Article Text

Abstract
Objectives This study aims primarily to determine whether whole body MRI (WB-MRI) and Sestamibi Technetium-99m-bone marrow (MIBI) scans in the same patients produce the same estimate of disease load and location, and secondly, to study possible association between the bone disease detected by these scans and the effect on disease outcome and survival. Bone disease occurs in about 90% of multiple myeloma (MM) patients. There are no data comparing the new diagnostic modalities with WB-MRI and MIBI in MM.
Design A prospective comparative study between WB-MRI and MIBI scans in assessing bone disease and outcome of MM.
Participants and methods Sixty-two consecutive patients with confirmed MM underwent simultaneous WB-MRI (both axial T1 and turbo spin echo short tau inversion recovery (STIR)) and MIBI scans at a single institution from January 2010 to January 2011, and their survival status was determined in January 2012. The median age was 62 years (range 37–88) with a male-to-female ratio of 33 : 29.
Results In vertebrae and long bones, MRI scan detected more disease compared with MIBI scan (p<0.001) but there was less difference in the skull (p=0.09). In the ribcage, the MIBI scan detected more lytic lesions of the ribs compared with MRI scan (p<0.001). Thirteen of the 62 patients died during the 24-month follow-up. Increased disease detected in all bones by both scans was associated with increased mortality risk (MIBI p=0.001; MRI-STIR p=0.044; but not MRI-T1 p=0.44). In all combined bone groups, the mean MIBI scan results provided a better prediction of mortality than MRI scan over the follow-up period (MRI-T1 vs MIBI p=0.019; MRI-STIR vs MIBI p=0.047).
Conclusions Although WB-MRI detected more MM bone disease, MIBI scan predicted overall disease outcome and mortality better than MRI scan. Further studies to define optimum use of these imaging techniques are warranted.
Trial registration number The study was registered prospectively in the Australian and New Zealand Clinical Trials Registry at http://www.ANZCTR.org.au under No: ACTRN12609000761268.
- Nuclear Medicine
- Radiology & Imaging
- Qualitative Research
This is an open-access article distributed under the terms of the Creative Commons Attribution Non-commercial License, which permits use, distribution, and reproduction in any medium, provided the original work is properly cited, the use is non commercial and is otherwise in compliance with the license. See: http://creativecommons.org/licenses/by-nc/2.0/ and http://creativecommons.org/licenses/by-nc/2.0/legalcode.
Statistics from Altmetric.com
Article summary
Article focus
-
Bone disease occurs in about 90% of multiple myeloma (MM) patients.
-
Among the four available radionuclear imaging techniques, there are no data comparing whole-body MRI (WB-MRI) and Sestamibi Technetium-99m-MIBI bone marrow (MIBI) scan in assessing bone disease in MM.
-
Therefore, there is a growing interest in the role of MIBI scanning in conjunction with WB-MRI in determining the extent of myeloma bone disease and the prediction of disease outcome.
Key messages
-
WB-MRI scan identifies more myeloma bone disease than the MIBI scan with more sensitivity in detecting myelomatous deposits in the spine and to a lesser extent, in the pelvic and long bones. However, in the ribcage, MIBI scan detected more disease compared to MRI scan (p<0.001).
-
A novel finding shows that MIBI scan obtains an image of all important bone compartments in the body in one single examination, and is less time consuming and more comfortable for the patient than MRI.
-
MIBI scan was able to predict overall disease outcome and mortality better than MRI scan.
Strengths and limitations of this study
-
The study was performed prospectively in 62 consecutive MM patients.
-
The two scan modalities were performed within 2 days of each other and were assessed uniformly by expert radiologists and nuclear medicine physicians in order to minimise possible bias.
-
This is considered as the first study with head-to-head comparison between both modalities, and can therefore be used as a basis for larger studies.
-
It was assumed that the MRI and the MIBI scan scoring scales were measuring the same disease properties. This, however, may have introduced an unknown degree of imprecision in our estimates.
-
The studied group represents a heterogeneous group of myeloma patients. In theory, different treatments and lytic lesions may be detected by one method over the other due to the potential different sensitivity between both imaging modalities. However, this was not addressed by the current study and may require further investigation.
