Article Text

Abstract
Objectives To evaluate the long-term consequences of pregnancy-related venous thrombosis (VT) by the assessment of generic quality-of-life (QOL), well-being, general health and daily-life functioning. We also wanted to evaluate the impact of the frequently occurring complication post-thrombotic syndrome (PTS) after that of deep vein thrombosis (DVT).
Design Population-based cross-sectional, case–control study.
Setting 18 Norwegian hospitals during 1990–2003.
Participants The study population comprised 559 cases with a validated first-ever, pregnancy-related VT and 1229 controls naïve for VT at the time of index pregnancy. Cases were identified using the Norwegian Patient Register and the Medical Birth Registry of Norway and the latter was used to select as controls women who gave birth at the same time as a case. After exclusion of two cases with missing location of VT, the final study population comprised 311 cases and 353 controls.
Methods Self-completion of a comprehensive questionnaire in 2006.
Main outcome measures Generic QOL and well-being assessed by the Ferrans and Powers QOL Index (QLI) and the General Health Questionnaire (GHQ-20).
Results QOL assessed by QLI did not differ between cases and controls; mean score 23.1 (95% CI 22.7 to 23.5) vs 23.7 (23.3 to 24.0), neither did well being assessed by GHQ-20; 18.7 (18.0 to 19.4) vs 17.9 (17.3 to 18.4). However, cases reported pain other than in the lower limbs and muscle–skeletal problems more often and were more often physically worn out after work compared with controls. Cases which developed PTS reported poorer health, had pain more often, developed skin and psychiatric problems, used analgesic drugs more frequently and were more often on sick leave as compared to those without PTS.
Conclusions Long-term generic QOL and subjective well-being 3–16 years after a pregnancy-related VT were not different from a reference population, but women with PTS after DVT seemed to have poorer QOL and an impaired general health.
- Epidemiology
- Qualitative Research
This is an open-access article distributed under the terms of the Creative Commons Attribution Non-commercial License, which permits use, distribution, and reproduction in any medium, provided the original work is properly cited, the use is non commercial and is otherwise in compliance with the license. See: http://creativecommons.org/licenses/by-nc/2.0/ and http://creativecommons.org/licenses/by-nc/2.0/legalcode.
Statistics from Altmetric.com
Article summary
Article focus
-
To evaluate the long-term consequences of pregnancy-related venous thrombosis (VT) on generic quality of life (QOL) and subjective well-being, general health and daily-life functioning.
-
To evaluate the impact of the frequently occurring complication of post-thrombotic syndrome (PTS) following deep-vein thrombosis (DVT) on the long-term outcomes.
Key messages
-
Long-term generic QOL and well-being did not differ between cases and controls 3–16 years after a pregnancy-related VT.
-
Cases reported pain other than in the lower limbs and muscle–skeletal problems more often and were more often physically worn out after work compared with controls.
-
Women with PTS after DVT seem to have poorer QOL and an impaired general health.
Strengths and limitations of this study
-
The first study to report on generic QOL, general health and functioning after pregnancy-related VT.
-
A large, population-based study with validated diagnoses of VT and a follow-up over a long period.
-
Quality-of-life Index and General Health Questionnaire-20 are validated diagnostic tools for assessing QOL and well-being.
-
Selection bias cannot be excluded.
-
The entire questionnaire was based on self-reporting and data on comorbidity and use of medication were not validated.
-
Self-reported Villalta score is not validated as a diagnostic tool for PTS.
-
Information on recurrent VT is lacking.
Introduction
Pregnancy-related venous thrombosis (VT) is a disorder with potentially severe short-term and long-term outcomes.1 ,2 A substantial number of women with deep vein thrombosis (DVT) of the lower limbs develop long-term sequelae such as leg oedema, pain, skin discolouration and sometimes overt ulcers, which are collectively commonly known as the post-thrombotic syndrome (PTS).2 There is, however, a paucity of data regarding the long-term consequences of quality of life (QOL) and general health.
