Article Text

Abstract
Objectives The purpose of this study was to provide a more precise definition of an integrated oncogeriatric approach (IOGA) through concept analysis.
Data sources The literature was reviewed from January 2005 to April 2011 integrating three broad terms: geriatric oncology, multidisciplinarity and integrated care delivery models.
Study eligibility criteria Citation selection was based on: (1) elderly cancer patients as the study population; (2) disease management and (3) case studies, intervention studies, assessments, evaluations and studies. Inclusion and exclusion criteria were refined in the course of the literature search.
Interventions Initiatives in geriatric oncology that relate to oncology services, social support services and primary care services for elderly cancer patients.
Participants Elderly cancer patients aged 70 years old or more.
Study appraisal and synthesis methods Rodgers’ concept analysis method was used for this study. The analysis was carried out according to thematic analysis based on the elements of the Chronic Care Model.
Results The search identified 618 citations. After in-depth appraisal of 327 potential citations, 62 articles that met our inclusion criteria were included in the analysis. Three IOGA main attributes were identified, which constitute IOGA's core aspects: geriatric assessment (GA), comorbidity burden and treatment outcomes. The IOGA concept comprises two broad antecedents: coordinated healthcare delivery and primary supportive care services. Regarding the consequents of an integrated approach in geriatric oncology, the studies reviewed remain inconclusive.
Conclusions Our study highlights the pioneering character of the multidimensional IOGA concept, for which the relationship between clinical and organisational attributes, on the one hand, and contextual antecedents, on the other, is not well understood. We have yet to ascertain IOGA's consequents.
Implications of key findings There is clearly a need for a whole-system approach to change that will provide direction for multilevel (clinical, organisational, strategic) interventions to support interdisciplinary practice, education and research.
- Oncology
- Geriatric Medicine
This is an open-access article distributed under the terms of the Creative Commons Attribution Non-commercial License, which permits use, distribution, and reproduction in any medium, provided the original work is properly cited, the use is non commercial and is otherwise in compliance with the license. See: http://creativecommons.org/licenses/by-nc/2.0/ and http://creativecommons.org/licenses/by-nc/2.0/legalcode.
Statistics from Altmetric.com
Article summary
Article focus
-
An integrated oncogeriatric approach (IOGA) has emerged as a top priority within the international geriatric oncology community.
-
Given the novelty of the IOGA concept and the possible contributions of the clinical and organisational domains to its development, there is a need for a common understanding of IOGA if healthcare system actors are to work together to achieve it.
-
This article attempt to clarify the IOGA concept using a systematic literature review and concept analysis methods.
Key messages
-
Sixty-two articles were retained for in-depth analysis.
-
Over 70% of the articles were related to the development or utilisation of geriatric assessment, 50% focused on clinical guidelines to support treatment. Very few focused on care coordination or multidisciplinarity and none addressed the specific question of an integrated approach to cancer care for the elderly.
-
This study highlights the pioneering character of the multidimensional IOGA concept, for which there is a lack of pertinent data to understand the nature of such a complex approach, the organisational and practice changes required, and the outcomes that may realistically be anticipated.
Strengths and limitations of this study
-
The strengths of this study are the use of Rogers’ concept analysis method, the integrative search strategy, the data extraction based on the Chronic Care Model and the control for bias using two researchers.
-
Our focus on identifying articles that could enhance our understanding of the IOGA concept led us to include studies that were not all equally robust.
-
While concepts are evolving, our study must therefore be understood as a first attempt at clarifying, at a particular point in time, an emerging concept in the field of geriatric oncology.
Introduction
As the world's population ages, the risk of cancer increases. In developed countries, more than half of cancers occur in patients aged 70 years and older. Consequently, geriatric oncology is now at the forefront of oncology practice. Over the past 15 years, the development of clinical practices and healthcare delivery systems based on an integrated oncogeriatric approach (IOGA) has emerged as a top priority within the international geriatric oncology community.1 ,2 Geriatric oncology focuses on the specific needs of elderly cancer patients related not only to their chronological age, but to the uniqueness of each person's pattern of aging. It is widely recognised that coordination and collaboration along the cancer care continuum should focus on individual needs, values and preferences, but little is said on the appropriate configurations services should adopt to achieve these goals. While evidence reports that integrated approaches are designed to overcome clinical, administrative and policy barriers and improve the quality and the security of care for elderly persons,3 there is as yet no shared definition of an integrated approach to cancer care for the elderly.
