Article Text

Abstract
Objectives To explore experiences of UK-based South Asian and White patients with diabetes in relation to their support systems for and barriers to diabetes management.
Design Qualitative study (semistructured interviews analysed using a form of Interpretative Phenomenological Analysis).
Participants 20 outpatients with diabetes (12 British South Asians and 8 British Whites) with either good or poor glycaemic control.
Setting Hillingdon Hospital, Uxbridge, UK.
Results Qualitative analysis revealed distinct themes for the two ethnic groups. For the South Asian participants, challenges surrounding diet management and social stigma attached to having diabetes were the two predominant barriers to effective diabetes management. Support from immediate family members was commonly reported as a strong support system for optimising diabetes management by the South Asian sample in addition to the perceived positive impact of religion (healing power of prayer), the valuable informational support from their diabetes-care team, patient leaflets and diabetes magazines. Similar to the South Asians, adhering to dietary recommendations was the most difficult aspect of diabetes management for the White participants followed by the inconveniences surrounding injecting insulin. The hospital diabetes-care team was considered as the most effective support system for diabetes management by the White sample and interestingly, this was the only dominant theme in their reported sources of support.
Conclusions Both South Asian and White participants emphasised adherence to dietary recommendations as the most difficult aspect of living with diabetes. In addition, social stigma attached to diabetes was a prominent concern among South Asian participants that seemed to have a significant negative impact on their diabetes control and overall management. Given South Asian patients’ reliance on their family for the management of their condition, interventions targeting improved diabetes outcomes in this population may prove more successful if they are designed to involve significant family members.
- Diabetes
- South Asians
- Stigma
- Family
- Religion
- Diet management
This is an open-access article distributed under the terms of the Creative Commons Attribution Non-commercial License, which permits use, distribution, and reproduction in any medium, provided the original work is properly cited, the use is non commercial and is otherwise in compliance with the license. See: http://creativecommons.org/licenses/by-nc/2.0/ and http://creativecommons.org/licenses/by-nc/2.0/legalcode.
Statistics from Altmetric.com
Article summary
Article focus
-
UK-based South Asians (SAs) develop diabetes significantly early in life and have a higher mortality risk compared with their British White counterparts. Research into glycaemic control in SAs with diabetes has shown either similar or worse control compared with Europeans.
-
Qualitative research into the problem of diabetes in British SAs has often only focused on SAs from a particular health centre without comparing them to White patients from the same health setting. Without these comparison data, it becomes difficult to compare the experiences of diabetes management (DM) between these two communities who are being cared for in the same clinical setting.
-
The primary objective of this qualitative study was to explore barriers to and support systems for optimising DM in British SA and White outpatients with optimal and suboptimal diabetes control.
Key messages
-
SA patients reported diet management and social stigma related to diabetes as their primary barriers to effective DM. Although, support from the immediate family was a strong support system for this group, younger SAs reported significant cultural pressure from their families to hide their diabetes from others.
-
Given the level of involvement of family members in SA patients’ DM, interactions between the patient, their family members and healthcare professionals in patients’ preferred language of communication could help to ensure that significant others also receive clear messages from health experts regarding what is best for patients’ DM.
-
Adhering to dietary recommendations and inconveniences surrounding injecting insulin were reported as the most difficult aspects of DM by the White patients. The hospital diabetes care team was considered the most effective support system by this group.
Strengths and limitations
-
Strengths included recruiting British SAs and Whites from the same health setting in the UK. Previous qualitative research into the problem of diabetes in British SAs has often only focussed on SAs from a particular health centre without comparing them to White patients from the same health setting. Without these comparison data, it becomes difficult to compare the experiences of diabetes management between these two communities who are being cared for in the same clinical setting.
-
We were unable to involve patients from other hospitals as participants because we were primarily interested in the diabetes community from Hillingdon Hospital. Involving patients from other hospitals would have allowed for a more generalizable sample.