For VT outside pregnancy QOL has been shown to be reduced as compared with population norms, and the presence of PTS seems to be the most important predictor for a poor outcome.3–5 A study from the Mayo clinic found VT to be associated with impaired activities of daily living (ADL) and increased pain.6 Another small study with a mean follow-up of 5 years found that 17 of 39 patients with prior iliofemoral DVT developed venous claudication, resulting in interruption of walking in six patients and claudication was not seen in the limbs of the control patients.7 In a highly selective population with severe iliofemoral DVT more than 10 years back, 17 of 21 patients were essentially invalid as a consequence of long-term DVT they had suffered, being unable to work or care for their families.8 Other possible long-term consequences after VT, such as reduced general health, increased comorbidity and use of medication, reduced participation in professional life and increased sick leave have not been explored. We have previously published data that suggest a significant reduction in disease-specific QOL after pregnancy-related DVT assessed by the VEINES-QOL/Sym questionnaire,9 but generic QOL and functioning has not been evaluated in this population.
Generic QOL questionnaires can be used across diseases and treatment groups as opposed to a disease-specific questionnaire, which focuses on a particular condition or disease. SF-36 is the most widely used generic QOL questionnaire,10 but many other instruments have been validated and are often used. The Ferrans and Powers Quality of Life Index (QLI) measures both satisfaction and importance attached to various aspects of life.11 ,12 The General Health Questionnaire (GHQ) was originally developed by Goldberg as a screening instrument to identify depression and anxiety among general medical patients,13 but it is also believed to assess QOL and well-being and has frequently been used in this setting.14 ,15
The primary aim of the present study was to investigate the impact of pregnancy-related VT on long-term generic QOL and well-being assessed by QLI and GHQ-20. Secondary aims were to detect possible differences in general health, medication and daily functioning between cases and controls 3–16 years after a pregnancy-related VT. We also wanted to evaluate the impact of PTS on QOL, well-being and functioning among cases with DVT.
Methods
Study population
This study is a part of The Venous Thrombosis in Pregnancy study, and the selection of cases and controls have been described earlier.16 ,17 In short, the Norwegian Patient Register and the Medical Birth Registry of Norway were used for identifying all those women who have been diagnosed with pregnancy-related VT at 18 Norwegian hospitals during 1990–2003. The latter was also used for selecting as possible controls women who gave birth at one hospital (Oslo University Hospital Ullevål) at the same time as a case. A total of 531 cases and 1092 controls were invited to participate in the study. Of these, 313 cases with pregnancy-related VT and 353 controls with no VT prior to the index pregnancy entered the study and answered a comprehensive questionnaire in 2006 (figure 1). This population was also studied in our two previous publications regarding disease-specific QOL and PTS.2 ,9
