Article Text

Abstract
Context Reports evaluating a possible association between necrotising enterocolitis (NEC) and blood transfusion have been predominantly case–control studies. As the possible associations of disease with any variable on which cases and controls have been matched cannot be explored, a cohort study would offer a solution to this problem.
Objective Our objective was to evaluate the association between exposure to a packed red blood cell (PRBC) transfusion and development of NEC in a cohort where biases of matching are omitted.
Design In a retrospective cohort, exposed infants were defined as those who received a transfusion and did not develop NEC or developed NEC within 48 h of the transfusion. All others were considered unexposed.
Setting A single regional perinatal centre in Memphis, Tennessee, USA.
Patients 3060 ≤1500 g birth weights (BW) were included.
Outcome measures The relative risk of developing NEC after exposure to a PRBC transfusion was measured.
Results 3060 infants were identified. 174 infants (5.7%) developed NEC; 116 of the 174 infants (67%) were exposed. NEC infants had a significantly lower BW (924 vs 1042 g) and required a longer stay on a ventilator (7 vs 2 days). Divided into groups, infants with BW ≤750 , 751–1000 , 1001–1250 g and 1251–1500 g (n=52, 51, 46 and 25, respectively) had a relative risk of 0.14, 0.46, 1.83 and 1.78 (p<0.01, 0.02, 0.07 and 0.17), respectively, to develop NEC after an exposure. Infants with longest ventilator days were also significantly less likely to develop NEC after an exposure; relative risk=0.11 (p<0.01).
Conclusions Exposure to transfusions was less likely associated with NEC in ≤1000 g infants and remained a risk factor in 1001–1500 infants. BW has to be factored in any study evaluating the association between PRBC transfusions and NEC.
- NEONATOLOGY
- PAEDIATRIC SURGERY
This is an Open Access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 3.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/3.0/
Statistics from Altmetric.com
Strengths and limitations of this study
-
A large single centre cohort over a 16-year period and the new findings of different associations between transfusions and necrotising enterocolitis based on birth weight groups were among the main strengths.
-
Retrospective nature and unavailability of haematocrit data were among the main limitations.
Introduction
Recent evidence supports an increased risk for the development of necrotising enterocolitis (NEC) after a transfusion with packed red blood cells (PRBC).1–3 Transfusion-related acute gut injury has been proposed4 as one of the many terms used to describe this process. Difficulties in evaluating any association between NEC and blood transfusions stem from two main facts. The first pertains to the low incidence of NEC; the second relates to NEC's unclear multifactorial pathogenesis.5 These are probably the reasons that all the previous reports studying this association could only be carried out as retrospective case–control studies, as it is more practical to find the NEC cases and their respective controls.1–4 6–8
One of the major disadvantages of case–control studies concerns matching. The possible association of disease with any variable on which cases and controls have been matched cannot be explored. For example, birth weight (BW) and gestational age have been common denominators to identify the controls in case–control studies. Large-cohort studies do not have this problem. We thus hypothesised that including the variables such as BW and gestational age in the analysis would lead to new information that may improve our understating of the relationship between blood transfusions and NEC. Hence, our objective was to use an established database to study the association between exposure to a PRBC transfusion and development of NEC in all very low-BW infants (VLBW) over an extended period of time without the need for matching.
Methods
This was a retrospective cohort study. Data were obtained for all infants discharged between 1 January 1996 and 31 December 2011, from the Neonatal Intensive Care Unit (NICU) at The Regional Medical Center, Memphis, Tennessee, USA. The study protocol was approved by the Institutional Review Board at the University of Tennessee Health Science Center.
Patients
All infants with BW of ≤1500 g were included for further evaluation. To decrease the effects from perinatal factors, infants who died or were transferred out within the first 7 days of life were excluded. Infants who died after 7 days of life were included.
Transfusion practices
There were no written guidelines on transfusion thresholds during the study period. Transfusion was a clinical decision by the care team. The default PRBC unit used was O negative, irradiated, leucocyte depleted and cytomegalovirus negative. The preservative used was citrate-phosphate-dextrose-adenine-1. Patients were not assigned to receive blood from a dedicated unit. We used one or two ‘active’ units that served as the source of all transfusions for every recipient in the NICU, until this unit is depleted. A unit was typically received within 3–4 days from the collection, and was exhausted in a week. During a transfusion, feedings were maintained and advanced similarly to those infants not receiving a transfusion. Erythropoietin was not used.
