Article Text

Abstract
Objective To analyse the effectiveness of hospital-based case management (CM) in terms of patient-reported outcomes.
Design Randomised controlled trial allocating participants 1 : 1 to either a CM intervention or a control group. Allocation status was evident to participants and case managers, but blinded to researchers.
Setting Patients were recruited at a Danish surgical department where the case managers were situated.
Participants Colorectal cancer patients who were to undergo further investigation or treatment. Exclusion criteria were participation in another study, poor Danish language skills or apparent cognitive impairment. 140 participants were randomised to each group. Recruitment period was 11 March 2009 to 29 December 2010.
Interventions Control group patients had usual care. Intervention group patients had usual care supplemented by hospital-based CM started at first visit to the out-patient clinic (before treatment start) and ended 4 weeks after completed cancer treatment. CM was conducted by nurse case managers who undertook care pathway supervision, information dissemination to health professionals and outreaching patient support.
Outcome measures Patient-reported global quality of life measured with the EORTC QLQ-C30 and eight ad hoc, piloted patient evaluation items assessed at eight, 30 and 52 weeks after randomisation.
Results The two groups were comparable as to questionnaire response rates and completed scales/items. There were no statistically significant group differences on any of the health-related quality of life subscales at eight, 30 or 52 weeks. In patient evaluations, all point estimates favoured CM at week 8 and 30; at week 52, 6 of 7 estimates favoured CM.
Conclusions We found no evidence that CM influenced colorectal cancer patients’ health-related quality of life. Patients allocated to CM evaluated their care more positively than patients receiving usual care.
Trial registration Clinicaltrials.gov identifier: NCT00845247.
This is an open-access article distributed under the terms of the Creative Commons Attribution Non-commercial License, which permits use, distribution, and reproduction in any medium, provided the original work is properly cited, the use is non commercial and is otherwise in compliance with the license. See: http://creativecommons.org/licenses/by-nc/2.0/ and http://creativecommons.org/licenses/by-nc/2.0/legalcode.
Statistics from Altmetric.com
Article summary
Article focus
-
Case management (CM) models are increasingly engaged in healthcare systems to improve coordination and continuity of care. Most programmes are based on case managers who are experienced nurses engaged full-time to undertake coordination and support in relation to individual patients having complex healthcare needs.
-
Danish hospital departments treating cancer patients have been committed to deploy case managers to improve coordination and continuity of care. However, scientific evidence of the effect of CM in this context is scarce.
-
This article presents results from a randomised controlled trial (RCT) of nurse CM for colorectal cancer (CRC) patients.
Key messages
-
The manual-based CM intervention was conducted by two experienced nurses with regard to CRC care, the patient perspective and the Danish healthcare system. Main CM activities were care pathway supervision and optimisation, dissemination of patient-specific information to general practitioners and other involved healthcare personnel, and outreaching patient support.
-
The CM intervention did not affect patients’ health-related quality of life as measured by the EORTC QLQ-C30.
-
The CM intervention showed a tendency to improve patients’ evaluations of care received.
Strengths and limitations of this study
-
The CM intervention was manual based, pilot tested and analysed in an RCT.
-
The RCT was implemented at only one department with the consequence that patients potentially were aware about the purpose of the trial and their allocation.
Introduction
Treatment modalities for cancer evolve rapidly and cancer survival rates are rising modestly,1 but cancer patients still suffer from reduced health-related quality of life (HRQoL) due to their disease, its treatment and the effects of existential concerns.2 ,3 Many cancer patients experience cancer care as episodic and incoherent as to treatment and care, information provided and relationship with health professionals.4–7 Importantly, some studies have found a positive correlation between patients’ evaluations of their care and their HRQoL.8 ,9
Case management (CM) is often recommended as a method to improve coordination and continuity of care for individual patients having complex care needs. CM is usually conducted by a nurse, the case manager, who is engaged solely to function as a consistent and proactive cross-disciplinary member of the healthcare team.10
CM may be an effective method to improve coordination and continuity of cancer care and to improve cancer patients’ HRQoL. However, the effectiveness of CM in cancer care has been sparsely studied.11 In the present study, we tested the hypothesis that hospital-based CM during the treatment period would improve colorectal cancer (CRC) patients’ HRQoL and their evaluations of care.
Materials and methods
Study design
Randomised controlled trial (RCT) allocating CRC patients to a CM intervention group or a control group (ratio 1 : 1).
