Article Text

Abstract
Objective The Department of Health's Enhanced Recovery Partnership Programme (ERPP) started a spread and adoption scheme of Enhanced Recovery After Surgery (ERAS) throughout England. In preparation for widespread adoption the ERPP wished to obtain expert consensus on appropriate outcome measures for ERAS, emerging techniques being widely adopted and proposed methods for the continued development and sustainability of ERAS in the National Health Service. The aim of this study was to interrogate expert opinion and define areas of consensus on these issues.
Design A Delphi technique using three rounds of reiterative questionnaires was used to obtain consensus.
Participants Experts were chosen from teams with experience of delivering a successful ERAS programme across different surgical specialties and across various disciplines.
Setting The first two rounds of the questionnaire were completed online and a final, third round was undertaken in a meeting using interactive voting.
Results 86 experts took part in this study. Consensus statements agreed that patient experience data should be recorded, analysed and reviewed at regular ERAS meetings. Recent developments in regional analgesia, the increased use of intraoperative monitoring for fluid management and cardio-pulmonary exercise testing were the main emerging techniques identified. National standards for those outcome measures would be welcomed. To sustain success in ERAS, the experts highlighted clinical champions and the presence of a dedicated ERAS facilitator as essential elements. For future networking, a unanimous agreement was achieved on the formation a national network to facilitate spread and adoption of ERAS and to promote research and education across surgery.
Conclusions Consensus was achieved on regular measurement and review of patient experience in ERAS. Agreement was reached on the role of regional analgesia and the use of oesophageal Doppler for intraoperative goal-directed fluid therapy. In order to facilitate the further spread and adoption of best practices and to promote research and education, an ERAS-UK network was recommended.
- Enhanced Recovery After Surgery
- Consensus Views
- Perioperative care
- Patient feedback
- Oesophageal doppler
- CPEX testing
This is an open-access article distributed under the terms of the Creative Commons Attribution Non-commercial License, which permits use, distribution, and reproduction in any medium, provided the original work is properly cited, the use is non commercial and is otherwise in compliance with the license. See: http://creativecommons.org/licenses/by-nc/2.0/ and http://creativecommons.org/licenses/by-nc/2.0/legalcode.
Statistics from Altmetric.com
- Enhanced Recovery After Surgery
- Consensus Views
- Perioperative care
- Patient feedback
- Oesophageal doppler
- CPEX testing
Article summary
Article focus
-
Enhanced Recovery After Surgery (ERAS) protocols have been shown in multiple systematic review and meta-analyses to improve postoperative outcomes, including length of stay, re-admission and complication rate.
-
A national initiative of the Enhanced Recovery Partnership Programme, which aimed to promote spread and adoption of ERAS in England, has recently come to an end.
-
In response to this initiative, this study wished to examine methods of measuring and reporting patient experience in ERAS, to evaluate the impact of new technologies and techniques and to seek consensus on how to sustain the success of ERAS in the future.
Key messages
-
Experts reached consensus on methods of capturing and reporting patient experience. The role of goal-directed fluid therapy in major surgery was also highlighted, along with the wide use of regional analgesia across surgical specialities in ERAS.
-
Collaborative research to develop large randomised controlled trials to generate robust evidence supporting one new surgical technique over the other is now indicated.
-
The expert participants have recommended the creation of a British forum, the function of this will be to continue supporting research and education in ERAS in the UK.
Strengths and limitations of this study
-
Consensus statements, such as those used in this study can be viewed as a weak source of evidence, but it is still felt that in this context they provide the best platform to channel further research.
-
The experts in this study were able to reach consensus in all areas examined allowing recommendations to be made that can used to direct future practice and research in ERAS.
Introduction
Enhanced Recovery After Surgery (ERAS) protocols aim to reduce the stress response to surgery and optimise postoperative recovery by employing a multimodal approach to perioperative management. The safety of ERAS protocols has been demonstrated in numerous randomised trials1–4 and a number of studies and meta-analyses have shown the efficacy of ERAS. Reduced length of stay, reduction in morbidity in the elderly, faster return of bowel function, earlier mobilisation and lower pain scores have all been demonstrated.5–9
Despite the evidence and encouraging results demonstrated by pioneering groups,10 ,11 the initial uptake of ERAS across the UK has been slow. In 2009, a collaborative initiative, the Enhanced Recovery Partnership Programme (ERPP), was established in England with aim of promoting spread and adoption of ERAS, in colorectal, musculoskeletal, gynaecology and urology major elective surgical pathways. This initiative successfully raised awareness of the benefits of ERAS and promoted sharing of good practice between expert teams and novice centres.12
As the ERPP was coming to an end, it became apparent that certain ambiguous issues existed surrounding how to sustain success of ERAS delivery and the measurement of patient experience in ERAS, which are not well addressed in the literature. There was also a need to explore the adoption and impact of the emerging new techniques, which are not included in the original ERAS protocol. Examples include preoperative cardiopulmonary exercise (CPEX) testing, use of minimal access surgery (MAS), goal-directed fluid therapy and alternative analgesic modalities. Hence, the aim of this study was to obtain consensus views on these key elements to ensure continual success of ERAS delivery in England.
