Article Text

Abstract
Background Large gaps exist in the implementation of guideline recommendations for cardiovascular disease (CVD) risk management. Electronic decision support (EDS) systems are promising interventions to close these gaps but few have undergone clinical trial evaluation in Australia. We have developed HealthTracker, a multifaceted EDS and quality improvement intervention to improve the management of CVD risk.
Methods/design It is hypothesised that the use of HealthTracker over a 12-month period will result in: (1) an increased proportion of patients receiving guideline-indicated measurements of CVD risk factors and (2) an increased proportion of patients at high risk will receive guideline-indicated prescriptions for lowering their CVD risk. Sixty health services (40 general practices and 20 Aboriginal Community Controlled Health Services (ACCHSs) will be randomised in a 1:1 allocation to receive either the intervention package or continue with usual care, stratified by service type, size and participation in existing quality improvement initiatives. The intervention consists of point-of-care decision support; a risk communication interface; a clinical audit tool to assess performance on CVD-related indicators; a quality improvement component comprising peer-ranked data feedback and support to develop strategies to improve performance. The control arm will continue with usual care without access to these intervention components. Quantitative data will be derived from cross-sectional samples at baseline and end of study via automated data extraction. Detailed process and economic evaluations will also be conducted.
Ethics and dissemination The general practice component of the study is approved by the University of Sydney Human Research Ethics Committee (HREC) and the ACCHS component is approved by the Aboriginal Health and Medical Research Council HREC. Formal agreements with each of the participating sites have been signed. In addition to the usual scientific forums, results will be disseminated via newsletters, study websites, face-to-face feedback forums and workshops.
Trial registration The trial is registered with the Australian Clinical Trials Registry ACTRN 12611000478910.
- Primary Care
- Cardiology
This is an open-access article distributed under the terms of the Creative Commons Attribution Non-commercial License, which permits use, distribution, and reproduction in any medium, provided the original work is properly cited, the use is non commercial and is otherwise in compliance with the license. See: http://creativecommons.org/licenses/by-nc/2.0/ and http://creativecommons.org/licenses/by-nc/2.0/legalcode.
Statistics from Altmetric.com
Article summary
Article focus
-
The development of a multifaceted decision support tool and quality improvement (QI) intervention.
-
The methods to test the effectiveness of this intervention in improving guideline-recommended screening for cardiovascular risk and management for individuals identified at high risk.
Key messages
-
This study tests a novel intervention that incorporates point of care decision support, risk communication and resources for patients, health service audit tools and use of data for supporting QI initiatives.
-
In addition to assessing practitioner performance on indicators correlated with improved health outcomes, the study also includes detailed process and economic evaluations.
Strengths and limitations of this study
-
The strengths of the study are that it assesses an innovative complex intervention that is implemented in routine primary healthcare settings. It will provide rigorous evidence on process, clinical and economic outcomes and addresses an important issue facing health systems worldwide—namely scalable interventions that are able to achieve improvements in performance.
-
The main limitation is that it is conducted in one country, Australia, and thus its generalisability may be influenced by the prevailing health system context.
Background
Cardiovascular disease burden in Australia
Despite recent gains, cardiovascular disease (CVD) remains Australia's biggest killer accounting for 18% of the total disease burden and 11% of health system expenditure in Australia.1 Aboriginal and Torres Strait Islander peoples experience around five times greater CVD burden than other Australians.2 Current estimates project that by 2030 annual CVD expenditure will rise by around 100% to $16 billion.3 Primary care-based strategies that improve the uptake of best-practice recommendations could substantially reduce both the Indigenous and non-indigenous CVD burden and help improve health system efficiencies.