Given the complexity of the IOGA concept and the possible contributions of the clinical and organisational domains to its development, we considered that a systematic review of the literature integrating these perspectives was needed. The purpose of this study was to provide a more precise definition of an IOGA through a concept analysis.
Methods
The IOGA concept was analysed using Rodgers’ method (table 1).4 According to Rodgers, a concept is not a word, but rather the expression of the mental representations of this word at a particular point in time and in a particular context. This method entails identifying the attributes (characteristics), antecedents (preconditions for IOGA in action) and consequents (outcomes) of a concept. The concept's attributes refer to its main characteristics. Its antecedents represent the contextual factors, situations or processes that must occur beforehand and that encourage the translation of the IOGA idea into concrete practices. Finally, the consequents pertain to the behaviours or actions resulting from the use of the concept.
Rodgers’ method of concept analysis3
Search strategy
The aim of the search strategy was to identify an appropriate realm for data collection in which to perform the IOGA concept analysis4 The strategy was based on the methodological approach to systematic and comprehensive literature reviews developed by Cooper5 and updated by Whittemore and Knafl.6 This approach can incorporate various types of studies (ie, qualitative and quantitative research) and reveal a variety of perspectives on the phenomenon of concern. We also followed the Preferred Reporting Items for Systematic Reviews and Meta-Analyses checklist as close as possible7 to the extent that it was applicable to concept analysis which is descriptive synthesis of the literature. We focused on articles published between January 2005 and April 2011. The databases searched were CINAHL, PubMed, MEDLINE, SocIndex, PsychInfo, International Political Science Abstracts, Ageline and Abstracts in Social Gerontology. Keywords used in combination were: ‘elderly’, ‘70+ years’, ‘older’, ‘old’, ‘cancer’, ‘geriatric oncology’, ‘geriatric oncology assessment’, ‘interdisciplinarity’, ‘multidisciplinarity’, ‘transdisciplinarity’ ‘multidisciplinary team cancer’, ‘multidisciplinary practice’, ‘interdisciplinary collaboration’, ‘interprofessional’, ‘interprofessional relations’, ‘collaborative care’, ‘health services’, ‘healthcare’, ‘healthcare services’, ‘healthcare reform’, ‘integration’ and ‘integrated service delivery’. The literature search was performed by two researchers (DT and KC).
Article selection
To select articles, we followed a three-phase approach. The first phase, citation selection, was based on: (1) elderly cancer patients as the study population; (2) disease management as an intervention and (3) case studies, intervention studies, assessments and evaluation studies as study characteristics. In the second phase, inclusion and exclusion criteria were gradually refined. Inclusion criteria were: (1) integration or coordination along the cancer care continuum; (2) geriatric assessment (GA) and approach; (3) cancer treatment decision-making; (4) patients aged 70 years and more and (5) multidisciplinarity. Exclusion criteria were: (1) literature reviews; (2) case reports; (3) particular therapeutic regimens; (4) opinion pieces or essays; (5) studies without any abstract; (6) professional training programmes; (7) specific episodes of the cancer care continuum (systematic screening, palliative care and cancer survivorship) and (8) access to medical insurance and treatment cost (the USA). The third phase consisted of assessing which citations (titles and abstracts) were relevant to the understanding of the concept. The initial title and abstract selection was done independently by DT and KC using the inclusion and exclusion criteria. This selection was validated by a third researcher, CT. Differences were resolved through discussions between DT and CT until a consensus was reached.