Methods
The Delphi technique was used in this study. This technique involves a reiterative process of interrogation of a group of experts. Expert opinion from various sources is combined using qualitative then quantitative methods with the aim of converging on a shared consensus result.13 ,14 Notable characteristics of the Delphi technique include anonymity, controlled feedback of opinion, reiteration of concept and potential for application of statistical analysis techniques. It has been widely used in healthcare in areas such as epidemiology, education and improving clinical practice.15–17
Expert centres were defined by the ERPP as units with established ERAS programmes over 1 year, in at least one specialty. The units had displayed measurable reduction in the length of stay of at least 2 days. Experts were selected from these centres based on nomination from their peers within the unit as the leaders of ERAS. Eighty-six experts including 71 consultant clinicians 15 ER multidisciplinary team representatives from 32 different National Health Service (NHS) trusts across England were recruited into this study and were invited to complete the first round questionnaire. These represented 41 colorectal surgeons, 18 anaesthetists, 8 musculoskeletal specialists, 2 gynaecologists and 2 urologists. The expert group also included 15 other members of the multimodal team, such as an ERAS facilitator, preassessment clinic specialists and primary care specialists.
The first round questionnaire addressed the following themes:
-
Measuring patient experience.
-
Impact of new technologies and techniques on ERAS in the context of the greater use of laparoscopic surgery.
-
Ensuring sustainability including data collection and networking.
Open-ended questions were formulated by the authors in collaboration with key members of the ERPP Advisory Board (listed in Acknowledgments). Experts were invited by e-mail to either complete an online questionnaire (box 1) or to complete a paper version and return by post during May 2010. The responses to this first round were then grouped together to generate a limited number of statements or choices to form the second-round questionnaire in July 2010 (appendix 1). Experts were then asked to rank their agreement against each statement.
Round 1 questionnaire
-
Measuring patient experience
-
How do you measure patient experience of enhanced recovery in your centres?
-
How do you use this feedback to improve enhanced recovery pathways?
-
-
Impact of new technologies and techniques
-
What new technologies or techniques are you aware of that may have a positive future impact on enhanced recovery?
-
-
Ensuring sustainability
-
How can the good results from initial adoption of enhanced recovery be sustained overtime?
-
What ideas do you have for future clinical governance?
-
Is there a need for expert enhanced recovery sites to continue to communicate/network in the future and what from should this take?
-
How can expert enhanced recovery sited assist novice groups with adoption and implementation?
-
Categorisation of group responses
The third round was carried out during the first ERAS conference in Bristol in September 2010. It was facilitated by key members of the ERPP advisory board who did not vote but defined the terminology and encouraged group discussion before voting on each and every issue.
Results
Twenty-six NHS trusts responded to the first round questionnaire, with a total of 86 experts contributing to these replies (81.2% (26/32)), while 66 experts across 27 NHS trusts contributed to the second round responses (77.1% (27/35)). 32 experts representing 21 NHS trusts attended the third round meeting and contributed to the consensus statements.
Patient experience data
Round 1 identified several methods used at present to record and use patient experience data, which were then categorised and voted upon in round 2 (figure 1). The preferred methods of recording data were routine patient satisfaction questionnaire, patient diaries, patient reported outcome measures and patient focus groups. There was also agreement in round 2 regarding how the data should be utilised; to adjust the pathways and complete audit cycles (figure 2). In this round also, an enhanced recovery facilitator was identified to be responsible for collecting data on patient experience by 63.3% (19/30) of the group (positive verdict), while 33.3% (10/30) preferred clinical governance team.

Methods of recording patient experience data—results of round 2 voting.

Preferred methods of using patient experience data—results from round 2 voting.