Introduction
Multiple myeloma (MM) is a malignant neoplasm of plasma cells resulting in osseous destruction.1–3 Most institutions utilise a skeletal survey in order to radiologically assess MM at diagnosis.3–5 Although skeletal survey was considered for many decades as a standard radiological technique in the diagnosis and staging of myeloma bone disease, it has a high false-negative rate of between 30% and 70% leading to underestimation of disease burden.6 ,7 MRI is currently used in several contexts in the monitoring of MM with high sensitivity compared with CT scan in detecting myeloma bone lesions.5–7 MRI is useful in identifying MM by its infiltration of normal fat within the bone marrow.5–8 Marrow infiltration seen on MRI can be used to assess the tumour burden present at diagnosis.7–9 In 2005, the Durie and Salmon staging system was refined to include whole body MRI (WB-MRI) where available.10 ,11
Sestamibi Technetium-99m MIBI bone marrow scanning (MIBI) accurately represents myeloma activity in the bone marrow with high sensitivity and specificity.12–14 There is also a linear correlation between bone marrow biopsy results and uptake on MIBI scan.12 However, there are no available data comparing MRI and MIBI scans in assessing disease activity and mortality in MM. Currently, MRI is the imaging modality of choice in staging MM disease according to the Durie-Salmon-PLUS staging system.10 Radionuclide imaging offers a potential alternative or supplement to radiographic detection and assessment of disease activity.11–17 There is scant evidence comparing MRI and MIBI bone marrow scans in assessing disease activity in MM in a cohort of this size. Therefore, there is a growing interest and recognition of the important role of MIBI bone marrow scan in imaging malignant tumours.
Rationale and aims of the study
Bone disease occurs in about 90% of MM patients.3 There are four available routine radio-nuclear imaging techniques for the diagnosis of bone disease in MM, which are plain x-ray, CT, MRI and bone scans.5 ,11 ,15 Another technology employing positron emission tomography (PET) is considered mainly for research purposes and is not performed routinely for the diagnosis of myeloma. Plain radiographs can only demonstrate lytic bone disease when 30% or above of trabecular bone has been lost, which represents a late stage of the disease.15 ,16 Furthermore, skeletal survey is not sensitive enough to monitor the responses to therapy.
Technetium-99m bone scanning without sestamibi is not appropriate for evaluating myeloma bone disease since bone scans reflect osteoblastic activity and thus, underestimates the extent of osteolytic lesions characteristic for myeloma bone disease.12–14 MIBI scanning has been investigated in myeloma patients because it is concentrated in myeloma tissue and thus, was found to be more sensitive than skeletal survey (77% vs 45%) and was highly specific for staging myeloma patients.17
MRI has been proven in many studies to be more accurate than plain x-ray or CT scan in detecting myeloma bone lesions with a higher sensitivity.6–9 Therefore, MRI is considered to be a useful tool in the prediction of myeloma disease response; hence, new guidelines have integrated MRI as part of the staging of myeloma bone disease.10 ,11 However, WB-MRI is a potential imaging method for high-resolution screening of the whole skeleton in patients with MM.8
There are little data available regarding this new technique especially in conjunction with other newly developed techniques like Sestamibi Technetium-99m in diagnosis and follow-up of MM or prediction of disease outcome. To date there is no head-to-head comparison between WB-MRI and MIBI scans in MM.
This study aims to determine whether: (1) In simultaneous WB-MRI and MIBI scans in the same patients, do both scans produce the same estimate of disease load and location (intermodality reliability), or does one of the scans suggests more extensive disease than the other. (2) Is there a greater association between the estimate of the extent of bone disease in one or other of the scans and the likelihood of death?
Subjects and methods
This study was conducted at the Launceston General Hospital, a tertiary referral centre for Northern Tasmania, Australia and was approved by the state-wide Human Ethics Committee of Tasmania. Informed consent was obtained from all participants in accordance with the Declaration of Helsinki. The study was registered prospectively at the Australia and New Zealand Clinical Trial Registry web site under registration No: ACTRN12609000761268 and in the NHS-UK website:http://www.nhs.uk/Conditions/MRI-scan/Pages/clinical-trial-details.aspx?TrialId=ACTRN12609000761268.
