Article Text

Abstract
Objectives The natural history of early-onset Alzheimer's disease (AD) and fronto-temporal dementia (FTD) remains to be described in detail. We seek to describe the natural history of early onset AD and FTD in terms of changes in cognitive assessment and staging, medical history and survival.
Design Longitudinal prospective cohort analysis.
Setting Neurodegenerative disorders research clinic.
Participants In total, 155 consecutive patients with clinically confirmed sporadic early-onset AD or FTD at a neurodegenerative disorders research clinic in Subiaco, Western Australia (The Artemis Project).
Methods A detailed history was recorded from the patients at baseline, including education, family history and medical history. Mini-mental state exam (MMSE), Global Deterioration Scale (GDS) and total functional capacity (TFC) were determined at each visit from 1994 until 2011. Kaplan-Meier survival analysis was performed.
Results Patients with FTD were more likely to have a family history of dementia (p=0.026), to develop at least one cerebrovascular risk factor (p=0.003), manifest depression (Fisher's exact p=0.007) and to die during the follow-up period (Pearson χ2 8.97, p=0.003). Kaplan-Meier survival estimates revealed a highly significant difference in the proportion of patients surviving the follow-up period (log rank 7.25, p=0.007) with FTD patients experiencing poorer survival than those with AD. The mean MMSE and TFC were consistently lower in those with FTD compared with those with AD over a decade of follow-up; mean GDS was consistently higher in those with FTD over the follow-up period.
Conclusions We believe that the difference in survival in patients with AD and FTD in our cohort might relate to the development of one or more cerebrovascular risk factors in FTD patients and the severity of the underlying pathology.
- Genetics
This is an open-access article distributed under the terms of the Creative Commons Attribution Non-commercial License, which permits use, distribution, and reproduction in any medium, provided the original work is properly cited, the use is non commercial and is otherwise in compliance with the license. See: http://creativecommons.org/licenses/by-nc/2.0/ and http://creativecommons.org/licenses/by-nc/2.0/legalcode.
Statistics from Altmetric.com
Article summary
Article focus
-
To describe the natural history of early onset Alzheimer's disease (AD) and fronto-temporal dementia (FTD) in terms of changes in cognitive assessment and staging, medical history and survival.
Key messages
-
The difference in survival in patients with AD and FTD in our cohort might relate to the development of one or more cerebrovascular risk factors in FTD patients.
Strengths and limitations of this study
-
A longitudinal prospective cohort of patients with a good sample size and long duration of follow-up using brief robust clinical measures. The limitations of this study are that the investigation was performed at a single study centre and more comprehensive assessments of memory and executive functions need to be performed in future studies.
Objectives
It is estimated that 24.3 million people worldwide have dementia and this is expected to rise to 81.1 million people in 2040.1 Alzheimer's disease (AD) is the leading cause of dementia, contributing to up to three-quarters of dementias.2 Early-onset dementia is the onset of dementia in those aged 65 years and under, the most common causes being AD and fronto-temporal dementia (FTD).3 ,4 Patients with early-onset AD often present to the clinic with defective episodic memory, while those with FTD are characterised by disturbances in speech and behaviour.3 While progress has been made describing the natural history of AD and FTD in older adults, the natural history of early-onset AD and FTD remains to be more fully elucidated. We seek to describe the natural history of early onset AD and FTD in terms of changes in cognitive assessment and staging, medical history and survival.
Methods
This study is a longitudinal prospective cohort analysis of a group of patients identified in a neurodegenerative disorders research clinic in Subiaco, Western Australia, from 1 January 1994 until 31 January 2011: The Artemis Project. The Artemis Project is an attempt to study the neurobiology of early onset dementia of all causes in Western Australia. Participants consisted of 155 patients with clinically confirmed sporadic early-onset AD or FTD, with onset prior to 65 years, who gave informed consent and attended the clinic on more than one occasion.
Patients with early onset AD were diagnosed using NINCDS-ADRA criteria and supported by structural and functional imaging (FDG PET) and neuropsychometry.3 ,5 ,6 Patients were diagnosed with FTD using existing published criteria7 and refined as new technology (such as FDG PET) became available6 and at annual review using contemporary international guidelines.3 ,8 With this approach, no patients have been excluded and our neuropathological sensitivity and specificity for the diagnosis of AD and FTD=100%.
The FTD group comprised only patients with the behavioural variant of FTD for uniformity of analysis; patients identified with semantic dementia (n=1), primary progressive aphasia (n=8) and motor neuron disease–FTD complex (n=2) were not included.