Setting
The Danish healthcare system is primarily tax-financed and grants Danish citizens free access to general practitioner (GP) and public hospital services. Almost all Danes (98%) are listed with a general practice. The GP is a gatekeeper with regard to the patient's referral to specialist services and functions as a key healthcare coordinator outside the hospitals.12
The Surgical Department P, Aarhus University Hospital, Denmark, treats all categories of CRC patients, including those who suffer from locally advanced or recurrent disease.
Participants
During the inclusion period from 11 March 2009 to 29 December 2010, all patients at Department P were assessed for inclusion. We included patients with a diagnosis of CRC or ‘a highly probable diagnosis of CRC’ who were to undergo further investigation or treatment at Department P. Exclusion criteria were participation in another study (see the Discussion section), poor Danish language skills or apparent cognitive dysfunction.
Control: usual care
Control group patients were treated and cared for as usual. No designated health professional overlooked the coordination of health services for this group and they did not receive telephone calls to systematically assess their well-being and the coordination and continuity of their care. In accordance with a paragraph in the Danish Health Act,13 all control group patients were given the name and a phone number on an employee at Department P to grant them easy access to the department during the treatment period.
CM intervention
The main aims of the CM intervention, which was conducted supplementary to usual care, were to streamline individual patients’ care pathways and improve their well-being and experiences of care. Two experienced nurses were employed from January 2009 to May 2011 to work principally as case managers. They initially went through 2 months of combined additional training and pilot testing of the manual-based CM intervention and its appertaining checklists. The case managers had their office at Department P, worked daytime and weekdays only, were introduced as members of the multidisciplinary team (MDT) and they attended all MDT meetings where most patients had their cancer staged and treatment options discussed.
A detailed manual, which was pilot tested before the trial, chronologically described the case managers’ duties. As soon as possible after randomisation, the case manager scheduled a meeting with the patient to provide detailed information about the CM services and availability. In addition, the case manager made a formal assessment of the patient's medical and non-medical condition, his or her expectations regarding care, and his or her knowledge about the disease and care. An ad hoc developed needs assessment checklist was used to guide the conversation.
Throughout the period of treatment, the case manager regularly (∼every fortnight) telephoned the patient to assess his or her biopsychosocial status and screen for barriers to optimal care related to coordination and awareness of the care plan. Potential inadequacies were addressed by involving relevant health professionals and by increasing the frequency of outreach telephone calls.
Patient-specific information was passed on to the GP and other relevant health professionals initially and at transitions between care settings.
Most patients met the case manager at their first meeting in the outpatient clinic which took place a few days after the patient's primary colonoscopy or for patients referred from another CRC specialist to Department P at the patient's first encounter in the Department. The duration of active CM varied between patients but did not terminate before 4 weeks after the patient had completed planned CRC treatment. There was no formal time at which patients could no longer exercise their option to contact the case manager by telephone.
Online supplementary figure S1 provides an overview of the CM intervention and the usual care in a Pat plot(figure 1).14 The CM intervention was pragmatically designed and operationalised the case manager's function as described in the Danish Generic Model for Care Pathway Programmes.15 The CM intervention and the methods and feasibility of the trial have been described in detail elsewhere (paper submitted to BMC Health Services Research 9 December 2011).

Overview of the interventions.
