportion with >15 letter gain. (C) central macular thickness.

Ranibizumab 0.5 mg plus laser versus ranibizumab 0.5 mg alone. (A) Mean change in best corrected visual acuity. (B) Proportion with >15 letter gain. (C) central macular thickness.
RISE (n=377) and RIDE (n=382) were identical in design. The study arms are similar to those in the RESOLVE study, 0.3 or 0.5 mg ranibizumab compared with sham. In the RISE study, the proportion of patients with 15 or more letter gain was greatest in the 0.3 mg group at 24 months, whereas in the RIDE study this was greatest in the 0.5 mg group. In the DRCRN trial (n=854), Elman and colleagues compared ranibizumab (0.5 mg) plus prompt (within 3–10 days post ranibizumab) or deferred (≥24 weeks) laser with sham injection plus prompt laser, or triamcinolone (4 mg, Trivaris) plus prompt laser (table 8). At 1 year, both ranibizumab groups reported greater gains in mean BCVA change than triamcinolone or laser alone. Interestingly, at 2 years (n=628), the proportion of patients with 10 or more letter gain was not statistically significantly different between ranibizumab plus prompt laser and laser alone groups, but was statistically significant in the ranibizumab plus deferred laser compared with laser alone comparison. The reason for this is not clear.
READ-3 (n=152) has been published in abstract form and compared monthly injections of intravitreal ranibizumab high dose (2.0 mg) and low dose (0.5 mg).50 At 6 months, there was no statistically significant difference in BCVA between groups.
One study (n=63), published in abstract form, was identified which directly compared monthly injections of ranibizumab (0.5 mg) with bevacizumab (1.5 mg).51 At 48 weeks, the authors found no statistically significant difference between bevacizumab and ranibizumab.
RESTORE, READ-2 and DRCRN (12 month data used) were suitable for pooling through meta-analysis to compare ranibizumab plus laser and laser alone (figure 4). Ranibizumab plus laser resulted in a statistically significantly greater change in mean BCVA, proportion of patients with more than 15 letter gain and CMT reduction versus laser alone.
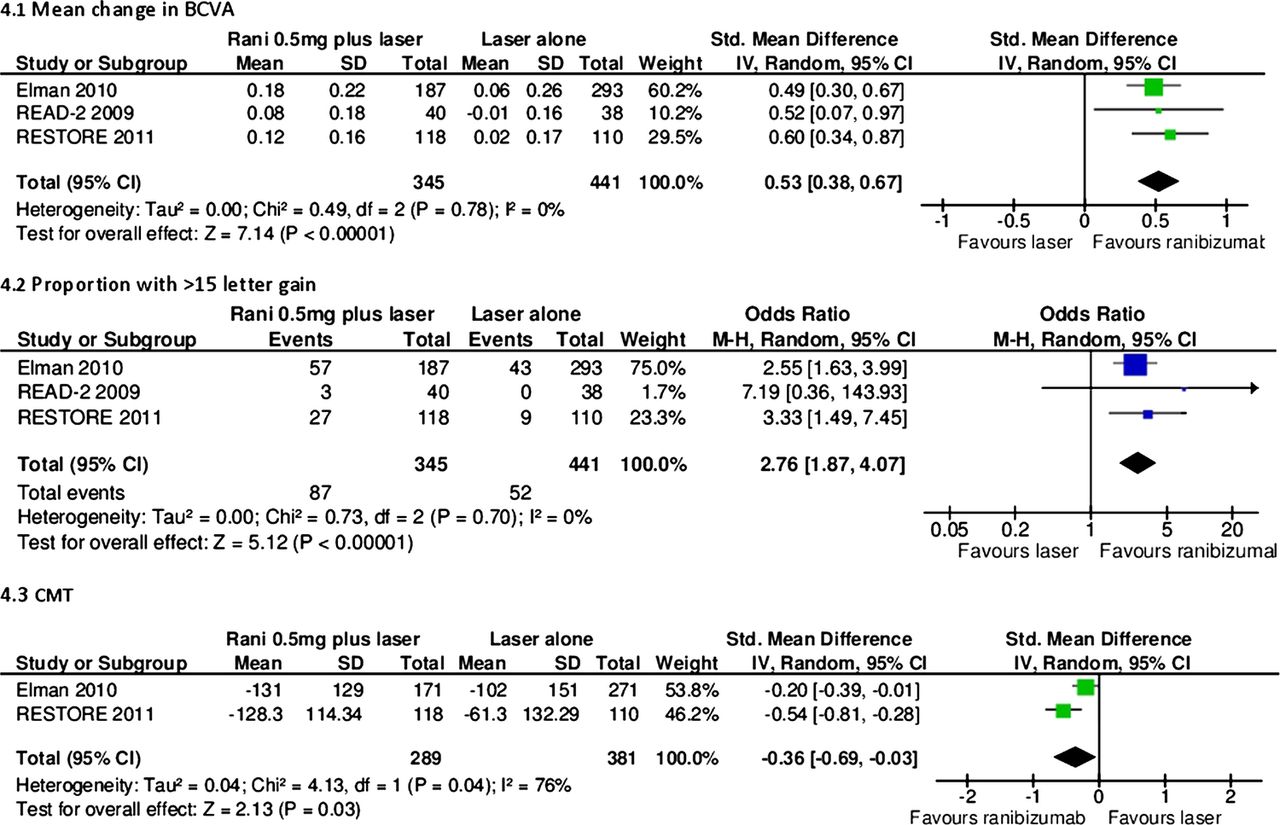
Ranibizumab 0.5 mg plus laser versus laser alone. (A) Mean change in best corrected visual acuity. (B) Proportion with >15 letter gain. (C) Central macular thickness.
Adverse events are shown in tables 9 and 16. Conjunctival haemorrhages were higher in the ranibizumab arms compared with laser (RESTORE) or no treatment (RESOLVE). In the RESOLVE, RISE and RIDE studies, a considerably higher incidence of intraocular pressure (IOP) increase was reported in the ranibizumab arm compared to control. This increase in IOP was not demonstrated in the RESTORE study. There were no consistent differences in systemic adverse events between ranibizumab and laser or placebo.
Bevacizumab
Eight RCTs investigating the use of bevacizumab in DMO were identified (tables 4 and 8). One RCT, the BOLT study (n=80), randomised patients to laser therapy or 1.25 mg intravitreal bevacizumab.23 ,52 At 24 months, the mean changes in BCVA and the proportion of patients who gained 10 ETDRS letters or more was statistically significantly higher in the bevacizumab arm than in the laser arm. Faghihi et al53 (n=80) compared 1.25 mg bevacizumab (average 2.23 injections per patient) with 1.25 mg bevacizumab plus a single laser treatment (average 2.49 injections per patient). After 6 months, the authors found both treatments to be effective at improving BCVA, but neither treatment was found to result in a greater benefit.
