Article Text

Abstract
Objective The aim of this study was to examine whether low-dose acetylsalicylic acid (ASA) influences the rate of cognitive change in elderly women.
Design Prospective, population-based cohort study.
Setting The city of Gothenburg, Sweden, including those living in private households as well as in residential care.
Participants The sample was derived from the Prospective Population Study of Women and from the H70 Birth Cohort Study in Gothenburg, Sweden. Both samples were obtained from the Swedish Population Register, based on birth date, and included 789 (response rate 71%) women aged 70–92 years. After the exclusion of individuals with dementia and users of warfarin, clopidogrel or heparin at baseline, 681 women were examined. Among all participants, 95.4% (N=601) had a high cardiovascular risk (CVD), defined as 10% or higher 10-year risk of any CVD event according to the Framingham heart study and 129 used low-dose ASA (75–160 mg daily) at baseline. After 5 years a follow-up was completed by 489 women.
Primary outcome and secondary outcome measures Cognitive decline and dementia incidence in relation to the use of low-dose ASA and cardiovascular risk factors. Cognition was measured using the Mini Mental State Examination (MMSE), word fluency, naming ability and memory word tests. Dementia was diagnosed according to the DSM-III-R criterion. As secondary outcome incidence of stroke and peptic ulcer in relation to low-dose ASA use was studied.
Results Women on regular low-dose ASA declined less on MMSE at follow-up than those not on ASA. This difference was even more pronounced in those who had ASA at both examinations (p=0.004 compared with never users; n=66 vs n=338). All other cognitive tests showed the same trends. There were no differences between the groups regarding short-term risk for dementia (N=41).
Conclusion Low-dose ASA treatment may have a neuroprotective effect in elderly women at high cardiovascular risk.
This is an open-access article distributed under the terms of the Creative Commons Attribution Non-commercial License, which permits use, distribution, and reproduction in any medium, provided the original work is properly cited, the use is non commercial and is otherwise in compliance with the license. See: http://creativecommons.org/licenses/by-nc/2.0/ and http://creativecommons.org/licenses/by-nc/2.0/legalcode.
Statistics from Altmetric.com
Article summary
Article focus
-
Several studies have examined the effect of non-steroidal anti-inflammatory drugs on cognitive function and dementia.
-
Acetylsalicylic acid (ASA) is the most widely prescribed drug to prevent cardiovascular disease.
-
No study has examined the effect of ASA on cognitive function in persons at high cardiovascular risk.
Key messages
-
Low-dose ASA use in women at high cardiovascular risk was related to less cognitive decline during a 5-year follow-up.
-
Low-dose ASA treatment may have a neuroprotective effect in elderly at high cardiovascular risk.
Strengths and limitations of this study
-
Among the strengths of this study are the population-based sample, the comprehensive examinations and the longitudinal design. In addition, we were able to create homogenous groups regarding high cardiovascular risk.
-
This is an observational study and we can therefore not exclude the possibility that the results are influenced by confounding by indication, and we cannot exclude a selection bias so that individuals with incipient cognitive decline are less likely to take ASA.
-
The primary outcome is the Mini Mental State Examination which is not sensitive to detect small changes in cognitive function. However, a low sensitivity would decrease the possibility to find differences between the groups.
Introduction
Life expectancy, and thus the number of elderly people, increases worldwide. Cardiovascular disease (CVD) and cognitive decline are among the most important causes for disability and illness in this age group.
