Article Text

Abstract
Introduction Limb salvage with endoprosthetic reconstruction is the standard of care for the management of lower-extremity bone tumours in skeletally mature patients. The risk of deep postoperative infection in these procedures is high and the outcomes can be devastating. The most effective prophylactic antibiotic regimen remains unknown, and current clinical practice is highly varied. This trial will evaluate the effect of varying postoperative prophylactic antibiotic regimens on the incidence of deep infection following surgical excision and endoprosthetic reconstruction of lower-extremity bone tumours.
Methods and analysis This is a multicentre, blinded, randomised controlled trial, using a parallel two-arm design. 920 patients 15 years of age or older from 12 tertiary care centres across Canada and the USA who are undergoing surgical excision and endoprosthetic reconstruction of a primary bone tumour will receive either short (24 h) or long (5 days) duration postoperative antibiotics. Exclusion criteria include prior surgery or infection within the planned operative field, known colonisation with methicillin-resistant Staphylococcus aureus or vancomycin-resistant Enterococcus at enrolment, or allergy to the study antibiotics. The primary outcome will be rates of deep postoperative infections in each arm. Secondary outcomes will include type and frequency of antibiotic-related adverse events, patient functional outcomes and quality-of-life scores, reoperation and mortality. Randomisation will be blocked, with block sizes known only to the methods centre responsible for randomisation, and stratified by location of tumour and study centre. Patients, care givers and a Central Adjudication Committee will be blinded to treatment allocation. The analysis to compare groups will be performed using Cox regression and log-rank tests to compare survival functions at α=0.05.
Ethics and dissemination This study has ethics approval from the McMaster University/Hamilton Health Sciences Research Ethics Board (REB# 12-009). Successful completion will significantly impact on clinical practice and enhance patients’ lives. More broadly, this trial will develop a network of collaboration from which further high-quality trials in Orthopaedic Oncology will follow.
This is an open-access article distributed under the terms of the Creative Commons Attribution Non-commercial License, which permits use, distribution, and reproduction in any medium, provided the original work is properly cited, the use is non commercial and is otherwise in compliance with the license. See: http://creativecommons.org/licenses/by-nc/2.0/ and http://creativecommons.org/licenses/by-nc/2.0/legalcode.
Statistics from Altmetric.com
Article summary
Article focus
-
Prophylactic antibiotic regimens in tumour surgery (PARITY) is a multicentre, blinded, randomised controlled trial, using a parallel two-arm design to investigate whether long-duration (5 days) postoperative prophylactic antibiotics will decrease the rate of infection compared to short duration (24 h) among patients undergoing surgical excision and endoprosthetic reconstruction of lower-extremity primary bone tumours.
Key messages
-
The immediate goal of PARITY is to provide high-quality evidence that can be used in the development of clinical guidelines for antibiotic prophylaxis following lower-extremity tumour excision and endoprosthetic reconstruction.
-
Whereas sarcomas of the long bones are very rare tumours, multicentre international collaboration on a large scale is necessary to adequately power any high-quality trials in this field.
-
PARITY will mark the first such undertaking, and the rigorous design, organisation and execution of this trial will set a high standard.
Strengths and limitations of this study
-
PARITY will establish a successful network of collaboration from which further high-quality trials in Orthopaedic Oncology will follow.
-
The rationale supporting the study design includes demonstrated clinical uncertainly, lack of high-quality evidence and documented strong investigator support.
-
The methodology is supported by tremendous expertise and experience in running large international surgical trials of the Methods Center at the McMaster Center for Evidence-Based Orthopaedics.
-
This is a protocol paper; this trial is underway, but has not been completed.
Background
Magnitude of the problem
Sarcomas, or malignancies of connective tissue, are a rare form of cancer. These tumours may arise in the long bones of the extremities, and when doing so they often affect adolescents and young adults. Long-bone sarcomas were historically managed with amputations, but the current standard is limb salvage surgery. Limb salvage involves wide tumour resection followed by functional reconstruction. With the aid of modern imaging techniques and chemotherapeutic regimens, limb salvage is possible in 95% of patients.