Lam et al35 (n=52) compared two doses of bevacizumab (1.25 and 2.5 mg) in patients with diffuse DMO. Patients with focal DMO associated with localised retinal thickening were excluded. At 6 months, following 3 initial monthly injections (no treatment in the remaining 3 months), both groups showed a statistically significantly increased mean BCVA compared with baseline vision, but there was no difference between doses.
Four trials have investigated the combination of bevacizumab and triamcinolone. Ahmadieh et al31 (n=115) compared combined bevacizumab (three 1.25 mg injections at 6 week intervals) plus triamcinolone (2 mg baseline injection only, Triamhexal) with bevacizumab alone (three 1.25 mg at 6 week intervals) and sham injection in patients who had DMO unresponsive (definition not reported) to previous laser (last session more than 3 months previously). The combination arm and bevacizumab alone arm improved mean BCVA more than the sham injection. For BCVA, the combination of bevacizumab plus triamcinolone was non-statistically significantly better than bevacizumab alone.
Soheilian et al37 ,41 (n=150) compared combined bevacizumab (1.25 mg) plus triamcinolone (2 mg) with bevacizumab alone and laser alone in patients who were laser naïve. At 36 weeks, bevacizumab alone improved BCVA more than either combination therapy or laser, although the difference was not statistically significant. Extended follow-up at 24 months showed that there was no statistically significant difference between groups for BCVA; however, the direction of effect favours the bevacizumab and combination arms more than the laser.54
Lim et al55 (n=111) also evaluated the combination of bevacizumab plus triamcinolone when compared with bevacizumab alone or triamacinolone alone. At 12 months, the authors found no statistically significant difference between groups for BCVA or CMT.
The Efficacy Study of Triamcinolone and Bevacizumab Intravitreal for Treatment of Diabetic Macular Oedema (ATEMD) study, currently only published in abstract form, compared combined therapy with bevacizumab (1.25 mg) and triamcinolone (4 mg) with each of these alone.56 At 6 months, they found no statistically significant difference between groups. One study comparing bevacizumab with ranibizumab is discussed above.51 No bevacizumab trials were suitable for meta-analysis because treatment arms were not comparable among included studies.
Adverse events are shown in tables 10 and 16.There was a low frequency of adverse events reported in the included trials. A higher incidence of mild anterior chamber reaction was reported in bevacizumab groups compared with controls. The incidence of IOP increase was comparable between bevacizumab and laser. Soheilian et al37 ,41 were the only authors to report the incidence of lens opacity. No patients in the bevacizumab alone group were found to have lens opacities but in four patients (8%) in the bevacizumab plus triamcinolone group, this finding was observed over the 36-week follow-up period.
Pegaptanib
Two studies have evaluated pegaptanib in DMO and both compared it with sham injection (table 5). Cunningham et al39 ,57 compare three doses of pegaptanib (0.3, 1 and 3 mg) and sham injection in laser-naive patients (n=172). At 6 months, patients in the 0.3 and 1 mg groups performed statistically significantly better than those in either the 3 mg or sham groups. Six injections (median) were administered in the 0.3 and 1 mg groups, whereas only five (median) injections were administered in the 3 mg group.
The second trial (n=260), reported by Sultan and colleagues in 2011, compared pegaptanib (0.3 mg) and sham injection. At 2 years, the pegaptanib group showed a statistically significantly greater improvement in mean BCVA compared with sham.40 However, there was no statistically significant difference in the proportion of patients with an improvement of 10 letters or more. Patients were allowed rescue laser at the assessors’ discretion (25.2% of patients in the pegaptanib group and 45% of patients in the sham group received rescue treatment). In regard to meta-analysis, data were only available to combine these trials for the proportion of patients with more than 15 letter gain. Although neither trial individually demonstrated a statistically significant difference favouring pegaptanib over sham (figure 5), when pooled together in meta-analysis, a statistically significant difference was found in favour of pegaptanib (OR 1.94, 95% CI 1.01 to 3.71).

Pegaptanib 0.3 mg versus sham injection. (A) Proportion with >15 letter gain.
Adverse events for pegaptanib are shown in table 11. There was a higher incidence of eye pain compared to control (31% vs 17%).39 ,57 Cataract formation was similar between the pegaptanib and control groups. There was a higher incidence of IOP increase in the pegaptanib arm compared to control (17.4% vs 6.3%).40
Other anti-VEGF
Aflibercept has been evaluated in the Da Vinci study (n=219)30 ,58 (table 5). Four regimens of aflibercept (0.5 mg 4 weekly, 2 mg 4 weekly, 2 mg monthly for 3 months, then every 8 weeks, and 2 mg monthly for 3 months followed by treatment as required) were compared with laser. At 6 months, all aflibercept arms had a statistically better BCVA and CMT change than the laser arm. The regimen that resulted in the greatest BCVA gain and CMT reduction was 2 mg every 4 weeks; however, statistical significance between aflibercept arms was not reported. One year extended follow-up showed that all aflibercept arms were found to have a statistically significantly better BCVA compared to laser.58
Adverse events are shown in table 12. There was a higher incidence of IOP increase and eye pain in the aflibercept group compared with laser. Other adverse events were too infrequent to draw meaningful conclusions. The incidence of cataracts was not reported.
Steroids
Dexamethasone
Two included trials assessed the use of dexamethasone to treat DMO (table 6): Haller 2010 (full text available)59 and Callanan (available to date only in an abstract form).44 Haller 2010 (n=171) compared two doses of dexamethasone, administered as an intravitreal implant (350 and 700 µm) through a 20-gauge transscleral incision, with no treatment. At 90 days only, the 700 µm group showed a statistically significantly higher proportion of patients with 10 or more letter gain compared to no treatment (33% compared with 12%, p=0.007). The 350 µm group showed a non-statistically significant improvement compared with laser alone (21% compared with 12%). At 180 days, there was no statistically significant difference between either the dexamethasone group or no treatment group. The treatment effect appeared to peak at 3 months.
The second trial, by Callanan and colleagues (n=253), compared dexamethasone (dose not reported) plus laser with laser alone. Although a greater improvement in mean BCVA was seen at 1–9 months in the dexamethasone plus laser group compared with laser alone, there was no statistically significant difference at 12 months. A mean of 1.6 implants were used over the 12 month period.