Inflammation might be important in the pathogenesis of cognitive decline1 as well as CVD.2 ,3 There is a large literature on the possible preventive effect of non-steroidal anti-inflammatory drugs (NSAID) on dementia.4–8 Population-based observational studies generally report that the use of NSAIDs decreases the risk of Alzheimer's disease,4 ,6 ,8 ,9 while randomised controlled trials have most often given negative results.7 ,10 Despite the large literature on NSAIDs, few studies have examined the effect of acetylsalicylic acid (ASA) on dementia.5 ,6 ,11 ,12
Daily low-dose ASA is established in the secondary prevention of CVD and in some countries also for primary prevention in individuals at sufficiently high CVD risk.13 However, the use of low-dose ASA for primary prevention is debated.14 For example, in Sweden and many other countries, low-dose ASA is mainly prescribed to prevent CVD in individuals with already manifest vascular disease, for example, myocardial infarction or stroke. For this purpose, it is given in doses sufficient to inhibit coagulation. The anti-inflammatory effect seems to come at higher doses than the doses generally used in Scandinavia.15
Studies on the effect of ASA on dementia and cognitive change are contradictive. Most studies on ASA in relation to Alzheimer's disease have given negative results5 ,6 with some exceptions.11 ,12 In the Rotterdam Study, low-dose ASA use was even related to an increased incidence of vascular dementia.6 Few studies have examined the role of ASA on cognitive change, which is the earliest sign of dementia.8 ,16 ,17 The Baltimore Longitudinal Study on Aging, with a mean participant age of 51 years, reported conflicting results using mixed effects regression models.18 Thus, ASA use was related to better concurrent result on the Mini Mental State Examination (MMSE) and some other tests, and had an interaction effect with age on memory tests, interpreted as more prospective decline in these tests. A large double-blind placebo-controlled trial showed no effect of ASA on global cognitive function during 4 years of follow-up in mainly healthy women (mean age 66 years).19 Secondary analyses suggested, however, that ASA might have an effect in individuals with cardiovascular risk (current smokers and hyperlipidaemia). No studies have been done in elderly women at high risk for cardiovascular disease. Swedish populations may be especially suited for these kinds of studies, as ASA is not widely recommended for use in individuals at high cardiovascular risk.
The aim of this study was to examine the effect of low-dose ASA on cognitive function in an elderly population, taking into account the cardiovascular risk profile based on the primary care formula from Framingham Heart Study for Use in Primary Care.20
Methods
Sample
The sample was derived from the Prospective Population Study of Women21 and from the H70 Birth Cohort Study in Gothenburg, Sweden.22 Both samples were obtained from the Swedish Population Register, based on birth date, and included both those living in private households and in residential care.
The baseline sample has been described previously.22 Briefly, the study included women (born on certain dates in 1908, 1914, 1918, 1922 and 1930) living in Sweden from 1 September 2000, according to the Swedish Population Register. Among 1200 selected, 48 died before they could be examined, 12 could not speak Swedish and 21 had emigrated outside Sweden, leaving an effective sample of 1119. Among these, 789 women accepted to participate in the psychiatric examination (response rate 70.5%). Among those, 91 were excluded due to dementia and 17 because they used warfarin, clopidogrel or heparin, leaving 681 women for this study.22 Of the 681, four women were born in 1908, 23 women were born in 1914, 133 were born in 1918, 186 were born in 1922 and 335 were born in 1930.
There were no significant differences regarding birth year, age or hospital discharge diagnoses of dementia between participants and non-participants. Compared with non-participants, participants were more likely to survive until November 2003 (p=0.037) and were less often registered with stroke (p=0.038) or psychiatric diagnoses (p=0.005) in the Swedish Hospital Discharge register that contains diagnoses according to the International Classification of Diseases from 1980 and onwards.
A follow-up examination was conducted in 2005–2006. Of the 681 examined in 2000, 521 were available for participation in 2005 and 489 (response rate 71.5%) accepted participation in a psychiatric follow-up examination and completed all tests. Of those, 266 women were born in 1930 and 223 women were born in 1914, 1918 or 1922.
The majority of participants were examined at the geriatric outpatient clinic of Vasa Hospital in Gothenburg. Those who declined examination at the outpatient clinic, as well as those who had moved to other regions within Sweden, were offered home visits. After complete description of the study to the subjects, written informed consent was obtained from all participants and/or their informants. The study was approved by the Ethics Committee for Medical Research at the University of Gothenburg.
Assessments
The examinations were conducted at an out-patient department or in the participant's home and included comprehensive social, functional, physical, neuropsychiatric and neuropsychological examinations.