The most common type of functional reconstruction involves the use of tumour endoprostheses. Tumour endoprostheses are modular metallic and polyethylene implants that replace surgically resected bones and joints. Due to the complexity and length of these procedures, as well as the immunocompromised nature of patients treated with chemotherapy, the risk for deep postoperative infection is high and the outcomes can be devastating.1 ,2 Deep infections require staged endoprosthetic revision surgery and long-term intravenous antibiotic therapy.3 Even following this management, subsequent repeat infection and ultimate amputation are not uncommon.1 ,4 ,5 Patients’ function and quality of life are dramatically impacted, as are healthcare costs.6
Published guidelines for postoperative antibiotic prophylaxis following many standard elective surgical procedures dictate that prophylactic antibiotics be discontinued after 24 h.7 However, the most effective prophylactic antibiotic regimen to prevent deep postoperative infection following surgical excision and endoprosthetic reconstruction of lower-extremity bone tumours remains unknown. Current clinical practice is highly varied, particularly with respect to antibiotic duration. Strategies to optimise the prevention of these infections while mitigating healthcare costs are needed.
Best evidence for infection rates
We performed a systematic review to determine reported infection rate outcomes following the treatment of primary long bone tumours (malignant and benign aggressive) by surgical excision and endoprosthetic reconstruction. A literature search of Medline, EMBASE and the Cochrane database was conducted, and the proceedings of past American Society for Clinical Oncology Annual Meetings were also searched. The search was limited to articles published in English, and no restrictions were placed on dates of publication.
This search generated 3889 titles. In order to minimise bias and ensure that studies were not overlooked, all titles and abstracts were screened by two independent reviewers. Those papers reporting outcomes of endoprosthetic reconstruction in the treatment of malignant or benign aggressive long bone tumours were selected for review. Studies reporting on the use of allografts or allograft-prosthesis composites were excluded. Studies investigating soft-tissue sarcomas, metastatic lesions, recurrent lesions or lesions that had received prior surgical treatment were excluded. The reported infection rates were extracted from the remaining papers and compared. Both reviewers performed data extraction and assessment of data quality independently, and differences were reconciled by mutual agreement or an independent third party.
Of the 3889 titles, there were 48 eligible studies (table 1). The deep-infection rates ranged from 0% to 22.2%, with a weighted mean of 9.5% (95% CI 8.1% to 11.0%). Duration of antibiotic prophylaxis was reported inconsistently, but ranged from ‘intraoperative dosing only’ to ‘greater than 72 h’.
Deep infection rates reported by systematic review
Complications of antibiotic overuse
Antibiotic resistance is an issue of steadily increasing clinical importance. Our systematic review demonstrated that the most common reported pathogen to infect endoprosthetic reconstructions after surgical excision of long-bone tumours is Staphylococcus aureus. Although methicillin-sensitive S aureus remains overwhelmingly susceptible to Ancef (cefazolin),51 the prevelance of methicillin-resistant S aureus (MRSA) is rising. In Canada, the incidence of MRSA as a proportion of all S aureus has increased from 1% in 1995 to 27% in 2008.51 Zhanel et al51 found that 68.8% of all MRSA isolates were healthcare-associated strains [HA-MRSA], while 27% were community-associated [CA-MRSA]). In 2009, all HA-MRSA and CA-MRSA isolates were susceptible to vancomycin, with varying sensitivities to other agents.51
Two main factors in the development of antibiotic resistance are antibiotic misuse and overuse.52 Antibiotic misuse is the selection of antimicrobial agents with inappropriately broad spectrums of efficacy, and antibiotic overuse is an inappropriately excessive frequency or duration of antibiotic prescription. Whereas increasing antibiotic resistance has the potential to significantly impair management of patients with infected endoprostheses, an evidence-based approach to antibiotic use is critical.
Other important complications of antibiotic overuse include the development of Clostridium difficile-associated colitis and life-threatening toxic megacolon, opportunistic fungal infections, indwelling-catheter related sepsis and seizures.53–57
Lack of consensus in antibiotic regimens and global interest in randomised controlled trial
We conducted a survey addressing the practices of Orthopaedic Oncologists registered with the Musculoskeletal Tumor Society (MSTS) and the Canadian Orthopaedic Oncology Society.58 From this survey, we concluded that there are currently no guidelines for the prescription of prophylactic antibiotics in musculoskeletal tumour surgery, and that current opinion and practice are highly varied. Of the 97 surgeons who received the questionnaire, 72 responded (75% response rate (95% CI 65.5% to 82.5%)). Almost all respondents agreed that prophylactic antibiotic regimens were important in reducing the risk of postoperative deep infection, but there was considerable variety in antibiotic choice and duration. Seventy-three per cent (95% CI 61% to 82%) of respondents reported prescribing only a first generation cephalosporin, while 11% reported prescribing a first-generation cephalosporin in combination with an aminoglycoside and/or vancomycin. Thirty-six per cent (95% CI 25% to 48%) discontinue antibiotics after 24 h, compared with 41% (95% CI 30% to 53%) who continue antibiotics until the suction drain is removed.
