Article Text

Abstract
Objectives This service evaluation examines how efficiently an innovative, simple and interactive blood pressure (BP) management intervention improves BP control in general practice.
Design Prospective service evaluation.
Setting Ten volunteer general practitioner (GP) practices in Stoke on Trent, UK.
Participants Practice staff identified 124 intervention patients and invited them to participate based on two inclusion criteria: (1) patient has chronic kidney disease (CKD) stages 3 or 4 with BP persistently >130/85 mm Hg or (2) patient is >50 years-old (without CKD stages 3–5) with BP persistently >140/90 mm Hg despite prescribed antihypertensive medication. Three selected hypertensive control patients per intervention patient underwent usual clinical care (n=364).
Interventions Intervention patients used ‘Florence’, a simple, interactive mobile phone texting service with BP management intervention for 3 months, or for less time if their BP became controlled. Patients measured their BP, text their readings to Florence, received an immediate automatic response and had results reviewed by their GP/practice nurse at least weekly.
Main outcome measures Baseline data including recent BP readings and medications were collected; similar information was obtained for 6 months for both control and intervention patients. Average BP readings and medication usage were determined.
Results At final data collection, five intervention patients had not yet completed the full programme. Control and intervention patients were well matched except that intervention patients had significantly greater baseline BP. Greatest BP reductions were among hypertensive intervention patients without CKD stages 3–5. Intervention patients had significantly more BP readings and more changes in medication over the 3-month data collection period.
Conclusions Simple telehealth is acceptable and effective in reducing patients’ BP. In future, poorly controlled patients could be targeted to maximise BP reductions or broader use could improve diagnostic accuracy and accessibility for patients who struggle to regularly attend their GP surgery.
- Primary Care
- Telehealth
- Patient Experience
- Text Message
This is an open-access article distributed under the terms of the Creative Commons Attribution Non-commercial License, which permits use, distribution, and reproduction in any medium, provided the original work is properly cited, the use is non commercial and is otherwise in compliance with the license. See: http://creativecommons.org/licenses/by-nc/2.0/ and http://creativecommons.org/licenses/by-nc/2.0/legalcode.
Statistics from Altmetric.com
Article summary
Article focus
-
Hypertension carries significant risks but is commonly poorly managed and controlled.
-
Telehealth technology appears to be a useful strategy for managing chronic conditions; however equipment deployed is often complex and costly.
-
Use of a new, simple and low-cost telehealth intervention was evaluated to establish if it can efficiently manage hypertension in a way that suits patients.
Key messages
-
A simple, interactive telehealth intervention effective and acceptable way of quickly gaining control of blood pressure (BP) in hypertensive individuals—even among those who had been previously difficult to engage.
-
Maximal BP reductions using this type of telehealth intervention appear to occur among hypertensive older adults without chronic kidney disease.
-
There may be a place for wider utilisation of this technology to assist in the diagnosis of hypertension, monitoring hypertension and remote clinical management, and in those who find it difficult to attend their general practitioner surgery.
Strengths and limitations of this study
-
As this is a service evaluation, the results obtained accurately reflect actual use of the technology in the clinical setting.
-
Aside from BP measurements in intervention patients, no measurements or tests were undertaken in any patient specifically for this service evaluation, therefore there were some missing data.
-
Control patients were less hypertensive at baseline than intervention patients and may have been fundamentally different to intervention patients—it appeared that intervention patients were more likely to have been difficult to control in the past.
Introduction
Hypertension is an asymptomatic but lethal condition, which carries risks of catastrophic cardiac, renal and cerebrovascular events. However, commonly, it is inadequately controlled.1 Dangers of poor-hypertension control do not simply lie with undertreatment. Overtreatment resulting from inadequate follow-up or falsely high blood pressure (BP) readings taken by health professionals in healthcare settings can potentially result in dizziness, falls and fractures. Given its prevalence among the general adult population, the risks of poorly managed hypertension are substantial with potentially avoidable costs to the health service. In their most recent guidelines for hypertension, the National Institute for Health and Clinical Excellence (NICE)2 highlights the need for good control of hypertension to avoid a consequent treatment-resistant state and also advocate home measurements to prevent treatment of ‘white coat syndrome’ in an otherwise normotensive individual. Therefore, intermittent clinic BP checks alone are now inadequate and new, efficient and effective means of accurately diagnosing and managing hypertension must be sought.