Data analysis
All relevant papers to be included into the full review were compiled into a formal database and managed using QDA Miner software. We developed an open-ended coding grid based on the elements of the Chronic Care Model (CCM): (1) health system—organisation of healthcare; (2) self-management support; (3) treatment decision-making support; (4) delivery system design; (5) clinical information systems and (6) community resources and policies.8 This approach enabled us to focus the analysis on concepts related to the CCM and also to integrate other concepts that emerged iteratively from our analysis. The CCM was chosen because it specifies linkages between professionals and between professionals and patients, as well as among different levels of care (eg, hospital and community care).8 ,9
The following information was systematically extracted from each article: (1) basic information on the article (title, year, authors, journal title, abstract, objectives and framework and keywords); (2) purpose of the study (evaluation tools, epidemiology, comorbidity and care coordination or system integration); (3) methods (qualitative, quantitative and mixed); (4) study design (eg, descriptive case study, randomised controlled trials and time series); (5) participants (setting, sample, data collection, procedures and tools) and (6) results. A coding process allowed us to build the thematic network of the IOGA concept's attributes, antecedents and consequents.
Results
Figure 1 shows the number of citations at each of the three phases of the selection process. The search strategies identified 618 potential citations from our three broad domains. A screening of the titles and abstracts led to 327 potentially eligible citations. Based on our inclusion and exclusion criteria, 62 articles were retained for in-depth analysis. A little over 70% of the articles were related to the development or utilisation of GA tools (table 2). Half of the articles focused on clinical guidelines to support medical treatment decision-making and individualised care planning. Very few studies focused on care coordination or multidisciplinarity. None addressed the specific question of an integrated approach to cancer care for the elderly.
Integrated oncogeriatric approach concept (attributes, antecedents and consequents)

Article selection flow diagram.
Attributes
Three main attributes were identified: GA, comorbidity and treatment outcomes. The reviewed literature on geriatric oncology frequently aimed to clarify the relationships between these attributes.
Geriatric assessment
Development of GA tools and guidelines emerged as the cornerstone of the IOGA concept.10–42 However, the exact purpose of GA remains unclear. The consensus conference held in 1987 defined Comprehensive Geriatric Assessment (CGA) as: ‘a multidisciplinary evaluation in which the multiple problems of older persons are uncovered, described and explained, if possible, and in which the resources and strengths of the person are catalogued, need for services assessed, and a coordinated care plan developed to focus interventions on the person's problems’.43 When used in geriatric oncology, CGA has been frequently cut down to the preliminary step of describing the older person's health problems. Several CGA-based tools have been developed and studied in the oncology setting.12–17 ,19 ,22–24 26–31 ,37 ,38 ,40 These tools provide data on older cancer patients’ characteristics through validated geriatric tools designed to detect, but not diagnose, problems in the main dimensions of GA.44 In addition to these kinds of instruments, which can be described as multidimensional geriatric assessment tools, another group of tools has been developed recently, called screening tools,14 ,29 ,31 ,48 which may, for instance, help determine which healthy older patients are candidates for standard cancer treatment.
GA has been associated with numerous benefits. It can bring to light unknown problems in domains that may clearly interfere with cancer treatment decision-making.27 ,37 In particular, cancer treatment may generate declines in physical and functional abilities that represent crucial domains for older patients in terms of quality of life and survival.45 GA tools may help professionals ascertain a patient's functional status and then tailor cancer treatment to avoid over-treatment in patients at high risk of functional decline.19 GA has also been associated with improved tolerance to therapy and high prognostic value19 and may provide valuable prognostic factors.46 ,47
However, while various instruments have been studied, no definitive consensus has yet been reached regarding assessment tools’ correct use and place.13 ,14 The current trend is to start with a screening tool to narrow the target population down to those in need of more in-depth and CGA. However, screening tools vary in their sensitivity for measuring different items.13 ,14 Consequently, depending on the choices physicians make in applying these instruments, there is a risk of over-treatment or under-treatment of patients.
Moreover, whereas the literature reviewed extols the virtues of GA, Puts et al16 highlight the divergences between oncologists’ and geriatricians’ experience of it. Oncologists usually carry out non-systematic and non-standardised GA. Differences in perception between oncologists and geriatricians regarding the use of GA tools have also been reported by other authors.32 Hurria et al 24 concluded there is no consensus within the geriatric oncology community regarding a standard GA instrument for older patients with cancer. International Society of Geriatric Oncology (SIOG) experts have declared they cannot recommend any specific GA tool.43 Hence, in spite of its advantages, GA is not necessarily current practice for oncologists.