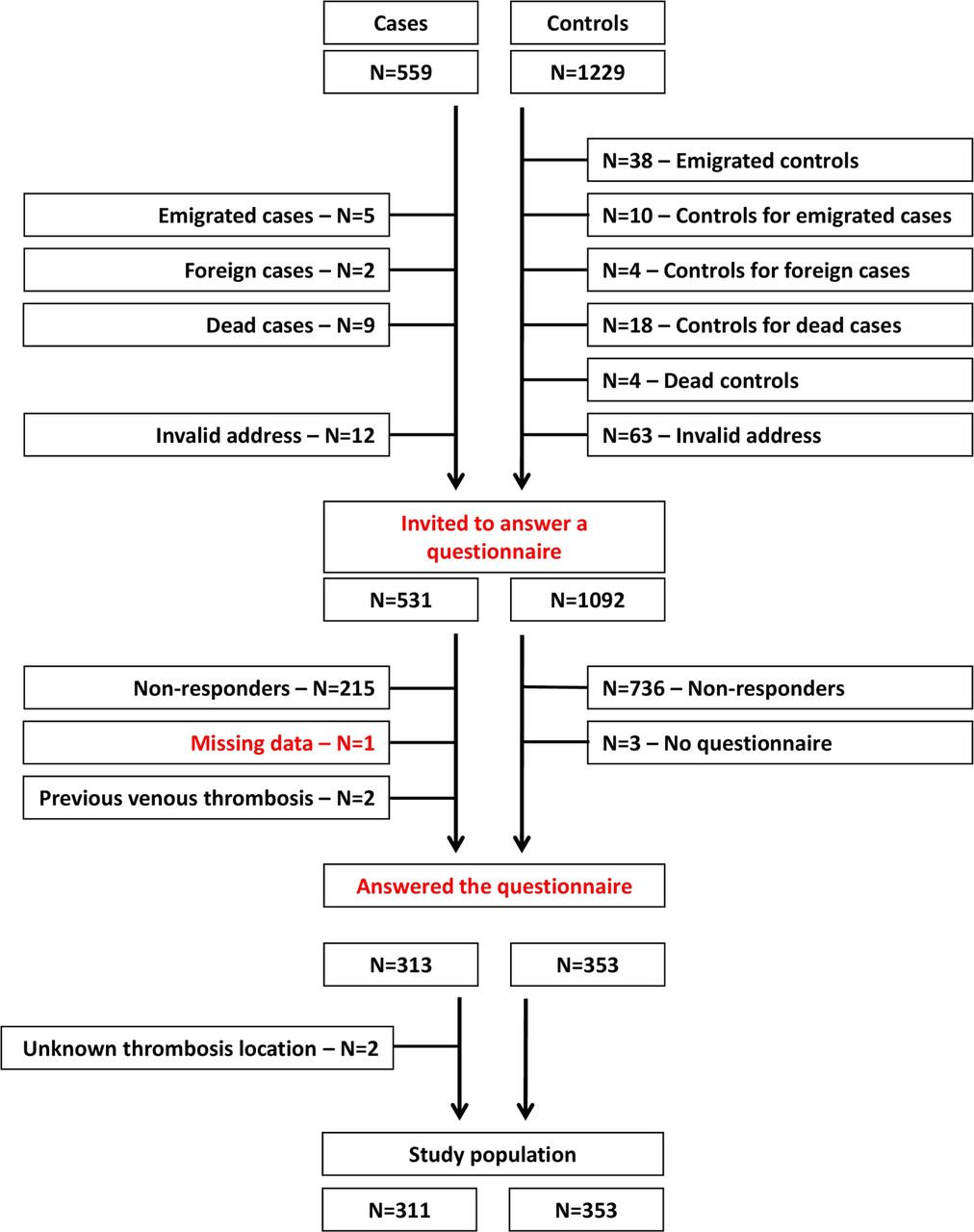
{kind=link}
Flow chart of the study population.
Variables and instruments
Medical records were reviewed at the participating hospitals and relevant medical information from the time of the index pregnancy was recorded. For the cases, the index pregnancy was the pregnancy during which their first-ever VT occurred; for the controls, it was the pregnancy leading to labour at the same time as the respective cases. For the cases, we recorded the type of VT (ie, DVT in the lower limbs, only PE or thrombosis at other locations). All cases of combined symptomatic DVT and PE were categorised in the present analyses as DVT.
A comprehensive questionnaire was completed by the participants when they presented at the hospitals for participation in the study in 2006. The entire questionnaire was self-reported, but health personnel were present during completion for instructions to the participants, if necessary. The questionnaire included information on marital status, parity, education, employment, income, sick leave, comorbidity, medication, weight and height, among other questions. Body mass index (BMI) was calculated from weight and height given in the questionnaire, and overweight was classified according to the WHO definition, that is BMI ≥25 kg/m2.
The questionnaire also included the Ferrans and Powers QLI.11 ,12 The definition of QOL upon which this questionnaire is based is ‘A person's sense of well-being that stems from satisfaction or dissatisfaction with the areas of life that are important for him/her’. We used the generic version II which has been translated into and validated in Norwegian.18 The current version III was not available in Norwegian at the beginning of the study. One section in the questionnaire measures satisfaction and the other measures the importance of each domain for the subject, each section includes 34 items. The items are scored from zero (very dissatisfied/very unimportant) to five (very satisfied/very important). No negative items are included. The overall score is determined as the product of the satisfaction responses and the importance responses, this corrects for the influence of individual values. The highest scores are produced by combinations of high satisfaction/high importance responses, whereas the lowest are produced by high dissatisfaction/high importance. The QLI produces five scores: overall and in four subdomains; health and functioning, socioeconomic, psychological/spiritual domains and family. The possible range for the overall and the subscale scores is zero to 30, the higher the score, the better the QOL.