The alarming rise in the incidence of chronic diseases and the marked differences in treatment outcomes across various ethnic groups are leading the healthcare community to consider the potential impact of patients’ social and cultural environment on their disease management.1–3
South Asians (SAs) form the largest UK ethnic minority group representing almost 4% of the entire UK population.4 Age-standardised prevalence of type 2 diabetes is estimated to be between three and five times higher among the British SAs compared with the UK White population.5–9 Almost 20% of British SAs have type 2 diabetes compared with 3% of the general population.10 Diabetes profiles of UK SAs have consistently shown that they develop diabetes significantly earlier in life, endure diabetes-related complications for longer and have a higher mortality risk compared with their White counterparts.11–13
UK research into glycaemic control in SAs with diabetes has shown either similar14 or worse control15–17 in this population compared with Europeans. Factors affecting the quality of diabetes control may include aspects of patients’ self-care as well as clinical management of the condition therefore, understanding people's perceptions of barriers that prevent them from achieving their glycaemic targets and support systems that assist them in optimising diabetes management (DM) may contribute towards designing and targeting diabetes interventions more effectively.
Past research efforts into understanding poor diabetes control in British SAs have highlighted various sociocultural factors including a diet rich in sweets and saturated fats.18–21 Food is an integral part of socialising in the SA community and not only are hosts expected to serve a variety of rich foods but it would be impolite to refuse.18 ,21–23 Language could be a major barrier to communication with healthcare professionals for British SAs. Estimates for British SA communities suggest that fewer than 50% would reach a ‘survival level’ of competence in English 24 and older British SAs, particularly women, are less likely to speak English.25 Diabetes care teams may struggle to provide culturally competent healthcare to British SAs who have poor English.26 ,27
Qualitative research into the problem of diabetes in British SAs has often only focused on SAs from a particular health centre without comparing them to White patients from the same health setting.18–21 Without such comparison data, it becomes difficult to compare the experiences of DM between patients from these two communities who are being cared for in the same clinical setting. The present study was a follow-up to two quantitative studies involving adult diabetes outpatients conducted at Hillingdon Hospital (UK),28 which together demonstrated significantly poorer glycaemic control (glycosylated haemoglobin or HbA1c) in SAs compared to other (mainly White) outpatients with diabetes. The primary objective of this qualitative study was to explore barriers to and support systems for optimising DM in samples of British SA and White outpatients with optimal and suboptimal diabetes control.
Research design and methods
Sample recruitment and characteristics
Participants for this study were recruited from Hillingdon Hospital's outpatient clinic list as part of a larger HbA1c and ethnicity study. Ethical approval was obtained from the Hillingdon Local Research Ethics Committee. Potential participants (N=815 patients including 585 SAs and 230 Whites) were sent postal invitations. Patients consenting to interview were asked to specify their preferred language for the interview from English, Hindi or Punjabi. Most recent HbA1c levels were obtained for each consenting patient and these values along with other demographic data were used to identify potential interviewees.
In all, 92 patients (SA=48, Whites=44) expressed interest in the interview study. The majority of SAs identified themselves as Hindus (n=19) followed by Sikhs (n=15), Muslims (n=11), Christians (n=2) and one Buddhist. Most White patients were Christians (n=34) while eight reported having no religion. There were more men than women in both sample groups (SA: 62.5% men, Whites: 70.5% men). SAs were younger (mean 52.6 years, SD=13.3) than the Whites (62.4 years, SD=11.7; p<0.01). Duration of diabetes was similar in both groups (11 years, SD for SA=8.3 and SD for Whites=10.6) but SAs reported a younger age of diagnosis of diabetes (mean 41.4 years, SD=12 vs 51.3 years and SD=15.3; p<0.01). The majority of patients in both sample groups had type 2 diabetes (SA: 91.7%; Whites: 97.7%). Of all SA with type 2 diabetes (n=44), the largest proportion of participants reported being on a ‘tablet only’ regimen (n=20, 45.5%) followed by ‘insulin only’ (n=12, 27.3%). For the Whites with type 2 diabetes (n=43), most participants were using ‘insulin only’ (n=13, 30.2%) followed by those who were on a ‘tablet and diet’ regimen (n=12, 27.9%). There was no significant difference in mean HbA1c values between the two ethnic groups of volunteers.