Evidence-practice gaps in CVD prevention
In addition to lifestyle modification, a number of drug therapies have been shown to be highly effective in preventing cardiovascular events, primarily through modification of blood pressure, lipids and platelet function.4–8 However, there is compelling evidence of the failure of current clinical practice to adequately implement such treatments, and to translate current knowledge into maximally improved health outcomes. Three recently completed cross-sectional studies of CVD risk management in Australian general practice and Aboriginal Community Controlled Health Service (ACCHS) settings9–11 demonstrated that 50% of routinely attending adults lacked sufficient recorded information to comprehensively evaluate vascular risk. For those identified at high vascular risk, only around 40% were prescribed guideline-indicated medicines. Similar findings have been noted in other Australian studies.12–15 These surveys have demonstrated failure to adequately implement the ‘absolue risk’ paradigm for CVD prevention. Numerous tools are now available to estimate an individual's 5-year or 10-year absolute risk of coronary heart disease and/or CVD.16–21 Despite their availability, only a minority of Australian general practitioners (GPs) use these risk assessment tools, and then primarily for patient education, rather than to guide management decisions.9 ,22 ,23 Australia's first absolute risk assessment guideline was released in 2009 by the National Vascular Disease Prevention Alliance (NVDPA)17 and in 2012 this was augmented by a single management guideline.24 Despite these guidelines now becoming available, there remain substantial challenges in effectively implementing their recommendations. We have found that CVD-risk assessment and treatment work best when negotiated as part of a shared decision-making approach, taking an average of 15 min even where only one guideline needs to be consulted.25
The role of electronic decision support in closing evidence practice gaps
Electronic decision support (EDS) systems are among the most promising interventions to improve uptake of guideline-based recommendations in clinical practice. In five systematic reviews on the effectiveness of EDS, around two-thirds of studies demonstrated improvement in practitioner performance.26–30 One systematic review identified four decision support system features associated with improved performance: incorporation in routine work flow, provision at the time and location of patient consultation, use of computer-based tools and provision of treatment recommendations rather than just assessments.28 Of 32 systems that incorporated all of these elements, significant improvements in performance were noted in 30. There are relatively few controlled evaluations of EDS systems that are integrated with electronic health records (EHRs) in the area of CVD.31–35 Effect sizes vary greatly depending on the variables studied and the type of EDS system. In one systematic review of on-screen point-of-care reminder systems the absolute improvements ranged from 1% to 24% for test ordering and from 3% to 28% for medication prescribing.27 In New Zealand, an EDS system that is fully integrated with the country's most popular primary care software has been successfully implemented.36 To date, we are unaware of an EDS system aimed at assisting comprehensive cardiovascular risk management based on Australian guidelines. Furthermore, we are not aware of any randomised evaluations of such systems in Australian primary care settings. Globally, few examples exist and the evidence base remains poor.
Intervention development
HealthTracker is a novel EDS system to facilitate guideline-based assessment and management of CVD risk. Outlined below are the key steps taken in the development of the intervention.
Algorithm development and validation
A single screening and management algorithm was developed based on a synthesis of recommendations from several primary care screening and management guidelines (table 1). The algorithm calculates a person's 5-year absolute CVD risk based on the Framingham risk equation and NVDPA recommendations 17 ,20 and provides management recommendations based on the guidelines listed in table 1. In 2008–2009, a β-version of HealthTracker was developed in a stand-alone software system and independently validated for accuracy and compliance with the prevailing guidelines.22 In 2011, the algorithm was extensively revised to incorporate recommendations from newly published guidelines. A similar validation process was then conducted consisting of three levels:
-
Level 1 was an iterative process where each of the calculations programmed in the algorithm were tested to ensure they were consistent with recommendations from the guidelines. This was conducted using deidentified data from 337 patients involved in the pilot. Programming modifications were made where necessary and all variables were retested to ensure they were programmed correctly.
-
Level 2 involved giving a plain language summary of the algorithm to a research fellow who had not been involved in the development of the algorithm. She independently programmed the algorithm into a statistical software package. Using data from 9077 patients from three representative cross-sectional general practice surveys,9–11 we then assessed whether the outputs from HealthTracker correlated with those generated from the independently programmed version. For 60 of the 63 output variables HealthTracker achieved perfect correlation with the independently programmed version. For the remaining three variables minor programming errors were identified and corrected.
-
Level 3 involved user acceptance testing and scrutiny of the algorithm by the study investigators, 20 health professionals working in both General Practice and ACCHSs and three national professional organisations—the NVDPA, the Royal Australian College of General Practitioners and the National Prescribing Service. Following this feedback, a number of minor algorithm and user interface changes were incorporated into the final version of the tool. The level 2 testing process was repeated following these changes and perfect correlation between HealthTracker and the independently programmed version was achieved for all variables.
