Article Text

Abstract
Introduction Pharmacotherapy and cognitive behavioural therapy (CBT) are consistently effective as first-line treatments for social anxiety disorders (SADs). Nevertheless, pharmacotherapy is often the first choice in clinical practice. In many countries, the first line of pharmacotherapy involves the administration of a selective serotonin reuptake inhibitor (SSRI). Although a significant proportion of patients with SAD fail to respond to the initial SSRI administration, there is no standard approach to the management of SSRI-resistant SAD. This paper describes the study protocol for a randomised controlled trial to evaluate the clinical effectiveness of CBT as a next-step strategy, concomitant with conventional treatment, for patients with SSRI-resistant SAD.
Methods and analysis This Prospective Randomized Open Blinded End-point study is designed with two parallel groups, with dynamic allocation at the individual level. The interventions for the two groups are conventional treatment, alone, and CBT combined with conventional treatment, for 16 weeks. The primary end-point of SAD severity will be assessed by an independent assessor using the Liebowitz Social Anxiety Scale, and secondary end-points include severity of other social anxieties, depressive severity and functional impairment. All measures will be assessed at weeks 0 (baseline), 8 (halfway point) and 16 (postintervention) and the outcomes will be analysed based on the intent-to-treat. Statistical analyses are planned for the study design stage so that field materials can be appropriately designed.
Ethics and dissemination This study will be conducted at the academic outpatient clinic of Chiba University Hospital. Ethics approval was granted by the Institutional Review Board of Chiba University Hospital. All participants will be required to provide written informed consent. The trial will be implemented and reported in accordance with the recommendations of CONSORT.
Clinical Trial Registration Number UMIN000007552.
- Mental Health
This is an open-access article distributed under the terms of the Creative Commons Attribution Non-commercial License, which permits use, distribution, and reproduction in any medium, provided the original work is properly cited, the use is non commercial and is otherwise in compliance with the license. See: http://creativecommons.org/licenses/by-nc/3.0/ and http://creativecommons.org/licenses/by-nc/3.0/legalcode
Statistics from Altmetric.com
Article summary
Article focus
-
Selective serotonin reuptake inhibitors (SSRIs) are the first choice for the treatment of social anxiety disorders (SADs) in clinical practice; however, there is no standard approach for cases that fail to respond to the initial treatment with SSRIs.
-
Cognitive behavioural therapy (CBT) intervention will be examined to determine its effectiveness for treatment of SAD patients not responding to SSRI treatment.
Key messages
-
A randomised controlled trial protocol is outlined for the evaluation of the clinical effectiveness of CBT as a next-step strategy, when administered concomitantly with conventional treatment to SSRI-resistant SAD patients, in a clinical setting.
-
No restrictions will be placed on the treatment options selected by the patient's general practitioner.
-
Patients with comorbid diagnoses, similar to those seen in clinical practice, will be recruited.
Strengths and limitations of this study
-
This is the first randomised controlled trial to focus on CBT as a therapeutic option for SSRI-resistant SAD patients.
-
This study reflects good clinical practice, and its results will contribute to the development of second-line treatments and establish future treatment algorithms.
-
The main limitation of this study is that the specific effects of the CBT programme based on Clark and Wells (including the videotape feedback and behavioural experiment sessions) cannot be revealed because a psychosocial comparison group will not be employed in this study.