Of all patients who agreed to participate in the larger HbA1c and ethnicity study (n=108), only 16 (SAs n=8, Whites n=8) actively declined to take part in the interviews. SA non-participants were younger than their White counterparts (median age 60.5 years, IQR=26.25) vs 62.0 years, IQR=21). White non-participants had had diabetes for a longer period compared with their SA counterparts (diabetes duration (median) 12.5 years, IQR=22.25 vs 10.6 years, IQR=9). The majority of patients in both groups of non-participants (87.5%) had type 2 diabetes. There were no significant differences in the mean HbA1c value of SA (7.5%, SD=0.7) and White (7.1%, SD=1.1) non-participants (n=8 in each ethnic group).
Selection of interviewees
Twenty people with diabetes (SAs=12; Whites=8) were interviewed (figure 1). Ten of the 12 SAs were first-generation migrants to the UK. We decided to include SA and White men and women with optimal and suboptimal glycaemic control (ie, low or high HbA1c values, respectively) using a variety of treatment regimens in order to explore their experiences of having and treating diabetes. At the time of the study, HbA1c values >7.5% were classified as suboptimal29 and patients with HbA1c >7.5% were compared with those who had HbA1c values of ≤7.5%. Four SA (two men and two women) with type 1 diabetes were included for interviews to explore barriers and support systems surrounding diabetes care in this subgroup and understand whether there were any overlapping themes with the SA subgroup of patients with type 2 diabetes. No White patients with type 1 diabetes were included as there was only one such patient in the sample.

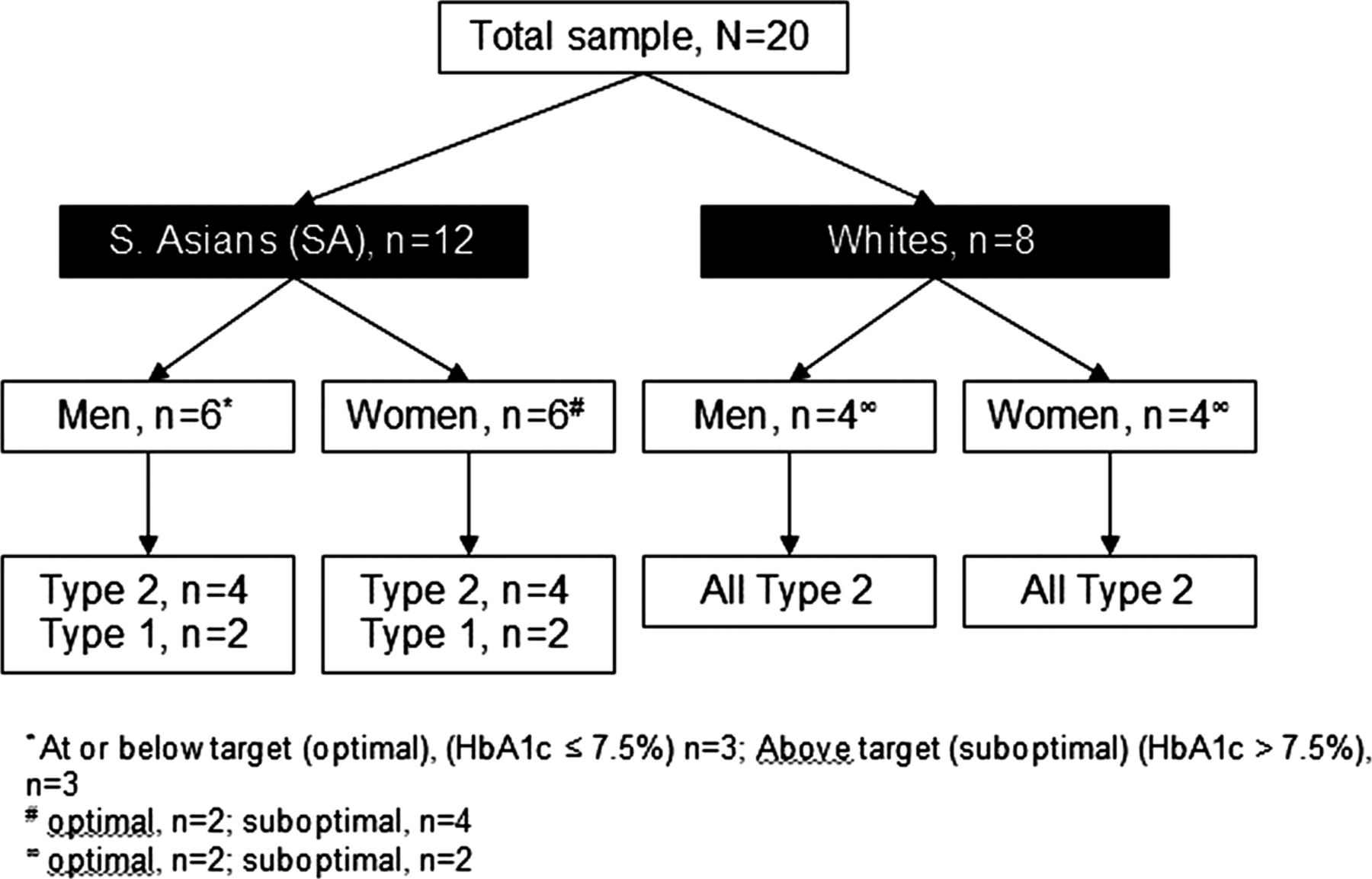{kind=link}
Distribution of participants in the qualitative study.
Qualitative procedure and analysis
The interviews (n=20) were semistructured and lasted for approximately an hour. All interviews were face-to-face, audio-recorded and later transcribed verbatim into English. Interviews were conducted by the first author (HS) at the hospital and arranged to coincide with patients’ regular hospital appointments. HS is trilingual in Hindi, Punjabi and English and able to switch language within interviews as SA patients often wished to do. A form of Interpretative Phenomenological Analysis (IPA)30 ,31 was used to analyse the interview data. In keeping with the epistemological approach of IPA we did not derive a priori hypotheses and instead embraced the aim of finding a window in participants’ phenomenological sense-making in relation to diabetes.