Comorbidity burden
Comorbid conditions are common among ageing people,11–14 16–19 21–23 ,25 ,27 ,30 ,35 ,37 ,38 ,40 ,49–66 posing a challenge to treatment decision-making and the organisation of care.22 The comorbidity burden may thus influence integrated cancer care for elderly patients. Properly assessing the relationships between comorbid conditions and cancer treatment or patient outcomes such as functional decline and mortality is a major concern.11 ,18 ,25 ,40 ,59 ,66 ,67 The reviewed literature provides contradictory data on key issues in geriatric oncology: (1) correlation between comorbidity and mortality and (2) comorbidity impacts on functional decline.
First, it is not clear as to whether comorbidity generates increased mortality in older patients with cancer. Alphs et al,50 whose aim was to predict the impact of surgical outcome on survival among elderly women with ovarian and primary peritoneal cancer, stated that comorbidity is associated with an increased risk in mortality. Janssen-Heijnen et al11 reported that comorbidity has an independent prognostic effect on survival among patients with colorectal and breast cancer. Another study25 concluded that it is not so much the number of comorbid conditions that affects survival, but their severity. In fact, comorbidity was associated with survival outcomes depending on the presence of functional limitations and geriatric syndromes (delirium, falls, incontinence and frailty).68 In colorectal cancer patients, comorbidity negatively influenced cancer-specific mortality, and not overall survival, whereas geriatric syndromes and functional limitations affected overall survival.74 Arnoldi et al38 made a similar observation regarding an outpatient population. Considering these results, the presence of comorbidity does not appear to have a direct prognostic effect on mortality, and its severity matters more than the fact of its absence or presence. Therefore, the extent to which comorbidity has an independent prognostic effect on mortality is challenged by certain studies reporting that the effect of comorbidity on survival is contingent upon patients’ functional status and the severity of their comorbid conditions.
Second, comorbidity's impact on functional decline is also controversial. Gironés et al22 reported that comorbid conditions had little impact on functional decline among elderly breast cancer patients. However, it remains difficult to ascertain whether it is the aging process or the cancer treatment that produces functional decline. Although Kurtz et al66 underlined the role of functional decline in increased hospital admission rates, they failed to determine the role of the cancer itself, as opposed to other comorbid conditions, in the decrease of physical functioning.
Relationships between comorbidity and functional decline have therefore not been clearly demonstrated in geriatric oncology. In some studies, comorbidity affected patient outcomes.11 ,38 ,50 In others, functional decline worsened following cancer treatment17 ,31 and affected survival when combined with comorbidity. However, studies focused on this issue reported no association between comorbidity and functional decline, which speaks to the lack of validated measurement methods rather than to the real absence of relationships.67 The development of such instruments may not only help clarify the interactions between comorbidity and functional decline, but also their potential impact on survival.
Treatment outcomes
Regarding treatment outcomes,10 ,11 ,16 ,17 ,26 ,28 ,30 ,31 ,34 ,37 ,40 ,49–58 ,60 ,63 ,65 ,66 ,69 the main preoccupation in geriatric oncology revolves around finding the most effective treatment regimen with an acceptable toxicity risk. While ultimately the goal remains cancer control, greater consideration must be given to the variability of elderly cancer patients’ health status and independence. On the one hand, patients may be undertreated because of physicians’ fears regarding their patients’ greater susceptibility to toxicity. On the other hand, standard protocols may lead to increased risk of toxicity and overtreatment for some patients.70 Moreover, cancer stage may sometimes be underestimated if patients’ non-specific symptoms are attributed to comorbid conditions or the ageing process.10 Optimal functional status represents a critical outcome in older cancer patients. The association between cancer treatment and functional decline remains an open question. More specifically, fatigue brought on by cancer treatment may accelerate functional decline.17 Functional dependence was more frequently observed in patients who had surgery or radiation therapy in addition to chemotherapy.31 Impairment may affect instrumental activities of daily living, in particular the capacity to drive and/or use public transportation.22 However, in older cancer outpatients, functional status was reasonably preserved, even among patients considered frail.38 Similar proportions of patients with functional decline were observed between cancer and non-cancer older patients admitted to a geriatric unit.60 The relationships between cancer treatment and functional decline thus remain unclear because of the heterogeneity of patients’ characteristics in the studies reviewed, especially cancer type, stage and treatment, functional status measurement methods and time of the functional assessment.