Telehealth is being increasingly used to assist patients and healthcare professionals responsible for their care to monitor medical conditions. A variety of delivery methods are available, from web-based methods to telephone touch pads3 to complex ‘pods’ that can transmit multiple readings and symptom reports to healthcare settings from patients’ homes. Home telehealth interventions have been shown to substantially reduce mortality, hospital (re) admissions, emergency visits, length of hospital stay and costs of care, while improving quality of life for a number of chronic conditions.4–11 A meta-analysis by Bray et al12 concluded that self-monitoring results in small but significant reductions in BP. Further, McManus et al13 suggest that this may be ‘a result of better adherence to treatment’. A recent systematic review and meta-analysis found that the benefits of home BP monitoring can be maximised if telemonitoring is used.14 However, equipment for complex telemonitoring can be expensive, needs extensive training for its use, may require a dedicated non-clinical triage service to receive messages and relay to community nursing teams and, in the case of hypertension, may have functions that are surplus to requirements. This has led, in some areas, to costly equipment being left unused. Therefore a simple, accessible and cost-effective approach to home BP monitoring is desirable.
This service evaluation aims to determine the effectiveness of a simple, interactive telehealth system in reducing BP to a normotensive range in poorly controlled hypertensive adults.
Method
This service evaluation was undertaken in a materially deprived area of the UK with poor health. Local practices were invited to volunteer to take part in this simple telehealth programme and participating practices were briefly trained in the use of the telehealth intervention. Intervention patients were recruited between April and November 2011 to undertake a 3-month programme using Florence. Patients could continue using Florence after this period if they so desired and at the discretion of the practice. Data collection continued for 6 months from recruitment. Final data collection took place at the end of February 2012.
The simple telehealth intervention utilised in this project required patients to use a home, electronic sphygmomanometer and text via a mobile phone. Patients obtained their BP readings and texted the results to a secure server, ‘Florence’. Florence is an interactive service, which reminds patients to text their BP readings each day, and sends reminders if a reading is not received within 2 h. It also sends automatic responses to patients regarding any further required actions based upon the BP readings obtained, from sending a repeat reading if the programme detects that an error may have occurred, through advising patients to contact their doctor or practice nurse. This allows for ‘closed loop’ monitoring with weekly, or more frequent, review by the patient's own general practitioner (GP)/nurse who can log into the secure server and access their results. Messages can be sent back to the patient from their primary healthcare team with advice on continuing management. Although Florence had not been used in this context prior to this project, local pilot use for other conditions resulted in positive anecdotal reports from patients and professionals.
One member of the practice team, usually a practice nurse, led the telehealth programme in each practice. They were responsible for explaining the programme to patients and training them in the use of the software and BP recording devices. Patients were invited to be included in the intervention according to two criteria:
-
Patients with chronic kidney disease (CKD) stages 3 or 4 with BP>130/85 mm Hg.
-
Patients >50 years without CKD stages 3–5, with recent BP>140/90 mm Hg despite prescribed antihypertensive medications.
For each intervention patient, three similar control patients were identified, who underwent usual clinical care. Practice staff were asked to match controls according to inclusion criteria and demographic details; then patient records of control patients were used for data collection while they underwent usual care. Intervention patients were invited to undertake the programme for 3 months or for less time if they became normotensive. Patients were able to continue using the system at the discretion of their practice if they wished to after this time.
Baseline data were collected by practice staff using a proforma for all intervention and control patients. This requested information about demographics, medications, comorbidities, BP at recruitment, most recent BP prior to recruitment and BP 1 year before, most recent estimated glomerular filtration rate (eGFR) and healthcare service use over previous 12-month period. This baseline data allowed calculations of change in BP control as well as comparison between the intervention and control patients at baseline and end of the evaluation. Practices were then asked to complete a proforma which asked for information about BP readings, eGFR, medications, comorbidities and healthcare service use every 2 months for intervention patients for a total of 6 months. Due to administrative burden, data collection occurred every 3 months for control patients. No specific tests of eGFR were organised purely for the sake of this evaluation. Therefore, eGFR results were only available if the practice had initiated this test as part of usual care. Qualitative data were collected at various stages throughout the programme using questionnaires, text messages and a discussion group, the results of which are discussed in an accompanying paper.