NEC
Only infants meeting the Bell's stage II criteria9 or above for the diagnosis of NEC were included. To reduce a potential bias from infants receiving transfusions at a time point when the NEC incidence was rare, we defined a period beyond which infants’ data were not included in the final analysis. The upper limit of this period was set at 2 SDs from the average timing of all NEC cases based on postmenstrual age (PMA). This would avoid dampening a possible positive association between transfusions and NEC.
Definition of exposure
Most of the previous reports have concluded that transfusion-associated NEC is likely the result of transfusions given within the 48 h prior to the development of NEC.3 ,7 ,8 With this as a premise, infants were considered exposed if they developed NEC within 48 h following a transfusion. Infants that developed NEC and had received a transfusion within a period longer than 48 h were considered not exposed. Data from infants after they developed NEC were excluded. Overall, there were six groups of patients (table 1).
Exposure and outcome infant groups
Data collection
For the purpose of our study, the collected data included BW, gestational age, gender, race, 5 min Apgar score and small for gestational age (SGA) status defined as BW below 10% for gestational age, pharmacological treatment of a patent ductus arteriosus (PDA), ventilator days (high-frequency plus conventional mechanical ventilation), NEC, umbilical arterial catheter (UAC) insertion days and survival outcome.
Statistics
SAS V.9.1.3 was used for the statistical evaluation. A χ2 test was used to measure the degree of association between the categorical variables. A relative risk with the 95% CI was calculated for each test. A Wilcoxon rank-sum test was used to compare the continuous variables between the NEC and non-NEC groups. All tests were two-sided; p<0.05 was considered as statistically significant. Data were presented as mean±SD and as median, IQR. A simple logistic regression model was initially run between NEC as the outcome and all independent variables of interest including exposure to blood transfusions. When p<0.1, interactions and collinearity among variables were evaluated before progressing with the model. If collinearity was present, the independent variable was divided in groups and quartiles. The association between transfusion exposure and NEC was then analysed in each of these groups. Tables 4⇓⇓–7 have been adjusted for gender, race and SGA status. Extended Mantel-Haenszel test was used to evaluate the linear trend using OpenEpi V.3.0.1. Pharmacological treatment of PDA and 5 min Apgar score were excluded due to covariance with BW. The final number of patients in these tables was slightly lesser than 3060, as some non-NEC cases were lost due to incomplete data in the multivariable analyses. To address potential variations in the secular rates of NEC over time, the 16-year study duration was divided in two 8-year periods. The time NEC occurred in either period was entered as another variable in the analysis.
Results
A total of 3462 VLBW infants were admitted in the study period; 397 infants, including 3 with NEC, were excluded as they died or were transferred out by day 7 of life. The mean PMA for developing NEC was 30.4±2.6 weeks; median was 30.4 (3.4) (figure 1). Using this mean, the upper limit of the NEC period was thus defined at 35.6 weeks. Five infants were also excluded as they developed NEC after this period. Three thousand and sixty infants were available for the analysis. The median number of transfusions received by each infant was 2 (6). The incidence of NEC remained constant over this time with a mean 6.0±1.9% (figure 2).
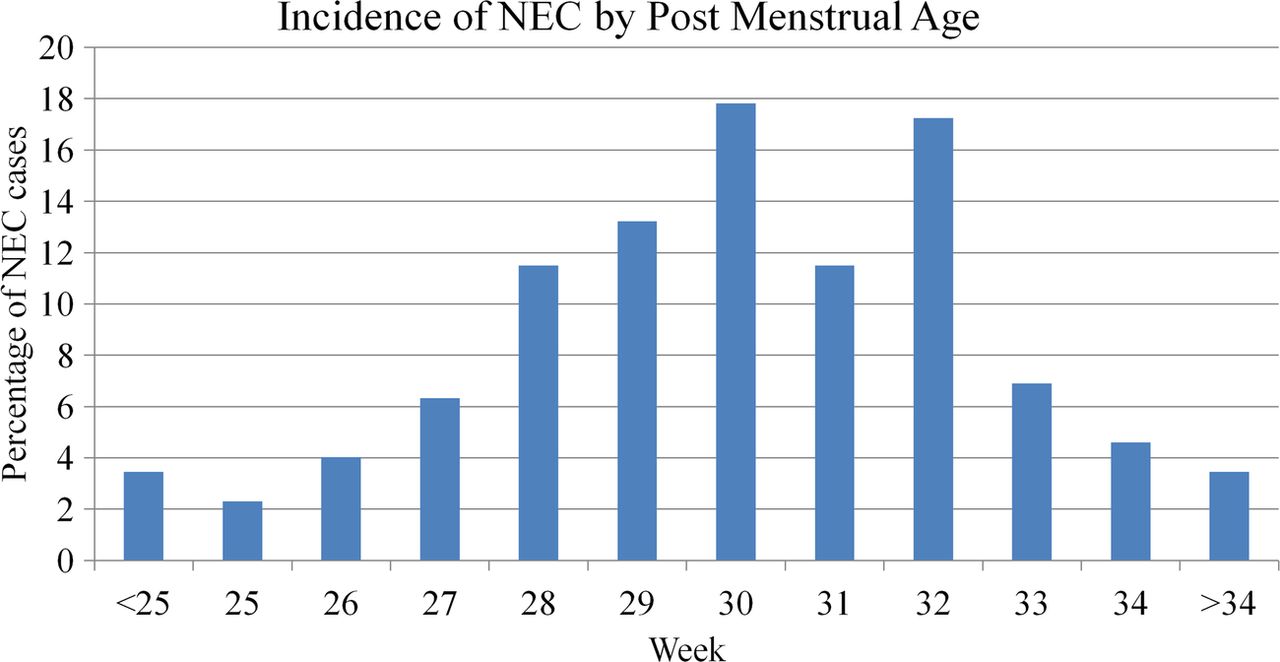
Incidence of necrotising enterocolitis by postmenstrual age.