Interview data were analysed by HS in the following stages: (1) transcripts were read for initial observations; (2) themes were identified for each interview; (3) summary tables were produced for each of the interviewees based on the identified themes. Attempts were made to identify whether any relationships existed between the various themes for each participant.; (4) summary tables for all participants with optimal and suboptimal glycaemic control in each of the four sample groups (ie, SA men and women, White men and women) were combined; (5) consequently, common themes representing barriers and support systems for SA and White participants were identified. Emergent themes at various stages of the analyses2–5 were reviewed and confirmed by research supervisors (MC and CB).
To maintain anonymity, SA participants, in the results section, have been referred to as SAm 1–4 (for men) and SAw 1–4 (for women). Similarly, the White participants have been identified as Wm (men) and Ww (women).
Results
SAs participants: perceived barriers to DM
Difficulties with diet management
All SA participants felt that adhering to dietary restrictions was very difficult.
▸ “The most difficult thing is that you have to stop eating sweet things…in our community, eating sweets is very common because it is always one festival or the other … there is always a box of sweets in the house.” (SAm 3, type 2)
▸ “It is very tempting when nice sweets are there at home but I don't touch them. I can't eat them …I should not eat them. That is the most difficult thing. I never touch.” (SAm 2, type 2)
▸ “Oh God! It is difficult, isn't it!? All the time you have think whether a particular food item has sugar in it or not…isn't it? So, all the time you have to think what you can and cannot eat.” (SAw 4, type 2)
SA women with type 1 diabetes who had young children found it especially difficult to manage their diet as they often found themselves ‘finishing off’ after their children.
▸ “Occasionally I would like to have a little bit of chocolate. Since I have had children, I think I find it more difficult … if they want ice cream or something or they leave the crisps for you or they leave sweets for you.” (SAw 6, type 1)
Social stigma and other cultural pressures
Almost all SAs reported that there were enormous social and cultural pressures from within their community that made it harder to manage diabetes. Patients chose to compromise their diet and treatment regimen in order to comply with their community's social etiquette and avoid the social stigma surrounding their condition.