There were 62 consecutive patients with a median age of 62 years (range 37–88) and a male-to-female ratio of 33 : 29 recruited at a single centre. Median duration of follow-up was 16.8 months (maximum 24 months), during which 13 of 62 patients succumbed. Most of the patients had IgG (35 patients) myeloma while 15 patients had IgA myeloma, four patients had smouldering myeloma and the remaining eight patients had light chain myeloma. The WHO criteria were used for the diagnosis of MM.18
A standard therapy with dexamethasone and thalidomide was applied in most of the cases (table 1). Second-line treatment was started after failing to achieve at least a minimal response with the first treatment defined by disease progression of 25% in serum M protein (at least 5 g/l) or urinary Bence Jones protein (at least 200 mg/day), or 50% increase of serum free light chain level, or 10% increase of marrow plasmacytosis, or increase of the number of lytic lesions, or the presence of hypercalcaemia (corrected serum calcium >2.65 mmol/l), or finally in case of non-toleration to the first-line treatment. The salvage therapy include lenalidomide (12) or bortezomib (8), determined by disease stage and toleration of treatment. Ten patients underwent bone marrow transplantation.
Patient characteristics
Diagnostic management
Once enrolled in the trial, the participants underwent a MIBI scan and a WB-MRI. The vast majority of patients had both scans on the same day and all of them were performed within 48 h of each other with the MRI scan performed first. This was to avoid any possible effect of the Sestamibi Technetium-99m injection on the MRI scan results. The scans were interpreted by two independent consultant radiologists and nuclear medicine physicians with greater than 15 years of experience. The results were converted into a spreadsheet format where the body was represented as 61 bone compartments for statistical analysis. The same radiologists and nuclear medicine physicians were used to interpret all the scans using the same special format. Standardised protocols and assessments were used for both MRI and MIBI scans.
MRI protocol
The same machine was used for all the MRIs performed—an Avanto 1.5T system from Siemens Medical Solutions. A similar protocol to Baur-Melnyk et al8 was employed with some modifications. The patients were placed head-first in the supine position. Head, neck, body-matrix and peripheral coils were utilised. For the examination of the spine, T1-weighted turbo spin-echo (TR/TE 584/10 for upper and 520/11 for lower, field of view 350 mm upper 380 mm lower, slice thickness 3 mm upper, 3.5 mm lower) and turbo spin echo short tau inversion recovery (STIR; TR/TE/T1 5000/51/180, field of view 350 mm upper, 380 mm lower, slice thickness 3 mm upper 3.5 mm lower) were performed in the sagittal plane.
The base of skull and vertex were imaged in the axial plane with T1-weighted spin-echo (TR/TE 575/11, field of view 230 mm, slice thickness 5 mm) and turbo spin echo STIR (TR/TE/T1 6980/11/180). The sternum and posterior ribs were imaged in the coronal plane with T1-weighted turbo spin echo (TR/TE 596/7.8, field of view 480 mm, thickness of slice 5 mm) and turbo spin echo STIR (TR/TE/T1 7490/100/170). However, the ribs are too small for their internal marrow signal to be confidently interpreted, especially on T1 images, unless they are obviously destroyed or if there is a large lesion arising from the ribs. The pelvis was imaged in the coronal plane with T1-weighted turbo spin echo (TR/TE 682/11, field of view 480 mm and slice thickness 5 mm) and turbo spin echo STIR (TR/TE 4200/87/170). The lower limbs down to the mid-shin of the tibia were imaged in the coronal plane spin with T1-weighted turbo spin echo (TR/TE 504/11, field of view 480 mm, slice thickness 5 mm) and turbo spin echo STIR (TR/TE/T1 3850/87/170). The mean time for each scan to occur was 50 min.
Sestamibi bone marrow scan protocol
The same dose of MIBI—30 mCi (1110 MBq)—was used for each patient. Prior to intravenous injection, each patient was rested on the bed for at least 20 min.