Some attention was given to the impact of various support services on patient outcomes. On the one hand, GA may help define older cancer patients’ health status, especially risk factors for frailty; GA may also clarify patients’ needs for specific services. However, patient outcomes also depend on cancer characteristics, which explain why survival might not be quite different in patients with advanced disease receiving cancer treatment or supportive care.38 On the other hand, a study conducted in an acute care geriatric ward found that older cancer patients received suboptimal cancer treatment and were more likely to suffer from depression and malnutrition.57 The need for a more complete assessment to detect geriatric problems in older cancer patients admitted to geriatric wards was underlined by the same authors. Finally, the review emphasised the need for a more responsive healthcare system due to the intricacy of older patients’ health problems.69
Antecedents
The reviewed literature showed that the IOGA concept comprises two broad antecedents: coordinated healthcare delivery and primary care and support services in the community.12 ,14 ,16 ,17 ,21 ,23 ,24 ,30–32 35–37 ,39 ,49 ,56 ,61 ,62 ,64 ,69 ,71–73 ,75
Coordinated healthcare delivery
Coordinated healthcare delivery refers to the patterns of interaction between healthcare professionals within an interdisciplinary team in order to successfully meet the needs of patients and, in particular, ensure that health and social services are delivered in tandem and according to a patient's specific needs.16 ,32 ,69 ,71 ,76 In the literature on geriatric oncology, multidisciplinary teamwork is considered the core mechanism to improve both collaboration and care coordination. Emphasis is put on the relationships between oncologists and geriatricians. In one study that examined oncologists’ and geriatricians’ views of the French geriatric oncology system, which aims to improve care coordination for elderly cancer patients, the authors observed multiple heterogeneous practices based on local resources and care models that left geriatricians’ involvement in patient with cancer care, most often, incomplete.32 According to the authors, the successful implementation of an integrated approach is challenged by everyday work relationships as well as by professional turf protection. A Canadian study16 explored the relationship between oncologists and geriatricians within a university hospital. The authors recommended more effective collaboration between specialists. Hence, coordination of care is crucially defined by interprofessional relationships between geriatric and oncology teams.
There are also calls for improvements at the organisational level, although they are nascent. For example, Puts et al16 recommended the creation of networks that would include geriatricians. More broadly, there is a call in the geriatric oncology literature to organise the healthcare system so that the needs of the elderly cancer population, and particularly functional outcomes, will be properly taken into consideration.31
Primary care and support services in the community
Numerous services are considered necessary for appropriate care of elderly cancer patients. In particular, access to social services, mental health services, transportation services and home care services would help limit patient hospitalisations motivated by social reasons.12 ,16 ,23 ,35 ,36 ,56 ,69 ,71–73 The association between lack of social support and depression was raised in one study.23 Furthermore, elderly patients living alone tended not only to be depressed, but also to be malnourished, which may cause poor tolerance to cancer treatment.12 Also, living alone, not driving, mobility and vision problems and a willingness to maintain independence were reported to affect the cancer care experience.71 Elderly cancer patients seemed reluctant to assert their needs to healthcare professionals, thereby decreasing the probability of those needs being met.71 This situation led Kurtz et al35 to refer to ‘unmet needs’ as ‘unknown needs’. Kahana et al73 reported that elderly patients may remain cautious and passive about seeking social support. However, a transition in older patients’ behaviour has been observed from passivity to proactive consumerism, suggesting the possibility of fruitful healthcare partnership between patients and professionals.73 Providing the appropriate social support for elderly cancer patients thus depends on the extent to which the latter are given the opportunity to voice their needs.