Subjective well-being was assessed using the GHQ-20.13 The 20-items version has been translated into Norwegian and tested for its validity and reliability.19 ,20 The 20 items are scored from zero (less than usual) to three (rather more than usual), making a sum score from zero (good well-being) to 60 (poor well-being). It reflects both positive as well as negative aspects of life. For both Ferrans and Powers QLI and GHQ-20 we defined 0.5×SD of the mean scores of the control group to be the smallest change considered to be clinically important between cases and controls in QOL and well-being.21 ,22
A self-reported Villalta score was also included in the questionnaire.2 The Villalta score is currently the standard method used for diagnosing PTS.23 The participants graded five symptoms (pain, cramps, heaviness, paraesthesia and pruritus) and six clinical signs (pretibial oedema, skin induration, hyperpigmentation, redness, venous ectasia and pain on calf compression) from zero (absent) to three (severe) making a sum score from zero to 33. We defined PTS as a score of ≥5 in a leg with a previous DVT.2
Statistical analyses
The scores of the Ferrans and Powers QLI were computed using standard scoring algorithms for the QLI version III available at http://www.uic.edu/orgs/qli/. The scoring algorithm presented on the website was modified by us to be applicable for the QLI version II which was used in the questionnaire for the present study. When more than five items were missing among the satisfaction items or among the importance items, the entire QLI was considered missing. The scores of the GHQ-20 were computed simply by adding the value (between 0 and 3) from each of the 20 items. Missing scores were calculated when more than half of the 20 items of the GHQ-20 scale were available (‘half-item rule’).24 The individual's mean score of the non-missing items was imputed for the missing items. Data were presented as mean and SD and 95% CI for the point estimates were also included. Comparison between groups of continuous data that was not deviating markedly from the normal distribution was done using an independent-sample's t test. Dichotomous variables were compared using a χ2 test. Differences with a p value below 0.05 were considered to be statistically significant. Adjustments for possible confounders were done using logistic regression when the dependent variable was dichotomous (the Wald test) and linear regression when the dependent variable was continuous. The 95% CI of the mean total QLI and mean GHQ-20 scores were used for indicating whether the study had sufficient test power to discover a real difference in QOL between cases and controls. All analyses were performed using the Statistical Package for the Social Sciences V.18.0 (IBM SPSS Inc, Chicago, Illinois, USA).
Results
Total 313 cases with a validated diagnosis of VT and 353 controls agreed to participate in the study, signed an informed consent and completed a comprehensive questionnaire. Two cases were excluded from the present study because of an unknown location for VT (figure 1). Of the remaining cases, 214 had DVT in lower limbs, 74 had PE and 23 had DVT located other than in the lower limbs/lungs (10 had upper extremity DVT, 2 portal vein thrombosis, 9 sinus vein thrombosis, 1 superior vena cava thrombosis and 1 ovarian vein thrombosis). The mean time since VT was 8.9 (95% CI 8.4–9.3) years among cases and the mean time since index pregnancy was 7.7 (7.2–8.1) years among controls. The final study population comprised 311 cases and 353 controls. Cases and controls were comparable concerning age, marital status and parity, but cases had significantly less education, fewer had a full-time job, a lower family income, smoked more often, and had a higher BMI (table 1). Morbidity at the time of index pregnancy was very low according to the medical records and did not differ between cases and controls.2
Demographic and socioeconomic characteristics of the study population, questionnaire data from 2006
Quality of life among study participants
Total QOL assessed by the Ferrans and Powers QLI was slightly poorer among cases when compared with controls; mean 23.1 (95% CI 22.7–23.5) vs 23.7 (23.3–24.0, table 2). The difference between cases and controls of 0.6 was nearly statistically significant, but was not clinically significant when we used 0.5×SD (corresponding to a value of 1.7) to define the smallest change considered to be clinically important. The differences between the two groups in the four subscales were not considered to be of any clinical importance. General well-being assessed by GHQ-20 did not differ between cases and controls; 18.7 (95% CI 18.0–19.4) versus 17.8 (17.3–18.4). Cases and controls did not differ substantially regarding QOL and well-being when adjusting for possible confounders. QLI and GHQ-20 scores did not differ between cases with DVT in lower limbs and cases with PE (23.3 vs 22.7, p=0.26 and 18.8 vs 18.7, p=0.82, respectively).