Data were collated and analysed using PASW Statistics 18 (Release 18.0.0, 2009) and Microsoft Excel. Missing data were coded as such and requests to practices for these data were made to promote as complete a data set as possible. Intervention patients were analysed as such even after they stopped using Florence. BP readings that were physiologically impossible (eg, diastolic BP higher than systolic BP (SBP)) and those that appeared to be typos and duplicates were excluded. Due to incomplete data collection in some cases, the denominator varied for different calculations. Denominator values used are given in tables and figures.
Home BP readings were adjusted up by 5/5 mm Hg, as per current NICE guidance,2 to ensure that comparisons of BP readings between intervention (in whom the predominant place of BP measurement would be at home) and control patients (in whom the predominant place of BP measurement would be at the GP surgery) were fair.
Control of, and change in, BP and eGFR over the 3-month programme period and follow-up for 6 months from baseline was identified and average changes for both intervention and control groups were calculated and compared for significant differences using a paired sample and an independent sample t test, respectively. The two groups were also examined for variations in medication and healthcare service usage and negative hypertension-related events (eg, stroke/transient ischaemic attack (TIA)) and medication-related events (eg fall and fracture). Statistical significance was assumed at the level of p<0.05.
Results
In total, 490 patients were recruited, of whom 126 were intervention patients and 364 were controls. Of the intervention patients, two were excluded from analyses (with their respective controls) as the patients did not submit any BP readings correctly. Four practices did not identify sufficient control patients, for each intervention patients thus there are eight fewer control patients than would be expected according to the number of intervention patients.
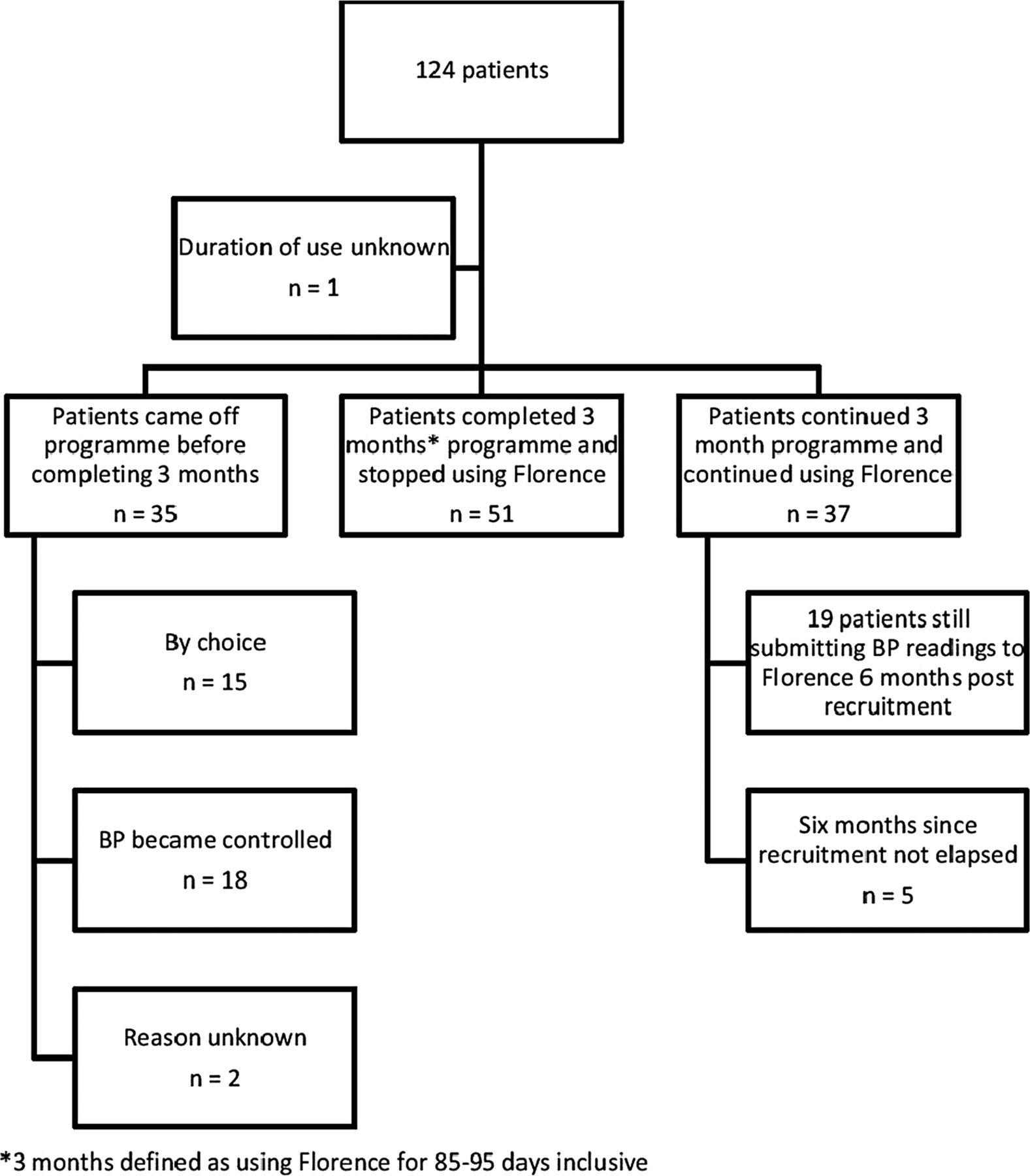
At the point of final data collection, the duration of use of Florence was unknown for one patient and 6 months had not yet elapsed since recruitment for five patients (see figure 1). Fifty-one patients stopped using Florence 3 months from baseline, as per the intervention protocol. An additional 37 patients continued to use Florence beyond the required 3 months, of whom 19 continued to submit BP readings to Florence for at least 6 months postrecruitment. Of the 35 patients who did not complete 3 months using Florence, 18 stopped using it as their