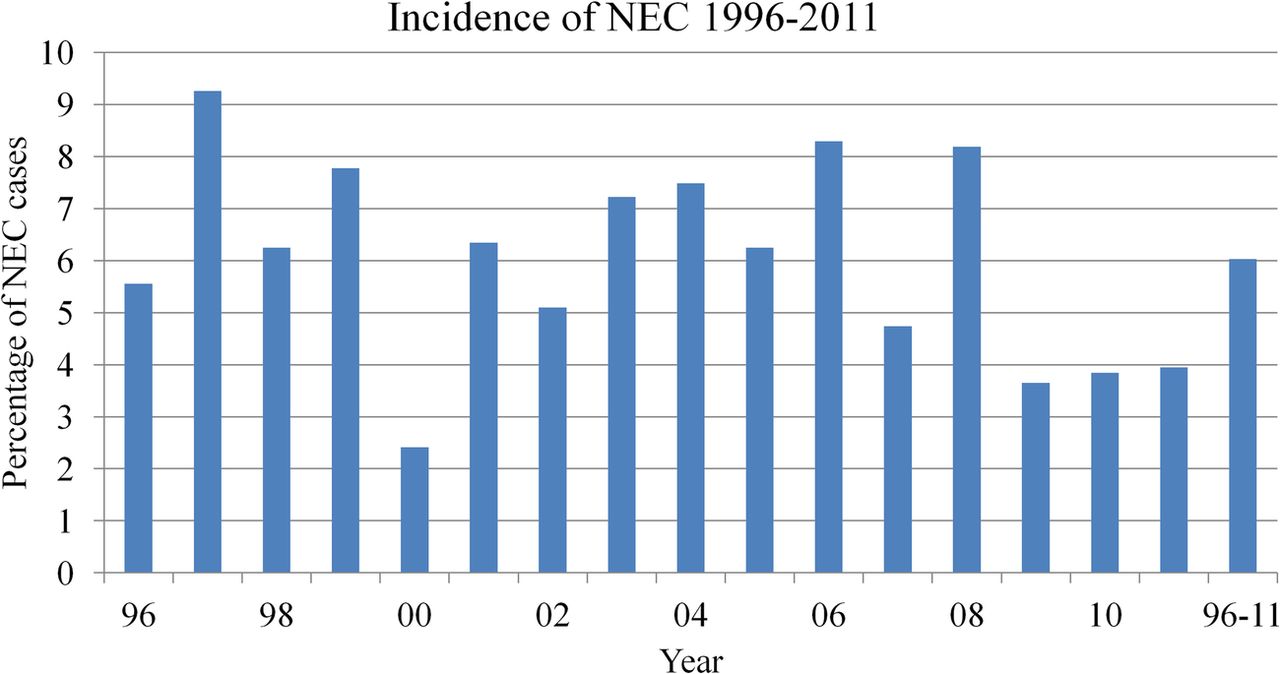
Incidence of necrotising enterocolitis over the study period.
One hundred and seventy-four infants (5.7%) developed NEC; 116 of the 174 (67%) infants had NEC within the 48 h after exposure to a blood transfusion. In the univariate analysis, NEC was associated with BW, gestational age, UAC insertion days, the number of days on a ventilator and the number of transfusions (table 2).