Outcome measures
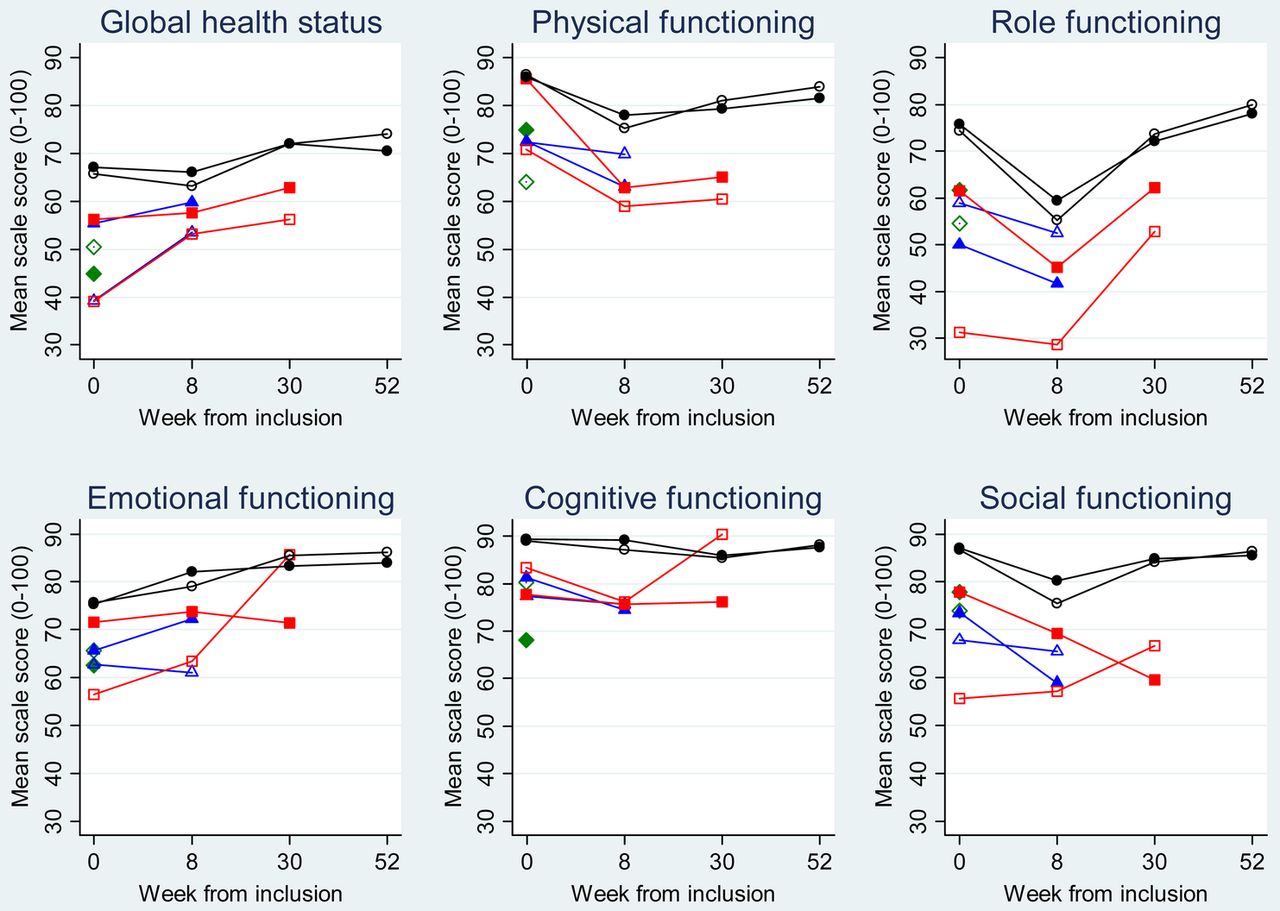
HRQoL was assessed with the use of the Danish version of the European Organisation for Research and Treatment of Cancer Core Quality of Life Questionnaire V.3.0 (EORTC QLQ-C30), which is a validated, cancer-specific, 30-item questionnaire measuring HRQoL on: one global health status scale, five functioning scales and nine symptom scales.16 ,17 The primary endpoint of this study was the global health status scale. The secondary endpoints were scores on the functioning scales: physical, role, cognitive, emotional and social functioning.
EORTC QLQ-C30 scores were calculated according to the scoring manual.18 Thus, a continuous scale score ranging from 0 to 100 was calculated if the patient had answered at least half of the items of the scale. A score of 100 indicated the highest functioning. For interpretation of EORTC QLQ-C30 results we set 10 units as the minimally relevant scale contrast regardless of the subscale.19 ,20
Eight ad hoc items from a piloted questionnaire were pre hoc selected as the primary patient-evaluation endpoints (see table 3). Six items meant to determine information and support from health professionals and continuity of care were answered using the following response categories: ‘Completely agree’, ‘Agree’, ‘Do not agree’, ‘Completely disagree’ and ‘Do not know/Not applicable’. Two items asked the patients to assess the quality of care at the surgical department and in general. These items used the following response categories: ‘Excellent’, ‘Very good’, ‘Good’, ‘Less good’ and ‘Bad’.
Follow-up
HRQoL and patient evaluations were assessed 8, 30 and 52 weeks after the patient's inclusion with copies of the same questionnaire that featured the EORTC QLQ-C30 items plus 64 other items. The questionnaires and the reminders to non-responders (after 3 weeks) were sent by ordinary mail. Non-response 6 weeks after the time of the initial follow-up questionnaire prompted a reminder phone contact. HRQoL was also assessed at baseline using a questionnaire handed out at the hospital.