BP had become controlled, 15 patients chose to stop using it and the reason is unknown for 2 patients. Among those patients who chose to stop using Florence before they had completed the 3-month programme, reasons included the patient left the practice (n=2), family and/or social commitments prevented continuation (n=2), abroad for significant period(s) of time (n=2), did not wish to continue (n=2), difficulty using the system (n=1), problems texting (n=1), difficulty relaxing to take BP (n=1), found taking BP anxiety provoking (n=1), spouse very ill (n=1), incorrectly thought the programme period had ended (n=1), preferred to see GP face to face and the patient only wanted to use it short term (n=1).

Use of Florence and reasons for stopping.
*3 months defined as using Florence for 85–95 days inclusive.
Table 1 outlines the baseline data while figure 2 represents an overview of the patients at baseline and 3-month postrecruitment. The average age of all patients involved in this project was 59.7 years, with intervention patients having an average age of 58.9 years and control patients having an average age of 60 years. There were no statistically significant differences between participating and control patients with regard to their age, most recent eGFR and number of antihypertensive medications prescribed at baseline. There was no significant difference between intervention patients and controls in the comorbidities they had at baseline, except for osteoporosis for which 4% of intervention patients and <1% controls had been previously diagnosed.
Baseline data

Overview of patient details at baseline and 3-month postrecruitment.
Intervention patients had significantly greater SBP and diastolic BP readings at recruitment and for the year prior to recruitment, see table 2. This remains true even when only patients who were hypertensive at recruitment (intervention patients n=84, control patients n=137) were examined, see table 3 and figure 3.
BP readings from 1 year prior to baseline to 6-month postrecruitment among all intervention and control patients
BP readings from 1 year prior to baseline to 6 months post-recruitment among all intervention and control patients who had systolic hypertension at baseline (SBP>130 mm Hg if patients had CKD stages 3–4 or SBP>140 mm Hg if no CKD stages 3–5)

Blood pressure readings at baseline and months 1, 3 and 6 postrecruitment among all intervention and control patients who had systolic hypertension at baseline (systolic blood pressure (SBP)>130 mm Hg if patients had chronic kidney disease (CKD) stages 3–4 or SBP>140 mm Hg if no CKD stages 3–5).