When asked if they would change their practice if a large randomised controlled trial (RCT) showed clear benefit for an antibiotic regimen different from their own current practice, 90% (95% CI 81% to 95%) of respondents reported they would. Further, 87% (95% CI 77% to 93%) expressed an interest to participate in such a trial.
Summary: rationale for a definitive RCT
Deep infections following surgical excision and endoprosthetic reconstruction of lower-extremity bone tumours are devastating complications. In combination with the existing literature, our earlier work has demonstrated: (1) high infection rate outcomes following the treatment of primary long bone tumours by surgical excision and endoprosthetic reconstruction; (2) a lack of high-level RCT evidence to guide the prescription of prophylactic antibiotic regimens; (3) highly variable opinion and practice regarding prophylactic antibiotic regimens among Orthopaedic Oncologists and (4) extensive investigator support for a definitive large RCT.59 These findings provide a strong rationale for undertaking a definitive RCT. The direct potential clinical implications of this work include both fewer endoprosthetic infections and fewer antibiotic-related complications.
Study design
Overview of study design
Prophylactic antibiotic regimens in tumour surgery (PARITY) is a multicentre, blinded, RCT, using a parallel two-arm design to investigate whether long duration (5 days) postoperative prophylactic antibiotics will decrease the rate of infection compared with short duration (24 h) among patients undergoing surgical excision and endoprosthetic reconstruction of lower-extremity primary bone tumours. Randomisation will be stratified by study centre and tumour location (femur vs tibia). Patient enrolment will occur over approximately 1 year and enrolled patients will be followed for 1-year postoperatively. Infection rates will be assessed within 12 months after initial surgery across both study arms. Patient function and quality of life will be assessed preoperatively and at 3-month, 6-month and 1-year follow-up visits. Trial conduct procedure is shown in figure 1. This trial is registered [NCT01479283] and has received ethics approval from the McMaster University/Hamilton Health Sciences Research Ethics Board (REB# 12-009).
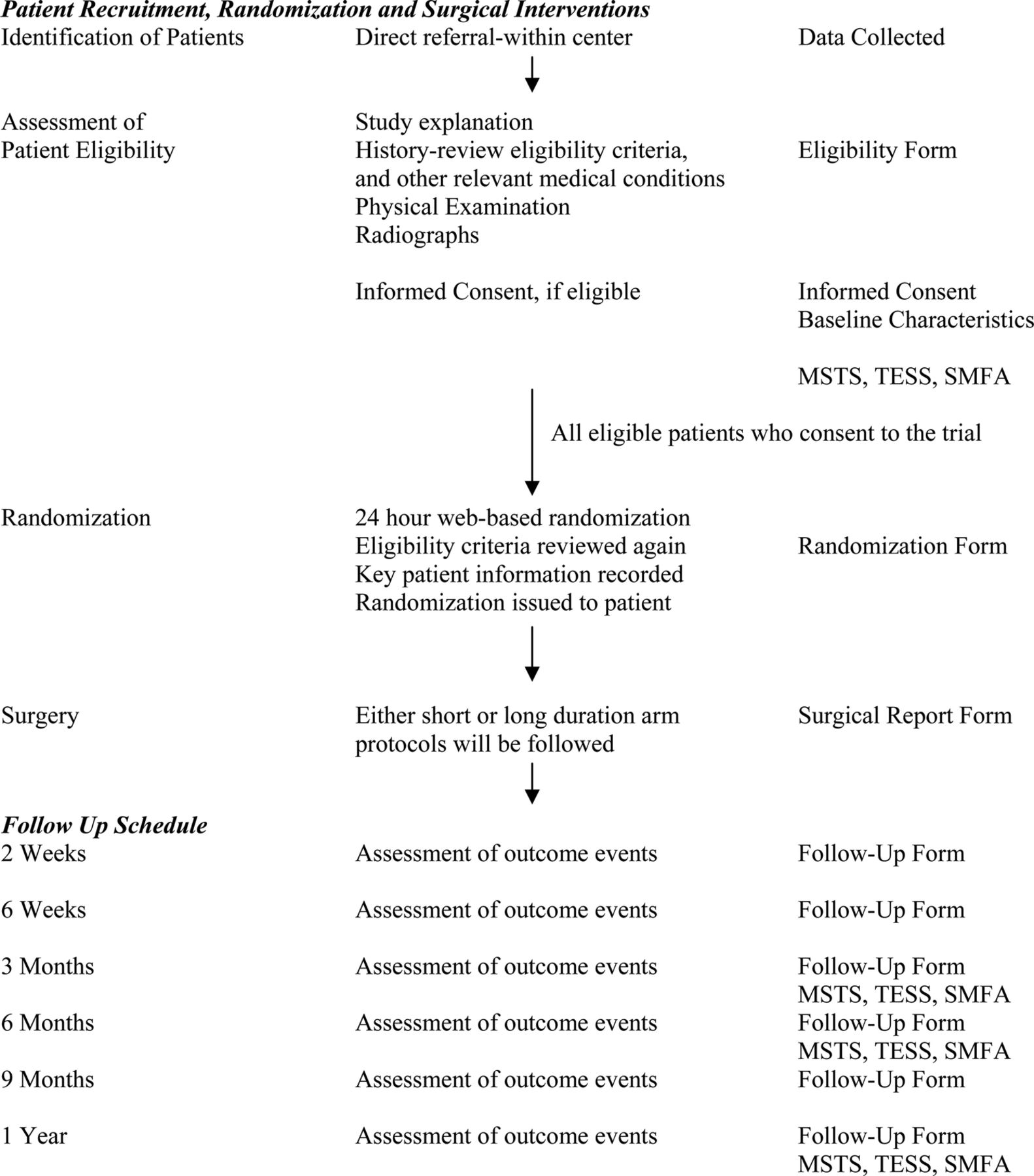