These trials were not suitable for meta-analysis since one study is only available in abstract form.
Adverse events are shown in table 13. In the 350 and 700 µm groups compared with no treatment, there was a higher incidence of anterior chamber cells (29.1/26.4% compared with 1.8%), anterior chamber flare (27.3/20.8% compared with 8.8%), vitreous haemorrhage (20/22.6% compared with 5.3%) and increased IOP (14.5/9.4% compared with 0%). However, there was no statistically significant difference in cataract formation between groups at 12 months.59 Callanan et al44 reported an increase in IOP in the dexamethasone plus laser group compared with laser alone (20% compared with 1.6%).
Fluocinolone
Two trials assessed fluocinolone implant for DMO (table 6). The FAME study (n=956) compared two doses of fluocinolone (0.2 and 0.5 µg/day) with sham injection in patients with at least one prior laser treatment.29 Approximately 25% of patients in each group had more than one prior laser treatment. At 24 months, both doses of fluocinolone showed a statistically significant improvement in mean BCVA compared to sham. There was a modest difference between fluocinolone groups. Rescue laser was given after the first 6 weeks for persistent oedema and was allowed every 3 months. A range of 35–37% of patients in the fluocinolone group and 59% in the sham injection group required rescue laser. Extended follow-up at 36 months showed that both the fluocinolone arms continued to result in a statistically significant benefit compared with sham.60
Pearson et al43 (n=196) compared fluocinolone (0.59 mg) with standard of care, either laser or no treatment. At 3 years, there was no statistically significant difference in the proportion of patients with 15 letter gain or more (31% fluocinolone compared with 20% standard of care) between groups and the proportion of patients losing 15 letters or more in the fluocinolone group (17% compared with 14%). Increased incidence of cataracts may have contributed to this difference.
These trials were not suitable for meta-analysis.
Adverse events are shown in table 14. Pearson and colleagues reported a higher incidence of cataracts at 3 years in the fluocinolone group compared with standard of care (55.9% compared with 21.7%). In the extended report of the FAME study, there was a considerably higher incidence of cataract surgery in phakic eyes in the 0.2 and 0.5 µg/day fluocinolone groups (80% and 87.2% compared with 27.3%) and increased IOP at any point (37% and 46% compared with 12%).
Following the demonstration in the FAME trial that a lower dose was about as good as higher ones, the higher doses are unlikely to be used.
Triamcinolone
Ten trials evaluating triamcinolone were identified (tables 7 and 8). All trials evaluated intravitreal administration of triamcinolone, but there were no trials evaluating posterior or anterior subtenon injections. Two trials used Trivaris,21 ,61 two trials used Kenacort,32 ,33 one trial used Kenalog,62 one trial used Trimahexal31 and four trials did not report the type of triamcinolone used.34 ,37,45 ,56 Three doses were assessed in the included studies (1, 4 and 8 mg) and triamcinolone has been combined with laser or bevacizumab.
Ip and colleagues (n=840) were the only authors to evaluate triamcinolone 1 mg (Trivaris).22 ,61 ,63 ,64 They found a statistically significant improvement in mean BCVA at 2 years in the laser group compared with the triamcinolone group and no significant difference between 1 compared with 4 mg.
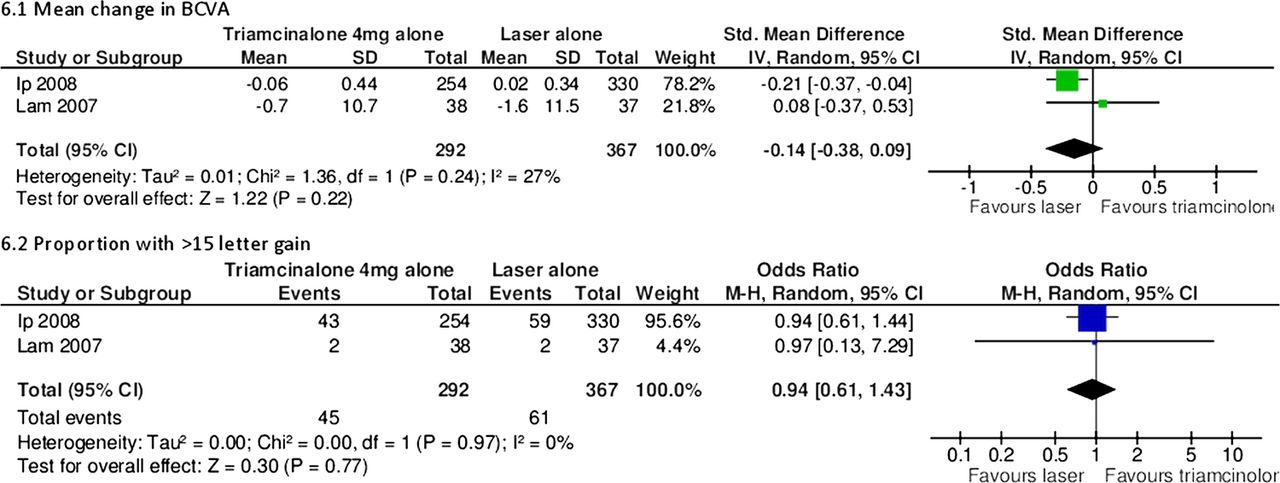
Several trials compared 4 mg intravitreal triamcinolone. Ip and colleagues (n=840) found that laser therapy resulted in a greater improvement in mean BCVA at 2 years compared to 4 mg triamcinolone (Trivaris).22 ,61 ,63 ,64 Lam et al34 (n=111) found no statistically significant difference between laser and triamcinolone at 6 months (triamcinolone type not reported). When these two trials were pooled through meta-analysis, the treatment effect favoured laser but the differences were not statistically significant (figure 6). Ockrim et al62 (n=88) compared 4 mg intravitreal triamcinolone (Kenalog) with laser alone. At 12 months, they found no statistically significant BCVA improvement between the triamcinolone and laser groups. Gillies et al32 (n=69) compared 4 mg of triamcinolone (Kenacort) with sham injection. Mean BCVA improved statistically significantly with triamcinolone at 24 months compared with sham injection (3.1 letter gain compared with 2.9 letter loss, p=0.01).

Triamcinolone 4 mg versus laser alone. (A) Mean change in best corrected visual acuity. (B) Proportion with >15 letter gain.