In terms of primary care, the reviewed literature indicated variability regarding referrals of elderly cancer patients. While referral rates decreased as a function of age,12 ,35 age itself was not the overriding factor for the lower frequency of referrals.35 Functional dependency,31 ,35 comorbidity and patients’ preferences35 were also important parameters. For instance, Goodwin et al31 reported that functional dependency may influence clinicians’ care plans, as well as patients’ adherence to treatment. This tended to result in undertreatment of cancer in elderly patients. Finally, shortcomings in multidisciplinary teamwork may also translate into less frequent referrals. In particular, Lynch et al36 reported that patients seen by a social worker were not referred for evaluation into the programme, whereas those seen by a nurse or a physician were referred.
A few other studies focused more squarely on the role of families and/or caregivers.56 ,72 While there are calls for the family to take part in treatment decision-making,56 such help may be at times ‘neutrally received’ by the elderly patient.71 Since a patient's perception of the availability of social support services may play a role in treatment refusal, Sinding et al71 stressed the need for ‘adequately resourced and skilled hospital care and sufficient, consistent and reliable community care’, particularly because of some patients’ reluctance to accept help from family members. While families and caregivers play an important role in terms of social support, elderly patients’ reluctance to seek help requires that skilled primary healthcare professionals accompany caregivers.
Consequents
Regarding the consequents of IOGA, the studies reviewed were inconclusive. No study specifically explored how different organisational models of care may shape the cancer care experience for the elderly. Cancer treatment outcomes have been examined more closely than the overall cancer care experience.
In sum, the IOGA concept may be usefully defined as follows: IOGA refers to a coherent and coordinated set of services that are planned, managed and delivered to elderly cancer patients across a range of acute and primary care settings and by a range of collaborating care providers including oncologists, geriatricians, interprofessional team members and lay caregivers. The essence of IOGA is that elderly cancer patients and their loved ones receive whatever best-practice-based services they need, when and where they need them, in order to optimise health status and independence, and that all services are delivered from a whole-system perspective.
Discussion
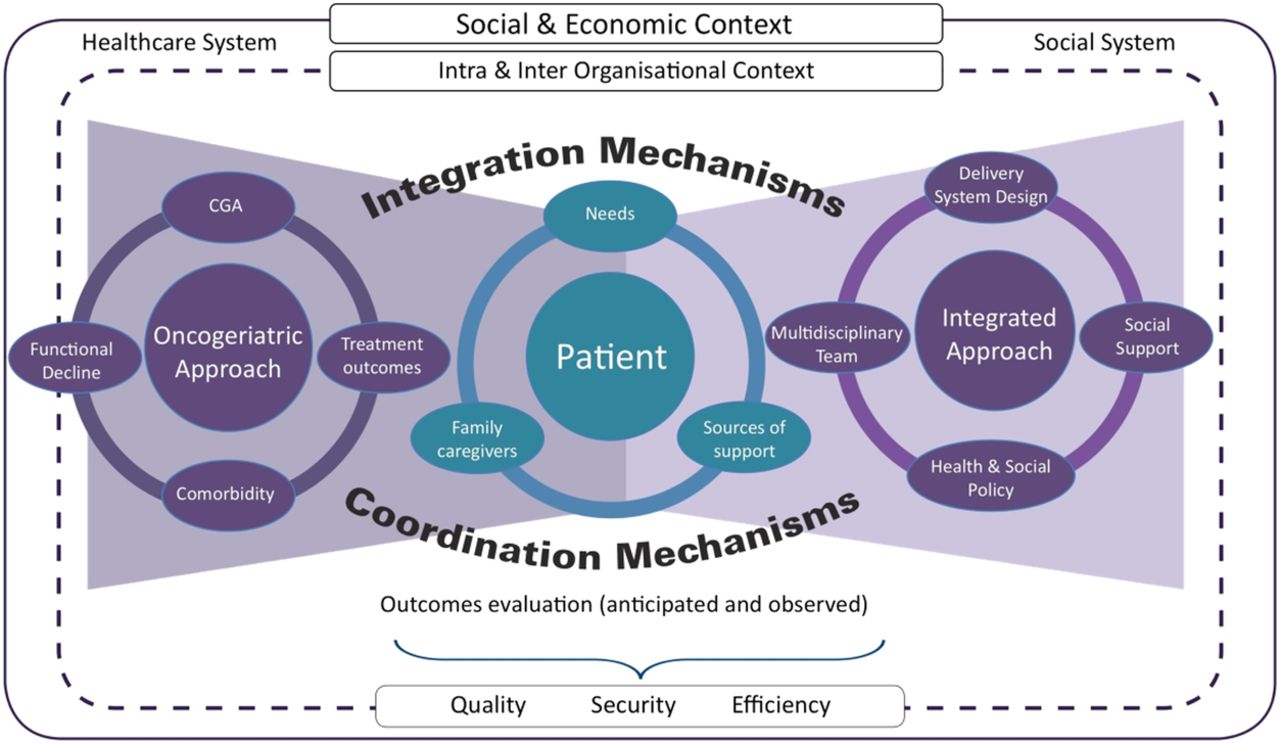
To date, IOGA mostly revolves around four main attributes, that is, CGA, functional decline, comorbidity evaluation and management, and treatment outcomes. More specifically, one challenge of the IOGA concept is to assess the relationships between cancer, comorbidity, functional decline and patient outcomes. While there is still uncertainty in the literature on the nature of these relationships, there is also great variability in the measurement methods used to evaluate functional decline as well as comorbidity. In fact, there is no consensus on a recommended assessment tool. The literature suggested actual interactions between comorbidity, functional decline and GA, but these were not supported by robust evidence. This can be attributed to the variability in research designs and in the instruments used to measure comorbidity and functional decline, as well as to the relatively recent emergence of the concept of geriatric oncology. Moreover, to date, geriatric oncology and an integrated approach to cancer care are two separate worlds, where coordination and integration mechanisms depend in part on patients’ capacity to activate them. As shown in the figure we developed on the basis of our literature review, IOGA is still mired in a two-discipline geriatric and oncology dilemma (figure 2).77