Trial Conduct Procedure. *Follow-Up Forms include adverse events (AE)s, serious adverse events (SAE)s, infections, reoperations, protocol deviations and wound healing problems and other appropriate forms.
Primary research question
In patients with a diagnosis of a primary malignant or benign aggressive bone tumour of the lower extremity, do long-duration prophylactic antibiotics following surgical excision and endoprosthetic reconstruction of lower-extremity bone tumours, in comparison with short-duration prophylactic antibiotics, lead to decreased rates of postoperative deep infections over 12 months?
Secondary research questions
In patients with a diagnosis of a primary malignant or benign aggressive bone tumour of the lower extremity, do long-duration prophylactic antibiotics following surgical excision and endoprosthetic reconstruction of lower-extremity bone tumours, in comparison with short-duration prophylactic antibiotics, lead to:
-
Any differences in frequency or type of antibiotic-related adverse over 12 months?
-
Any differences in patient functional outcome and quality-of-life scores over 12 months?
-
Any differences in occurrence of adverse events, serious adverse events, infections other than deep-surgical site infections, complications of wound healing, tumour recurrence or metastases, reoperation or mortality between long and short-duration prophylactic antibiotics over 12 months?
Hypothesis
As a primary outcome, there will be significantly fewer deep postoperative infections and no significant increase in frequency or severity of antibiotic-related complications associated with long duration in comparison with short-duration prophylactic antibiotics. As secondary outcomes, we expect no differences in patient functional outcome scores, quality-of-life scores, adverse events, serious adverse events, infections other than deep-surgical site infections, complications of wound healing, tumour recurrence or metastases, reoperation or mortality between long and short-duration prophylactic antibiotics. This study is powered to address the primary outcome and will also be powered to identify minimally important differences in functional outcomes.
Eligibility criteria
Inclusion criteria
Men and women 15 years of age or older who meet all the following criteria will be included in the study:
-
Diagnosis of a primary malignant or benign aggressive bone tumour of the lower extremity;
-
Planned treatment of surgical excision and endoprosthetic reconstruction;
-
Provision of informed consent.