Sample size
Power calculations on the global health status scale revealed that we needed responses from 116 patients in each group (power of 90%, two-sided significance level of 5%, 1 : 1 allocation) to detect 10 units of difference between groups. Due to inevitable drop-out, we aimed at including a total of 280 patients.
Randomisation and allocation concealment
The two case managers undertook recruitment in turns. After an assessment of inclusion and exclusion criteria, potential patients were informed about the trial. Those who were willing to participate were asked to fill in a consent form and the baseline questionnaire. Patients returning these documents were randomised 1 : 1 by an independent secretary using the minimisation technique21 and the SiMin software.22 To ensure comparable groups in terms of characteristics possibly associated with the outcomes, the following stratification factors were used: gender (male/female), cancer type (rectal cancer/colon cancer) and age (<65/65–79/>79 years). A random factor of 1 : 4 was used (ie, allocation included 20% randomness).
Group assignment was evident to the patients and the case managers, but was blinded to the researchers.
Analyses
Analysis of covariance (ANCOVA), which in effect adjusts each patient's follow-up score for his or her baseline score,23 was used to calculate the group difference on each of the HRQoL subscales at each time of follow-up. Analyses were accompanied by graphical presentations of the groups’ mean scores stratified by the patients’ last consecutive questionnaire response. These longitudinal graphical presentations served two purposes: To provide an overview of all the data at the same time; and to suggest whether any data complexity might bias the statistical analyses.24
The patient evaluation answers were dichotomised (‘Completely agree’ vs ‘the rest’ and ‘Excellent’ plus ‘Very good’ vs ‘the rest’). The positive proportion of answers to each item was compared at each time of follow-up using a generalised linear model with log link for the Bernoulli family and robust variance; relative differences are presented as prevalence proportion ratios (PPRs).25
All analyses were conducted according to the ‘intention-to-treat’ principle, that is, patients were kept in the analyses regardless of their final diagnosis and exposure to CM (decided by duration of treatment). Statistical significance was set at p≤0.05 and results should be interpreted in awareness of multiple comparisons.
To address potential attrition bias caused by uneven attrition in the two groups,26 sensitivity analyses was conducted, that is, data were analysed with adjustment for the minimisation variables and categories. We did not impute missing data because most missing data were HRQoL and patient evaluations (outcome data) from dead persons.
Primary endpoints were tested for subgroup-treatment effect interaction as to cancer type, gender and age using same categories as used in the minimisation.27 Due to the multiple testing, effect measure modification should be present at minimally two time points to be accepted as an indication of a subgroup-treatment effect.
All analyses were conducted with the use of Stata V.11.2.
Ethics
The project was ethically acceptable to both control group and intervention group patients because diagnostics and treatment were unaffected, and we did not know whether CM was superior to usual care. According to the Danish Research Ethics Committee System,28 the trial was not a biomedical intervention and did not need the ethics committee's approval. This was confirmed by correspondence with the chair of the regional ethics committee. The Danish Data Protection Agency approved the research database (J.nr. 2008-41-2932). The RCT was indexed at www.clinicaltrials.gov (ID number: NCT00845247).
Results
Flow of participants
We assessed 532 patients for inclusion and included 280 patients. Online supplementary figure S2 shows the reasons for non-participation and the group-wise flow of patients (figure 2). Table 1 shows that the patients in the two groups were similar as to age, gender, disease characteristics and self-reported variables at baseline. The CM group had marginally higher mean baseline HRQoL scores than the control group, except for cognitive functioning.
Participants’ characteristics

Trial profile
Online supplementary figure S2 shows similar response rates in the two groups at 8, 30 and 52 weeks. Attrition occurred during the trial. Mortality 52 weeks after inclusion was higher in the CM group (31 patients) than in the control group (20 patients), but this difference was not statistically significant and the two groups appeared almost similar in terms of the remaining patients’ characteristics (not shown). Importantly, no clinically significant differences between the unadjusted and the adjusted estimates appeared.
HRQol
Table 2 presents the EORTC QLQ-C30 mean baseline and follow-up scores at each time of follow-up and the ANCOVA-calculated differences between the two groups. No statistically significant difference between groups appeared on any subscale at any time point.