Introduction
Social anxiety disorder (SAD; also known as social phobia) is characterised by extreme fear of embarrassment in social situations involving performances or interactions.1 It is one of the most prevalent psychiatric disorders in developed and developing countries,2 typically beginning in childhood or adolescence. If left untreated, SAD is associated with the subsequent development of major depression, substance abuse and other mental health problems. Thus, SAD can be associated with functional disability (including social and occupational impairment), low health-related quality of life and economic burden.3–5
As of 2012, though empirically derived treatment algorithms for SAD do not exist, pharmacotherapy and cognitive behavioural therapy (CBT) have consistently been shown to be effective as first-line treatments in a large database of randomised controlled trials, and are recommended in many countries.6 ,7 The following summary is based on the primary literature, meta-analyses, systematic reviews, ongoing clinical experience, published guidelines and the current status of treatment in clinical practice.8–11
First-line CBT
CBT has consistently been shown to be effective as first-line treatments in randomised controlled trials.6 There are basically three types of CBT: individual CBT, group CBT and internet CBT. Recent studies have demonstrated the superiority of individual format CBT over group format,12 ,13 and internet CBT has shown comparable effectiveness to group CBT.14 While no clear evidence has shown that the combination of selective serotonin reuptake inhibitor (SSRIs) and CBT is more effective than single-modality treatment,15 ,16 CBT has a number of potential advantages over pharmacotherapy in the treatment of anxiety disorder (including individual -based, group -based and internet-based): longer effects, fewer adverse effects, smaller relapse rates and greater acceptability.17–20 Pharmacotherapy has disadvantages such as more side effects and higher rates of relapse with the discontinuation of medication,21 ,22 and patients often prefer psychological treatment (even if this is more well known in the depression literature).23
Nevertheless, CBT is used much less frequently in clinical practice because of the limited availability of specialised practitioners and it has received much less promotion from pharmaceutical companies than pharmacotherapy.24 Thus, pharmacotherapy is actually used as a first choice treatment for SAD by most clinicians, even in countries with initiatives to improve access to psychological therapies (eg, the UK, Australia).25–27
First-line pharmacotherapy
With regard to pharmacotherapy, treatment varies according to the subtypes (generalised and non-generalised). However, we focus primarily on treatment options for generalised SAD because currently there is very limited clinical trial-based evidence for the treatment of non-generalised SAD.28 ,29 Pharmacotherapy, as a first-line treatment for SAD, currently involves the use of SSRIs. A growing database of randomised controlled trials had demonstrated that SSRIs are effective and well tolerated.7 ,30 ,31 Further, there is strong evidence that SSRIs are also effective for treating many of the comorbid conditions, such as depression and other anxiety disorders, frequently associated with SAD.
Serotonin-noradrenaline reuptake inhibitors are also recommended for first-line pharmacotherapy. However, there are comparatively few studies on this class of drugs, in comparison with SSRIs, and only venlafaxine has been demonstrated to be effective22 ,32 ,33; therefore, fewer countries have approved serotonin-noradrenaline reuptake inhibitors for treating SAD than SSRIs (eg, they have not been approved in Japan).
SSRIs have a relatively flat dose–response curve.34 Nevertheless, evidence suggests that a superior response may be obtained with higher doses of SSRIs.35 Clinical experience also suggests that some patients may require higher than normal starting doses to achieve an optimal response, and may even require maximal doses. SSRI administration should last for at least 12 weeks before its efficacy is assessed.36 Of course, SSRI treatment usually includes some type of non-specific psychotherapy (eg, supportive counselling) from the general practitioner.
Second-line treatment options for SSRI-resistant SAD cases
A significant proportion of SAD patients fail to respond to initial treatment with SSRIs.37 The presence of residual symptoms is known to be associated with higher relapse rates, decreased quality of life and greater functional impairment38; however, there is no standard approach to their management. On the whole, conventional second-line treatment is based on the clinician’s own judgement. Clearly, it is of increasing importance to consider therapeutic alternatives for patients with SAD who demonstrate resistance to SSRIs. A systematic review has advocated reviewing treatment options with limited evidence, including augmentation with another pharmacological agent or switching to another antidepressant, if patients show little or no response to the initial SSRI treatment after 12 weeks.36
Limited evidence supports the value of augmenting SSRI treatment with buspirone,39 clonazepam40 and atypical antipsychotic medications, such as risperidone and aripiprazole.41 ,42 A few studies have shown positive results when treatment was switched to a second SSRI or to a serotonin-noradrenaline reuptake inhibitor in SAD patients who failed to respond to initial SSRI treatment.43–45
CBT as a second-line treatment for SSRI-resistant SAD cases
While there is some evidence of the effectiveness of combined pharmacotherapy and CBT, the evidence for an additive effect when combining the two modalities is mixed; further, there is no evidence concerning the effectiveness of combined therapy specific to SSRI-resistant cases.15 ,16 ,46 Previously published systematic reviews, including case reports with ≥11 cases are not available regarding the use of CBT as a next step for SSRI non-remitters among SAD patients.47 In our preliminary study, most patients with SAD exhibited substantial resistance to SSRIs; however, 73% of the participants in the study were judged to be treatment responders, with 40% meeting the criteria for remission. The within-group effect size, between pre-CBT and post-CBT, on the Liebowitz Social Anxiety Scale (LSAS) total score was also large (Cohen's d=1.71). Thus, this preliminary study suggested that CBT might have potential as a next-step strategy, even for cases of SSRI-resistant SAD.