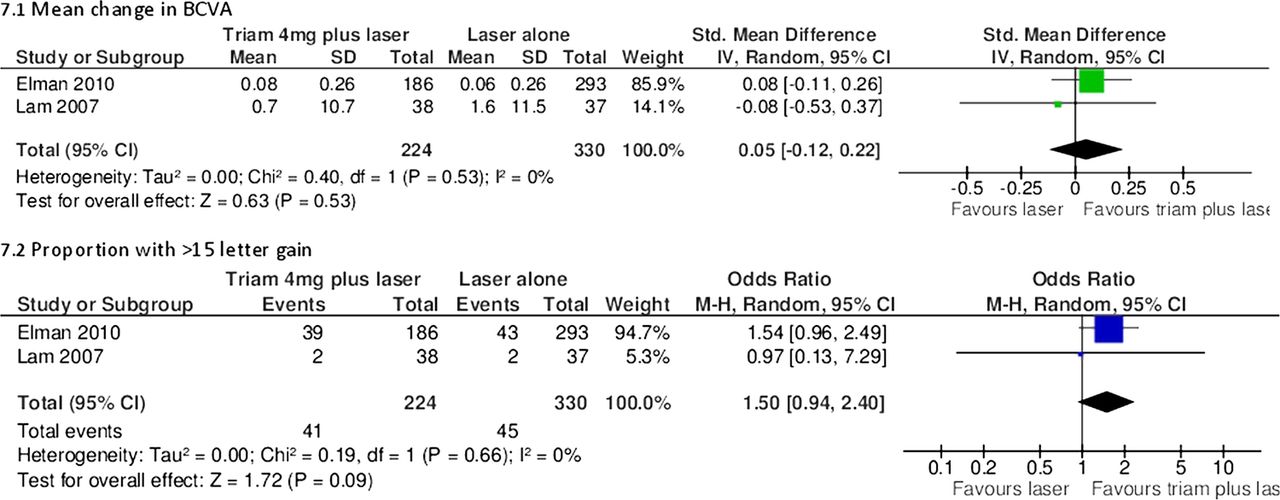
Lam et al34 (n=111) compared triamcinolone 4 mg alone with 4 mg of triamcinolone plus laser or laser alone. At 6 months, the authors found no difference in BCVA between any of the groups. Elman et al21 (n=854) compared 4 mg of triamcinolone (Trivaris) plus laser with ranibizumab plus prompt (within 3–10 days) or deferred (more than 24 week) laser and laser alone. At 2 years, they found a statistically significant difference in mean BCVA between ranibizumab plus prompt/deferred laser compared with laser alone (7 letter gain/9 letter gain compared with 3 letter gain), but no difference with triamcinolone plus laser compared with laser alone (2 letter gain compared with 3 letter gain). Neto et al56 (n=120) compared 4 mg triamcinolone alone (triamcinolone type not reported) with 4 plus 1.25 mg bevacizumab. At 6 months, they found no statistically significant difference between groups.
The Elman and Lam studies were suitable for meta-analysis, which showed non-statistically significant improvements in mean BCVA and the proportions of patients with more or equal than 15 letter gain in the triamcinolone plus laser group compared with laser alone (figure 7).

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Triamcinolone 4 mg plus laser versus laser alone. (A) Mean change in best corrected visual acuity. (B) Proportion with >15 letter gain.
Adverse events are shown in tables 15 and 16. Triamcinolone was associated with consistently higher incidences of IOP increase and cataracts. Gilles and colleagues reported a cataract rate of over 50% by 3 years in patients treated with triamcinolone.
Other pertinent studies
Only one study in abstract form directly compared bevacizumab with ranibizumab.51 Bevacizumab and ranibizumab have been compared through an indirect comparison of five trials.65 There was no evidence of a difference between the drugs; however, wide credible intervals meant that the superiority of either drug could not be excluded.
Two-year results of the CATT (Comparison of AMD Treatment Trials) and 1 year results of the IVAN (Inhibit VEGF in Age-related choroidal Neovascularisation), recently published, have demonstrated a good safety profile of anti-VEGF therapies when used to treat patients with age-related macular degeneration.66 ,67 The CATT study randomised 1208 patients with AMD to monthly or as required injection of either ranibizumab or bevacizumab. At 1 year, the mean BCVA was similar in both groups (8 letter gain in bevacizumab and 8.5 in ranibizumab). Over 2 years, the rates of deaths, myocardial infarction and stroke did not differ between the ranibizumab and bevacizumab treatment groups. However, there was a higher rate of serious adverse events in the bevacizumab group compared with the ranibizumab group. This increased event rate was driven mainly by hospitalisations (RR 1.29, 95% CI 1.01 to 1.66). However, the hospitalisations were not caused by known adverse events of bevacizumab. Arteriothrombotic events and heart failure occurred in less than 2% of participants in the IVAN, and they were more often observed in the ranibizumab group than in the bevacizumab group (p=0.03). Further data from other ongoing clinical trials may provide more insight on the safety or anti-VEGF treatment and possible differences on this respect among available drugs.
Campbell et al68 conducted a population-based nested case–control study of 91 378 older adults with a history of physician-diagnosed retinal disease. The authors found that neither ranibizumab nor bevacizumab was associated with significant risks of ischaemic stroke, acute myocardial infarction, congestive heart failure or venous thromboembolism.
A recent systematic review specifically assessing adverse events in anti-VEGF drugs found a low incidence of serious (below 1 in 100) and non-serious ocular events (below 1 in 500) from ranibizumab, bevacizumab and pegaptanib.69
Fung et al70 used an internet-based survey of clinicians to assess the safety of bevacizumab. The survey covered over 5000 patients and found that bevacizumab was associated with an infrequent incidence of adverse events (all less than 0.21%).
One study, which assessed diclofenac, did not meet the inclusion criteria (follow-up for only 12 weeks).71 The authors randomised 32 patients to either intravitreal diclofenac or triamcinolone and found that both diclofenac and triamcinolone reduced CMT, but a statistically significant visual improvement was observed only in the triamcinolone group.
Sfikakis et al72 undertook a 30-week randomised crossover trial comparing infliximab and placebo. The study failed to meet our inclusion criteria (only 11 patients included). The authors found that infliximab resulted in a 28.6% improvement in vision compared with 4.3% with placebo. The improvement seen with placebo could be due to a ‘carry over effect’, seen in cross-over trials.
The Fenofibrate Intervention and Event Lowering in Diabetes (FIELD) trial was primarily a study to see if the lipid-lowering agent fenofibrate could reduce macrovascular and microvascular events in type 2 diabetes.73 However, a substudy within FIELD recruited 1012 patients to a retinopathy study. The primary outcome in the main study was need for laser therapy (3.4% on fenofibrate vs 4.9% on placebo), but the substudy used retinal photography to assess progression of retinopathy or development of macular oedema. The HR at 6 years for DMO was 0.69 (95% CI 0.54 to 0.87) in the fenofibrate group compared to placebo.