Average SBP and diastolic BP readings for all intervention patients fell within the normotensive range from month 1 of the programme (see table 2). From subgroup analysis, intervention patients included with uncontrolled hypertension without CKD stages 3–5 became normotensive (≤140/90 mm Hg) by month 2. Despite intervention patients having significantly elevated SBP compared with control patients at baseline and 1 year prior to this, intervention patients had no significant difference in their average SBP from control patients from month 1 of the programme.
Average BP readings from patients with CKD stages 3–4 only fell into the normotensive range (≤130/85 mm Hg) in month 3. Changes in BP from baseline at each month among intervention patients, were greatest and most significant among patients without CKD stages 3–5 who had systolic hypertension at baseline, see table 4 and figure 2. These patients had significant reductions in SBP ranging from −15 to −16 mm Hg during the 3 months of the programme, a significant difference of at least −10 mm Hg continued to be observed up to 6 months postrecruitment (see table 4 and figure 4); controls who were hypertensive at baseline did not have an equivalent reduction in BP identified until month 3.
Average change in BP from recruitment to 6-month postrecruitment in intervention and control patients >50 years included due to having BP>140/90 mm Hg despite prescribed antihypertensive medications who had systolic hypertension at baseline

{kind=link}
{kind=link}
{kind=link}
{kind=link}
Average change in blood pressure (BP) from recruitment to 6-month postrecruitment in intervention and control patients >50 years included due to having BP>140/90 mm Hg despite prescribed antihypertensive medications who had systolic hypertension at baseline.
In addition to the changes in BP observed, significantly greater numbers of BP readings were obtained by patients using Florence than those receiving usual care; 13, 12 and 10 readings per month were obtained in months 1–3, respectively, among intervention patients compared with an average of 0.2 readings a month among controls for the same 3 months.
Significantly more changes, 0.31 vs 0.08 (p<0.05; CI for difference 0.16 to 0.32) were made to the medications of intervention patients, compared with control patients over the 3-month programme, respectively. There was no evidence of inappropriate overprescribing for white-coat hypertension prior to the programme period as no intervention patients had already prescribed antihypertensive medications stopped due to hypotension. However, 25 patients had systolic hypertension at baseline from clinic readings and were found to be normotensive on home readings in months 1–3 of the programme without any change in medication.
No intervention or control patients suffered from stroke/TIA or hip fracture during the 6-month data collection period. Five control patients and no intervention patients experienced falls during the 6-month data collection period; however, this difference was not statistically significant. Three falls were related to icy weather and the fourth was classified as a trip. There was no significant change in healthcare use or eGFR readings between intervention and control patients during the 6-month data collection period.
Discussion
This pragmatic service evaluation has demonstrated the use of a simple interactive telehealth intervention in a real-life clinical primary care setting across 10 general practices. Overall, patients using Florence demonstrated a significantly greater average reduction in SBP, compared with their associated controls, during the initial 3-month programme. This was informed by significantly greater numbers of BP readings and may have arisen as a result of significantly more frequent changes in antihypertensive medications enabled by the telehealth system, more appropriate timing of BP recordings, an increased awareness among patients of their BP values and the significance of the same and/or an increased sense of control among patients. A recent qualitative study by Jones et al15, examining patients’ experiences of using self-monitoring, self-titration and telemonitoring for hypertension, revealed that once patients had been involved in the self-management programme and witnessed the variability of their BP readings they felt that it was inappropriate for changes to be made to medication based on fewer readings.
When results were analysed according to the inclusion criteria the practices allocated the patient to, no significant improvement in BP control was noted among participating patients with CKD stages 3–4 compared with their associated controls. Among the small number of patients who were normotensive at baseline, an elevation in average SBP was noted (see figure 2). The greatest average reduction in SBP among participating patients were noted among those patients recruited for uncontrolled hypertension, without CKD stages 3–5 who were hypertensive at recruitment (see figure 2 and table 4).