A detailed history was recorded from the patient at baseline, including education, family history and medical history. This information was then corroborated with the spouse or primary carer, and the general practitioner. Additionally, during follow-up this information was updated if the patient characteristics changed; for example, if a patient developed cancer.
Age at onset was determined from self and carer/spouse report of the onset of symptoms. Education is defined as self-reported years of formal education. Family history is defined as a self-reported family history of dementia in first-degree and second-degree relatives. Cerebrovascular risk factors are hypertension, hypercholesterolaemia, increased girth, obesity, diabetes, smoking, excessive alcohol consumption, coronary heart disease and peripheral vascular disease, the measurement of which has been described elsewhere.9 The presence of at least one of these risk factors was determined from self-report and medical notes. The presence of mental illness (depression or psychosis) or other comorbidities was also determined through self-report, carer information and medical notes.
Mini mental state exam (MMSE) was performed at each visit as a measure of cognition.10 Global Deterioration Scale (GDS) and Total Functional Capacity (TFC) staging were determined for each visit as markers of the severity of the dementia and abilities to perform acts of daily living.11 ,12 The ratings were performed by the same trained team of cognitive assessors.
DNA screening was performed on our patients with an autosomal-dominant pattern of inheritance—nucleotide changes in the coding sequences of the amyloid precursor protein, progranulin gene, presenilin-1 and presenilin-2 genes, Tau and SIGMAR 1 gene were performed by direct sequencing of polymerosechoid reaction (PCR) products derived from genomic DNA. Nucleotide sequence information from each PCR product was obtained from both strands and possible mutations were verified by an independent amplification of the PCR product and resequenced. ApoE genotypes were determined by restriction fragment polymorphism analysis of PCR amplified products. Individuals identified with presenilin-1 mutation (Q222H), progranulin mutations and SIGMAR 1 mutations are not included in this study and will be reported elsewhere.
Statistical analyses, including χ2 tests for difference in proportions, t tests for difference in means and Kaplan-Meier survival analysis, were performed using Stata VII. As the MMSE and other variables are not normally distributed, the t test was not used and the Kolmorgorov-Smirnov test employed to test for differences in means. No assumptions were violated for the log-rank test, nor drawing of the Kaplan-Meier curves—this is a non-parametric method. The Proportional Hazard Model was not used, which expects the baseline hazards for the two groups to be proportional.