Imaging started at 5 min postinjection with a wide field of view γ-camera equipped with a low-energy high-resolution collimator. The WB scan proceeded at 30 cm/min. When completed, lateral femora images were taken with each view, took approximately 2 min and, if required, a single positron emission CT was performed.
Outcome measures
The extent of bone MM as interpreted using the MRI scans was classified anatomically as focal or diffuse and then, according to intensity of the lesion, to high, intermediate and low. The extent of bone marrow MIBI uptake was scored accordingly. Morphology was classed as normal, diffuse, focal or micronodular. Severity was graded as low (<20% infiltration), intermediate (20–50% infiltration) or high (>50% infiltration), and the severity scale was applied only to the focal morphology. The severity and grade of positive diagnostic imaging reports were treated as a single rank order scale: 0=no lesions; 1=low-density focal; 2=intermediate-density focal; 3=high-density focal; 4=focal diffuse; 5=diffuse. The posterior ribs could not be imaged in the MRI scan, but the sternum could be imaged. Thus, the results for 25 ribcage bones in each patient (12 ribs by 2 sides plus sternum) were available for the MIBI and MRI-STIR scans, and one ribcage bone result (sternum only) was available for the MRI-T1 scan.
In a number of the result scale versus scan categories, no patient existed in that condition, or there was no death in a patient with that condition. In order to allow analysis of mortality data: (1) the no detection and low-intensity focal disease categories were combined and (2) the focal diffuse and diffuse categories were combined. The mortality status of the patients in January 2012 was determined using the Australian National Death Register to avoid distress to relatives caused by sending communications to patients who have died.
Statistical analysis
Concordance between MIBI and WB-MRI (either axial plane with T1 or turbo spin echo STIR) was tested by calculation of the kappa statistic for inter-rater agreement, expressed as observed and expected agreement (expected agreement is based on the random distribution of diagnostic results); κ value (range −1.00 to 0 to 1.00 indicating high discordance to no concordance to full concordance, respectively); and p value. The number of positive results reported from the three scan modalities for each bone group (using the scan scale score for each scan as the outcome variable and the scan method as the predictor variable) were compared in the same patients at the same time using repeated-measures ordered logistic regression (a non-parametric equivalent of general linear modelling; with results expressed as OR with 95% CIs and p values). Adjustment for age, gender and time from diagnosis did not alter the OR estimates, so no adjusted results are reported for this analysis. Each group of bones was assessed separately, but the readings from all the bone compartments in each group were pooled. The association between time in months from the scan performance to death or censoring date of 1 January 2012 and the severity and grade of positive diagnostic results was compared using repeated-measures Cox proportional hazards regression (HR; 95% CIs; p values), adjusted for age and gender, time from diagnosis to imaging scans, clinical stage, number of lines of treatment, M-component and cytogenetic abnormalities. This was done using simultaneous interaction analysis with inclusion of each of the results of the three imaging modalities in the models, in order to determine which imaging modality most closely predicted mortality under the clinical management given to the patients. Results were corrected for multiple comparisons which were appropriate using the Holm method. All analyses were performed using Stata SE12.0 for Windows (StataCorp, College Station, Texas, USA).
Results
We have analysed both scan results according to bone compartments. Furthermore, we have entered the results of MRI scan images in two different categories according to image type as MRI-T1 (axial plane with T1) or MRI-STIR (turbo spin echo STIR). In detecting skull lytic lesions, there were no significant differences between the scans; however, there was a tendency for MRI scan to detect more MM lesions than MIBI scan (p=0.09). Nevertheless, for vertebral lytic disease (cervical, thoracic and lumbar), both MRI-T1 and MRI-STIR detected more disease than MIBI scan (p<0.001). There was no statistical difference between both MRI techniques in detecting myeloma bone disease in the spine. In the pelvis, MRI-T1 detected significantly more disease than MIBI scan (p=0.03) while there is no statistical difference between MRI-STIR and MIBI scan. In the long bones (femur, humerus, clavicle and scapula), MRI-T1 detected less disease than MIBI scan (p<0.001), while there were no significant differences noted between both MRI-STIR and MIBI scans. In the ribcage, the MRI-T1 imaged the sternum but was not technically able to detect the myeloma involvement of the ribs, while the MIBI scan showed a significant ability in detecting lytic lesion of the ribs over MRI-STIR scan (p<0.001).