Exclusion criteria
Patients who meet any one or more of the following criteria will be excluded from the study:
-
Known skin colonisation with MRSA, or vancomycin-resistant Enterococcus at the time of enrolment;
-
Allergy to Ancef (cefazolin) or penicillin, consisting of anaphylaxis or angioedema;
-
Prior surgery within the planned operative field, excluding a biopsy;
-
Prior infection within the planned operative field.
Recruitment and screening
Each clinical site will have a locally responsible investigator that will oversee local administration of the trial. The treating physicians, investigators, study coordinators and/or their delegates at each site will identify potentially eligible patients upon presentation with a lower-extremity bone tumour requiring surgical excision and endoprosthetic reconstruction. All potentially eligible patients will be screened and documented as: (1) eligible and included, (2) eligible and missed or (3) excluded. The study coordinator or designee will obtain informed consent for participation in the study using local IRB/REB approved Informed Consent forms. Consent will be obtained at the final preoperative visit 1–2 weeks prior to the anticipated date of the surgery and at the same time that consent is obtained for the procedure. Baseline characteristics forms and preoperative functional outcome and quality-of-life questionnaires will be completed at the time of consent.
Allocation of patients to study groups
Patients will be randomised to either short-duration or long-duration prophylactic antibiotics only after patient eligibility is established and patient consent is obtained. Actual randomisation will occur during surgery, prior to case completion and will be carried out by the pharmacy technician using an internet-based randomisation system that ensures concealment. The pharmacy will be notified of upcoming study participants both at the time of consent and on the morning of surgery. Randomisation will be blocked, with block sizes known only to the methods centre responsible for randomisation. Patients will be the unit of randomisation. Randomisation will be stratified for: (1) location of tumour (femur vs tibia) and (2) study centre.
Study interventions
Surgical excision and endoprosthetic reconstruction will be performed according to the standard practice of the participating surgeons. This typically involves a wide extensile surgical exposure, isolation and protection of major neurovascular structures, resection of the segment of bone affected by tumour with a 2–3 cm bone margin, and a soft-tissue margin dictated by the amount of available tissue that can be safely resected from both oncological and functional standpoints. Endoprostheses may be implanted with either press-fit or cemented techniques. Soft-tissue reconstruction may or not may not require tissue transfer based on the original extent of the tumour and required soft-tissue excision to establish wide oncological margins.
Tumor Characteristics Forms, Surgical Report Forms, Peri-operative Forms and Antibiotics Logs will be completed at the time of surgery. Patients will be assessed for adverse events and protocol deviations in the perioperative period. All patients will receive 2 g of intravenous Ancef preoperatively and every 3–4 h intraoperatively.
Short-duration antibiotics
Patients randomised to the short-duration regimen will receive 2 g of intravenous Ancef postoperatively every 8 h for 24 h, followed by intravenous ‘sham’ antibiotics (normal saline) for an additional 4 days.
Long-duration antibiotics
Patients randomised to the long-duration regimen will receive 2 g of intravenous Ancef postoperatively every 8 h over a 5-day period (maximum), or until hospital discharge if acute care stay is less than 5 days.
Blinding
All antibiotic bags will be identically shrouded. No other antibiotics will be administered for infection prophylaxis. Patients, surgeons, nurses, research personnel, data analysts and the Central Adjudication Committee (CAC) will be blinded to the antibiotic duration. The pharmacy technician preparing and shrouding the solutions will not be blinded.
Outcome measures
Primary cutcome
The primary study outcome will be rates of deep postoperative infections in each of the study arms. The CDC definition of a deep surgical site infection (below) will be employed (http://www.cdc.gov/nhsn/PDFs/pscManual/9pscSSIcurrent.pdf). Patients will be monitored regularly for this outcome by their treating physicians at 2 and 6 weeks, and 3, 6 and 9 months, and 1-year postoperatively. If deep infection does occur, the causative organism will be determined and documented.
The CDC criteria we will use define infection as follows: The infection occurs within 30 days after the operative procedure or within 1 year if an implant is in place and the infection appears to be related to the operative procedure. The infection may involve any part of the body, excluding the skin incision, fascia or muscle layers that is opened or manipulated during the operative procedure. The patient must have at least 1 of the following:
-
Purulent drainage from a drain that is placed through a stab wound into the organ/space;
-
Organisms isolated from an aseptically obtained culture of fluid or tissue in the organ/space;
-
An abscess or other evidence of infection involving the organ/space that is found on direct examination, during reoperation or by histopathological or radiological examination;
-
Diagnosis of an organ/space SSI by a surgeon or attending physician.