▸ “The other reason is the culture of eating sweets in our Indian community … sometimes you just eat it, sometimes someone urges by saying, “come on just eat it today there is a function in the house” … I do refuse sometimes but sometimes, you feel like taking it.” (SAm 3, type 2)
▸ “If we refuse to eat some food items people think that we are too hard to please. Many times they will say ‘Oh, it's not going to harm you if you have this bit here’ and if you do not eat it when they offer, it is a really bad thing.” (SAm 4, type 2)
▸ “Yes, it is a bit bad … I mean you try and hide your illness; no one should know that you have any illness.” (SAm 1, type 2)
▸ “‘I got a shock when they put me on insulin … I asked doctors to give me two weeks to decide whether I want to start taking insulin or not , it is not difficult in the personal sense … it is more because of our culture and community. People look at you and go, ‘Oh God! Is he taking insulin?’ … people feel that you have a very dangerous kind of disease …it is really embarrassing.” (SAm 4, type 2)
Stigma attached to having diabetes seemed to be considerably greater for individuals (especially women) who were younger and unmarried. Diabetes was viewed as a sign of physical inadequacy, which could seriously impair marriage prospects in a social system where family elders arranged the majority of marriages. It was noted that immediate families of patients often contributed to this stigma by encouraging or even forcing individuals not to disclose their diabetes to others.
▸ “The biggest obstacle is the stigma around diabetes. There are not a lot of people, family friends who know that we (brothers) are diabetic. I have no problem telling anyone. My father does not really want anyone else to know. I remember my grandparents saying, ‘no one is going to marry him because he is a diabetic’.” (SAm 5, type 1)
▸ “My parents, my family they stopped me and they didn't let her (fiancé) know. I don't mind. It is a life's decision for her, right? I was willing to tell her every single thing. However, they didn't let me.” (SAm 6, type 1)
▸ “When I am back in Pakistan they (family) don't let me tell anybody that I have it, which makes it very difficult for me when I go out. If I am going around somebody's house for a meal, they make me do the injection before I go. I can sit there and they won't have their meal ready till two hours later and I will just have to keep popping myself with coke…” (SAw 6, type 1)
SA participants: perceived support systems for DM
Immediate/close family members
Family structure is very important in the SA community and it is common to find multigenerational, extended families living together in the same household. DM often becomes a family issue instead of an individual's private affair. Unsurprisingly, support from family seemed to be very important for our SA sample.
▸ “My wife really supports me. Does not allow me to eat even a small piece of sweet … I like the fact that she looks after me. Even my children look after me … I would not have been able to manage my sugar levels without family support …” (SAm 3, type 2)
▸ “I feel there is no life without wife. After a certain age there is a desperate need for a partner … they will remind you and say, ‘have you taken your insulin?’ or ‘take your insulin and in the mean time I will prepare food for you and lay it on the table’ … this way, together you can look after diabetes better.” (SAm 4, type 2)
▸ “I am very lucky that my children are very, very good. Because of them I am happy … they give me first preference. Three or four times I get phone call from them whether I am all right or not, even my sister from back India … they are very worried … they always say, ‘Please don't eat anything’ … they are very concerned.” (SAw 3, type 2)
▸ “If there are people in the house who care for you, then you can enjoy your life … you can forget your pain. I have two grandsons. All day I have very good company and I don't even remember that you have diabetes. My daughter-in-law looks after me a lot. She knows what I like to eat …” (SAw 2, type 2)
Religious beliefs and values
Religion and spirituality are very prominent in the SA community and most SA participants reported a positive impact of religion on their DM.
▸ “Prayers give me a lot of support. There is a lot of support from God. Prayers have a lot of healing power, they do have a lot of effect. They help control all diseases, reduce tension a lot.” (SAm 2, type 2)
▸ “Oh, you cannot forget God! I pray every day. There is a lot of power in a prayer. He has given me this condition so he knows about it.” (SAw 1, type 2)
▸ “I read my Namaz (Islamic form of prayer) … I read the Quran (holy book for Muslims). It is true that the great power who sits up there will listen to us. It's after God that we have doctors and nurses.” (SAw 4, type 2)
Healthcare team and diabetes-related literature
All SA participants regarded their hospital diabetes clinic as their most important source of information.