Guidelines used in the HealthTracker algorithm
Integration of HealthTracker with the primary care electronic health record and quality improvement tools
HealthTracker interfaces with the two Australian clinical practice software systems most commonly used in general practice and ACCHS settings (Medical Director and Best Practice). There are four components to the system:
-
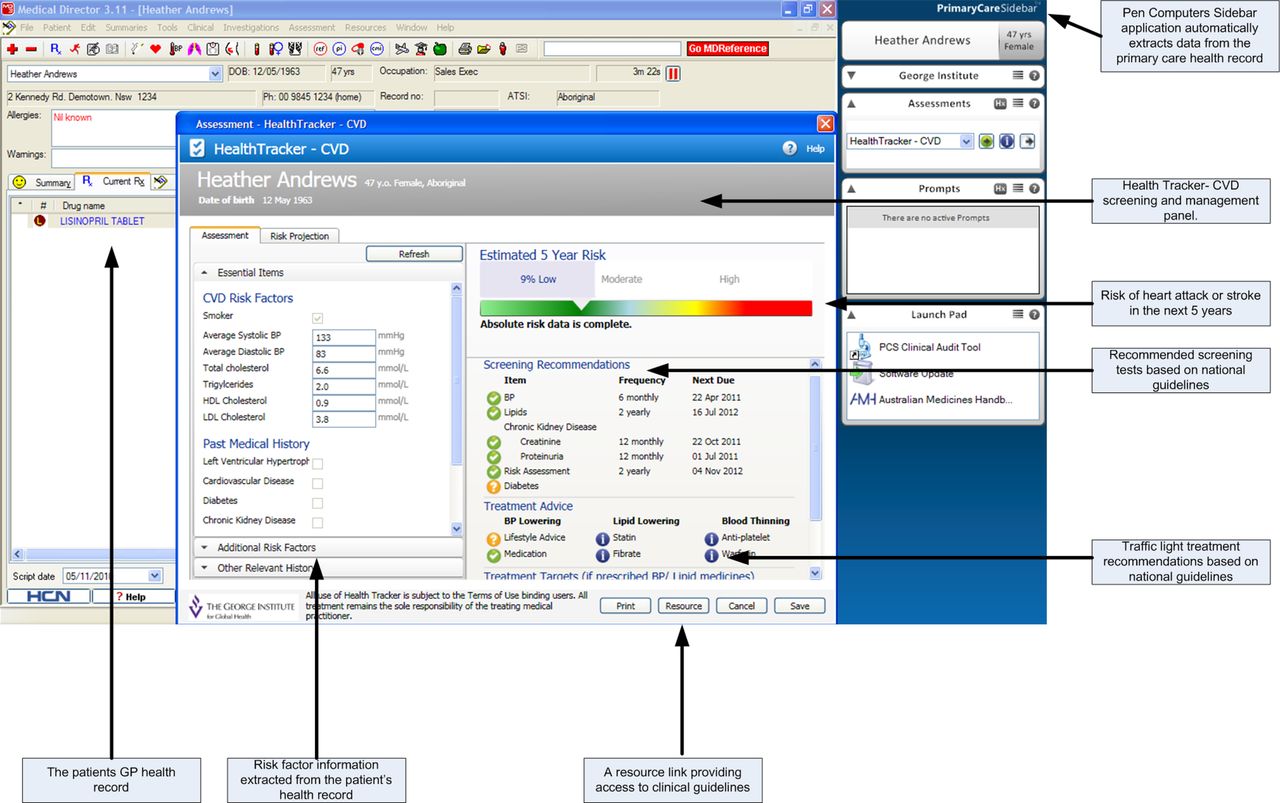
Point-of-care decision support: HealthTracker is built in the Pen Computer Systems PrimaryCareSidebar, third-party software that interacts with the primary EHR system. Figure 1 shows the HealthTracker user interface and its integration with the PrimaryCareSidebar and the EHR. A prompt function is used to encourage health professionals to conduct a cardiovascular assessment if guideline recommended. Where possible, the tool populates with information from the patient's record. If essential information required for the calculation of absolute risk is missing or out-of-date, a traffic light prompt alerts the health professional and updated information can be entered. If the patient is receiving suboptimal treatment then a traffic light recommendation is made to consider initiation of treatment or additional agents. Information about eligibility for the Australian Government Pharmaceutical Benefits Scheme subsidy is provided if lipid lowering medicines are recommended. All outputs are qualified by statements emphasising that the final decision to commence or change therapy should be made by the health professional based on all available information.
-
A patient-oriented risk communication interface: A key finding from the pilot evaluation was the role of the output in risk communication. GPs wanted to interactively alter current risk factors and perform ‘what if’ scenarios to demonstrate to patients the effects of current and altered risk over time. This functionality has been built into HealthTracker and uses the concept of ‘Heart Age’ to demonstrate to patients the discrepancy between current risk and an ideal risk based on well-controlled risk factor levels. Figure 2 shows an example of how a patient's heart age changes with the effect of smoking cessation.