Univariate analysis with NEC as outcome
Evaluating for collinearity, gestational age and the number of transfusions were dropped as BW and exposure, respectively, covaried with and represented both variables. BW, UAC insertion days, ventilator days and exposure to blood transfusions were highly collinear with each other. The correlation coefficients between any two of these four variables ranged 0.45 –0.64 (p<0.0001 for all coefficients). These coefficients were much stronger than each with NEC, where the correlation coefficients were lower, 0.052–0.077 (p<0.0001–0.006). These markers likely represented the same phenomenon, mainly the severity of illness. The transfusion-NEC association was thus evaluated in the context of each variable alone. BW was stratified into four clinical groups (table 3).
Clinical characteristics by birth weight group
Exposure to blood transfusions was protective in infants with BW ≤1000 g, those who stayed longer on a ventilator, and those who required a longer UAC insertion period. However, exposure to blood transfusions carried a risk for developing NEC in infants with less severity of illness markers. These infants with BW of 1001–1500 g and who did not need mechanical ventilation or did not require UAC insertion had a higher risk of developing NEC after a transfusion exposure (tables 3⇓⇓–6).
Multivariate risk of developing NEC by weight subgroup
Multivariate risk of developing NEC by ventilator day periods
Multivariate risk of developing NEC by UAC insertion day periods
The association of exposure and the development of NEC after 28 days of life was also examined (table 7). Smaller infants were again less likely to develop NEC after exposure to a transfusion.
Multivariate risk of the (late) onset NEC after day 28 by BW group
In the 174 infants who developed NEC, exposed infants (n=116) were of a lower postmenstrual age at the time of NEC, median=30.2 (3.2) compared with 31.1 (3.1) weeks in the non-exposed infants, p=0.02 (figure 3). When stratified by BW, there was no statistically significant difference in the incidence of NEC by PMA between the exposed and non-exposed infants based on the four BW groups. Evaluating the differences between two BW groups at 1000 g cut-off showed that infants with BW ≤1000 g had significantly more UAC insertion days, median 7 (9) vs 0 (4) days, more ventilation days, median 15 (22) vs 3 (5) and more transfusions 8 (12) vs 3 (4), p<0.01 for all, than infants with BW >1000 g.

{kind=link}
{kind=link}
{kind=link}
Effect of exposure on the incidence of necrotising enterocolitis by postmenstrual age.
Discussion
This is the first study showing that the association between NEC and transfusion is not similar among different BW groups. We expected to see a much higher association in the group that received transfusions the most: the extremely low BW infants with BW ≤1000 g. Our findings were completely the reverse. The exposure to transfusions was significantly less likely to be associated with NEC in ≤1000 infants and more likely associated with NEC in larger infants with BW of 1001–1500 g.
Because of their critical condition and finite blood volume, VLBW infants tend to have transfusion thresholds that are inversely proportional to their BW. In a systemic review of prospective randomised studies evaluating the haematocrit thresholds with morbidity outcomes, infants who were transfused more and maintained a higher haematocrit were less likely to develop NEC.10 Retrospective studies evaluating the association between anaemia, exposure and NEC also had similar conclusions.4 ,6 ,7 In our practice, VLBW infants were initially transfused when their haematocrit dropped below a predefined level in their first weeks of life. With age, these predefined levels changed from a preset haematocrit level to the presence of clinical signs combined with oxygen demands. Our practice has remained in parallel with the universal approach.11 In a recent survey, 1018 neonatologists from 11 countries responded with a minimal variability, that in the first week of life higher haematocrit thresholds were targeted irrespective of the degree of respiratory support. At the 4 weeks of life, however, decisions were more variable, with transfusion haematocrit thresholds being affected by the degree of oxygen requirements.12 By that time, variable levels of gut injury may already have been potentiating the development of NEC. The clinical signs such as tachycardia and increased frequency of apnoea could well represent preclinical NEC and not the severity of anaemia. This consensus among neonatologists of accepting lower haematocrit levels for larger infants and our findings of an increased risk of NEC postexposure only in the larger two BW groups strongly suggests that the severity of anaemia may have a significant impact on the development of NEC post-transfusion.
In some studies, infants with exposure associated NEC were reported as older by an average of 2–3 weeks compared with non-exposed NEC infants; they were also ‘stable’ with no clinical signs of illness.4 ,7 ,8 Being older may reflect a longer period of anaemia and lower haematocrit level. In our cohort, exposed infants with NEC were older by only 5 days compared with non-exposed NEC infants, much in contrast to the 2-week to 3-week period previously mentioned. We also did not observe different results when only infants with the late onset NEC were evaluated.