▸ “I used to read all these leaflets in my free time due to which I am quite aware about diabetes … the SA nurse can understand our language and she is a very nice lady. She is worth all the praise. Doctors here talk in English … he (a consultant) is also nice but most of the time he cannot understand my English.” (SAm 4, type 2)
▸ “I take all the leaflets home … I have seen the (S. Asian) nurse, she is very nice … this diabetes nurse.” (SAw 3, type 2)
▸ “The doctors … they just tell you about your blood levels … this and that … blah, blah, blah and you are out of there within 5 minutes … literally … so leaflets is what helps you.” (SAw 5, type 1)
White participants: perceived barriers to DM
Difficulties with diet management
As with the SAs, the majority of White interviewees also felt that adhering to dietary recommendations was the most difficult aspect of their DM.
▸ “Not eating chocolate … that's a major problem I don't always stick to it. I don't object so much to the medication because I know the medication gives me little bit more leeway on the food.” (Ww 2, type 2)
▸ “My diet … it's very hard … especially having children you have all these temptations around and you are like I mustn't eat it, I mustn't eat it. I am overweight and I do try to lose weight but if I cut down all my food then I tend to get hypo and I did have a really bad hypo once … I hate having hypos.” (Ww 4, type 2)
▸ “You have just got to watch what you eat. You can't eat sugary things or you have just got to learn to live with what you can eat and what you can't eat.” (Ww 1, type 2)
Inconvenience surrounding insulin injections
Four (men=3, women=1) of the eight White participants were taking insulin as part of their treatment for type 2 diabetes. The men found insulin injections to be inconvenient and reported difficulties with including them in their daily lifestyle, some of which were linked to societal stereotypes associated with injecting.
▸ “It's the inconvenience of the injections that annoys me most of all because it does stop you from doing quite a few things. It is just the inconvenience of … say … if I went into a gent's loo and a man standing injected himself. The first thing you think to yourself is, Oh! He is a drug addict. You think people look at you. One person said, “Do you have to do it in front of my kids?” I said, “Yes! I do actually … I said, I hope this happens to you and you have got to do it or your mum or dad then you will keep your mouth shut … you do get picked up on it and I do feel awkward.” (Wm 4, type 2)
▸ “I am a bit in awe of insulin because with your tablets it didn't affect you at all…you could go out…anywhere. As soon as you start to go on insulin…you can't go out…we used to love going…because its injection at 1'o clock…it messes things up completely. My wife says wouldn't it be nice if we have a meal today and I say, ‘but I haven't got my jab with me’… the last injection, I have got to do it roughly between 10–10.30 and that one is a bit of a nuisance because sometimes I want to go to bed earlier than that…I feel a bit tired but you feel that you have got to sit up and wait….” (Wm 3, type 2)
White participants: perceived support systems for DM
Healthcare team and diabetes-related literature
All White participants considered their hospital diabetes care teams as their most effective sources of support. As with the SAs, the White participants also seemed to rely heavily on leaflets, books and magazines to provide them with the latest information regarding diabetes.
▸ “It will be the hospital … it is quite comforting, I come here to be weighed and being told to cut down this or that and I have seen the dietician a few times as well … I suppose it's the best sort of information I have had so far.” (Wm 3, type 2)
▸ “When I first had diabetes they went through all the different things that you can do to make it better for yourself. I learnt all that here and all the diabetes-related information leaflets they give you … I have got a file on it.” (Wm 2, type 2)
▸ “They are very good at the hospital here. They've explained a lot of things to me … the diabetic nurse advised me a lot and then the doctor as well.” (Ww 4, type 2)
Conclusions
Adherence to dietary recommendations is central to the management of type 2 diabetes and is necessary for achieving optimal glycaemic control with some insulin regimens, for example, twice daily premixed insulin for types 1 or 2 diabetes. However, as highlighted by current findings, it is considered the most difficult aspect of DM. Dietary freedom has been shown in the UK and the USA to be the aspect of life, which is most negatively affected by diabetes (eg, refs. 32 ,33). Findings from studies conducted in Asian countries show that dietary freedom is rated as even more negatively affected by Asian patients with diabetes (eg, refs. 34 ,35). Although the majority of our SA participants had been living in the UK for most (and in two cases all) of their lives, the cultural and social practices of their countries of origin continued strongly to influence their dietary patterns. Excerpts from our SA participants reflect how patients may be dissatisfied or uncertain regarding the dietary advice they receive due to miscommunication or conflict with patient's personal, dietary preferences.