Ruboxistaurin is another oral agent which has been assessed for the treatment of DMO. Aiello and colleagues randomised 686 patients to receive placebo or one of three doses of ruboxistaurin.74 ,75 There was no statistically significant difference in delay to sight-threatening DMO in any ruboxistaurin group compared to placebo. The authors suggest that differences in laser treatment between groups may have contributed to the non-significant finding.
Assessment of heterogeneity within meta-analysis
Heterogeneity was assessed methodologically and statistically. Methodological heterogeneity was assessed by comparing the study population, interventions, outcome measures and follow-up. Studies that were not methodologically comparable were excluded from the meta-analysis. For example, bevacizumab trials were not pooled because Soheilian et al37 included patients who were laser naïve and Ahmadieh et al31 included patients who were unresponsive to laser. Some analyses were also excluded because sufficient details were not reported in the studies. For example, several studies failed to report SDs.35 ,39
Statistical heterogeneity was assessed through I2 scores. High statistical heterogeneity was found in two analyses (2.3 and 4.3). Therefore, these results should be interpreted with due caution. Moderate heterogeneity was found in three analyses (2.2, 3.1 and 3.2). Low heterogeneity was found in the remaining eight analyses.
Ongoing trials
There are numerous ongoing studies listed in appendix 2. The most salient studies include a study to compare ranibizumab and bevacizumab (Schmidt-Erfurth), a study investigating rescue ranibizumab treatment for patients who have failed on bevacizumab (Chaudhry), a study evaluating two algorithms for ranibizumab, ‘treat and extend’ and ‘as required’ (RETAIN), further studies of Trap-eye (VIVID and VISTA) and trials which are examining the use of NSAIDs, such as diclofenac and nepafenac (NEVANAC and Soheilian).
Discussion
It appears that anti-VEGF treatment is effective in DMO, especially ranibizumab and bevacizumab. Meta-analysis of available short-term data (up to 2 years) suggests that ranibizumab is superior to laser and that adding laser to ranibizumab treatment does not confer additional benefit. Steroid treatment has demonstrated mixed success and, almost uniformly, increased the incidence of cataracts and IOP. The licence for fluocinolone takes note of this and it is positioned as a treatment when others have failed.
Strengths and limitations of the review
There are a number of strengths of this review. A robust systematic review methodology was used. Reliability was improved by excluding trials with small sample sizes or short follow-up. Since a number of trials included similar intervention arms, consistent treatment effects further improve reliability. Validity was improved by assessing the quality of trials using the Cochrane risk of bias tables. Including abstracts from ARVO provided up-to-date results. Pooling results through meta-analysis provided further evidence. The random effects model was used throughout to allow for heterogeneity among studies.
This review, however, has limitations. Although the inclusion of abstracts provides more up-to-date results, the studies contained in these abstracts could not be assessed for risk of bias and should therefore be interpreted with caution. In addition, reporting of quality assessment criteria was variable. Allocation concealment was especially poorly reported. There was only one study which compared different anti-VEGFs51 and none that compared steroids (fluocinolone vs dexamethasone vs triamcinolone). Therefore, it is difficult to assess the effectiveness within drug classes. As with any meta-analysis, questions of heterogeneity arise. Follow-up periods varied among studies. A difference of 6 months was allowed for studies to be pooled for meta-analysis, but this could have still resulted in heterogeneity. High statistical heterogeneity was found in a quarter of the analyses. Furthermore, because of the low number of trials included, publication bias could not be assessed by funnel plot analysis. The manufacturers funded most of the trials for ranibizumab, pegaptanib, dexamethasone and fluocinolone, whereas trials for bevacizumab and triamcinolone were generally funded by non-pharmaceutical organisations. Generally, the non-commercial studies had smaller numbers, perhaps because of the funding restraints.
It is important to note that there may be differences in laser treatment protocol between studies. This applies to trials which combine drug treatments with laser or include laser as a comparator. All studies referred to the ETDRS protocol19 ,20 or a modified version of it. In the ETDRS, once a diagnosis of clinically significant macular oedema was made, an angiogram was obtained to identified ‘treatable lesions’. ‘Treatable lesions’ included discrete points of retinal hyperfluorescence or leakage (most of these are often microaneurysms), areas of diffuse leakage within the retina related to microaneurysms, intraretinal microvascular abnormalities, diffusely leaking retinal capillary bed and retinal avascular zones. In the ETDRS protocol, treatment of lesions closer than 500 microns from the centre of the macula was not required initially; however, if vision was less than 20/40 and the oedema and leakage persisted, treatment up to 300 microns from the centre of the macula was recommended unless there was capillary dropout; in the latter case, treatment was not recommended as it may lead to further loss of perifoveal capillaries.
However, in routine clinical practice, clinicians generally use lighter and less intense treatment than specified in the ETDRS protocol.76 In addition, some centres do not use fluorescein angiography (unlike the ETDRS study19) to guide treatment. The exact adherence to the ETDRS protocol within studies is unclear. For example, in the BOLT study, a modified ETDRS protocol was used. One of the aims of the protocol was ‘not darkening/whitening of microaneurysms’, which is not consistent with the ETDRS protocol.
Interpretation of the results
The anti-VEGF drugs appear to be clinically effective in treating DMO in short-term studies (up to 2 years). Ranibizumab has the most robust evidence base and has shown superiority compared to laser and sham injection in all trials and meta-analyses, except for the proportion of patients with 10 or more letter gain in the DRCR.net study published by Elman et al46 at 2 years follow-up. Adding laser to ranibizumab conferred no benefit. Bevacizumab has also been shown to be superior to laser. Three doses have been used (1.25, 1.5 and 2.5). The higher dose does not appear to add further benefit, and most studies in the literature use 1.25 mg. The addition of triamcinolone to bevacizumab did not provide further benefits. Pegaptanib has only been compared to sham injection. Mean change in BCVA favoured pegaptanib, but only through meta-analysis did the proportion of patients with more than 15 letter gain favour pegaptanib. Further published data are required before drawing conclusions on aflibercept. However, although the anti-VEGF drugs are a significant advance, they fail to improve BCVA by 10 or more letters in half or more patients, and so they do not provide a complete answer to DMO.