Aims
In summary, this paper describes the study protocol for a randomised controlled trial to evaluate the clinical effectiveness of CBT administered concomitantly with conventional treatment for patients with SSRI-resistant SAD.
Methods and analysis
Study design
A randomised controlled trial design employing psychological placebo conditions with single-blinded for patients to control non-specific factors (eg, time of contact between the patient and therapist, patient's expectations of a particular therapy, reasonable rationale for intervention and discussions of the psychological problem) is the most desirable trial design for verifying the effectiveness of psychological interventions.48 However, a psychological placebo differs from a pill placebo in that patient blinding is extremely difficult and is neither feasible nor practical in the former case; thus, placebo control conditions cannot control the patient's expectations from CBT. A psychological control condition, which is not single-blinded for patients, may be employed to control the time of contact (eg, relaxation training or supportive psychotherapy to be presented to share the same duration as the CBT); however, such methods are vastly different from conventional treatments.
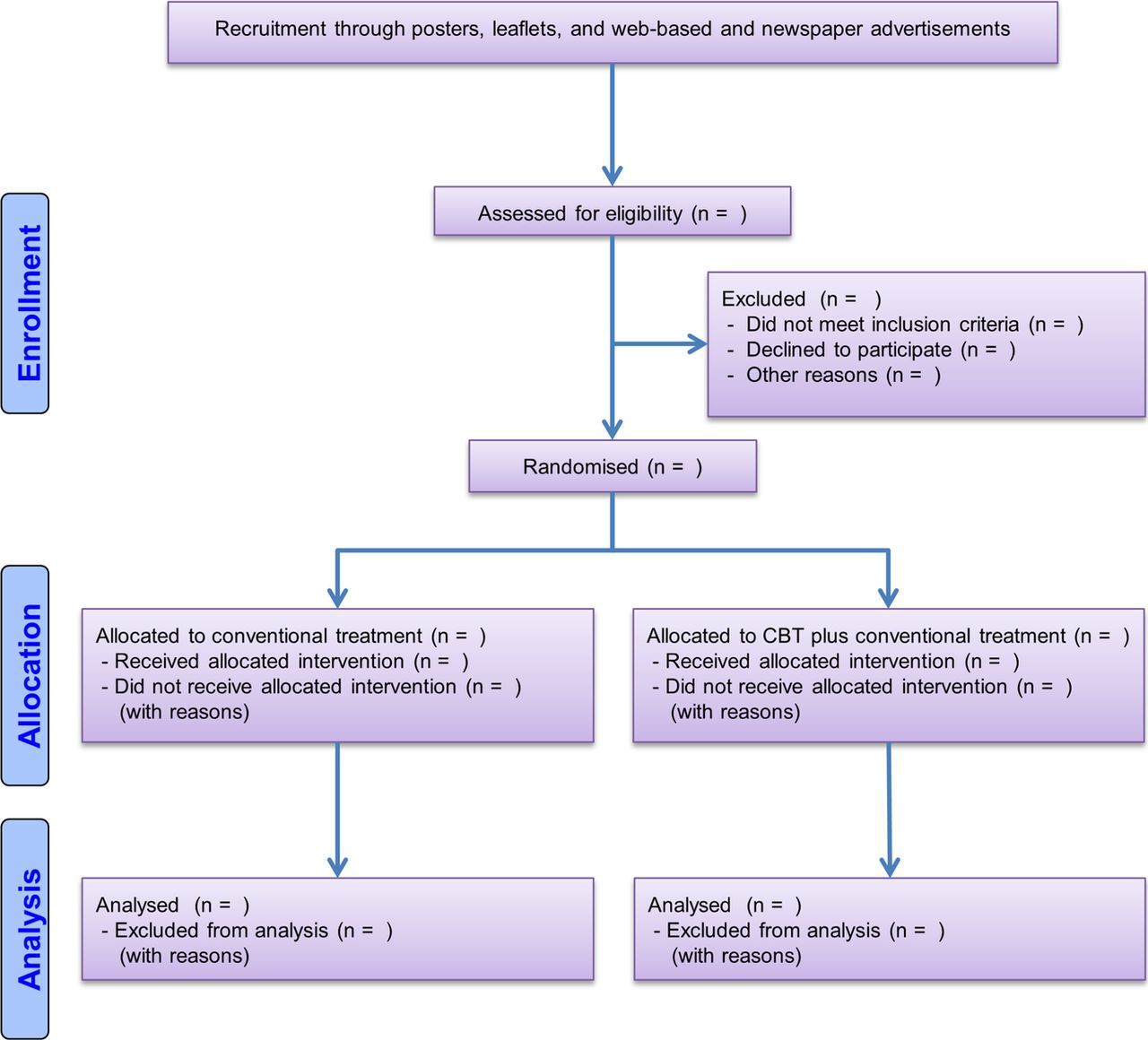
For the reasons listed above, this study was designed as a Prospective Randomized Open Blinded End-point trial with two parallel groups and with dynamic allocation at the individual level. Further, the intervention groups consist of a 16-week treatment regime of conventional treatment, alone, and a CBT programme combined with conventional treatment (see figure 1).