In round 3, 53.8% (14/26) of the expert group supported the current use of routine patient satisfaction questionnaires and 30.8% (8/26) supported patient recorded outcome measures. Finally, a majority positive verdict (96.2% (25/26)) agreed with the following consensus statement:
Patient experience data should be recorded, analysed and reviewed at regular enhanced recovery meetings, where problems are investigated and adjusted where necessary, thus completing the audit cycle.
Impact of new technologies and techniques
In the first round, participants described 23 technologies that may positively impact on ERAS in future. These spanned all surgical domains and are shown in table 2.
Suggestions of new technologies that may positively impact on ERAS in future
The four most popular areas were chosen for further investigation in future rounds. These were postoperative pain management, oesophageal Doppler, CPEX testing and MAS.
Postoperative pain management
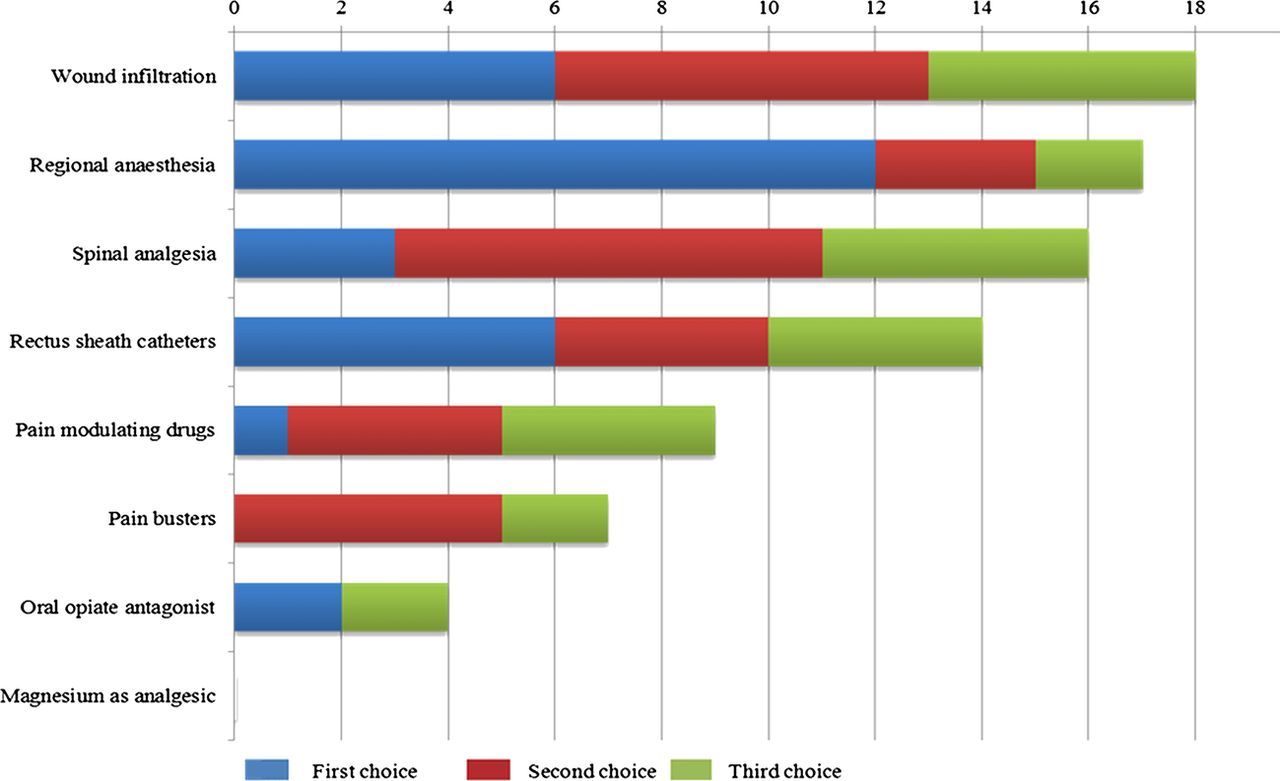
Round 2 presented to the participants a range of non-epidural pain management methods. Participants identified regional analgesia, including wound infiltration and spinal anaesthesia, as more likely to have the most impact on ERAS (figure 3). In addition, with the emergence of regional analgesia participants were asked to comment on the role of epidural analgesia; 36% (9/25) suggested open abdominal surgery and a minimal or non-existent role was suggested by 40% (10/25) of experts.