Steroid treatments have inconsistent results and are undoubtedly associated with increased IOP and cataract. The effects of dexamethasone appear to peak at 3 months. At 6 months, there was no significant difference compared with laser. This might imply that earlier retreatment is needed if the beneficial effect is to be maintained, but increasing the number of treatments would very likely increase the associated complications, especially with the relatively large needle size. The addition of laser did not appear to add further benefit. There was no significant difference in cataract formation at 6 months with dexamethasone compared to observation, but it is likely that a higher incidence of cataracts would be seen with longer follow-up. Significantly more patients suffered increased IOP in the dexamethasone group compared with observation. Fluocinolone has been shown to be effective compared with sham injection (FAME);29 ,60 however, when compared to standard of care (laser or observation at clinician's discretion), there was no significant difference in the proportion of patients with a 15 letter or more gain. Both studies reported higher incidence of cataract formation in the fluocinolone group, with over 80% at 3 years at the higher dose. Results for triamcinolone are inconsistent. Ip et al61 found that laser was more effective, while others have found no statistically significant difference. Triamcinolone combined with laser, however, seemed to have similar efficacy as ranibizumab combined with laser in pseudophakic eyes.21 ,46 Triamcinolone is more effective than sham injection. Triamcinolone has consistently been associated with increased incidence of cataract and raised IOP.
Steroids and laser therapy may affect CMT in a different manner from anti-VEGF drugs. For example, when ranibizumab alone is compared with ranibizumab plus laser, it appears to be more effective in terms of mean change in BCVA and proportion of patients with more than 15 letter gain. However, ranibizumab plus laser is more effective at reducing CMT. Furthermore, when triamcinolone plus laser is compared with ranibizumab plus laser, the latter appears to be more effective in terms of change in BCVA and proportion of patients with more than 15 letter gain, but triamcinolone plus laser is more effective at reducing CMT. The reasons for this are unclear. There is a weak correlation between CMT and BCVA. However, the long-term benefits of reducing CMT are currently unknown.
No large observational studies were identified that compared anti-VEGF drugs. Using an internet-based survey, Fung et al70 found the incidence of adverse events in bevacizumab to be low. One small outbreak of sterile endophthalmitis was reported with a single batch of bevacizumab in Canada, emphasising the need for sterility when preparing aliquots.77 Curtis et al78 carried out a very large retrospective cohort study in 146 942 patients aged 65 and over with age-related macular degeneration (AMD). Their aim was to examine cardiovascular outcomes in patients treated with the four options: photodynamic therapy (PDT), pegaptanib, bevacizumab and ranibizumab. The authors reported that one of their comparisons showed an increase in overall mortality and stroke risk with bevacizumab compared to ranibizumab, with HRs of 0.86 (95% CI 0.75 to 0.98) and 0.78 (0.64 to 0.96), respectively. However, owing to the very large cost differences between bevacizumab and ranibizumab, the authors noted that selection bias might be operating, with poorer people (with poorer health) more likely to be treated with bevacizumab. They therefore carried out another analysis using only ophthalmological clinics which used only one drug, to avoid selection bias. This analysis showed no significant difference: overall mortality HR for ranibizumab 1.10 (95% CI 0.85 to 1.141); MI 0.87 (0.53 to 1.14); stroke 0.87 (0.61 to 1.24).
Gower et al79 analysed 77 886 anti-VEGF injections from Medicare data (46% ranibizumab and 54% bevacizumab). Results have only been published in abstract form. The authors found an increased risk of overall mortality and cerebrovascular events in the bevacizumab group (HR 1.11 99% CI 1.01 to 1.23 and 1.57, 1.04 to 2.37, respectively). There was no statistically significantly increased risk in the ranibizumab group. The authors acknowledge that a limitation of the study is a failure to adjust for important confounding factors (such as smoking, hypertension and hyperlipidaemia). Considering the cost difference, it is likely that patients treated with bevacizumab would have been in a lower socioeconomic class and therefore at high risk of mortality and vascular disease.
Implications for clinicians
The anti-VEGF drugs appear to be a significant advance in the treatment of DMO and are regarded now as the treatment of choice for patients affected by this condition. Studies assessing the effectiveness of steroids have reported mixed results. The high rates of cataract and increased IOP are a drawback. Triamcinolone combined with laser may be a good option for pseudophakic patients and may be more cost-effective than treatment with ranibizumab. However, the need for fewer administrations, potentially one every 3 years with fluocinolone, is advantageous. From an administration perspective, some patients might prefer infrequent steroid injections with a sizeable risk of cataract, and a small, but existent, risk of glaucoma, to frequent anti-VEGF injections, even if the potential gain may not be fully comparable. Steroids may also be considered for patients who do not adequately respond to anti-VEGFs. Currently, the role of laser in the treatment of DMO is debatable. Short-term data from available trials have demonstrated the superiority of anti-VEGF with regard to laser treatment but have failed to demonstrate a benefit of combining both treatment approaches. It is possible that some ophthalmologists may still opt to offer laser treatment to patients with very focal areas of leakage.
Currently, there is more evidence for the effectiveness of ranibizumab and bevacizumab than for pegaptanib and VEGF-trap eye. The results of direct head to head trials of ranibizumab and bevacizumab are awaited. Bevacizumab is not licensed for intraocular use but costs considerably less than other forms of therapy. Ranibizumab is licensed and more expensive, but its use is supported by large manufacturer-funded trials demonstrating its clinical effectiveness. In the UK, the General Medical Council recommends that unlicensed medications should only be prescribed if ‘an alternative, licensed medicine would not meet the patient's needs’ and there is ‘a sufficient evidence base and/or experience of using the medication to demonstrate its safety and efficacy’.80 The FDA says that when using a drug ‘off-label’, clinicians ‘have the responsibility to be well informed about the product, to base its use on firm scientific rationale and on sounded medical evidence, and to maintain records of the product’s use and effects’.81 Patients should be fully aware of the use of any unlicensed medication and consent to any safety or efficacy uncertainties.
The place of intravitreal steroids needs consideration now that we have the anti-VEGFs drugs, as does the role of laser. The anti-VEGFs drugs may now be the first-line treatment in place of laser, with laser being used selectively for focal lesions, and in sequence after anti-VEGF therapy once the retinal thickness has been reduced. However, it should be noted that about half of the patients do not get good results with anti-VEGFs. In RESTORE, only 50% of patients had gains in VA of 10 or more letters. So the anti-VEGFs are ‘game-changers’, but their impact should not be overestimated.