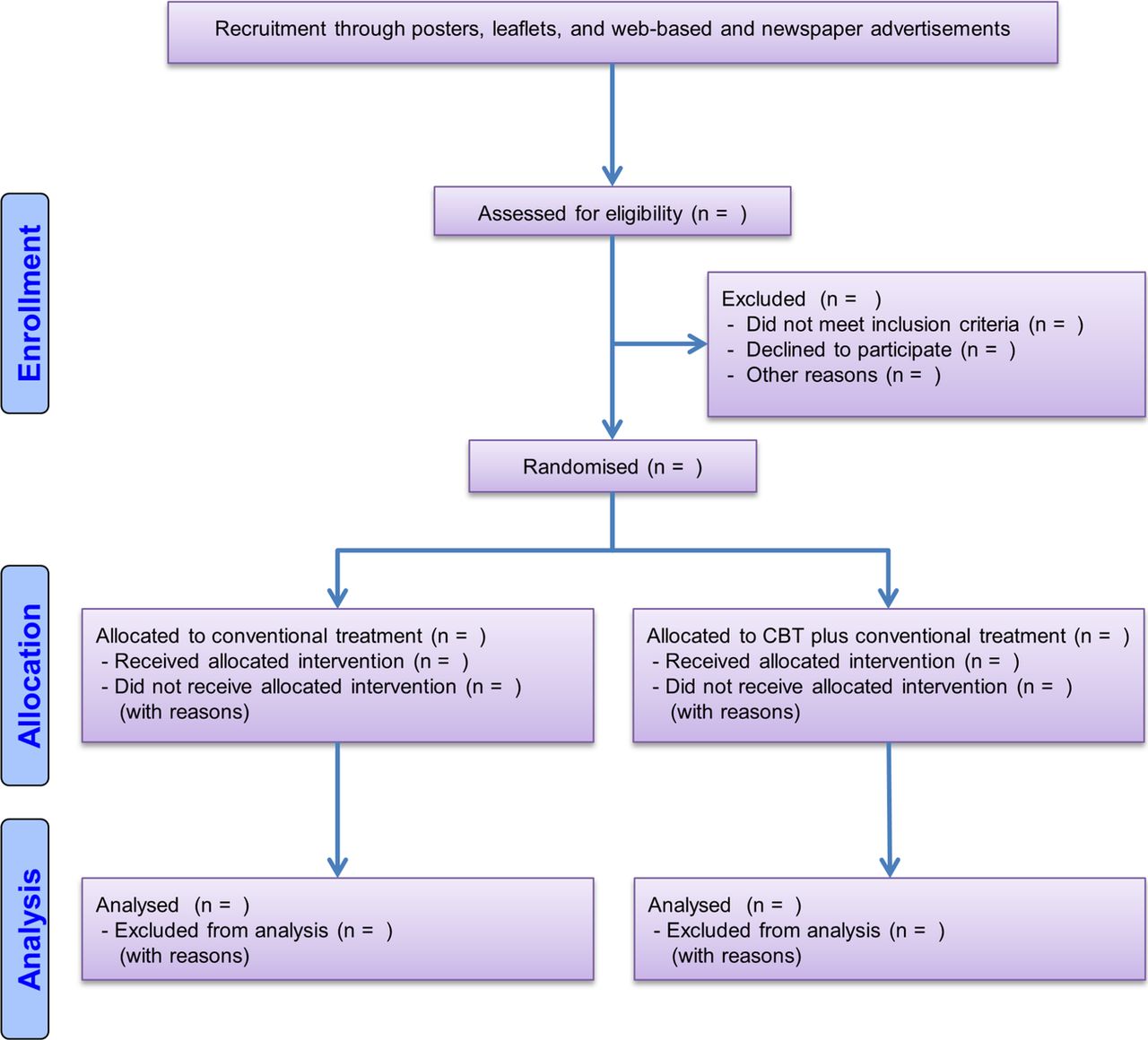
Patient flow during inclusion, randomisation and treatment.