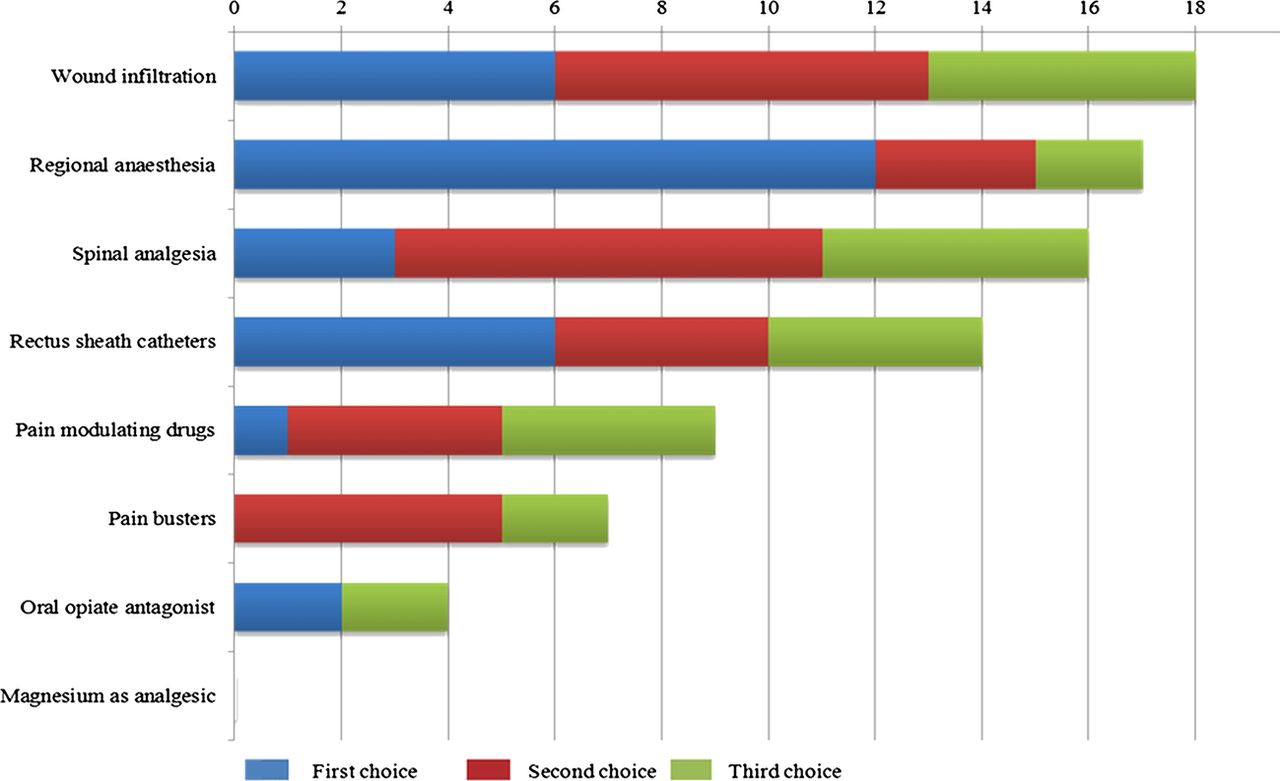
Non-epidural analgesic methods that will have the most impact on Enhanced Recovery After Surgery.
In the final round, a majority positive verdict (91.3% (21/23)) agreed with the consensus statement:
Epidural pain control should be used for specific types of operation (eg, open abdominal surgery) or for selected patients.
Oesophageal Doppler
Round 2 showed variability among centres in the impact of intraoperative oesophageal Doppler for goal directed fluid therapy with responses ranging from ‘excellent’ to ‘no benefit’. There was no consensus achieved to support its routine use for all cases. Concerns included financial restrictions (76.9% (20/26)) and lack of support from colleagues (57.7% (15/26)). However, a positive verdict (73.1% (19/26)) showed awareness of robust evidence to support its use and benefits in ERAS for selected cases.
CPEX testing
Round 2 identified that 43.3% (13/30) of the expert teams use CPEX testing for routine preoperative assessment, with two sites currently piloting its use. Participants stated various key factors that were necessary to successfully introduce CPEX testing such as ensuring funding, integration into the preassessment clinic and close liaison with anaesthetists. Of all the experts using CPEX testing, 61.9% (13/21) supported selective use in high-risk patients. There was a majority positive verdict (90.5% (19/21)) on the following consensus statement:
CPEX should be used selectively for high-risk patients and a multidisciplinary approach should decide which patients would benefit from this testing.