{kind=link}
{kind=link}
Integrated Oncogeriatric Approach (IOGA) Model
Beyond key issues like GA, functional decline and comorbidity, the complexity of cancer care among the elderly population justifies the need to focus attention and research on other aspects as well. Studies examining social support indicate that the lack of integration between health and social services complicates older patients’ cancer care experience, causing reduced tolerance to cancer treatment. The literature focused on social support systems may thus enhance the accuracy of knowledge on the complex nature of the disease by underlining its social dimension, as well as evaluating the anticipated quality, security and efficiency outcomes. Our resulting definition of IOGA espouses most of the elements of the CCM developed by Barr et al8 The CCM focuses on chronic disease management and has been used to develop a model for cancer care quality.78 However, while the CCM specifically supports multidisciplinary care, patient–professional relationships and outcomes, decision-makers also need strong scientific evidence upon which to base healthcare policies and programmes. Nevertheless, the CCM adequately supported our purpose of defining the IOGA concept, particularly with regard to: (1) self-management and decision support; (2) delivery system design and (3) healthcare policy.
Self-management and decision support refer to ‘a person's ability to manage the symptoms and the consequences of living with a chronic condition, including treatment, physical, social and lifestyle changes’.79 Self-management involves productive interactions between the patient and a multidisciplinary team to develop a collaborative care plan. Such interactions also enable decision support. Multidisciplinary teamwork ensures the coordination of patient-centred care and patients’ active role in their own care plan. However, in the literature, data on individualised management are limited to care attributes, toxicity grading and management of polypharmacy. The cancer treatment decision-making process remains limited to treatment options, although the role of patients, families and caregivers is acknowledged. Geriatric oncology teams must in the future encourage older patients to become proactive and feel involved in their own care plan and use of healthcare services. IOGA also aims to facilitate multidisciplinary coordination of biomedical and psychosocial care.78 Delivering an integrated cancer care system requires developing efficient networks between hospitals, primary healthcare facilities, human and social services and communities.76 Formalising such networks facilitates the seamless delivery of services76 and the comprehensive assessment of the patient's multiple evolving needs. Integrated cancer care in geriatric oncology revolves mainly around multidisciplinary teamwork and the use of GA. However, as previously emphasised, there is a significant lack of care coordination and of consensus on GA instruments. In terms of multidisciplinary teamwork, attention is focused mainly on the relationships between oncologists and geriatricians and less so on other professionals, reflecting a lack of recognition of the key position played by some professionals in accompanying patients on their cancer care pathway. Such attention may also reinforce professional silos, to the detriment of a whole-system approach. In geriatric oncology, GA has mainly been considered as an instrument to facilitate the cancer treatment decision-making process for the individual patient. The role of GA in care coordination for geriatric cancer patients remains underevaluated, in comparison with the geriatric non-cancer population.