Mean quality of life scores in the study population
General health and medication
The self-assessment of general health and use of medication among study participants is described in table 3. Ten per cent of the cases assessed their own health as bad or very bad compared with 4% of the controls. The cases also reported to have pain not related to lower limbs more often than did controls, almost 50% of cases had pain every week or more often compared with 32% of controls. Muscle–skeletal problems the last year were doubled in those with previous a VT related to pregnancy compared with controls (14% vs 7%, p=0.002), and cases also reported more constipation (12% vs 6%, p=0.008). Hypertension, allergy, lung diseases, kidney/urinary problems, metabolic diseases, skin problems, headache/migraine and psychiatric problems did not differ between the two groups. Heart diseases, peptic ulcers, diabetes and cancer were almost not reported in any group (results not shown). Analgesic drugs were used more often among cases than controls (14% vs 9%, p=0.028). The reported use of antidepressants and drugs against allergy and asthma were equally distributed among the study participants. Use of sleeping pills, tranquillizers, antihypertensive drugs, hormones, insulin and laxatives were almost not reported in any of the two groups (results not shown). Fifteen per cent of the women with a previous VT related to pregnancy 3–16 years ago were on anticoagulants at the time of filling out the questionnaire compared with 1% of controls (p<0.001). In total, 52% cases used vitamins, cod-liver oil or other dietary supplements, this was significantly less than that among controls where 68% reported such a use (p<0.001).
General health and functioning in the study population
When adjusting for possible confounders, pain other than in the lower limbs, muscle–skeletal problems and use of anticoagulants remained significantly more frequently reported among women with previous pregnancy-related VT and dietary supplements were used more often among controls.
Working ability
Women with previous VT were more often physically worn out after a day's work as compared with controls, but almost 60% in both groups were often or always mentally exhausted after work (table 3). One-third of the cases had 2 weeks or more of sick leave the previous year; this was significantly more than that in the control group were one-quarter reported sick leave of 2 weeks or more. When adjusting for possible confounders, cases were still physically worn out after a day's work more often than controls (p=0.010), but sick leave was not significantly different.
Impact of PTS on QOL and functioning
We have reported that 85 of 204 (42%) of the cases with DVT in the lower limbs had PTS (self-reported Villalta score ≥5) and 119 had a score of less than 5 corresponding to no PTS.2 Ten women of the 214 with DVT in lower limbs had missing Villalta scores and could not be evaluated for PTS. Cases suffering from PTS were slightly older than those without PTS (the mean age in 2006 40.2 vs 38.4, p=0.048), but marital status, parity, education, employment, household income, BMI and smoking were not different (results not shown). QOL and well-being were reduced among cases with PTS after pregnancy-related DVT compared with those without PTS, also when adjusting for possible confounders (p<0.001 and 0.003, respectively, see table 4). Women with PTS had a mean total QLI score of 22.2 (21.5–23.0) which was 1.8 points lower than that in those without PTS. This difference in the mean total QLI score was higher than 0.5×SD (which was 1.7), and we therefore considered the reduction in generic QOL among cases having PTS, as assessed by the Ferrans and Powers QLI, to be of a clinical importance. The mean GHQ-20 score was 2.5 points lower in the PTS group as compared with those without PTS, and this difference was not considered to be of a clinical importance (0.5×SD in the control group was 2.7).