Secondary outcomes
The secondary study outcomes include type and frequency of antibiotic-related adverse events, patient functional outcome scores, and patient quality-of-life scores. We will also evaluate for occurrence of adverse events, serious adverse events, infections other than deep-surgical site infections, complications of wound healing, incidence of tumour recurrence or metastasis, reoperation and mortality. As noted in figure 1, the MSTS functional score (clinician administered), the Toronto Extremity Salvage Score (TESS) (patient administered) and the Short Musculoskeletal Functional Assessment (SMFA) questionnaires will be used to assess functional outcomes prior to surgery, and at the 3-month, 6-month and 1-year follow-up visits. The MSTS and TESS instruments are based on validated, well-accepted functional scoring systems in Orthopaedic Oncology publications.59–61 The Short Musculoskeletal Function Assessment questionnaire is a reliable, responsive, validated instrument that evaluates general health status in patients with musculoskeletal disorders.62 ,63
Adjudication of outcomes
A blinded CAC will adjudicate all occurrences of deep-surgical site infection. The committee will also adjudicate all occurrences of an antibiotic-related complication, occurrence of an infection other than a deep-surgical site infection, occurrence of an adverse event or serious adverse event, complications of wound healing, recurrence, metastasis, reoperation, mortality or doubt of eligibility. The CAC will be comprised of three Orthopaedic Surgeons and one Infectious Diseases specialist and the Global Adjudicator web-based platform will be used.64
Patient follow-up
Patients will be assessed at the time of regular follow-up by their treating physician at 2 and 6 weeks, and 3, 6 and 9 months and 1-year postoperatively. Patients will be assessed for infections (surgical site and other), antibiotic-related complications, adverse events, serious adverse events, complications of wound healing, oncologic outcomes such as local recurrence and metastasis, reoperation, mortality and protocol deviations. Accompanying forms will be completed as scheduled on figure 1. A Missed Follow-Up Form will be completed if a patient misses a follow-up visit. An Early Withdrawal Form will be completed only if a patient withdraws their consent.
Maximisation of follow-up
Given the malignant potential and patient concern associated with long bone sarcomas, we anticipate only minimal losses to follow-up in our Orthopaedic Oncology population. Nonetheless, the following procedures will be implemented to minimise losses (1) exclusion of individuals who are likely to present difficulty with follow-up; (2) at the baseline assessment, each patient shall provide their own address and phone number, the name and address of their primary care physician, and the name, address and phone number of three people at different addresses with whom the patient did not live who were likely to be aware of the patient's whereabouts; (3) patients will receive reminders for upcoming clinic visits from the study coordinators; (4) follow-up schedules will coincide with normal postoperative clinic visits; (5) if a patient refuses to return for a follow-up assessment, his/her status with regard to the primary and secondary outcomes will be assessed as much as possible by telephone contact with the patient, alternate contact or their family physician.65
Minimisation of crossovers
Crossovers are extremely unlikely between the short-duration and long-duration antibiotic regimens given that patients will be blinded and acute infections are unlikely to be recognised in the first 5 days after surgery. Any patients who do crossover will be analysed in the group to which they were originally allocated, maintaining an ‘intention to treat’ analysis. Standardisation of antibiotic regimens will limit cointervention, and concurrent use of drugs that affect antibiotic metabolism will be documented. Any procedures that patients undergo while in hospital and any other infections that occur (urinary tract, Port or PICC line) will also be documented.
Sample size consideration
The sample size calculation for the definitive trial is based upon a between-group comparison for the primary outcome of deep infection following long-duration (experimental) or short-duration (control) antibiotics. Based on our survey of Orthopaedic Oncologists, we will set a threshold of an absolute difference of 5% to define superiority.58 As identified by our systematic review, infection rates after surgical excision and endoprosthetic reconstruction of bone tumours range from 0% to 22% with a weighted mean of 9.5% (95% CI 8.1% to 11.0%), hence variation in the rate of infection in the control group from 7% to 15%. Using a baseline estimate of 10% for infection and a presumed 50% or greater reduction in the risk of deep infection, with an % of 0.05 and β of 0.20, 435 patients per study arm will power our study at over 80% (table 2).66 ,67
Power table for sample size calculation
After adjustments for potential losses to follow-up, errors in eligibility, and study drop-outs (approximately 5% total), the total sample requirement [n_adjusted=n/(1−0.05) where n is the calculated sample size] will be 920 patients (460 patients per arm).