Minimal access surgery
In round 2 the impact of MAS to enhance recovery in various specialities is displayed in figure 4, with the maximum impact on ERAS still being seen in colorectal surgery. In round 3, there was discussion on importance of having training schemes, similar to that of the national training programme for laparoscopic colorectal surgery, in other specialties.19 There was no consensus achieved on this topic.

Expert opinion of impact of enhanced recovery after surgery on Enhanced Recovery After Surgery specific to specialty.
Ensuring sustainability
Sustainability
Table 3 shows proposals on how to sustain the success of ERAS taken from round 1 responses. The most prevalent suggestions were to hold regular team update meetings, to promote clinical champions, to deliver continual education and feedback teams and to have a designated ERAS facilitator.
Proposals on how to sustain success in ERAS
Participants in rounds 2 and 3 highlighted clinical champions and a motivated team, plus the presence of a dedicated ERAS facilitator, as essential elements to sustain success (figure 5).

Promoting sustainability in Enhanced Recovery After Surgery—results from round 2 voting.
Audit and data collection
Round 1 generated several ideas for clinical governance issues related to ERAS data collection. These included regular local audits of data and central databases of results/complications. The issues that emerged here were what to measure and who should have overall responsibility for data collection.
Round 2 identified measuring patient readmission (97.0% (32/33)) patient experience (97.0% (32/33)), complications (93.9% (31/33)) and length of stay (93.9% (31/33)) as key areas for data collection. However, after discussing outcome measures in round 3, it was recognised that there is no current evidence to define the optimum standard of complication rate or patient experience in ERAS. Thus, there was an agreement that there should be national standards for those outcome measures, reflected in the following consensus statement and supported by a majority positive verdict (95.8% (23/24)):
There should be a national standard written for ERAS to allow benchmarking.
An ERAS facilitator (85.3% (29/34)) was identified as the person who should have overall responsibility for data collection. However, the group also noted that consultants and the local clinical governance unit should also be involved in collection of data.
Future networking and support of novice sites
This section addressed the future of ERAS in England following the ERPP: is there a need for networking and, if so, how can this be achieved? The majority agreed that there is a need for continued networking.
Round 1 identified online forums and annual meetings as key future strategies to promote networking and to support novice sites. Round 2 supported the formation of a national network, an annual meeting and web-based forum as the preferred format of future networking (figure 6). This was confirmed at the final round with a unanimous agreement (25/25) with the consensus statement:
Future networking for the ERAS groups in the UK will be through a national network, an annual meeting and supported by a web-based forum.

Suggestions for future networking methods—round 2 results.
The main functions of the national network are to share experience and knowledge, to share consensus on best practice, to co-ordinate research projects and to support development of recommended standards of practice regarding outcome measures in ERAS (figures 6 and 7). There was a unanimous verdict on the aim of this association:
The Enhanced Recovery After Surgery Society (ERAS-UK) aims to advance research and education across all dimensions of enhanced recovery.

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Suggested roles of a national association for Enhanced Recovery After Surgery.
Discussion
The ERPP started a spread and adoption of ERAS programmes throughout England from 2009 to 2011, the current Delphi study examined ways to consolidate this initiative. In addition, this study aimed to examine expert opinion on the benefits of emerging techniques, for which there is currently no robust evidence to support their adoption. Finally, the identification of outcome measures to ensure the quality of ERAS protocols, and methods to sustain the initial benefits of ERPP across different surgical specialities required investigation.
Delphi method was used as a structured, opinion-based technique to reach consensus on a number of areas where clear evidence was lacking. Consensus statements, despite their weak evidence, are still the optimal method in identifying areas to channel further research and development in ERAS, including implementation and future practice. The initial rounds of this study identified many issues and the selection of those most relevant to practice in the UK were chosen for consensus statements.
An expert centre was defined as units with established ERAS programmes over 1 year and at least one specialty with a measurable reduction in length of stay of at least 2 days. Experts were selected from these centres based on nomination from their peers within the unit as the leaders of enhanced recovery in the centre. 86 experts responded to the generic questions in the first round questionnaire, including 71 clinicians and 15 ER multidisciplinary team members; however, as the questions became more focused and specialised the number of experts participating has reduced to 66 to round 2. The third round required experts to attend an interactive workshop and each centre nominated representatives to attend and vote.
The ERPP ran the campaign to increase spread of ERAS within the UK. In addition to this, the drive for this research was from the Cancer Action Team on behalf of NHS Improvement initiative and Department of Health in England. For these reasons, only centres from within the UK were appropriate for inclusion in the study.