-
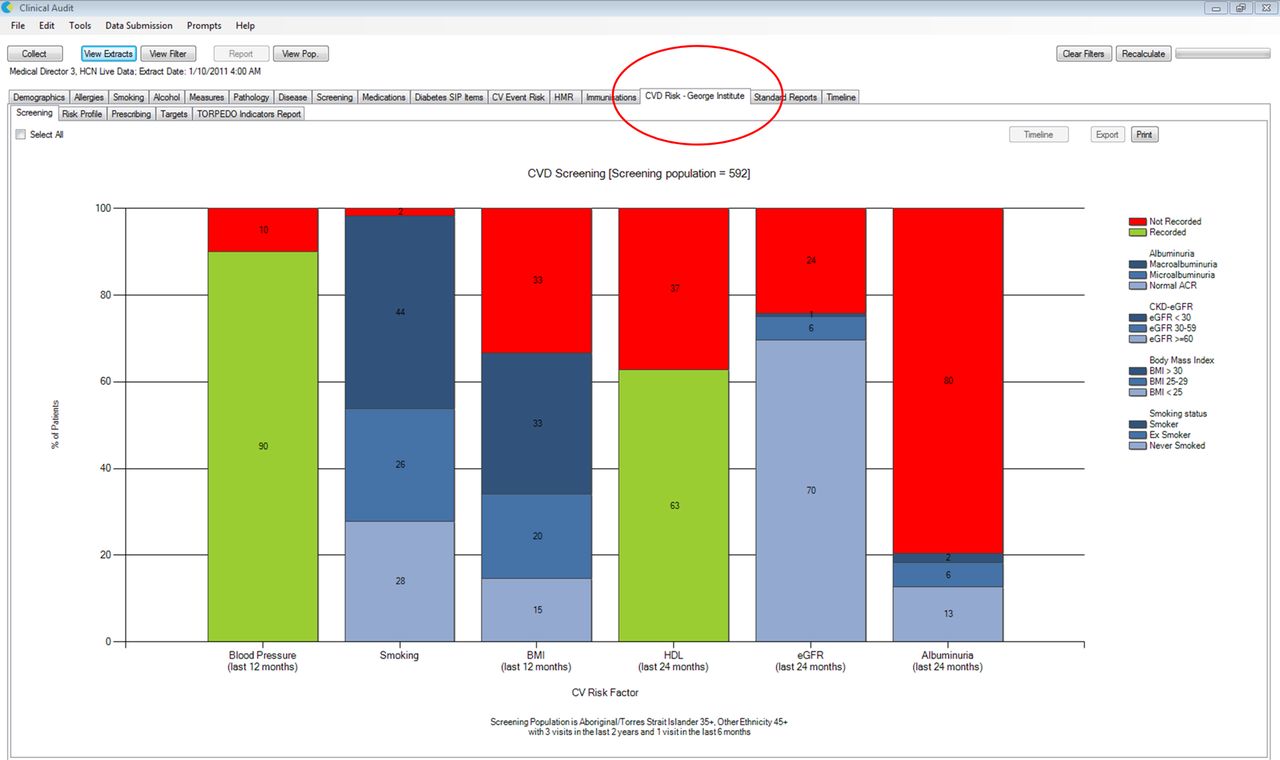
A data extraction tool: This provides health professionals with immediate feedback on their performance on screening and management of CVD risk for their entire patient population. Figure 3 shows an example of screening performance for a range of CVD risk factors. Practitioners can use this tool to identify specific patients in whom there may be a particular risk factor measurement missing or a potential prescribing gap. Customised point-of-care prompts can then be created. When a patient record is opened an alert is provided to notify the practitioner of the particular management issue and this can then be actioned.
-
A quality improvement (QI) component: This is aligned with the methods of the Improvement Foundation of Australia (IFA) Australian Primary Care Collaboratives (APCC) programme. Deidentified data extracts of clinical performance are securely exported to a web-based central repository managed by the IFA. This repository provides access to site-specific feedback reports on performance compared with other anonymised sites. Figure 4 shows an example of how this information is presented.

HealthTracker_user interface.

HealthTracker—cardiovascular disease-risk communication interface.