Results
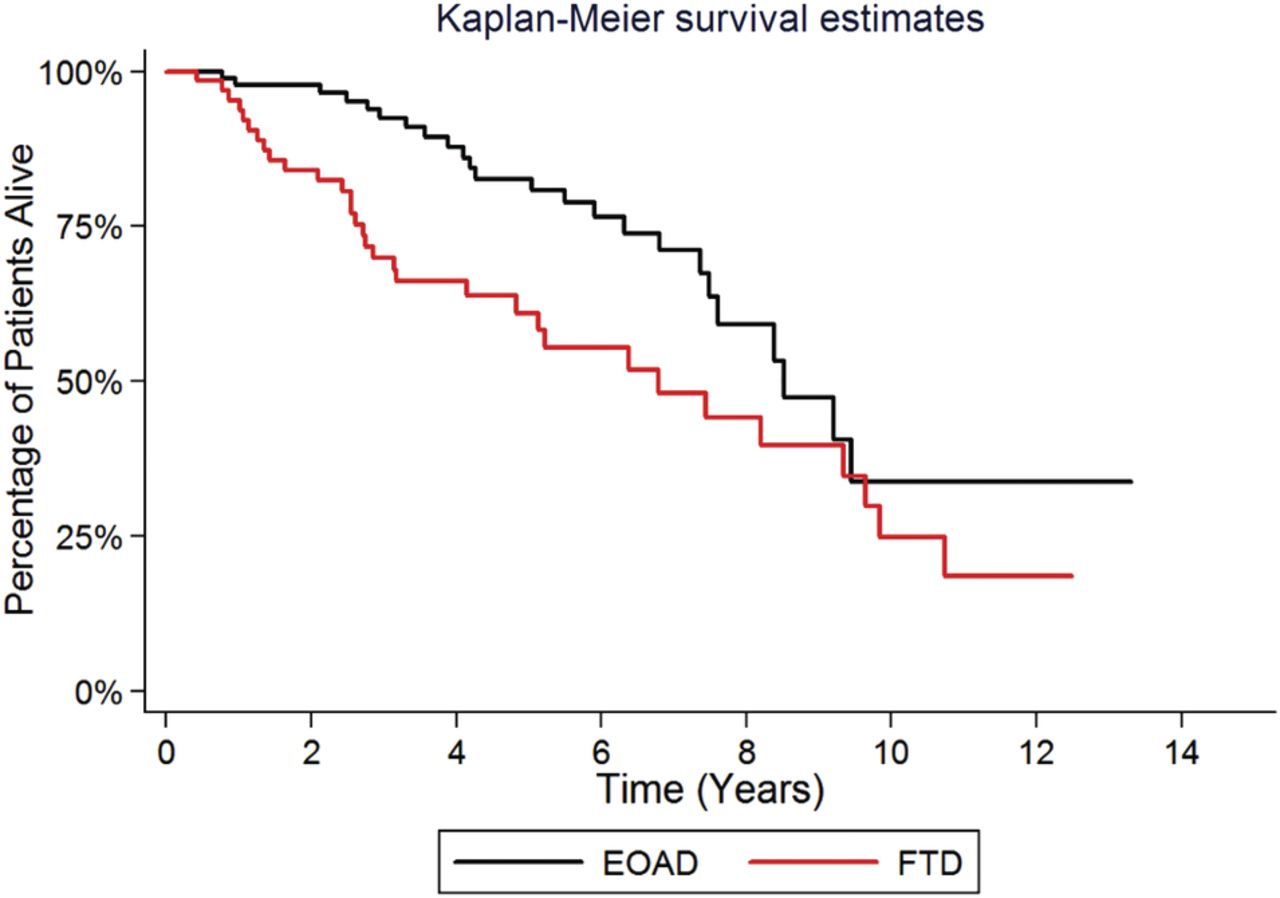
The cohort consists of 155 early-onset dementia patients (92 with AD, 63 with FTD) (table 1). Fifty-eight patients died during the study (AD=25; FTD=32); there were no drop-outs as spouses, carers and families remained in communication with study staff—even if admitted into nursing homes. There was a slightly greater, though not significant, proportion of men in the AD group compared with the FTD group (Pearson χ2 2.76, p=0.096). The mean age of onset was similar between diagnosis groups for men (56.46 vs 55.73 years, p=0.583) and women (56.24 vs 55.60 years, p=0.670). Both groups had an average 11 years of education (p=0.900). Patients with FTD were more likely to have a family history of dementia (p=0.026), at least one cerebrovascular risk factor (p=0.003), a history of major depression diagnosed using DSM-IV criteria and distinguishable from apathy commonly found in FTD (Fisher's exact p=0.007) and to die during the follow-up period (Pearson χ2 8.97, p=0.003). The cerebrovascular risk factors revealed a preponderance of diabetes, smoking and increased alcohol consumption in the patients with FTD (table 2). Kaplan-Meier survival estimates revealed a highly significant difference in the proportion of patients surviving the follow-up period, as can be seen in figure 1 (log rank 7.25, p=0.007). There was no effect of APOE ε4 allele on the natural history of early-onset AD.
Patient characteristics
Cerebrovascular risk factors in early-onset dementia
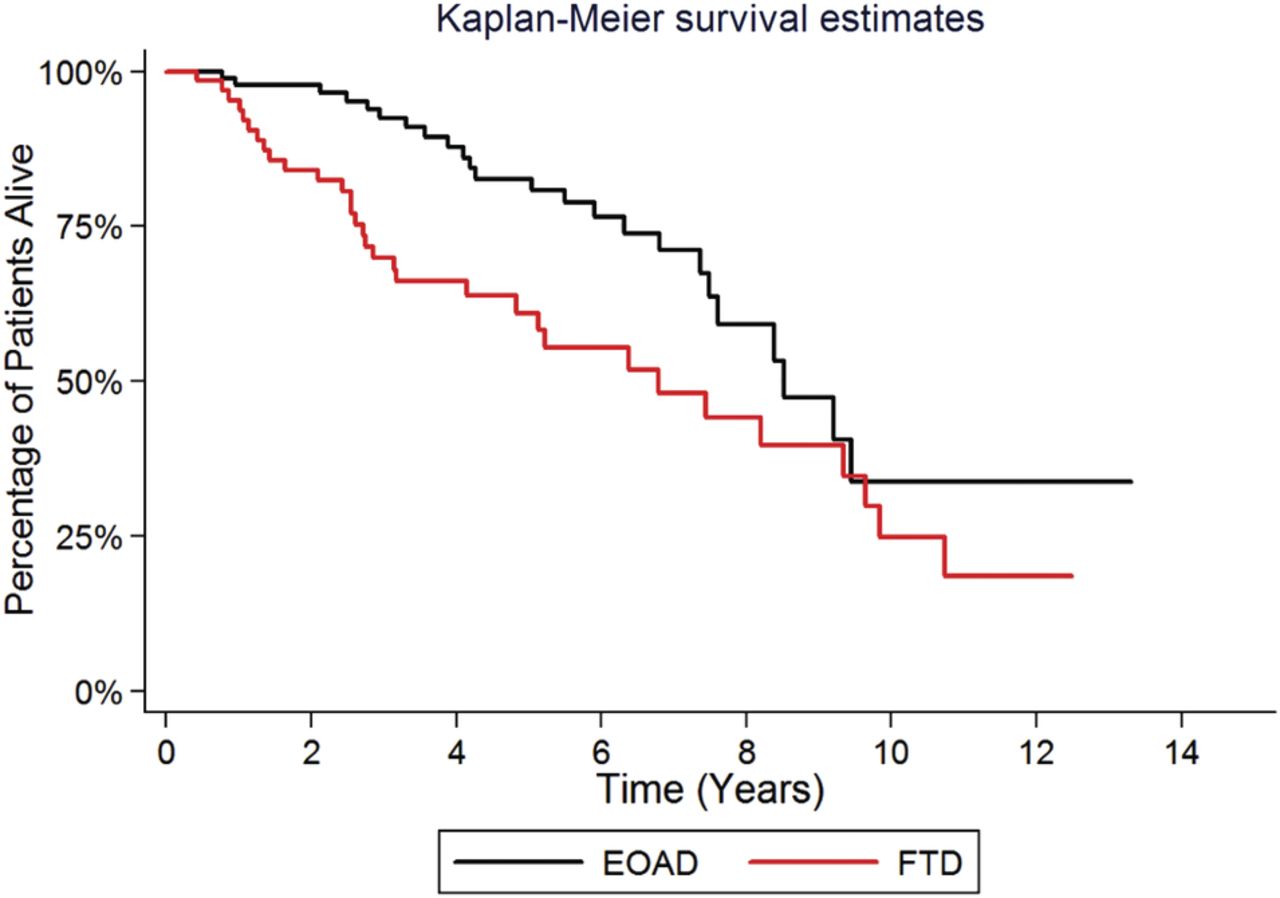
Survival analysis of early-onset Alzheimer's disease and fronto-temporal dementia patients in time (years) from baseline visit.
The mean MMSE was consistently lower in those with FTD compared with those with AD over a decade of follow-up (figure 2). At baseline the MMSE, TFC and GDS did not show any significant difference between AD and FTD, providing further evidence for a worse progression of early onset FTD in comparison to AD. The boxplot shows that spread of MMSE scores is more condensed in those with FTD compared with AD across follow-up time. Similar results were seen with TFC. A greater range of GDS scores was seen in FTD patients compared with AD patients at baseline; however, a more condensed range of scores was seen across follow-up time. Mean GDS was