In those who do not respond to anti-VEGFs or laser, there remains a place for steroids, despite their high adverse effect rates. The European licence for fluocinolone recognises this, by stating that it should be used when other therapies have not had sufficient effect.82 The commonest adverse effect is cataract, but that is very common in people with diabetes, and many are already pseudophakic when treatment of DMO is required.
Vitreoretinal surgery for the treatment of DMO was not included in our review. Laidlaw reviewed the literature and only found evidence for vitrectomy when there were signs of clinical or OCT traction.83 However, even in these cases, the evidence was not strong.
Implications for policy makers
In the UK, the National Institute of Health and Clinical Excellence (NICE) has recently made the decision not to recommend ranibizumab for the treatment of DMO.84 NICE concluded that ranibizumab, although clinically effective, was not cost-effective compared to laser therapy. Bevacizumab is less than a tenth of the cost of ranibizumab but is unlikely to be licensed. This beckons the question as to whether policy makers should recommend cheaper unlicensed medications over a more expensive licensed alternative when their efficacy and side effects appear to be similar.
Unanswered questions
Several unanswered questions remain. Studies evaluating the effectiveness of ranibizumab compared with bevacizumab are needed. Although the anti-VEGFs are clinically effective and a major step forward in the management of DMO, it has to be noted that they have little effect in a large number of patients. Generally speaking, the proportion of patients who have demonstrated 10 or more letter gain using anti-VEGFs is between 30% to 50% in the trials that demonstrate the greatest effectiveness. Most of these patients would not achieve the 20/40 visual acuity required for driving. More effective treatments, or combinations of treatments, are required.
There is a lack of specific evidence for the use of anti-VEGF drugs or steroids in patients with macular ischaemia secondary to DMO. A number of trials excluded patients with macular ischaemia.23 ,34 ,35 ,40 ,53 ,62 The RESTORE trial included patients with macular ischaemia and undertook a subgroup analysis.24 The authors compared patients with (n=34) and without (n=35) macular ischaemia at baseline. They found that those without macular ischaemia responded better to ranibizumab (mean average change in BCVA at 12 months 7.2 letters gain compared with 6.3 letters). Larger trials are needed to assess the use of anti-VEGF drugs and steroids in patients with macular ischaemia.
The duration of treatment is as yet uncertain. Most of the included studies use a retreatment protocol based on clinical need or OCT results. For example, in the BOLT study, patients received a median of nine injections of bevacizumab over 24 months.23 ,85 However, it is not yet known for how frequent long-term maintenance injections will be needed and whether laser treatment in sequence could potentially reduce the number of anti-VEGF injections required. Other treatment strategies to apply laser, such as using laser power at subthreshold levels, may prove more effective.86 Future trials should use active comparators which are used in routine clinical practice and avoid placebo-controlled trials.
Conclusion
This review evaluated current treatments for DMO. Undoubtedly, the use of anti-VEGFs heralds a new era for patients who suffer from DMO. Currently, the anti-VEGFs ranibizumab and bevacizumab have consistently shown good clinical effectiveness without major unwanted side effects. Steroid results have been mixed and are usually associated with cataract formation and IOP increase. Based on the short-term data available, adding laser therapy to anti-VEGFs does not appear to confer additional benefit.
Despite the current wider spectrum of treatments for DMO, only a small proportion of patients recover good vision (≥20/40), and thus the search for new therapies to prevent and manage DMO needs to be continued.
Appendix 1: Methods of the literature search
Searches for clinical trials
Ovid MEDLINE 1948-week 2 July 2012 and Ovid MEDLINE(R) In-Process and Other Non-Indexed Citations 11 July 2012
-
Diabetic Retinopathy/dt (Drug Therapy)
-
Macular Edema/dt (Drug Therapy)
-
(diabet* adj2 macular adj (edema or oedema)).tw.
-
(diabet* adj2 maculopathy).tw.
-
(diabet* adj2 retinopathy).tw.
-
1 or 2 or 3 or 4 or 5
-
(ranibizumab or lucentis or bevacizumab or avastin or pegaptanib or macugen or aflibercept or vegf trap-eye or steroid* or corticosteroid* or dexamethasone or fluocinolone or triamcinolone or anti-VEGF* or anti-vascular endothelial growth factor*).tw.
-
exp Vascular Endothelial Growth Factor A/
-
exp Fluocinolone Acetonide/
-
exp Triamcinolone/
-
7 or 8 or 9 or 10
-
6 and 11
-
randomised controlled trial.pt.
-
controlled clinical trial.pt.
-
(masked or sham or placebo or control group or random*).tw.
-
13 or 14 or 15
-
12 and 16
-
(case reports or editorial or letter or review).pt.
-
17 not 18
-
limit 19 to humans
EMBASE 1947–2012 week 27
-
(ranibizumab or lucentis or bevacizumab or avastin or pegaptanib or macugen or aflibercept or vegf trap-eye or dexamethasone or fluocinolone or triamcinolone or anti-VEGF* or anti-vascular endothelial growth factor*).m_titl.
-
(diabetic macular edema or diabetic macular oedema or diabetic retinopathy or diabetic maculopathy).m_titl.
-
1 and 2
-
random*.tw.
-
3 and 4
Cochrane Central Register of Controlled Trials, Issue 7 of 12, July 2012
Ranibizumab or lucentis or bevacizumab or avastin or pegaptanib or macugen or aflibercept or vegf trap-eye or steroid* or corticosteroid* or dexamethasone or fluocinolone or triamcinolone or anti-VEGF* or anti-vascular endothelial growth factor* in Record Title and diabetic macular edema or diabetic macular oedema or diabetic retinopathy or diabetic maculopathy in Record Title
Web of Science—with Conference Proceedings (updated 12 July 2012)
Title=(ranibizumab or lucentis or bevacizumab or avastin or pegaptanib or macugen or aflibercept or vegf trap-eye or steroid* or corticosteroid* or dexamethasone or fluocinolone or triamcinolone or anti-VEGF* or anti-vascular endothelial growth factor*) AND Title=(diabetic macular edema or diabetic macular oedema or diabetic retinopathy or diabetic maculopathy) AND Title=(random*)
Searches for systematic reviews
Ovid MEDLINE(R) Daily Update 11 July 2012, Ovid MEDLINE(R) In-Process and Other Non-Indexed Citations 11 July 2012
-
Diabetic Retinopathy/dt (Drug Therapy)
-
Macular Edema/dt (Drug Therapy)
-
(diabet* adj2 macular adj (edema or oedema)).tw.
-
(diabet* adj2 maculopathy).tw.
-
(diabet* adj2 retinopathy).tw.