Participants
Inclusion criteria
The inclusion criteria for this study include a primary diagnosis of SAD, according to the Diagnostic & Statistical Manual for Mental Disorders, Fourth Edition, Text Revision (DSM-IV-TR)1; patients between 18 and 65 years, SAD of at least moderate severity, based on an LSAS score ≥50,49 and defined as resistant to SSRIs, with at least one SSRI found to be inadequate for treatment despite administration at the maximum dose for at least 12 weeks, or intolerance to SSRIs (eg, because of drowsiness, nausea, sleep disturbances, sexual dysfunction and appetite change). In order that the study population reflects routine clinical practice,50–52 comorbid diagnoses will be permitted if they are clearly secondary (ie, SAD symptoms are both the most severe and the most impairing).
Exclusion criteria
The exclusion criteria for this study include psychosis, pervasive developmental disorders/mental retardation, autism spectrum disorders, current high risk of suicide, substance abuse or dependence within the 6 months prior to enrolment, antisocial personality disorder, unstable medical condition, pregnancy or lactation. In addition, much to very much improvement resulting from some type of treatment within 12 weeks prior to the study, as ascertained by a Clinical Global Impression Improvement scale score of ≤2,53 as reported by the patient and confirmed by the prescribing clinician, when possible, will also be sufficient to exclude the patient from the trial.
Eligibility procedure for participation and diagnosis
All patients will be evaluated by a psychiatrist and a study investigator using the Structured Clinical Interview for Axis I Disorders (SCID-I)54 and SCID-II.55 Treatment history will be confirmed by the prescribing clinician and by chart review.
Eligibility for participation in this clinical trial will be determined with the aid of a three-step procedure. First, the diagnosis and eligibility for participation will be checked by both a psychiatrist and a study investigator. Second, the validity of the initial diagnosis and eligibility will be discussed at a general meeting, to include psychiatrists, nurses, clinical psychologists and psychiatric social workers. Third, patients will be re-evaluated to cover important missing information, based on the suggestions derived from the second step, and the final diagnosis and eligibility will be confirmed by both a psychiatrist and a study investigator.
Recruitment
The planned recruitment rate is two participants per month, between June 2012 and March 2014, or until a total of 42 participants have been recruited. Participants will be recruited through posters and leaflets placed at medical institutions in Chiba Prefecture and through web-based and newspaper advertisements. As all participants will continue to be treated by their general practitioners, the patients will be required to obtain permission from their general practitioner prior to study enrolment.
Interventions
Conventional treatment
There are no restrictions on treatment options for patients who receive treatments, naturally including medication change, from their general practitioners. General practitioners will be permitted to refer patients for counselling or to secondary care if this is deemed clinically appropriate. However, the initiation of a strictly structured CBT programme is banned in order to properly assess the effectiveness of the CBT intervention. All changes in conventional treatment, with the reasons for these changes, will be recorded throughout the study period.
CBT programme
Individual-administered CBT will be employed in this study. CBT intervention will be conducted over 16 weekly, individual sessions. Most sessions will last for a period of 50 min, but the protocol allows therapists to extend up to six sessions to a maximum of 90 min to facilitate behavioural experiments. The CBT programme is based on that of Clark and Wells56 because this CBT model has demonstrated excellent treatment outcomes.12 ,13 ,57–59 The main parts of this protocol include: (1) developing an individualised version of the cognitive-behavioural model of SAD, (2) conducting role play-based behavioural experiments, with and without safety behaviours, (3) restructuring distorted self-imagery using videotape feedback, (4) practicing external focus and shifting attention, (5) performing a behavioural experiment to test the patient's negative beliefs, (6) modifying problematic pre-event and post-event processing, (7) surveying the differences between the beliefs of self and those of others, (8) dealing with the remaining assumptions (schema work), (9) rescripting early memories linked to negative images in social situations and (10) preventing relapse. Participants will be assigned homework after every session. Moreover, therapists will be allowed to customise the CBT programme, over the remaining sessions, in order to suit individual requirements, based on the symptoms and intelligibility (ie, another behavioural experiment, a review session to improve understanding and discussion of rigid dysfunctional schema). Further, therapists will be allowed to further customise the sessions at any stage of the CBT programme (figure 2 presents an overview).