Mean baseline and mean follow-up scale scores and ANCOVA-calculated group differences
Online supplementary figure S3 offers a visual representation of the EORTC QLQ-C30 scale scores by group and over time. Seventy-one per cent of all participants (103 control group patients and 95 CM patients) answered the baseline questionnaire and all answered the three follow-up questionnaires (complete follow-up; black markers and lines). Online supplementary figure S3 shows that non-random drop-out applied to most scales, that is, the non-responder group had statistically significantly lower scores at the assessment prior to non-response than the responder group. The mean scores of the two subgroups characterised by complete follow-up appeared not to differ, and the profiles of the mean scores changed similarly over time. The partial follow-up profiles appeared less uniform, but plots were based on a maximum of 20 responses per group (figure 3).
{kind=link}
{kind=link}
{kind=link}
Average EORTC QLQ-C30 scale scores by group and by length of follow-up.
Patient evaluation of care
Table 3 shows the dichotomised patient evaluations at week 8, 30 and 52. The two groups were almost identical as to numbers of ‘Don't know/ Not applicable’ answers and skipped items so these ‘responses’ were omitted from analyses. The PPRs of 23 of 24 items favoured the CM group. Five, three and zero items differed statistically significant at week 8, 30 and 52, respectively.
Numbers and proportions () of patients taking a very positive or less positive stand, and the group differences.
We found no statistically significant subgroup-treatment effect interaction as to the global quality of life-scale or the patient evaluation items.
Discussion
Statement of principal findings
We found no effect of a manual-based CM intervention on patients’ global health status or their functioning as assessed from the EORTC QLQ-C30 questionnaire. Patients of the CM group answered almost all (23 of 24) patient evaluation items more positively than the control group patients. The items regarding ‘the experience of being continuously followed by a doctor or a nurse’, and ‘confident about going home after surgery’ seemed, in particular, to be more positively evaluated by CM patients than by the control group. We found no statistical indication that any subgroup (gender, age or cancer type) benefited differently from CM.
Strengths and weaknesses
The principal strength of this study was the comprehensive, manual-based CM intervention performed in the RCT design. A statement of the case managers’ activities from the CM records and a debriefing of the case managers indicated that the CM intervention was conducted according to the manual (reported in a paper submitted to another journal).
Another strength was the use of the EORTC QLQ-C30, which is the most used validated HRQoL instruments in CRC settings and available in Danish. EORTC QLQ-C30 focuses on domains relevant to most cancer patients and minimally clinically relevant cross-sectional contrasts have been proposed to guide the interpretation of findings.19 In this study, all the confidence limits of the difference estimates were within ±10 units (after round off). We are therefore convinced that we do not reject a clinically significant effect of CM.
Patient evaluations were assessed using ad hoc items which may be a potential weakness compared with instruments with established measurement properties and ‘benchmark scores’. The use of ad hoc items was deemed necessary because existing relevant measures were found to focus on either the inpatient or the outpatient setting and not on care across care interfaces. We argue that it is acceptable to analyse non-validated items in a trial as long as items are presented by their exact wording and analyses are conducted item by item.
This RCT was implemented with randomisation at the patient level and with both patient groups being treated at the same department at the same time. We acknowledge that an intervention based on visibility and communication would have been more validly tested in a cluster-randomised trial with randomisation performed at department or hospital level. Anyway, the success of a cluster randomised trial relies on its inclusion of several treatment units which was hindered by our budget.29 The two main limitations caused by the single unit set-up were: (1) patient evaluations might have suffered from information bias because patients had information about the purpose of the trial and they were unblinded to group assignment. To reduce information bias caused by patients’ experience of ‘losing’ or ‘winning’ the randomisation procedure, patients were neutrally informed about the purpose of the trial at recruitment. In addition, we believe patients over time ‘forgot’ about taking part in a randomised study for which reason the patient evaluations were unaffected by information bias. (2) The usual staff noticed ‘effective’ CM actions which they tried to ‘copy’ to improve control group patients’ care (spill-over effect). It is very unlikely that control group patients had ongoing support and supervision, because this would require organisational restructuring (eg, revised work plans) or extra manpower, which did not take place.