Data analysis plan
The results of patient demographics and baseline characteristics will be summarised using descriptive summary measures: expressed as mean (SD) or median (minimum–maximum) for continuous variables and number (per cent) for categorical variables. The analysis and reporting of the results of the clinical outcomes will follow the CONSORT guidelines (www.consort-statement.org). Infection rates and secondary outcomes will undergo an intention-to-treat analysis. We will use multiple-imputation to handle missing data.68 The infection rates in each arm will be compared using the Cox-proportional hazards model. We will assess the proportional hazards assumption of the Cox model. We will use the log-rank test to assess difference between survival curves of the two groups. Estimates of treatment effects will be reported as HR with corresponding 95% CI and associated p values. p Values will be reported to three decimal places with values less than 0.001 reported as <0.001. All statistical tests will be performed using two-sided tests at the 0.05 level of significance. We will conduct a multiple Cox-regression model to determine if total operative time, tumour location, chemotherapy regimen, diabetes, smoking or other factors are related to infection rates. We will also conduct subgroup analyses for infection rates within each type of tumour (Ewing's, Osteosarcoma, Chondrosarcoma, Giant Cell Tumor) and tumour location (proximal femur, distal femur and proximal tibia). Our a priori hypothesis, based on retrospective data, is that reconstructions of the proximal tibia and tumours that have been treated with neoadjuvant or adjuvant chemotherapy (Ewing's Sarcoma and Osteosarcoma) will be at higher risk for deep infection based on difficulty with soft-tissue coverage in the tibia and the immunocompromised nature of patients on chemotherapy. If these subgroup analyses are underpowered, the subgroup data will be used to generate further hypotheses that can be tested in future trials.69 ,70 All analyses will be performed using SAS V.9.2 (Cary, North Carolina, USA).
Frequency of analyses
There will be only one analysis at the end of the trial. However, the Data Monitoring Committee (DMC) will meet biannually to review the safety data and monitor the progress of the trial.
Data monitoring committee
The DMC will be established at the onset of the trial to monitor the trial and review the study biannual progress report.69 ,70 The Committee members will be independent of the trial, free of conflicts with any of the investigative team and will consist of Orthopaedic Surgeons. The terms of reference and functions are derived from the principles established by the Data and Safety Monitoring Boards: Lessons, Ethics, Statistics Study Group charter.
Methods and coordinating centre
This study will be coordinated by the Center for Evidence-Based Orthopaedics (CEO) at McMaster University in Hamilton, Ontario (figure 2). The CEO provides faculty members within the Division of Orthopaedic Surgery with expertise, infrastructure and support with all aspects of clinical research project management. This includes assistance with project management, data management, biostatistics, report preparation and writing, and manuscript submission and tracking. For the PARITY trial, the Program Manager at the CEO will be responsible for overseeing the overall coordination of the study and helping to ensure that timelines are met and that data quality is maintained. The Research Coordinator at CEO will be responsible for the day-to-day coordination of this study, including organisation of the committees, development of the case report forms, training of the clinical sites, communicating with the clinical sites, data validation and preparation of the study reports. The Data Manager at the CEO will be responsible for programming the participant online randomisation system and the state-of-the-art data management system with electronic data capture capabilities. The Statistician will be responsible for conducting the analyses of the trial data.

{kind=link}
{kind=link}
Trial structure and organization.
Potential impact of study
This study's major strengths are numerous: The rationale supporting the study design includes demonstrated clinical uncertainly, lack of high-quality evidence and documented strong investigator support. The high response rate in our earlier survey underscores the cohesive nature of the Orthopaedic Oncology community, and the Methods Center at the McMaster Center for Evidence-Based Orthopaedics possesses tremendous expertise and experience in running large international surgical trials.
The immediate goal of PARITY is to provide high-quality evidence that can be used in the development of clinical guidelines for antibiotic prophylaxis following lower-extremity tumour excision and endoprosthetic reconstruction. More broadly, PARITY will establish a successful network of collaboration from which further high-quality trials in Orthopaedic Oncology will follow. Whereas sarcomas of the long bones are very rare tumours, multicentre international collaboration on a large scale is necessary in order to adequately power any high-quality trials in this field. PARITY will mark the first such undertaking, and the rigorous design, organisation, and execution of this trial will set a high standard. In so doing, PARITY will lead the development of Evidence-Based clinical guidelines and impact on an entire field.