{kind=link}
{kind=link}
Overview of the cognitive behavioural therapy (CBT) programme over 16 weekly sessions. Additional customisation of sessions are allowed at any stage of the CBT programme.
Therapists and therapy quality control
CBT will be delivered by therapists (psychiatrists, nurses, clinical psychologists and psychiatric social workers) experienced in the use of the CBT programme for patients with SAD, and by those who have already received the CBT training programme at Chiba University (Chiba Improving Access for Psychological Therapies project). To assist with planning future sessions, all therapists will attend weekly group-supervision sessions with other therapists and individual-supervision sessions with a senior supervisor throughout the study period. Senior supervisors will also assess the general quality of each CBT programme on the basis of the revised Cognitive Therapy Scale-Revised,60 by reviewing randomly selected, videotaped sessions. Study investigators will check the therapists’ protocol adherence and the homework adherence by patients using the original checklist.
Outcomes
Baseline and clinical characteristics
Baseline characteristics will include sex, age, education, marital status, employment status, age at SAD onset, duration of SAD and axis I comorbidities. Moreover, the treatment history will include the names of the SSRIs to which the participant has exhibited resistance, other prior treatments, current treatment (medication and others) at baseline and all changes in conventional treatment throughout the study period.
Primary outcome
The primary outcome will be clinician-determined symptoms of social anxiety, as measured on the LSAS,49 which is the most commonly used scale for assessing the SAD severity.61
Secondary outcomes
The secondary self-reported outcomes will be determined using the Social Phobia and Anxiety Inventory,62 Beck Depression Inventory-II,63 Sheehan Disability Scale,64 WHO Quality of Life-Brief version65 and the EuroQol-5 Dimensions.66 Moreover, the Clinical Global Impression Scale-Severity of Illness and Improvement67 will be rated by an independent assessor.
Blinding and quality control for the independent assessor
Treatment outcomes will be assessed by two independent assessors and the end-point committee who have no other contact with the study participants, to prevent identification of the treatment assignments. Further, participants will be instructed to not tell the assessor about their treatment assignment prior to the assessment. Independent assessors will receive training and supervision by the study investigator as well as a manual outlining the procedures for each clinician-administrated measure. The independent assessors will meet to review these procedures by the study investigator.
Sample size
Forty-two patients will be randomised into the study. This sample size was based on results from our previous pilot study that indicated that the estimated group difference in LSAS scores was approximately 30. The conventional treatment alone is assumed to be largely ineffective. Assuming a group difference of 30 points (SD=30), 18 subjects per arm will provide >80% power to detect a difference in LSAS scores between the conventional treatment arm and the arm with CBT combined with conventional treatment for at least 16 weeks, using a two-sided, two-sample t test at a 5% level of significance. Thus, allowing for a 20% dropout rate, 21 participants are required per group, for a total of 42 patients in the study.
Randomisation
At the end of the baseline assessment, the eligible patients will be randomly assigned to either the conventional treatment arm or CBT combined with the conventional treatment arm at a ratio of 1:1, with the assignments made at the data centre (the Clinical Research Centre, Chiba University Hospital) by means of the minimisation method,68 ensuring a balance in baseline LSAS scores (LSAS ≥70, or less), gender and current treatment with SSRIs (yes or no).
The study investigator will review the randomisation online, and the participant will then be provided with an appointment to undergo one of the two treatment regimes. The patient will be blinded to the group to which they are assigned before they consent to participate in the study.
Statistical analysis
Statistical analysis and reporting of this trial will be conducted in accordance with CONSORT guidelines, with the primary analyses based on the intent-to-treat principle without imputing missing observations. As a sensitivity analysis, the multiple imputation method will be applied to examine the effect of missing data. For the baseline variables, summary statistics are constructed employing frequencies and proportions for categorical data, and mean and SD for continuous variables. The baseline variables are compared using Fisher's exact test for categorical outcomes and unpaired t test for continuous variables, as appropriate.