A known problem when assessing patient-reported outcomes is missing data and, as for HRQoL-data, non-random dropout24 due to deaths. Importantly, although more CM patients than control group patients were dead at 52 weeks, online supplementary figure S3 does not indicate that we have overlooked a positive effect of CM on the global health status, physical functioning or the role functioning subscales due to non-random drop-out. On the other hand, the emotional functioning, cognitive functioning and social functioning differences might have been biased favouring the control group as a consequence of excess deaths in the CM group. Thus, online supplementary figure S3 insinuates that the CM patients who withdrew between weeks 30 and 52 might already have experienced diminishing functioning on these scales at 30 weeks.
Although the baseline questionnaire was returned before the concealed randomisation, CM patients had higher mean baseline scores on five of the six EORTC QLQ-C30 subscales than the control group patients. Importantly, ANCOVA appropriately handles such ‘by chance problem’ without introducing bias.23
Despite multiple comparisons, p≤0.05 was generally used as the level of statistical significance. Importantly, even if we had adjusted the p values to counteract the problem of multiple comparisons we would still report the tendency towards improved patient evaluations in the CM group.
Generalisability
Non-participants and participants differed in terms of cancer type and age. The group of CM participants counted statistically more rectal cancer patients than the usual care group and they were slightly, but statistically, significantly older. The primary reason for this was that another study included patients suffering from primary non-metastatic rectal cancer, who we thus could not include.
The results can be generalised to a wider group of cancer patients, primarily for two reasons: (1) interaction analyses indicated that no particular subgroup (gender, age or cancer type) benefited from CM and (2) previous research has shown that patients suffering from different cancer types face identical psychosocial problems and healthcare system-related barriers.30 ,31
Comparisons with other studies and meaning of the study
The present study found that CM improved patient evaluations of care even if attrition over time reduced the power of the analyses. Improved patient evaluations have also been reported in other CM RCTs.32–34 The consistent finding of improved patient evaluations despite the use of different measures is important because patient evaluations may be seen as a quality criterion at par with ‘technical quality’ and objective outcomes.35 Observational and qualitative studies including CRC patients have found that patients’ care evaluations correlate positively with their HRQoL.8 ,9 Anyway, based on the ‘neutral findings’ in present and previous CM trials,32 ,36 ,37 one may speculate whether it is possible for case managers to improve cancer patients’ HRQoL during the treatment phase. One explanation may be that CM does not alleviate the impact of cancer symptoms, adverse treatment effects and the existential concerns on patients’ HRQoL. Another plausible explanation is poor responsiveness of the existing HRQoL instruments in the ‘new’ settings they have been applied.38 Retrospectively, we regret that we did not consider including an anchor item in our questionnaire for the purpose of responsiveness analyses of the EORTC QLQ-C30 in the setting and context of present trial.
Unanswered questions and future research
This CM study focused on patient-reported outcomes. CM may also be implemented to reduce the amount of ‘inappropriate’ healthcare services (duplicated services, unplanned readmissions and out-of-hours services) or if it enhances information transfer and professional collaboration around the patient. Yet, these issues remain to be explored.
Conclusions
In this RCT of CRC patients undergoing treatment, we found no impact of hospital-based CM on patients’ HRQoL at week 8, 30 or 52 after inclusion, but several patient evaluation items were statistically significantly improved by CM, and a tendency towards better patient evaluations in the CM group than in the usual care group was observed.
Acknowledgments
The authors wish to thank all patients and the staff at Surgical Department P, Aarhus University Hospital, Aarhus, Denmark and all the GPs who filled in the questionnaires. We also wish to thank IT-officer Hanne Beyer for creating research databases and statisticians Ineta Sokolowski and Morten Fenger-Grøn for discussions regarding the analyses. Also thanks to Professor Frede Olesen for assistance developing and implementing the RCT.
References
Supplementary materials
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
Files in this Data Supplement:
- Data supplement 1 - Online figure
Footnotes
-
Contributors CNW is the guarantor of the paper, design of the study, handled the data and the statistical analysis and drafted the manuscript. JS and PV designed the study and drafted the manuscript. All authors read and approved the final manuscript.
-
Funding This study was funded by the Danish Cancer Society, the Novo Nordic Foundation, the Danish Council for Independent Research – Medical Sciences, and the Quality and Continuing Training Council for GPs in the Central Denmark Region.
-
Competing interests None.
-
Ethics approval The Danish Data Protection Agency approved the research database (J.nr. 2008-41-2932).
-
Provenance and peer review Not commissioned; externally peer reviewed.
-
Data sharing statement There are no additional data available.