There is significant cultural pressure on younger SAs with diabetes to hide their condition from others.36 This appears to be part of a more general trend to fear community knowledge of familial illness, which is perceived to threaten the marriage options of younger family members in the SA community. Unsurprisingly, this can increase the difficulty and complexity of DM and markedly reduce adherence to treatment.37 Due to lack of type 1 participants in our White sample, we were unable to assess whether younger Whites experienced a similar stigma in relation to their diabetes.
Family was the most essential source of support for SA in terms of both providing emotional support as well as assisting patients with DM. SA participants who lacked or reported less than adequate family support struggled to cope alone and reported greater distress. Strong family networks are an essential feature of SA communities,38–40 however, ‘family’ may not always be supportive of diabetes care and may sometimes be obstructive. For example, families may impose their sociocultural beliefs onto the person with diabetes or conceal the diabetes to avoid the social stigma surrounding diabetes in the SA community thereby making self-care for people with diabetes even more complex. In other words, for people with diabetes from the SA community, their condition is probably best understood within the context of their family/significant others and if healthcare recommendations are not consistent with the belief systems of significant others, it is likely that those recommendations will not be followed.
White participants viewed their diabetes care teams as their main source of support for their DM. SA on the other hand, considered their diabetes care teams as the most effective source of information and not necessarily as sources of ‘support’. SAs unable to communicate effectively in English particularly recognised the value of their SA diabetes-specialist nurse. Emotional support derived from religious beliefs was also reported exclusively by the SA sample.
Limitations of this study include interviewing patients from a single hospital site in the UK. Although involving patients from other hospitals would have allowed for a more generalisable sample, we were particularly interested in the patient population of Hillingdon Hospital. The current study allowed us to explore a few factors that may have contributed to differences in clinical outcomes between these two communities specifically at a single hospital site. Despite being offered a choice of three languages, SA interviewees generally, (regardless of whether they could/could not speak English fluently) wished to be interviewed in English. Only when they struggled to express themselves during the interview, did they switch to Hindi or Punjabi. The interviewer (HS) felt that the SAs interviewees (especially those first generation participants who had migrated to the UK), considered speaking in English, as a status symbol. It appeared that these participants wanted to demonstrate their command of the English language to the interviewer (an SA herself).
It will be useful to evaluate whether clinical outcomes improve, if SAs with diabetes are encouraged to attend hospital consultations with their significant others. For example, SA men with diabetes could be encouraged to bring their spouses or another significant female family member with them when they meet their diabetes nutritionists, given that women are more likely than men to be responsible for grocery shopping, cooking, and arranging meals/snacks in SA households. Interactions between the patient, their family members and healthcare professionals in patients’ preferred language of communication (where possible) could help to ensure that significant others also receive clear messages from health experts regarding what is best for patients’ DM. Such clarity may help in reducing family conflict due to sociocultural elements and reducing the demands on patients themselves to educate their significant others about their diabetes.
References
Footnotes
-
Contributors HS designed the study, the data collection tools, conducted all the interviews, analysed the qualitative data and drafted and revised the paper. She is guarantor. MC helped with the data analysis and revised the draft paper. CB helped with designing the study, monitored data collection, helped design the data collection tools and revised the draft paper.
-
Funding HS conducted the present study as part of her PhD research and she was awarded the Overseas Research Students Scholarship (ORSAS) and the Royal Holloway College Research Studentship to conduct her PhD research.
-
Competing interest None.
-
Patient consent Obtained.
-
Ethics approval Hillingdon Local Research Ethics Committee, UK.
-
Provenance and peer review Not commissioned; externally peer reviewed.
-
Data sharing statement No additional data are available.