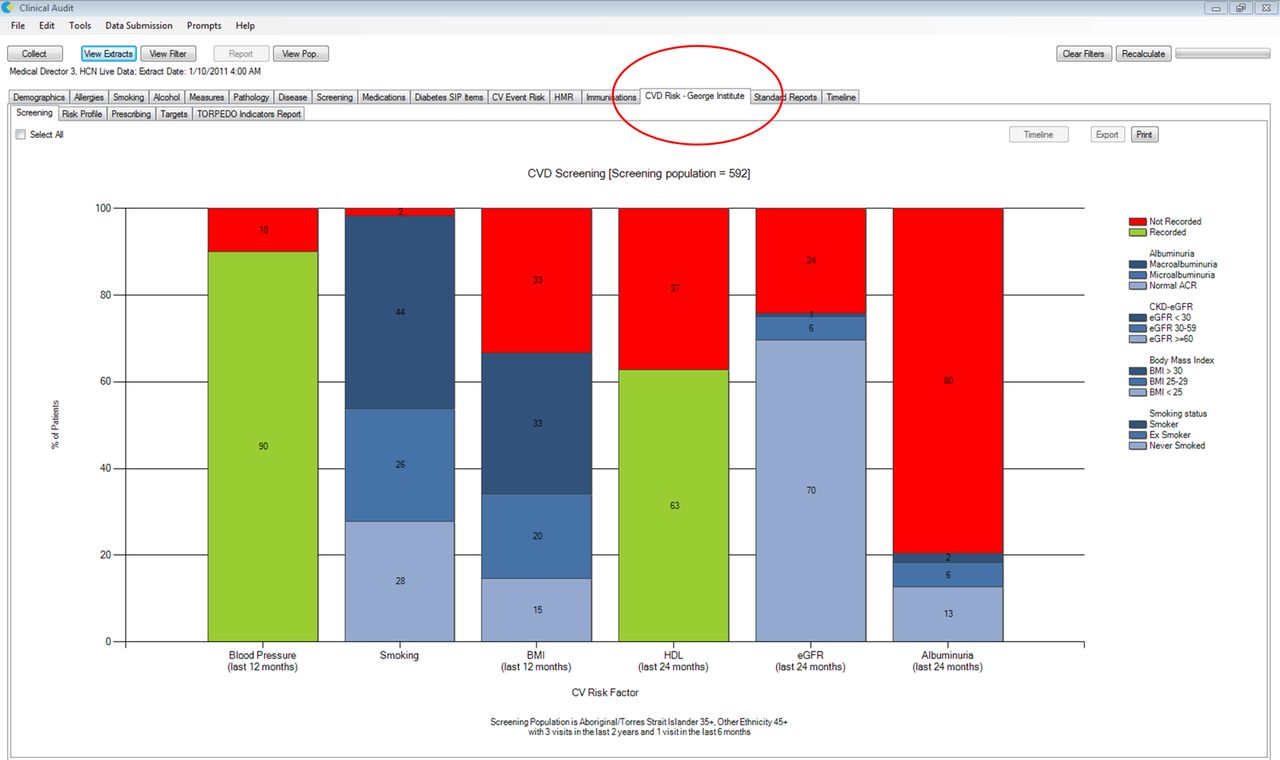
Sample output of performance in cardiovascular disease-risk factor screening.

Sample display from the quality improvement portal.
Study objectives
The TORPEDO study will test HealthTracker's performance in assisting health professionals and patients in making evidence-based management decisions to help prevent heart attack, stroke and related conditions.
Hypotheses
Using a cluster randomised, controlled trial design, two specific hypotheses will be tested. Compared with control practices, those practices randomised to receive HealthTracker will have:
-
An increased proportion of patients receiving appropriate (guideline-indicated) measurements of their CVD risk factors.
-
An increased proportion of patients at high risk receiving appropriate (guideline-indicated) prescriptions for the management of their CVD risk.
These aims will be augmented by formal economic and process evaluations to provide crucial information on large-scale implementation and sustainability.
Study design
HealthTracker will be evaluated using a cluster randomised, controlled trial design. At end of study, HealthTracker will be made available to both the intervention and control arms for a further 12 months free of any licence fees. The study schema including site and patient eligibility criteria are highlighted in figure 5.

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
TORPEDO study schema.
Eligibility criteria
Health service
-
Use of Medical Director or Best Practice for EHR management.
-
Exclusive use of these systems to record risk factor information, pathology test results and prescribe medications.
-
Agreement by all GPs and other designated staff to use HealthTracker.
Services that do not have a compliant software system will be excluded from participation. Services using ‘hybrid’ paper and electronic systems for recording risk factor information, pathology results and medication prescription will also not be eligible to participate.
Patients
-
Aboriginal and Torres Strait Islander people 35+ years and all others 45+ years (age criteria are based on NVDPA guideline screening recommendations37).
-
Attendance at the general practice or ACCHS at least three times in the previous 24-month period AND at least once in the previous 6-month period.
Site recruitment
Participating general practices have been recruited from the Sydney region in collaboration with primary healthcare organisations known in Australia as Medicare Locals. Participating ACCHSs have been recruited in partnership with two state representative bodies for ACCHSs, the Aboriginal Health & Medical Research Council (AH&MRC) of NSW and the Queensland and Aboriginal Islander Health Council (QAIHC). A $500AUD reimbursement to participating sites will be made to partially compensate for health service staff time commitment to study-related activities. Sites randomised to the intervention will receive training support in use of the system predominantly via face-to-face visits and webinars. All licence costs and technical support associated with the intervention will be provided free to the intervention sites in the first 12 months and to all sites for the following 12 months after completion of the trial. A newsletter and networking web site will be provided to participating sites. Royal Australian College of General Practitioners Quality Assurance and Continuing Professional Development points will be offered to participating GPs in both arms of the trial.
Randomisation
Sixty services (40 general practices and 20 ACCHSs) will be randomised in a 1:1 allocation to use HealthTracker or ‘usual care’ for 12 months. Clusters will be stratified at three levels:
-
ACCHS versus general practices.