Measuring patient experience has been highlighted as a fundamental aspect of ERAS and has now been supported by a national drive use patient experience as an outcome measure in England.20 Despite this, it remains recognised as an area that is currently not well practised in ERAS. Using patient experience data could benefit patients by illustrating areas of local ERAS pathways which need improvement, such as challenges with compliance. Also, understanding these experiences from the patients’ perspective will help clinicians, managers and commissioners to gain an accurate impression of how ‘useable’ the whole system is by a patient who interacts with it. This will encourage the delivery of more appropriate and more effective ERAS systems.
Although, this study identified patient satisfaction questionnaires, health-related quality of life and patient diaries as means of measuring patient experience, further validation studies on their format in ERAS are required.21
A key component of the ERAS pathway is effective postoperative analgesia, and routine use of epidural analgesia was recommended in the original ERAS pathway.22 However, with the MAS and the rapid emergence of alternative analgesic techniques, such as wound infusion catheters, Transversus Abdominis Plane block and spinal opioid analgesia, the role of routine use epidural analgesia has been questioned. This study highlighted the limited role of epidural analgesia in standard postoperative care following abdominal and musculoskeletal surgery, and as such it should potentially be limited to major open surgery. A recent randomised control trial found the failure rate of epidural analgesia for laparoscopic colonic resection to be 11%.23 However, randomised control trials are required in this field to ascertain optimal postoperative analgesia within ERAS and MAS.
The key factor to ensure sustainability was to adopt ERAS as the standard of care in routine surgical practice, which should continue beyond initial trials and funding. A motivated team with clinical leadership and supported by a dedicated ERAS facilitator were the main factors to maintain success of ERAS. Data collection should be carried out by each unit and in line with defined national standards (such as Health Episode Statistics) of clinical outcome measures such as length of stay, re-admission and complication rates in addition to patient experience. ERAS facilitators, local clinical governance and lead consultants should collectively be responsible for gathering and distributing the data.
The only domain with unanimous agreement in this study was towards the formation of a national ERAS network, encompassing all surgical specialties and members of the multidisciplinary team. The aims of this association would be to promote research and education and to encourage developing national standards in ERAS. In response to the findings of this manuscript, ‘Enhanced Recovery After Surgery-UK’ is in the process of registration and aims to fulfil the objectives created in this consensus study.
Conclusions
Consensus was achieved on the importance of the consistent measurement of outcomes including patient experience within ERAS. Agreement was also reached on the use of regional analgesia after major surgery and selective utilisation of CPEX. This study highlighted the increasing awareness of the evidence to support the use of oesophageal Doppler for intraoperative goal directed fluid therapy. Clinical championship and a dedicated facilitator underpin sustaining success in ERAS. A clear consensus was obtained to support the development of national standards and the formation of an ERAS-UK.
Acknowledgments
Thank you to all at the ERPP steering board for their help in the initial direction of this study. Fiona Carter (ERPP Operation Board Member), Andy McMeeking (NCAT), Janine Roberts (ERPP Lead), Monty Mythen (ERPP National Clinical Lead), Alan Horgan (ERPP National Clinical Lead) and John McGrath (ERPP Clinical Lead for Urology). And we are thankful to Mark Coleman the National Lead of Laparoscopic Colorectal National Training Programme for his advice.
References
Footnotes
-
This study was commissioned by the Cancer Action Team, on behalf of the Enhanced Recovery Partnership Programme, England.
-
Contributors AK participated in analysis of results, drafting and editing of paper. SP participated in analysis of results, drafting and editing of paper. JMG participated in study design and content, drafting and editing of paper. RK participated in study design and content, drafting and editing of paper. AH participated in study design and content, drafting and editing of paper. MM participated in study design and content, drafting and editing of paper. Dr FC participated in study design and content, analysis and results, drafting and editing of paper. NF participated in study design and content, analysis and results, drafting and editing of paper and the gaurantor.
-
Funding This work was supported by a grant from the National Cancer Action team to facilitate research and networking related to enhanced recovery in England as part of the Enhanced Recovery Partnership Programme.
-
Competing interests Olle Ljungqvist (a reviewer), Professor of Surgery, Örebro University Hospital 701 85, Örebro, Sweden personally knows several of the authors and has ongoing projects with two of them. Olle Ljungqvist serves as advisor for Nutricia, a producer of nutritional drinks that are used in ERAS recommendations.
-
Provenance and peer review Not commissioned; externally peer reviewed.
-
Data sharing statement Dataset available from the corresponding author (nader.francis@ydh.nhs.uk).