consistently higher in those with FTD over the follow-up period. Some of the boxplots are missing (eg, year 11 for early onset Alzheimer's disease (EOAD) and years 9 and 10 for FTD): this is because median value is 0, min=0, max=0 so there is no box; for year 12 there are no data, hence no box. The unusual distribution beyond 9 years is likely due to small sample size, which would also be affecting the boxplots. It is possible there is a survival effect; those few who survive to that point and with longer follow-up may have a slower disease progression. The boxplots may also be affected by a clustering of scores at zero (figure 2).

Boxplot and line graphs showing the change in distribution and mean mini-mental state exam, Global Deterioration Scale and total functional capacity score over time. Note the large variation in score from 9 years onward is the result of a small sample size at those time-points.

{kind=link}
{kind=link}
{kind=link}
Changes in mini-mental state exam and Global Deterioration Scale score in two patients with early-onset Alzheimer's disease. Patient 1 experienced a rapid deterioration, while patient 2 experienced slower disease progression (both patients were APOE ε4 homozygous). Patient 1 had no cerebrovascular risk factors. Patient 2 had poorly controlled hypertension, smoked and consumed excessive alcohol. His MRI revealed progressive atrophy and increase in white matter hyperintensities (A=baseline; B=24 months).
The majority of patients had a GDS score of four at baseline with a mean 4.02 years of follow-up (table 3).
Mean follow-up in years by baseline Global Deterioration Scale score
A graph of the changes in MMSE and GDS in two patients with early onset AD is presented in figure 3 to highlight the heterogeneity in natural history in individual patients which may be overlooked in a cohort analysis. Patient 1 has no cerebrovascular risk factors and remained cognitively stable for a period of 8 years. Patient 2 progressed rapidly over a period of 2 years. He was hypertensive, smoked and consumed excessive alcohol. The MRI shows white matter hyperintensities and progressive atrophy over this time. We did not observe such wide variation between FTD patients. White matter hyperintensities were identified in 10 patients with early onset AD (10.9%) and no patients with AD had evidence of small or large vessel ischaemia—apart from patient 2 (figure 3) there was no correlation in other patients with white matter hyperintensities, prognosis and survival. No patients with FTD had white matter hyperintensities or evidence of stroke (small and large vessel).