Impact of PTS on QOL, general health and functioning
Women with PTS assessed their health to be worse compared with those without PTS; almost 16% reported their health to be bad or very bad compared with 6% without PTS (p=0.027). Women with PTS also reported significantly more pain, as many as 73% of those with PTS reported pain not related to the lower limbs every week or more often, as compared with 27% of those with no PTS. Women having PTS also reported more muscle–skeletal, skin and psychiatric problems, but allergy, constipation and headache/migraine did not differ between the two groups. Heart diseases, hypertension, lung diseases, kidney/urinary problems, metabolic diseases, peptic ulcers, diabetes and cancer were not or almost not reported in any group (results not shown). Analgesics and allergy medicine were used more often among those with PTS, but the use of vitamins and anticoagulants daily were equally distributed among the cases with and without PTS. The reported usage of sleeping pills, antidepressants, tranquillizers, asthma medication, antihypertensive drugs, hormones, insulin and laxatives were very low (results not shown). Cases with PTS were more often physically exhausted after a day's work and had more sick leaves than those without PTS. When adjusted for possible confounders, women with PTS still reported a poor health, pain not related to lower limbs more often, more skin and psychiatric problems, and the use of analgesic drugs and allergy medication, more often physically worn out after work, and more sick leaves compared with women without PTS.
Discussion
Generic QOL assessed by QLI did not differ between cases and controls, neither did well-being assessed by GHQ-20 3–16 years after pregnancy-related VT. Nevertheless, previous VT was associated with pain other than in the lower limbs, being physically worn out after a day's work and having muscle–skeletal problems more frequently than that among the reference population. Women with PTS as a chronic complication to DVT in a lower limb seem to have a particularly reduced outcome.
The negative impact of VT outside pregnancy on generic QOL have been documented in several studies,3 ,5 ,25 but one study did not find any impact of VT on QOL assessed by SF-36.6 These studies are difficult to compare with our study because of entirely different populations. The study population of the present study was younger, of a lower BMI and experienced a very little comorbidity as compared to that in previous reports. QOL has not been investigated after pregnancy-related VT, although we have previously reported data on disease-specific QOL after DVT in the lower limbs assessed by the VEINES-QOL/Sym questionnaire in a subpopulation of the current study, including 208 patients with pregnancy-related DVT in lower limbs. We found that cases had significantly reduced outcomes as compared with controls,9 and our results are diverging. Even if we did not find important differences in generic QOL and well-being between cases and controls, we found other differences that might have a negative impact on QOL that is not displayed by the two questionnaires. It is possible that generic QOL questionnaires are too general and do not capture specific health problems after VT and that disease-specific questionnaires are more focused. It is usually recommended to include both generic and disease-specific questionnaires when assessing QOL.26
We are not surprised that more women who were previously suffered from VT still used anticoagulation even if the event occurred many years ago. It is likely that several women have experienced recurrent VT which might lead to long-term anticoagulation. The higher use of dietary supplements among controls is more difficult to explain. It is well-known that different foods, medication and dietary supplements can interact with warfarin,27 thus in a Norwegian patient warfarin users are recommended to consult a doctor before taking a new medication, dietary supplements or herbal products. This may have caused a persisting caution against dietary supplements among previous or current warfarin users.
PTS has in several studies been found to be the most important predictor for reduced QOL after DVT outside pregnancy,4 ,5 and our findings are in line with this observation. PTS can lead to pain, swelling, eczema and venous ulcers in the affected lower limb. We found that generic QOL assessed by Ferrans and Powers QLI was reduced among cases having PTS, and these women also assessed their general health to be worse as compared with the women who had suffered DVT in a lower limb, but did not develop PTS. Almost 75% of cases having PTS reported pain other than in their lower limbs every week or more often compared with 25% of cases without PTS and this might contribute to a reduced QOL and general health. The reason for cases with PTS having more pain other than in the lower limbs is not obvious, but might be caused by a failure load in other parts of the body owing to limb problems. Eczema and venous ulcers as a part of PTS can be the reason for increased skin problems. Women with PTS also reported more psychiatric problems, and this corresponds to the knowledge that chronic disorders increase the likelihood of having mood and anxiety disorders.28–30 The more frequent use of analgesic drugs might be explained by increased pain other than in the lower limbs among cases with PTS. The increased use of allergy medicine is more difficult to explain, but one explanation can be that antihistamines are sometimes used to relieve itching that can be one of the symptoms of PTS. PTS also seems to increase sick leave and physical tolerance for working leading to exhaustion after a day's work. This might be caused by the symptoms related to PTS and an increased comorbidity in this group.