-
Service size (<500 patients meeting eligibility criteria vs >=500).
-
Participation in existing QI programmes (current involvement in one of five national and state programmes involving regular audit and feedback versus past or never involved in these programmes).
A site assessment survey will be administered to all sites to assess for service eligibility and these stratifying variables. Permuted block randomisation will be centrally performed using a web-based form. As this is a pragmatic trial, allocation will be single blinded with outcome analyses conducted blinded to treatment allocation.
Intervention group
The intervention arm will receive the four components of the system described above (point-of-care decision support software, risk communication tools, data extraction tools and access to the QI portal). Clinical staff will be given training in use of the tools and a support service will be available for any technical queries. One initial face-to-face training visit and subsequent site visits and webinars targeting strategies to improve quality of care will be provided. Unless requested by health services the intervention will not be modified or discontinued. Reasons for discontinuation will be outlined and all analyses will be conducted on an intention-to-treat basis (see below).
Control group
Sites allocated to this arm will continue usual practice with their current systems without the implementation of HealthTracker. As the George Institute holds exclusive rights to the distribution of the system, there is no possibility of control sites having access to HealthTracker. If these sites already routinely use data extraction tools for assessing their quality of care then this will continue as normal. As with the intervention arm, services participating in any QI initiatives will continue participation as usual. For those sites not routinely using data extraction tools, the automated data extraction tool will be temporarily installed for data collection purposes only and then uninstalled that same day. A feedback report on performance will be provided at study completion only.
Quantitative data collection
Cross-sectional data will be collected in an automated manner for all patients who satisfy the eligibility criteria at each service (figure 5). These data will then be sent securely to the George Institute via an export function for the analysis of primary and secondary outcomes.
Prerandomisation: 1 month prior to randomisation, deidentified data will be collected from all sites. These data will be fed back to all sites as a formal report highlighting areas where data quality issues may occur.
Randomisation: Baseline data will be collected and sites will be randomised to intervention or control.
End of intervention period: At the end of 12 months, data will be collected in both study arms.
Primary outcomes
-
Change in the proportion of eligible patients receiving appropriate measurements of their CVD risk in the previous 12 months (measured at randomisation and at 12 months).
-
Change in the proportion of eligible patients assessed at high CVD risk receiving appropriate prescriptions for their CVD risk factors in the previous 12 months (measured at randomisation and 12 months).
Appropriate measurement of CVD risk factors is defined as having recorded or updated all the essential risk factors for the measurement of CVD risk (smoking status, blood pressure (BP) in the previous 12 months, total cholesterol and high-density lipoprotein (HDL) cholesterol in the previous 24 months) among those in whom risk assessment is guideline indicated. Unless explicitly recorded, diagnoses of diabetes or left ventricular hypertrophy will be assumed to be absent.
High CVD risk is defined as a calculated 5-year CVD risk of >15%, a history of CVD or the presence of any clinically high-risk conditions (as per NVDPA recommendations). Based on audit data, this is expected to comprise ∼30% of the patient population.10 ,11
Appropriate prescriptions is defined as a prescription for one or more BP lowering drugs and a statin for people at high risk without CVD; or a prescription for one or more BP lowering drugs and a statin and an antiplatelet agent (unless contraindicated by oral anticoagulant use) for people with established CVD.
Secondary outcomes
-
Change in the measurement of individual risk factors separately (smoking status, BP, cholesterol, other non-Framingham risk factors—BMI, chronic kidney disease (CKD) screening with urinary Albumin to Creatinine ratio, estimated Glomerular Filtration Rate);
-
Intensification of existing medication regimes among patients at high CVD risk (additional BP and lipid-lowering agents);
-
Changes in mean systolic BP, total cholesterol, LDL cholesterol and HDL cholesterol;
-
New CVD and CKD diagnoses.
Statistical considerations
Randomisation of 60 services (30 per arm) will provide 90% power to detect a ≥10% absolute higher occurrence in each primary study outcome among practices receiving HealthTracker. The following assumptions are based on our three audits in ACCHSs and mainstream general practices9–11 and include an assumed improvement of 10% in the two primary outcomes in control practices as a result of study participation.
-
Cluster size of eligible population will range from 200 in a small service through to 2000 in a large service. An average cluster size of 750 is assumed.
-
Recording rates of essential risk factors needed for risk assessment in the target group (first primary outcome) average 50%.10 ,11
-
Thirty per cent of the cluster will be either be at high CVD risk or have established CVD (n=250) and prescription of appropriate medicines to high-risk patients (second primary outcome) is 50%. This is based on our published data on drug prescriptions for individuals with and without established CVD.9–11
-
An intraclass correlation coefficient of 0.05 for both primary outcomes based on our audit data.9–11
-
Two-sided α=0.05
Data analysis will be performed on an intention-to-treat basis using generalised estimating equations.38 Subgroup analyses will be carried out using the three prespecified strata: (1) ACCHS versus general practices, (2) service size (small vs large) and (3) current participation in QI programmes vs past or no involvement in these programmes.