Discussion
A greater proportion of patients with FTD had a family history of dementia compared with AD patients. This is a similar result to those reported by Pasquier et al.13 They found a family history of dementia to be similar between AD and FTD patients, but a family history of dementia or psychiatric disorder to be much greater in FTD patients.13 We are currently investigating further the role of family history as a risk factor in early-onset AD and FTD.
The difference in depression between those with FTD and those with AD is a complex issue. It may be that those with a history of depression are more at risk of FTD, or that patients with FTD are more likely to develop depression.
We found a difference in the MMSE, GDS and TFC between AD and FTD patients during the progress of the study, but not at the commencement of the study. The greater decline in MMSE in FTD patients might be attributable to the more aggressive nature of the dementia in FTD: findings supported by the changes in the functional scales and the differences in survival.
We sought to describe the natural history of early-onset dementia, particularly AD and FTD. We found that survival is significantly reduced in those with FTD compared with those with AD, as seen by Koedam et al.4 In contrast, Pasquier et al13 found survival to be similar between patients with AD and FTD after controlling for sex, age, age at onset and education level, although they did find sudden death to be more frequent in FTD. These differences may be related to the inclusion of older onset dementia patients in this study. There was approximately a decade difference in mean age between Pasquier's AD and FTD patients while mean average was the same in our population. We speculate that the difference in survival between AD and FTD in our cohort might relate to the greater presence of one or more cerebrovascular risk factors in FTD patients—an unexpected finding. While our previous research had identified hypertension to be a risk factor in the development of AD, it does not appear to affect survival. Other elements of cardiovascular risk including smoking, increased alcohol consumption and obesity may develop in FTD as part of the frontal disinhibition syndrome and these factors may impact on survival. We need to be mindful of the risk profile in individuals with early onset AD as management of cerebrovascular risk factors will affect progress (figure 3).
Our experience of different rates of progression in AD appears to be similar to the results of Thalhauser and Komarova.14 They used a different staging system, the functional assessment staging (FAST) procedure and found that if a patient progressed rapidly through a FAST stage he or she was likely to experience rapid progression through the remaining stages (similar to the patient described in figure 3). It has been found that comorbidity can be associated with an increased disease progression,15 and this reflects our experiences with patients like patient 2 (figure 3). Additionally, poor physical health in those with AD is linked to poorer survival.16 Work by Paradise and colleagues modelled survival time from age, constructional and gait apraxia in a much older cohort (mean age 81 years). These patients experienced shorter survival (approximately 3 years), likely due to the age of the population studied, while others found a median survival of 6.7 years in a younger group of AD patients aged 60–69 years.17 ,18 While determining the predictors of survival in older age groups, Wolfson et al19 were unable to determine the estimated probability of survival in early-onset AD after adjustment for rapid progression (length bias) because of a small early-onset sample size. Rapid versus slow progression may be related to structural and functional changes in the brain. Kim et al20 suggested that a greater degree of glucose hypometabolism in the brain at the same level of dementia severity in early-onset versus late-onset AD patients might reflect rapid disease progression. Sluimer et al21 identified that more generalised whole-brain atrophy may reflect rapid disease progression in comparison with more localised hippocampal atrophy in slow progressing AD; Karas et al22 suggested the precuneus as a marker for progression of early-onset AD.
The major limitations of this study are the measures used to follow patients and future studies will benefit from a more comprehensive memory assessment and more sophisticated measures of frontal lobe functions. Multicentre studies with larger numbers of patients will help to elucidate further the natural history of early onset dementia.
Conclusion
In conclusion we have described the natural history of early onset AD and FTD, and observed that patients with FTD progress faster than those with AD: a finding that might relate to the development of cerebrovascular risk factors during the course of the illness and differences in aggression of the underlying pathology. Larger multicentre studies with neuropathological confirmation are necessary to confirm these findings.
References
Footnotes
-
Contributors ERA helped collect and collate data, analysed data and wrote the manuscript. MKB helped analyse data, performed the statistical analyses and helped draft the manuscript. PKP collected, collated and analysed data, and wrote the manuscript.
-
Funding This project was funded by York Neuroscience Discovery Inc (YND), the support organisation of Neurodegenerative Disorders Research Pty Ltd (NDR).
-
Competing interests None.
-
Provenance and peer review Not commissioned; externally peer reviewed.
-
Data sharing statement There are no additional data.