An integrated model of cancer care also requires innovations at the policy level regarding three key components: (1) delivery system design; (2) clinical information systems and (3) multidisciplinary care. Decision-makers develop policies composed of norms, incentives and regulations intended to facilitate the implementation of these three components and avoid the classic trap of reproducing new professional silos. The decision-making process around the development of such policies is also important. The effectiveness of such policies depends on the extent to which stakeholders, and in particular healthcare professionals and patients, are included in the policy process. This ensures that the norms, incentives and regulations are evidence based. Including healthcare professionals and patients in the policy process requires establishing governance mechanisms that engage various healthcare stakeholders in the development of policies around integrated cancer care. Apart from calls for changes at the policy level, the geriatric oncology literature has not identified the specific changes required to foster integrated cancer care, nor has it properly defined the role of healthcare professionals and patients in the policy-making process.
Strengths and limitations of the study
Our study highlights the pioneering character of the multidimensional IOGA concept, for which the relationship between clinical and organisational attributes, on the one hand, and contextual antecedents, on the other, is not well understood. However, there are some weaknesses. While the CCM is widely recognised in the field of chronic disease management, in using this general model we may have left out other concepts that could contribute significantly to refining the IOGA concept. Also, because our literature search covered three broad domains (geriatric oncology, integrated service delivery and multidisciplinarity), certain relevant articles may have been missed in spite of our systematic approach. Indeed, this limitation was reflected in the keywords chosen, such that, for example, the term ‘comorbidity’ was not included in the search strategy, and consequently, the number of articles focusing on this important clinical aspect may have been under-represented in our sample. It may also be that our focus on identifying articles that could enhance our understanding of the IOGA concept led us to include studies that were not all equally robust. Finally, as stated by Rodgers80, while concepts are evolving, concept analysis can only provide a snapshot of a given concept. Our study must therefore be understood as a first attempt at clarifying, at a particular point in time, an emerging concept in the field of geriatric oncology.
Implications for clinicians and policymakers
By highlighting ways to envision IOGA conceptually, our analysis of its attributes, antecedents and consequents represents an attempt to provide guidance to clinicians and decision-makers in the design of improved healthcare delivery models. Our in-depth analysis of the IOGA concept underscores the lack of pertinent data for really understanding the nature of such a complex approach, the organisational and practice changes required, and the outcomes that may realistically be anticipated for older patients with cancer, as well as for professional and lay care providers. The scarcity of conceptual and empirical evidence focusing on IOGA may reflect researchers’ predominant interest in cancer treatment options adapted for older adults’ specific conditions. In this context, the result of our integrative review is disappointing, since it does not provide solid ground to clarify the IOGA concept. Nevertheless, our study contributes to worldwide efforts to improve care at the interface of cancer and ageing. It may constitute a starting point for promoters of comprehensive cancer care, since they will need a common understanding of IOGA if they are to work together to achieve it.
References
Footnotes
-
Contributors DT and KC led on conception design, conducted the literature search, interpreted and analysed the data, as well as wrote the manuscript. CT, SJ and JL contributed to the design and critically appraised the content of the manuscript. All authors approved the final version of the article submitted.
-
Funding This research received no specific grant from any funding agency in the public, commercial or not-for-profit sectors.
-
Competing interests None.
-
Provenance and peer review Not commissioned; externally peer reviewed.
-
Data sharing statement No additional data are available.