Thirteen of the 62 patients died during the 24-month follow-up period, all from progression of MM. When the association between scan result and death rate secondary to disease progression (as measured by HR) was examined (figure 1), a clear step-wise increase in likelihood of death was seen for the MIBI scan for all bone compartments taken together, while the association was more irregular for the MRI scans (tables 2 and 3). This trend was seen in the combined all compartments analysis (MRI-T1 vs MIBI p=0.019; MRI-STIR vs MIBI p=0.047), the ribcage (MRI-T1 vs MIBI p=0.011; MRI-STIR vs MIBI p=0.004), but was particularly strongly seen in the thoracic vertebrae (MRI-T1 vs MIBI p<0.001; MRI-STIR vs MIBI p=0.001). This pattern was less discernible in the skull, pelvis, long bones and cervical and lumbar vertebrae (figure 2). When adjusted for other prognostic indicators, in all bones combined, the mean MIBI scan result provides a better prediction of mortality than the mean result from the MRI scans (MRI_T1 vs MIBI HR for trend 0.70; 95% CI 0.53 to 0.92; p=0.019: and MRI-STIR vs MIBI HR for trend 0.80; 95% CI 0.64 to 1.00; p=0.044) when patients receive standard therapy for myeloma (table 3). If the combined thoracic vertebrae and ribcage bones are examined in isolation, the MIBI results provide a good prediction of mortality over 24 months (mean result per bone group HR for trend 2.58; 95% CI 1.73 to 3.86; p<0.001), while the MRI scan results compared with MIBI had lower levels of prediction (MRI-T1 mean result per bone group HR for trend 1.11; difference from MIBI 0.43; 95% CI 0.27 to 0.67; p<0.001: MRI-STIR mean result per bone group HR for trend 1.14; difference from MIBI 0.44; 95% CI 0.30 to 0.66; p<0.001). However, this bone grouping was not part of a prior hypothesis. Possible covariate associations with death rate were calculated for age (HR 3.88; 95% CI 0.95–15.9; p=0.06), gender (HR 2.69; 95% CI 0.41 to 17.6; p=0.3), time from diagnosis to scan prior to follow-up period (HR 3.38; 95% CI 0.62 to 18.4; p=0.16), presence of five or more cytogenetic abnormalities (HR 2.49; 95% CI 0.77 to 8.02; p=0.13) and lines of treatment (HR 1.44; 95% CI 0.91 to 2.28; p=0.12).

Prediction of death due to disease progression by types of lesions in different imaging methods. In the 62 myeloma patients, the upper graph represents sestamibi bone marrow scan, middle graph; whole body MRI-T1 scan and the lower graph represents the STIR version of MRI scan.
Estimates of concordance of grading* of results of MIBI, MRI and STIR scans in patients with multiple myeloma, and the relative frequency of different positive results
Disease progression risk with subsequent mortality in association with positive bone marrow scan (MIBI) or MRI results

Association between result score of imaging modality: relative risk as HR (95% CIs; p value) was estimated using Cox proportional hazards regression, adjusted for age, gender and time from diagnosis to imaging scans; p values corrected for multiple comparisons by the Holm method. Each result score value was treated as a continuous variable to estimate the linear trends in mortality: the absolute trend for each modality was estimated (shown as symbol and error bars), and then the relative trends of the two MRI modalities were compared to the MIBI scan trend (shown as p values only).
Cost-effectiveness analysis
There is no cost item for WB-MRI scan at present in the benefit scheme of Medicare Australia; however, based on approximate costs of skull MRI ($403.20), pelvic MRI ($403.20) and Spine MRI ($358), the total costs would be about $1164.4 while MIBI scan cost is $489.7. Nevertheless, a full body MRI scan may cost less than combining different body parts as it is less labour intensive and time consuming. At the time of analysis $1 AUD is equal to $1 USD.