-
1 or 2 or 3 or 4 or 5
-
(ranibizumab or lucentis or bevacizumab or avastin or pegaptanib or macugen or aflibercept or vegf trap-eye or steroid* or corticosteroid* or dexamethasone or fluocinolone or triamcinolone or anti-VEGF* or anti-vascular endothelial growth factor*).tw.
-
exp Vascular Endothelial Growth Factor A/
-
exp Fluocinolone Acetonide/
-
exp Triamcinolone/
-
7 or 8 or 9 or 10
-
6 and 11
-
(systematic review or meta-analysis or pubmed or medline).tw.
-
meta-analysis.pt.
-
cochrane.af.
-
13 or 14 or 15
-
12 and 16
Cochrane Database of Systematic Reviews and Technology Assessments Database, Cochrane Library July Issue, 2012
Ranibizumab or lucentis or bevacizumab or avastin or pegaptanib or macugen or aflibercept or vegf trap-eye or steroid* or corticosteroid* or dexamethasone or fluocinolone or triamcinolone or anti-VEGF* or anti-vascular endothelial growth factor* in Record Title and diabetic macular edema or diabetic macular oedema or diabetic retinopathy or diabetic maculopathy in Record Title
Searches for safety and adverse events
Ovid MEDLINE(R) Daily Update 11 July 2012, Ovid MEDLINE(R) In-Process and Other Non-Indexed Citations 11 July 2012 ; EMBASE 1980–2012 week 27
-
(ranibizumab or lucentis or bevacizumab or avastin or pegaptanib or aflibercept or vegf trap-eye or macugen or dexamethasone or fluocinolone or triamcinolone or anti-VEGF* or anti-vascular endothelial growth factor*).m_titl.
-
(diabetic macular edema or diabetic macular oedema or diabetic retinopathy or diabetic maculopathy).m_titl.
-
1 and 2
-
(risk or safety or adverse or harm or pharmacovigilance).tw.
-
(side-effect* or precaution* or warning* or contraindication$ or contra-indication* or tolerability or toxic*).tw.
-
4 or 5
-
3 and 6
Searches of the annual meeting abstracts (for trials, reviews and safety studies)
-
ARVO (Association for Research in Vision and Ophthalmology) (2002–2012)
-
ADA (American Diabetes Association) (2002–2012)
-
EASD (European Association for the Study of Diabetes) (2002–2012)
Other searches
Web sites of the following
-
Drugs@FDA: FDA Approved Drug Products
-
European Medicines Association
-
ClinicalTrials.gov
-
EU Clinical Trials Register
National Institute for Health and Clinical Excellence
Appendix 2: Ongoing Trials in ClinicalTrials.gov
-
Schmidt-Erfurth and colleagues are comparing ranibizumab and bevacizumab in DME (NCT00545870)
-
TRIASTIN study is comparing ranibizumab, triamcinolone and sham injection (NCT00682539)
-
Maturi and colleagues are comparing bevacizumab plus dexamethasone with bevacizumab alone (NCT01309451)
-
IBeTA study (Jorge and colleagues) is comparing bevacizumab (1.5 mg) plus laser, triamcinolone (4 mg) plus laser with laser alone (NCT00997191)
-
Chaudhry and colleagues are evaluating ranibizumab in patients who have failed with 3–6 injections of bevacizumab (NCT01253694)
-
MIDME study (Pfizer) is comparing pegaptanib 0.3 mg with sham injection (NCT01175070)
-
Figueira and colleagues are comparing pegaptanib plus laser with laser alone (NCT01281098)
-
RESPOND (Novartis) is comparing ranibizumab (0.5 mg) alone with ranibizumab plus laser or laser alone (NCT01135914)
-
RETAIN (Novartis) study is comparing two different ranibizumab algorithms; ‘treat and extend’ versus as needed (NCT01171976)
-
RED-ES (Novartis) is comparing ranibizumab with laser in patients with visual impairment due to DME (NCT00901186)
-
READ 3 study (Do and colleagues) are comparing two doses of ranibizumab 0.5 and 2 mg (NCT01077401)
-
VIVID-DME and VISTA DME studies (Bayer) are comparing aflibercept with laser. (NCT01331681 and NCT01363440)
-
Gillies and colleagues are comparing bevacizumab with dexamethasone (NCT01298076)
-
Soheilian and colleagues are performing a phase I study looking at the use of diclofenac compared with bevacizumab in DME (NCT00999791)
-
López-Miranda and colleagues are comparing the use of bevacizumab before and after laser therapy (NCT00804206)
-
NEVANAC study is comparing triamcinolone alone with triamcinolone plus nepafenac (NSAID) (NCT00780780)
-
Elman and colleagues are comparing laser alone, laser combined with an intravitreal injection of triamcinolone, laser combined with an intravitreal injection of ranibizumab, or intravitreal injection of ranibizumab alone (NCT00444600)
-
BRDME (Schlingemann and collagues) study is comparing the use of bevacizumab and ranibizumab in the treatment of patients with DME (OCT central area thickness > 275 μm) (NCT01635790)
-
Wiley and colleagues are comparing bevacizumab and ranibizumab in patients with DME in at least one eye (NCT01610557)
-
Protocol T study (Wells and colleagues) is comparing effectiveness of a aflibercept, bevacizumab and ranibizumab for DME (NCT01627249)
-
Allergan-funded study comparing safety and efficacy of 700 µg dexamethasone implant against 0.5 mg ranibizumab in patients with DME (NCT01492400)
-
Pfizer-funded study comparing effectiveness of 0.3 mg pegaptanib against sham injection (NCT01100307)
-
Allergan-funded study comparing safety and efficacy of an intravitreal dexamethasone implant (700 and 350 µg) against sham in patients with DME (NCT00168389)
-
Allergan-funded study comparing safety and efficacy of an intravitreal dexamethasone implant (700 and 350 µg) against sham in patients with DME (NCT00168337)
References
Footnotes
-
Contributors JAF screened titles, checked data extraction, performed the meta-analysis and drafted the manuscript. NL conceived the idea, interpreted the results and provided clinical expertise throughout. PR performed the literature search, updated the searches, screened the titles and managed the references. CC extracted data from the studies. DS screened the titles and checked the meta-analysis. NW designed the review and supervised the running of the study. All authors contributed to the final draft.
-
Competing interests None.
-
Provenance and peer review Not commissioned; externally peer reviewed.
-
Disclosure The authors report no proprietary or commercial interest in any product mentioned or concept discussed in this article.
-
Data sharing statement No additional data are available.
-
Protocol This review was built upon several technology appraisals for NICE, and therefore no protocol exists.