References
Footnotes
-
Collaborators PARITY investigators: The following persons are involved in PARITY—Co-Principle Investigators: Michelle Ghert, Benjamin Deheshi. Steering Committee: Michelle Ghert (co-Chair), Mohit Bhandari (co-Chair), Gordon Guyatt, Benjamin Deheshi, Ginger Holt, Jay Wunder, Peter Ferguson, Lehana Thabane, Tim O'Shea, Lor Randall. Central Adjudication Committee: Michelle Ghert, Ben Deheshi, Lor Randall, Tim O'Shea. Methods and Coordinating Center: Mohit Bhandari, Michelle Ghert, Benjamin Deheshi, Nathan Evaniew, Antonella Racano, Marilyn Swinton, Sheila Sprague, Lehana Thabane, Lisa Buckingham. Data Safety Monitoring Board: Peter Rose, Brian Brigman, Vikram Venkateswaran. Participating centers—Juravinski Hospital and Cancer Center/McMaster University, Hamilton, Ontario: Michelle Ghert, Ben Deheshi; Mount Sinai Hospital/University of Toronto, Toronto, Ontario: Peter Ferguson, Jay Wunder; McGill University Health Center/McGill University, Montreal, Quebec: Robert Turcotte; Ottawa Hospital/University of Ottawa, Ottawa, Ontario: Joel Werier; Vancouver General Hospital/University of British Columbia, Vancouver, British Columbia: Paul Clarkson; Vanderbilt Medical Center/Vanderbilt University School of Medicine, Nashville, Tennessee: Ginger Holt; SUNY Upstate University Hospital/SUNY Upstate, East Syracuse, New York: Timothy Damron; University Hospital/University of Medicine & Dentistry of New Jersey, Newark, New Jersey: Joseph Benevenia; Beth Israel Deaconess Medical Center and Children's Hospital Boston/Harvard Medical School, Boston, Massachusetts: Megan Anderson and Mark Gebhardt; Huntsman Cancer Institute/University of Utah, Salt Lake City, Utah: R. Lor Randall; University of Montreal, Montreal, Quebec: Marc Isler, Sophie Mottard; Memorial Sloan-Kettering Cancer Center, New York, New York: John Healey.
-
Contributors The following authors made substantial contributions to conception and design, acquisition of data, analysis and interpretation of data; were involved in drafting the article or revising it critically for important intellectual content; and gave final approval of the version to be published: MG, GH, RLR, BD, PF, JW, RT, JW, PC, TD, JB, MA, MG, MI, SM, JH, NE, AR, SS, MS, DB, LT, GG, MB.
-
Funding This work was supported research grants by the Musculoskeletal Tumor Society and the Orthopaedic Research and Educational Foundation, and the Physicians Services Incorporated Foundation. These funders had no role and did not influence in any way the study design; collection, management, analysis, and interpretation of data; writing of the report; or the decision to submit the report for publication, including who will have ultimate authority over each of these activities.
-
Competing interests Paul Clarkson has received grant funding from Stryker Canada; Timothy Damron has received royalties from Lippincott Williams and Wilkins, and has received grant funding from Wright Medical, Zetrox, OrthoVita, Stryker and the Musculoskeletal Tumor Society; Peter Ferguson has received consultancy reimbursement from Amgen Canada; Mohit Bhandari has received consultancy reimbursement from Smith and Nephew, Stryker, Amgen, Zimmer, Moximed and Bioventus and has received or has pending grant funding from Smith and Nephew, DePuy, Eli Lily and Bioventus; Dianne Bryant has received consultancy reimbursement from the University of Western Ontario and the Fowler Kennedy Sport Medicine Clinic and has received payment for the development of educational presentations by Health Canada.
-
Ethics approval This study has ethics approval from the McMaster University/Hamilton Health Sciences Research Ethics Board (REB# 12-009).
-
Provenance and peer review Not commissioned; externally peer reviewed.
-
Data sharing statement All data from this work will be maintained in security and confidentiality at the Methods Centre at McMaster University. Access to additional unpublished data will be reviewed on a case-by-case basis and will accord with the guidelines of our local institutional research ethics board.