Due to the protocol of the programme running only for 3 months, the most robust data set relates to this period. After this, data sets become increasingly incomplete as patients left the programme and returned to usual clinical care. Ongoing differences in BP control between intervention and control patients beyond 3 months may thus be masked.
Although the data collection was as complete as possible, robust comparisons are limited in this service-level evaluation, primarily as ‘control’ patients underwent usual clinical care. This may have involved not having any BP or eGFR readings recorded near to baseline or for the duration of the programme. Further, patients who initially were using Florence but then stopped before the 3-month programme period was complete may not have had any further BP measurements recorded. Therefore there are some missing data, but this has been indicated in each of the figures and tables.
BP readings that were recorded as ‘free text’, rather than on the practice computer electronic template, may not have been noted during the data collection for control patients. Therefore, if any practices were recording BP values in this way, this could have led to missing data. There is evidence that this may have occurred in some cases, for example, three control patients are recorded as having had hypertension reviews in the healthcare service usage data but no BP recordings were provided for this period. For one of these patients additional antihypertensive medication was started at the hypertension review by the practice but the BP reading is not provided. As the BP readings from Florence were directly forwarded for data input, any poor record keeping among practices will have had a more significant effect on the BP readings of control patients. The resultant effect on these data may be that any excess reduction in BP among intervention patients compared with control patients is underestimated.
Subjective assessment of a ‘typo’ in BP readings texted to Florence may not have been accurate at all times; however, the occurrence of these was rare and incorrect exclusion of such data is unlikely to have significantly affected the results.
Although prospective data collection was requested and encouraged, due to other pressures on practice staff, retrospective data collection in relation to medication and use of secondary care resources were undertaken for a significant number of cases and controls. This may well have led to inaccuracies in detail about medication changes, for example, as retrospective collection of this data was not always easy. But BP readings for intervention patients were texted in, in real time and readings were printed and forwarded directly from the secure server. BP readings that were recorded appropriately on practice templates for control patients would also have been noted contemporaneously.
Practices did not strictly match the given inclusion criteria, thus resulting in the recruitment of intervention patients at baseline who were subsequently confirmed as not being hypertensive (see figure 2). Practices indicated which inclusion criteria they had recruited patients according to and the results were analysed accordingly. Therefore, results of all patients were analysed according to stated inclusion criteria but also a breakdown of patients according to whether they were normotensive or hypertensive at baseline was given. This breakdown means that the outcomes of using the telehealth intervention reported here for all patients demonstrate actual clinical application rather than highly selected cases but also that an overview of a smaller hypertensive sample has been given. Patients who did not meet inclusion criteria according to age were included in all relevant analyses.
A previous systematic review of randomised controlled trials (RCTs) undertaken in both primary and secondary care settings demonstrated that SBP readings in people undertaking home monitoring are significantly lower (4.2 mm Hg, reducing to 2.2 mm Hg when publication bias allowed for) than control patients.16 Although, during this 3-month programme, there was no significant difference in the average SBP among intervention and control patients, the benefit of this intervention should not be overlooked. Anecdotal feedback from practices highlights that intervention patients may have been fundamentally different to control patients. Feedback from staff and patients implied that intervention patients were often those who, due to personal, family, occupational or unknown factors, had been previously difficult to engage or control. This is also indicated by the significantly greater BP readings at baseline and 1 year prior to baseline among intervention patients compared with control patients (see table 2). Therefore, although the quick reductions in BP among intervention patients into the normotensive range in line with control patients by month 6 may represent regression to the mean, it is more likely that achieving similarity in BP results represents a greater achievement than the numbers alone report.
McManus et al17 reported the results of an RCT in Birmingham, which utilised self-recording of BP at the GP surgery alongside provision of BP targets to patients. This demonstrated similar outcomes to the current service evaluation, that intervention patients had significantly greater reductions in their BP at 6 months from a higher baseline BP. However, they demonstrated that the difference between intervention and control patients was not sustained at 1 year. Therefore, to determine if the benefits of using Florence identified in this evaluation are prolonged, a longer period of follow-up is needed that can also track the use of healthcare resources.