Discussion
The true gold standard for myeloma disease detection would be bone marrow biopsy with histological, molecular biological and histochemical examination of the biopsy specimens in a laboratory where disease prognosis will be determined by the acquired genetic changes in the bone marrow cells and the resulting proliferation and location defects. This is obviously not feasible, since the relevant bones may be inaccessible, and the biopsy process would be destructive and unacceptable to patients and treating physicians.
Here, the clinicians are forced to apply indirect scanning methods, which involve transmission or emission of various radiations (x-ray, CT, MRI or nuclear medicine scans). These depend not on the absolute properties of the abnormal cells that directly control the disease severity, but on the relative absorption/transmission of the radiation compared with the non-diseased tissue. Therefore, each method will have its own rate of false-positive and false-negative results. Nonetheless, because none of these modalities has been validated against the true measure of the disease, those rates are unknown. However, as an indirect measure of this gold standard, the disease progression experience of the patients is used as a proxy for disease severity.
There are a number of positive findings which have emerged from our study. As a direct comparison between both MIBI and WB-MRI scans in diagnosis of bone disease of MM, it seems that the MRI scan identifies more MM bone disease than the MIBI scan with more sensitivity in detecting myelomatous deposits in the spine and to a lesser extent in the pelvis and long bones. In the ribcage, MIBI scan detected more disease compared with MRI scan (p<0.001), noting that the MRI scan of the ribcage is technically more difficult due to patient movement including breathing. Comparison between axial T1-weighted and STIR sequences shows that the former is more sensitive in detecting myelomatous disease in the vertebrae than STIR imaging. This is largely because the lesions are predominantly of intermediate and low signal at both T1-weighted and STIR imaging, and are better outlined and contrasted when marrow fat signal is preserved, as in T1-weighted imaging. The STIR sequence selectively suppresses the signal from fatty marrow in the spine, reducing lesion contrast and detection sensitivity (figure 3). Lesions that are of intermediate or low signal at T1-weighted MRI and high signal at STIR MRI are in the minority. Our analysis compares the results of the three scans (two interpretations of an MRI scan and an MIBI scan) for each patient, and then sums those comparisons across the entire patient group. Since each patient has the same age, gender and time from diagnosis for that internal comparison, those covariates will have no effect on the intrasubject comparison. Unless there is a systematic strong effect on the difference between the scans (which was not seen), the estimates of the difference across the group will not be changed. The pattern of prognostic prediction differs from the degree of identification of MM bone lesions suggesting that the nuclear medicine MIBI scan provides a better prediction of disease mortality than either of the MRI sequences (MRI-T1 vs MIBI p=0.19; MRI-STIR vs MIBI p=0.047). This may suggest that some MRI-detected lesions are of lesser significance than those imaged by the MIBI scan. This is intuitively unsurprising for at least two possible reasons: (1) not all lesions that are of intermediate or low signal on T1-weighted and STIR imaging represent myelomatous deposits; and (2) myeloma deposits that are clinically quiescent may appear morphologically similar to those that progress. It is worth noting that both MIBI scan and WB-MRI scans performed better than conventional skeletal plain x-ray survey as 15 patients and 14 patients, respectively, had a higher clinical staging according to both scans compared with routinely performed x-ray examination (table 1).