Economic evaluation
The economic evaluation will have a trial-based component and a modelled evaluation of long-term costs and outcomes. The incremental cost will be based on software, training and other costs incurred with transitioning practices to using HealthTracker. This will help determine the cost barriers experienced by different practices in adopting the system. Data on medications, laboratory tests, consultations and newly recorded diagnoses of CVD events incurred by eligible patients during the trial will be obtained from the data extraction tools. Costs will be calculated from prevailing Medicare rates and standard Australian National Diagnosis Related Groups cost weights for CVD hospitalisations. The incremental cost consequences of the HealthTracker system in achieving each of the primary outcomes will then be estimated, for example, cost per eligible patients assessed at high CVD risk receiving appropriate prescriptions. Trial-based data, however, cannot capture costs and outcomes beyond the trial. To address this, a modelled economic evaluation will enable quality of life and survival to be examined and allow incremental cost-effectiveness ratios to be calculated in terms of cost per Quality Adjusted Life Years gained. Using a Markov model, the eligible patient population in both study arms will be hypothetically tracked over an extended period. Transition between various defined health states, costs and quality of life attached to various health states and the projected long-term intervention effects from that observed in the trial will be based on published evidence. With appropriate discounting, estimates of long-term costs and outcomes will fold out of the model. Sensitivity analyses will be conducted on discount rate, uncertainty in outcome estimates and assumptions made in costing (eg, varying efficiencies with different patient practice ratios to those of the trial setting). This will better inform policy makers as to the resource consequences of rolling out this programme to scale.
Process evaluation
The qualitative evaluation of the β-version of HealthTracker suggested that a critical factor affecting the uptake of EDS interventions is whether and how they become embedded in routine healthcare.22 In the TORPEDO trial we will build on this observation through a detailed process evaluation to better appreciate the factors that might influence sustainability beyond the trial setting. Two qualitative methods will be used to explore these factors.
Semistructured interviews with health professionals and staff
A maximum variation sample will be taken to ensure diverse opinions are gained from patients, clinical and managerial health staff and sites with low and high uptake of the intervention.39 Key issues to be explored will include (1) how practitioners use HealthTracker; (2) what effects it has on organisational practices and personnel and (3) what are patients’ experiences of being presented with HealthTracker outputs and what impact does this have on the healthcare encounter. Individual informed consent will be sought and data will be collected towards the end of the intervention period so as not to unduly influence trial outcomes.
Audio/video ethnography
A key component of understanding barriers/enablers to use of HealthTracker is a better appreciation of how practitioners and patients use it at the point of care. Data collection using audio/video recording will capture how technological innovations are actually used in practice.40 Ethnographic analysis will greatly augment the interview accounts and will particularly shed important light on (1) how the intervention impacts on the flow of the clinical encounter; (2) how risk information is communicated between health professional and patient and (3) how the patient receives and interprets the information and the role it may play in shared decision-making processes. Although audio/video recorded clinical encounters are commonly used for primary care teaching purposes, such a technique can be potentially sensitive and therefore will be restricted to a small number of sites. Recordings will be conducted toward the end of the intervention period when both health staff and patients are thoroughly familiar with the system. This will occur over a 1-week period at each site. Participants who are approached for an interview will be invited to participate in this component. They will be given the option of having their healthcare encounter audio or video recorded. A follow-up interview will be arranged with these participants (both staff and patients) where the recording is played back for participant interpretation of the data.
These data will be supplemented by project officer field notes to identify any key processes, events, staffing and other resource issues occurring during the intervention period that may be relevant in gaining a better understanding of barriers and facilitators to implementation.
A multidisciplinary research team will guide the analysis process. As is common with qualitative inquiry, data analysis will commence early and be conducted contemporaneously with data collection. This method allows for interview content to be refined for subsequent data collection and to actively pursue emergent themes of interest. Although interviewing will continue until thematic saturation is achieved and therefore the exact number of interviews is unknown, we anticipate from prior experience that around 80 interviews (40 patients and 40 staff) will provide sufficiently rich data to meet our objectives.
Interview data will be digitally recorded, and professionally transcribed. NVivo 9 (QSR International Melbourne, Victoria, Australia) will be used to assist with data organisation and coding for key themes. Video data will be directly analysed and coded for key themes within NVivo. Feedback of findings to participants will be provided by a variety of methods, including workshops, summary reports, newsletters and via the study website.