Limitations of the study
Among subjects initially invited to participate in the study, a substantial number declined. The controls were matched by date of birth and not by the place of living; the selection of cases from only one hospital was done mainly owing to limited funds. These two facts might introduce a selection bias. We had access to the hospitals’ medical files for all cases and controls, participating or not.31 No significant differences regarding age, smoking and BMI were detected between those participating or those who did not and we believe that our data can be generalised to the population of women suffering from VT related to pregnancy. We do not have information on socioeconomic variables, general health condition and pain experienced prior to the thrombotic event, and we can not exclude the posibility that these differences existed before the event. For the QLI the mean difference between cases and controls was 0.52 (95% CI 0–1.05), which is much lower than our definition of a clinically relevant difference. The 95% CI, however, was narrow and indicates that our study had sufficient test power. According to the medical files, comorbidity was very low at the time of index pregnancy. Therefore it is not likely that comorbidity before the event would have confounded our findings.
Self-reported Villalta score has not been validated, but it is not likely that our results on PTS will deviate very much from results of the original Villalta scale. The five symptoms of Villalta scale are self-reported in both scales, and the six clinical signs are the same, but in the original Villalta scale they are reported by health personnel and not by the patient.
We have performed a high number of analyses without correcting the p values, this might lead to an overestimation of the differences between groups. We have chosen this approach because this is the first study on generic QOL, general health and functioning after pregnancy-related VT, and must therefore be considered as a hypothesis-generating study. The entire questionnaire was based on self-reporting and data on comorbidity and the use of medication were not validated.
Strengths of the study
To our knowledge our study is the first to report generic QOL, general health and functioning after pregnancy-related VT. The study sample was large, thus it is not likely that the lack of power is the reason for not finding a difference between cases and controls as far as QOL and well-being were concerned. The study was population-based and the diagnoses of VT were all validated. The follow-up was long and the women's condition was probably stable for many years after the acute event. We had access to the medical files of those who participated in the study and those who declined. QLI and GHQ-20 are validated diagnostic tools for assessing QOL and well-being.
Conclusions
Long-term outcomes 3–16 years after pregnancy-related VT on QOL and well-being were comparable with that of the control population, but the cases still had reduced long-term functional outcomes regarding pain, muscle–skeletal problems and a feeling of physical exhaustion after a day's work. Cases that had DVT in a lower limb and had developed PTS as a chronic complication, seem to have particularly reduced outcome.
Acknowledgments
We are grateful to all the women who participated in the VIP study without any personal benefits.
References
Footnotes
-
Contributors HSW performed the statistical analyses, interpreted the data and wrote the first draft of the manuscript. AFJ designed the original study, collected the data and critically reviewed the manuscript. LS contributed to the statistical analyses and critically reviewed the manuscript. PMS designed the original study, interpreted the data and critically reviewed the manuscript.
-
Funding This work was supported by grants from the South-Eastern Norway Health Authority, the Oslo University Hospital Trust and the Norwegian Research Council (grant no 160805-V50). The sponsors of the study had no role in the study design; the collection, analysis and interpretation of data; or writing, review or an approval of the manuscript. The authors are fully independent of the sponsors.
-
Competing interests None.
-
Ethics approval The research protocol was approved by the Regional Committee for Research Ethics in Health Region East and the Norwegian Ministry of Health and Social Affairs. The Norwegian Data Inspectorate approved the processing of data files with sensitive personal health information and the merging of clinical data and data from the register. Informed consent was collected from the participants at the time of filling out the questionnaire.
-
Provenance and peer review Not commissioned; externally peer-reviewed.
-
Data sharing statement No additional data are available.