{kind=link}
{kind=link}
{kind=link}
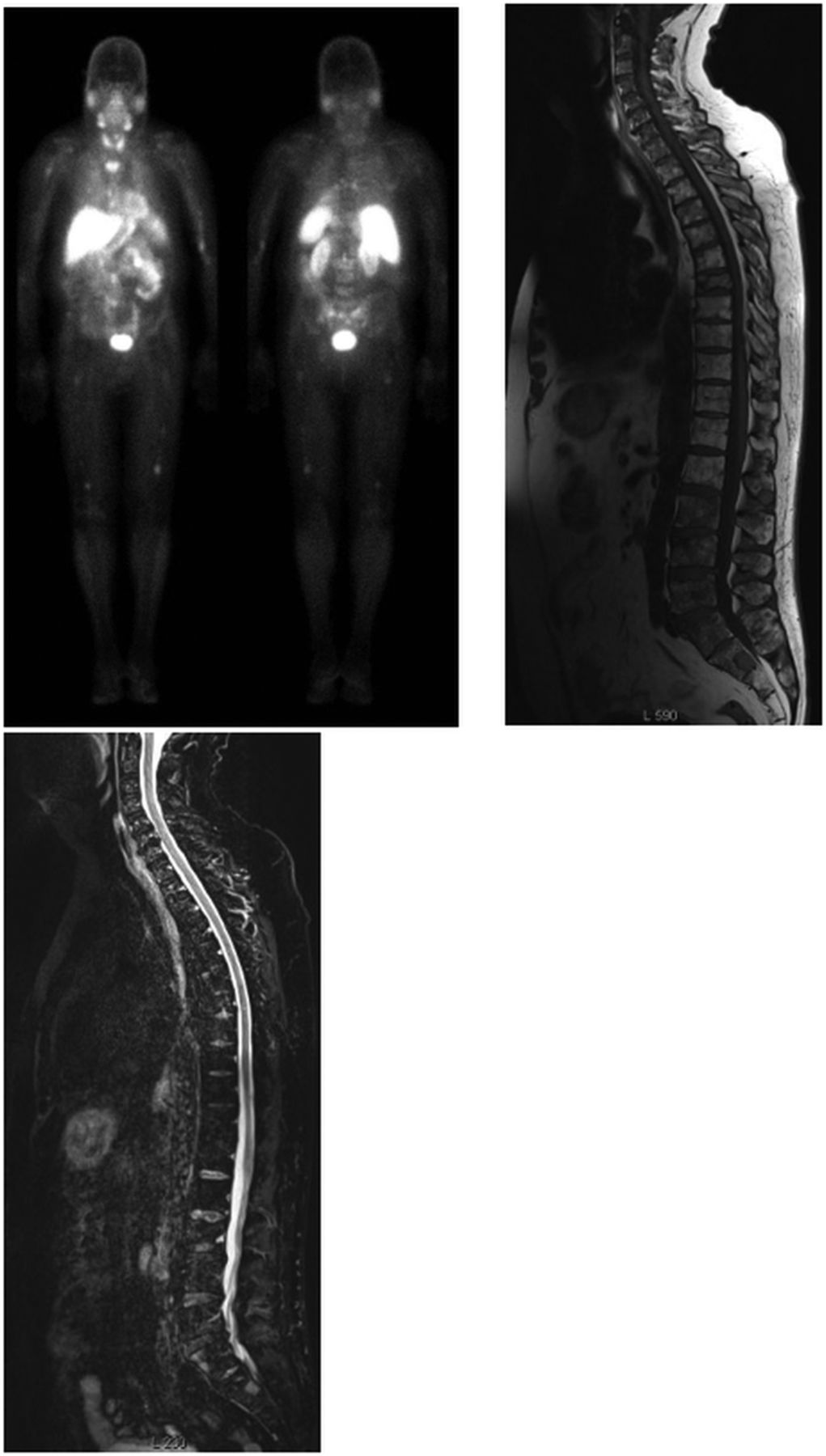
The image on the upper left is a Sestamibi Technetium-99m-bone marrow scan that demonstrates high-grade focal lesions in the sacrum plus L3, L4 and L5 vertebrae. Low-grade focal lesions are also seen in the T1 vertebrae, right scapula, right-sided sixth rib, bilateral femora and humeri. The upper right is a T1-weighted MRI of the spine that demonstrates high grade focal lesions from L2 to L5 and in the sacrum in the same patient. Low-grade focal lesions are also demonstrated in the T4–T7 vertebrae while T7 shows an old compression fracture. The lower image is a short tau inversion recovery sequence (STIR) MRI of the spine that demonstrates heterogeneous signal from L2-L5, compatible with but not as obvious as the findings on the T1 image in the lumbar region of the same patient in our study cohort.