For the primary analysis to compare treatment effect, the least squares means (LSMean) and their 95% CI, which are estimated by using analysis of covariance (ANCOVA) with LSAS total scores (untransformed) on week 16, were compared between treatments (the conventional treatment alone vs CBT combined with conventional treatment) using an ANCOVA model, taking into account the variation due to treatment effects, and using the baseline LSAS score (LSAS ≥70, or less), gender and current treatment with SSRIs as the covariate. The LSMean is calculated for each treatment. To compare the treatment groups, the difference in LSMeans and the associated 95% CI are expressed as a proportion of the reference treatment LSMean. As a sensitivity analysis, the outcomes at weeks 0, 8 and 16 are modelled as a function of time, treatment and treatment-by-time interaction using linear mixed-effects models. Secondary outcomes are scores on the Social Phobia and Anxiety Inventory, Beck Depression Inventory-II, Sheehan Disability Scale, WHO Quality of Life-Brief version, EuroQol-5 Dimensions, the Clinical Global Impression Scale-Severity of Illness and Improvement and rates of the responder (defined as a reduction of 31% or a greater reduction in the LSAS score over the course of treatment duration) and of remission (defined as a score of 36 or less on the final LSAS score and no longer diagnosed with SAD by the DSM-IV-TR).69 The secondary analysis is performed in the same manner as the primary analysis.
All p values calculated in the subgroup analysis are two-sided and are not adjusted for multiple testing. p Values of less than 0.05 are considered to indicate statistical significance.
Ethics and dissemination
This study will be conducted at the Academic Outpatient Clinic of Chiba University. The study protocol has been approved by the Institutional Review Board of the Chiba University Hospital (Reference number: G23075). The trial is registered as UMIN000007552.
When the potential participant contacts the study trial office, he or she will be informed of the objectives of the study and asked if they are willing to participate. Each patient will be informed that participation is voluntary and that full anonymity will be provided to each participant. Each person will then be required to provide written informed consent for their participation in this study. Each patient will also be informed that all of the participants will receive conventional treatment from their general practitioner; half of the recruited individuals will also receive CBT, in addition to their conventional treatment. A doctor’s examination at each assessment point (at weeks 0, 8 and 16) and blood withdrawn before and after the intervention will be performed for the evaluation of adverse events. An adverse event can be any unfavourable and unintended sign, symptom or disease temporally associated with this interventional study, whether or not considered related to this CBT, and all adverse events will be reported. Serious adverse events would be immediately reported to this committee as well as registered through the hospital risk management system. Furthermore, an independent data monitoring committee will accurate assess the progress of the clinical trial, the safety data and critical efficacy variables and provide recommendations to the sponsor regarding the continuation, modification or termination of the trial.
The results of the trial will be published in appropriate journals, regardless of the outcomes. The trial will be implemented and reported in accordance with the recommendations of CONSORT.
Discussion
This study is designed to address the lack of research on the use of CBT in combination with the conventional treatment of SSRI-resistant SAD, and is expected to have sufficient power to detect a meaningful difference in outcomes. Moreover, the findings of this study will provide valuable evidence to help develop second-line treatments and establish treatment algorithms. The limitation of this study is that the specific effects of the CBT programme, based on Clark and Wells (including the videotape feedback and behavioural experiment sessions), cannot be revealed because a psychosocial comparison group will not be employed in this study.
Acknowledgments
The authors express their gratitude to Mari Tanaka, Tomomi Kobayashi, Hanae Ibuki and Dr Kenichi Asano for creating the CBT manual. Further, we would like to thank Editage for providing editorial assistance.
References
Footnotes
Contributors NY initiated the project, designed the study and wrote the original protocol and draft manuscript. TN, FO, SM, OK, MN, AN and MI contributed to the conceptualisation and design of the study, and all revised this manuscript critically for important intellectual content. HH and YS participated in the design of the study conception, data managing and contributed to the analysis aspect of the protocol. ES supervised the overall conduct of the study. All authors read, critically revised and approved the final manuscript.
Funding The primary sources for funding for this project are grants from Grant-in-Aid for Scientific Research from the Japanese Ministry of Health, Labour and Welfare (MHLW) (22SE1P0051). The MHLW plays no role in the collection, management, analysis and interpretation of data, and will not have any impact on the trial and the publication of the results.
Competing interests None.
Patient consent Obtained.
Ethics approval Institutional Review Board (IRB) of Chiba University Hospital (Reference number: G23075).
Provenance and peer review Not commissioned; externally peer reviewed.