Ethical considerations
The general practice component of the study is approved by the University of Sydney Human Research Ethics Committee (HREC) and the ACCHS component is approved by the Aboriginal Health and Medical Research Council HREC. Formal agreements with each of the participating sites have also been signed. Quantitative data will be obtained from deidentified clinical audits. Ethical approval to grant waiver of the usual requirement to obtain individual patient consent has been obtained. In participating ACCHS sites, eligible patients can request to ‘opt out’ from having data in the clinical audit data extracts exported. Data exports will be compliant with privacy legislation, centrally managed by the George Institute and held in strict confidence. Some individual health professionals (GPs, practice nurses, etc) and patient participants will have their informed consent taken at the site to allow data collection through semistructured in-depth interviews and/or the use of audio/videotaped healthcare encounters. Participation in this component will be optional. Patient information statements and consent forms have been approved by each ethics committee and formatted in accordance with their own guidelines and requirements.
The study will be conducted in accordance with the principles set out in the National Health and Medical Research Council and the NSW Aboriginal Health and Medical Research Council guidelines. Specific effort will be taken to respect the autonomy and governance of participating ACCHSs. The intellectual property rights of ACCHSs will be recognised and preserved. It is also recognised that ACCHSs have rights and responsibilities regarding the use of health-related information for their attending clients. Collaborators on the TORPEDO study will be encouraged to disseminate information from the project in a manner that supports health improvement for Aboriginal and Torres Strait Islander peoples and local benefit to participating ACCHSs.
Discussion
The TORPEDO study will seek to provide reliable evidence about the effectiveness of QI interventions incorporating EDS in Australian primary care settings. The implications of use of such systems for CVD risk management extend well beyond being a point-of-care clinical resource. Improving health system performance is central to the aims of this initiative and this is especially pertinent to addressing Aboriginal health inequities where the CVD burden is five-fold greater. There is potential for substantially better health outcomes from CVD in Australia with improved implementation of existing evidence in primary healthcare, where most of the opportunity to manage cardiovascular risk occurs. The strategy proposed is the first of its kind in Australia and is strongly aligned with national strategy recommendations for health system reform. If effective, HealthTracker could have widespread applicability for the prevention and management of other chronic diseases.
Strengths and limitations of this study
The strengths of the study are that it assesses an innovative complex intervention that is implemented in routine primary healthcare settings. It will provide rigorous evidence on process, clinical and economic outcomes and addresses an important issue facing health systems worldwide—namely scalable interventions that are able to achieve improvements in performance.
The main limitation is that it is conducted in one country, Australia, and thus its generalisability may be influenced by the prevailing health system context.
Acknowledgments
We gratefully acknowledge the support of the general practices and Aboriginal Community Controlled Health Services involved in this study. We also acknowledge the support of the Queensland Aboriginal and Islander Health Council, Aboriginal Health and Medical Research Council, Western Sydney Medicare Local, Inner West Sydney Medicare Local, South Eastern Sydney, Eastern Sydney Medicare Local, South Western Sydney Medicare Local and Nepean-Blue Mountains Medicare Local.
References
Footnotes
-
Contributors DP, AP and TU developed the original concept of this study. All authors contributed to the study design. DP, KP, BP, MH, TU and JH are involved in the implementation of the project. DP wrote the first draft of the protocol and the final manuscript was reviewed by all the authors.
-
Funding This study is funded by an Australian National Health and Medical Research Council (NHMRC) Project grant (ID 1010547) and NSW Department of Health. DP is supported by a NHMRC Translating Research into Practice Fellowship. AP is supported by an NHMRC Senior Research Fellowship. JR is funded by a Postdoctoral Fellowship cofunded by the NHMRC and National Heart Foundation.
-
HealthTracker Steering Committee David Peiris (Co-Chair), Anushka Patel (Co-Chair), Mark Harris, Tim Usherwood, Nicholas Zwar, Katie Panaretto, Jenny Hunt, Julie Redfern, Stephen Colagiuri, Stephen McMahon, Rod Jackson, Bruce Neal, David Sullivan, Fiona Turnbull, Alan Cass, Noel Hayman, Alex Brown, Jessica Stewart, Bindu Patel
-
TORPEDO Study Project Staff Marilyn Lyford, Maria Agaliotis, Sharon Parker, Lyn Anderson, Melvina Mitchell, Chris Henaway, Catriona McDonnell, Olly Shestowsky
-
Pen Computer Systems for their support in developing the HealthTracker software and the data extraction tool. Improvement Foundation of Australia for their support in developing and hosting the quality improvement portal.
-
Competing interests None.
-
Provenance and peer review Not commissioned; externally peer reviewed.
-
Data sharing statement No additional data are available.