Severity of illness has been proposed as another factor affecting the association between exposure to PRBC and the development of NEC. Exposed infants were more likely to be ventilated,2 ,4 ,7 ,8 have a PDA,4 ,7 ,8 and have a lower BW.1 ,2 ,7 ,8 As all variables exhibit some interaction, interpretation of these results becomes difficult. We initially arrived at similar conclusions. In unadjusted analysis, longer ventilator days and longer UAC placement days increased the likelihood for developing NEC. A prolonged UAC period likely reflected poor intravascular access, frequent blood draws and/or haemodynamic instability. When both variables were stratified into four periods based on quartiles, infants who had longer periods on a ventilator and UAC placement were less likely to develop NEC. The linear change in the RR was very significant. These infants were also in the lowest BW group at ≤1000 g. Thus, and in contrast to current reports, severity of illness, represented here by infants with lowest BWs and longest ventilator days, was not a risk for exposure associated NEC.
Recently, a meta-analysis of reported case studies on the association of NEC and blood transfusion concluded that recent exposure to transfusion was associated with NEC.13 Case studies can produce an exaggerated effect size as compared with cohort studies.14 Kirpalani et al15 has recently reviewed the effects of study design on the outcome of the association between transfusions and NEC. Randomised control trials showed an opposite effect to observational trials; higher transfusions were associated with a lower incidence of NEC. Most observational trials had the problem of confounding or small sample size. Since there was not any matching performed in our study, we were able to evaluate BW as an independent variable and show its significance.
There were several limitations to our study. Bias due to its retrospective nature limited our ability to differentiate between the overlapping preclinical signs of NEC and those of anaemia. Information about haematocrit levels in the first half of the study period were inaccessible. This limited our ability to test for anaemia as a plausible explanation. Information about the use of antenatal steroids was also not available. The treatment with antenatal corticosteroids has been shown to be associated with an overall reduction in necrotising enterocolitis.16 Lower weight infants may have received antenatal steroids more frequently than larger infants, thereby lowering the risk for development of NEC. Another limitation pertains to the days to total feeds and formula versus breast milk use. Historically in our unit, breast milk use was less than 20% and only increased above 60% in the last 2 years of the study period. There are also concerns about the lack of increased superior mesenteric artery blood flow in response to a feeding, following a blood transfusion,17 suggesting that feeds should be held after a transfusion. These results could be attributed to using older blood as it has been shown that by 2 weeks of shelve life, stored PRBC lose the ability to cause regional vasodilation and to increase oxygen uptake by the tissue when compared with fresh PRBC stored for 3–7 days.18 ,19 In our practice, PRBC units are usually exhausted within 4–10 days of postcollection. Using fresh blood for transfusions may explain our study findings but with data not available, this would be a speculation.
A likely explanation of the study findings would be that as an infant's BW increases, there is a threshold crossed that changes the polarity of the association between exposure and NEC. This is nicely demonstrated in the progressive increase in the relative risk value with each weight group. The threshold could be a change in clinical practice like using a lower transfusion limit. It could also be some other factor related to gut maturity, to feeding practice, or altogether still to be discovered.
In summary, using cohort approach in the investigation eliminated the need for matching by BW and lead to new information about different levels of association between blood transfusions and NEC in different weight groups. Our findings show that exposure to transfusions does not increase the risk of NEC. Specifically, after exposure to a PRBC transfusion, ≤1000 g BW infants were less likely to develop NEC than were infants born 1001–1500 g BW. These larger infants were likely to have lower transfusion thresholds as they were less ill and probably more anaemic. We speculate that anaemia could be the cause of their exposure-associated NEC. Future studies evaluating this association should be prospective, should incorporate BW as a risk factor and should incorporate newer modalities such as near-infrared spectroscopy to evaluate hypoxia at the intestinal level.20
Acknowledgments
The authors would like to thank Dr David Armbruster for his help editing the manuscript.
References
Footnotes
-
Contributors All the authors have participated in the conception and design of the study and then in the analysis and interpretation of the data. They all contributed to the drafting of the article. They all gave final approval of the version submitted.
-
Funding This research received no specific grant from any funding agency in the public, commercial or not-for-profit sectors.
-
Competing interests None.
-
Ethics approval The study protocol was approved by the Institutional Review Board at the University of Tennessee Health Science Center.
-
Provenance and peer review Not commissioned; externally peer reviewed.
-
Data sharing statement No additional data are available.