Several trials compared WB-MRI scan versus CT scan and showed superior results favouring the MRI scan.7 ,8 ,10 However, no correlation has been made in the prediction of overall disease outcome or death rate as our study suggests. On the other hand, one study showed that MIBI scan detects additional MM sites compared with skeletal survey in 38 of 56 studied patients (68%). This is considered superior to FDG-PET scan that detects 50% of additional sites for MM over skeletal survey.19
Our study has a few shortcomings. First, the two scales of assessment of severity of MM bone involvement (none, focal, focal-diffuse and diffuse) and signal density (low, intermediate and high, applied only to focal morphology) were assumed to be able to be converted into a single sequential scale, that is, positively associated with tumour mass in order to simplify the analysis. It was also assumed that the MRI and the MIBI scan scoring scales were measuring the same disease properties. This, however, may have introduced an unknown degree of imprecision in our estimates. Second, all the patients were receiving standard chemotherapy for myeloma, and tumour infiltration that can be detected by one technique may be influenced by certain therapy compared with a tumour that can be detected by the other imaging modality.
In summary, MIBI scan obtains an image of all important bone compartments in the body in one single examination, and is less time consuming and more comfortable for the patient than MRI. Although there is a mild-to-moderate degree of intermodality reliability between the different imaging techniques, the two MRI modalities appear to report higher grades of bone lesions than the MIBI scan. Moreover, our study suggests that mortality is better predicted by components of the MIBI scan, although this observation would need to be confirmed in other studies. The greater apparent lesion detection and poorer prognostic performance of MRI scans may occur either through imaging of malignant tissue that has been possibly affected by chemotherapy, or through imaging of tissue reactions that have little prognostic significance. Alternatively, the MRI scans may be more sensitive to early disease than MIBI scans and that early disease may manifest itself at a date beyond our short window of observation. Our data suggest that it is beneficial to employ the new technology with WB-MRI and MIBI scans in prediction of myeloma disease progression as well as outcome. Further trials will be required to confirm the utility of these different imaging modalities.
Acknowledgments
The authors acknowledge Mr Garth Faulkner, Business Manager of the Radiology Department at the Launceston General Hospital for his continuous support that enable the conduction of the study. The authors also wish to acknowledge that statistical support was funded by the Clifford Craig Medical Research Trust, Launceston, Tasmania, Australia.
References
Footnotes
-
This paper was presented at the Annual Meeting of the Haematology Society of Australia and New Zealand, Sydney, NSW, Australia in October 2011 and 2012.
-
Contributors AAK is the principal investigator of the study who organised and coordinated all aspects of the research including all steps of the manuscript preparation. He designed the study and recruited the patients. He has contributed in writing, reviewing, editing and approving the manuscript in its final form. AS, RH and LBT contributed to study design, analysis and interpretation of data and revised the manuscript in its final form. IKR performed all statistical analyses and interpreted the data and wrote the results section and revised the manuscript in its final form. JA and RD conducted the scans for the patients and helped in drafting the manuscript and writing the results. RH, SR collected the clinical data, performed the literature search and wrote the introduction and drafted the article and finally approved the manuscript.
-
Funding This research received funding from the Clifford Craig Medical Research Trust, Launceston, Tasmania, Australia. Clifford Craig Medical Research Trust is a local community organisation in Tasmania, Australia that supports medical research by providing monetary funds without interference in the research design or outcome. Clifford Craig Medical Trust Fund has no influence in the study design; subject, methods, data collection, analysis, interpretation of data; writing the research report or the decision to submit the manuscript for publication. The grant was used to support the research assistants.
-
Competing interests None.
-
Patient consent Obtained.
-
Ethics approval This study is approved by the Tasmanian Human Ethics Committee, Australia and all participants have signed an informed consent form in accordance with the Declaration of Helsinki. The study was registered prospectively in the Australian and New Zealand Clinical Trials Registry at http://www.ANZCTR.org.au under No: ACTRN12609000761268 and in the NHS-UK website:http://www.nhs.uk/Conditions/MRI-scan/Pages/clinical-trial-details.aspx?TrialId=ACTRN12609000761268.
-
Provenance and peer review Not commissioned; externally peer reviewed.
-
Data sharing statement No additional data are available.