Healthcare professional concerns, detected in a previous UK study investigating the acceptability of the concept of monitoring of BP using mobile phones, which related to inconvenience of ‘continuous streams of readings,’18 were addressed by the current programme which was designed to take no longer than 1 min a week per patient for a health professional to review the BP results. Unacceptably high readings were automatically detected by Florence and patients were given appropriate advice on further action via text. Therefore, the concerns detected by Bostock et al did not become reality among practices involved in this service evaluation.
Although patients were trained how to take their BP at the start of the programme, no checks were undertaken to ensure patients were measuring BP as per instructions. Therefore, if patients had not taken multiple readings or used a different arm at different times, the recorded BPs may not have been accurate. In terms of this evaluation this may have affected the change in BP observed. However in the long term, a patient missing the difference in BP between their two arms may result in a missed opportunity to detect comorbid or contributory conditions, for example, peripheral vascular disease.19 Therefore safeguards need to be in place during wider implementation to ensure that patients are measuring their BP accurately throughout their time using this system and to ensure that any difference in BP between two arms that does exist is appropriately managed.
This intervention was well received and effective at quickly reducing elevated BP readings to normotensive ranges. The benefit of rolling this type of intervention out more widely to tackle hypertension in the primary care community could be great, provided patients are carefully counselled regarding what it involves and to ensure that they have the physical and cognitive ability to undertake BP readings and send text messages, or that they have regular contact with someone who is willing to do this on their behalf.
To maximise reductions in BP, careful selection of patients onto a simple telehealthcare programme (eg, patients without CKD stages 3–5 who are hypertensive >140/90 mm Hg) is required. However, anecdotal evidence obtained through the associated qualitative data indicates that less quantifiable benefits can be gained from recruiting patients with uncertain diagnoses of hypertension and/or suspected white-coat hypertension. Although there was no evidence of Florence helping to detect patients who were being over treated due to white-coat hypertension in this case, a systematic review of RCTs has found that home BP monitoring can result in down titration of hypertensive medication compared with usual care.14 Therefore, a broader application of this type of intervention may be considered. Poor previous patient concordance with management of hypertension should not be a barrier for introducing simple telehealth strategies to patients as the flexibility associated with this management strategy may overcome the difficulties that the patients had previously been experiencing in adhering to healthcare advice.
The likely benefits of improved BP control among intervention patients relate to reduced healthcare service use and reduction in BP-associated comorbidity. However, the impact of reducing BP on these factors is likely to be delayed by some months or years while the costs of reducing the BP (using simple telehealth system (system itself and appointments used training patients to use the system) and increased changes to medication) are realised now. Therefore, to undertake a thorough economic evaluation of an intervention such as and to determine the long-term benefits of this strategy requires follow-up of at least a year.
Acknowledgments
The authors thank John Blackburn, Chris Chambers, James Davies, Mike Dixon, Dave Sanzeri, Diane Wilshaw who work for NHS Stoke on Trent CCG and were part of the programme steering group and/or data collection team.
References
Footnotes
-
Contributor EC designed data collection tools, inputted and analysed data and drafted and revised the original paper. RC lead the programme of work and oversaw the processes of data collection, analysis and reporting, she also devised and revised this paper. PO collected data and revised the draft paper. EC, RC and PO are responsible for the overall content as guarantor(s). JB, CC, JD, MD, DS and DW were all involved in running the programme and for data collection.
-
Funding Funded by Health Foundation.
-
Competing interests All authors have completed the Unified Competing Interest form at www.icmje.org/coi_disclosure.pdf (available on request from the corresponding author) and declare that (1) EC, RC and PO have support from NHS Stoke on Trent for the submitted work; (2) EC and RC have no relationships with Mediaburst Limited that might have an interest in the submitted work in the previous 3 years; PO receives royalties from NHS Stoke on Trent for the use of background IP and PO is a minor stock holder of SCL Consultants limited which is the parent company of Mediaburst Limited (3) their spouses, partners, or children have no financial relationships that may be relevant to the submitted work; and (4) EC, RC and PO have no non-financial interests that may be relevant to the submitted work.
-
Ethics approval This was a service evaluation.
-
Provenance and peer review Not commissioned; externally peer reviewed.
-
Data sharing statement There are no additional unpublished data available.