At each examination, the participants underwent a physical examination, blood pressure determination and phlebotomy for vascular risk factors. Cigarette smoking was ascertained by self-report and report from a close informant. Blood pressure was measured in a sitting position on the left arm. Serum total and high-density lipoprotein cholesterol levels were determined and diabetes mellitus was defined as using insulin or oral hypoglycaemic medications and/or if the participant had a diagnosis of diabetes mellitus told by a physician. Apolipoprotein E (APOE) genotyping was performed by solid-phase mini sequencing.
Information on regular drug use, including ASA and other NSAIDs, was collected from multidose drug dispensing lists, a list of drugs delivered to individuals every second week. When such lists were unavailable, information on drug use was collected during home/nursing home visits. Participants were asked to show the interviewer the drugs they used. A participant was classified as a user of the drug if use was documented by either source. Information on duration of drug use or dosage regimen was not available. Low-dose ASA was defined as when the regimen was 75–160 mg daily.
Education was assessed as mandatory education (6 years in those born 1908–1922, 7 years in those born 1930), or more than mandatory.
Neuropsychiatric examinations were conducted by experienced psychiatric nurses in 2000–2003 and 2005–2006. The examinations were semistructured and included ratings of psychiatric symptoms and signs and tests of mental functioning, including assessments of episodic memory (short-term, long-term), aphasia, apraxia, agnosia, executive functioning and personality changes, as described previously.23 Cognitive function at baseline and at follow-up was also assessed using the MMSE,24 naming test, category fluency and word memory test.
Close informant interviews were performed by experienced psychiatric research nurses in 2000–2003 and 2005–2006. The interviews were semistructured and included questions about changes in behaviour and cognitive function (eg, memory, intellectual ability, visuospatial function, language and executive function), personality changes, psychiatric symptoms, activities of daily living, and in the case of dementia, onset age and disease course, as described previously.23
Dementia diagnoses
Dementia was diagnosed according to the Diagnostic and Statistical Manual of Mental Disorders, Third edition, revised (DSM-III-R) criteria25 by neuropsychiatrists at consensus meetings using information from neuropsychiatric examinations and close informant interviews.26 For those lost to follow-up (deceased and refusals), psychiatrists examined medical records from all major hospitals, geriatric and psychiatric institutions and outpatient services in Gothenburg. The Swedish Hospital Discharge Register was also used. The diagnosis of dementia from these sources was made if medical records revealed a diagnosis of dementia or impairments of memory and other cognitive functions producing significant difficulties in activities of daily living. Almost all people in Sweden have access to public health services and have therefore equal chances to have medical records, or being in the hospital discharge register.
A 10-year cardiovascular risk score was applied based on the primary care formula from the Framingham Heart Study.20 High CVD risk was defined as 10% or higher 10-year risk of any CVD event. This score was used to control for the confounding effect of cardiovascular disease. It was also used for subanalyses of the effect of ASA on cognitive change in those with high CVD risk. The American Heart Association recommends the use of low-dose ASA in this group.13
Statistical analysis
Differences in proportions were tested with Fisher's exact test. Differences in MMSE change from 2000 to 2005 were tested with the non-parametric Mann-Whitney U test. Multiple linear regression models were used to explore the factors related to changes in MMSE score. Factors used in the models included age, APOE ɛ4 carriership, baseline MMSE score, high cardiovascular risk score and education.
Statistical tests were carried out using SPSS for Windows (V.17, SPSS, Chicago, Illinois, USA). A two-tailed level of significance, p<0.05, was used for all tests.
Results
Baseline characteristics in 2000
Baseline characteristics in 2000 for those treated (N=129) and not treated (N=552) with low-dose ASA are shown in table 1.
Baseline characteristics of the study population* by the use of ASA
Among all 681 participants, 129 had ASA (18.9%). Of these, 104 had a daily dose of 75 mg, and 25 a daily dose of 160 mg. Among all women, 94 were on daily treatment with other NSAIDs than ASA. Of these, 18 also had ASA.
Those on low-dose ASA treatment had lower MMSE score and lower word fluency scores at baseline than those without (table 1). There were no relations between NSAIDs and cognitive test scores at baseline (data not shown).
Change in MMSE score between 2000–2001 and 2005–2006
Without controlling for any other covariates the average MMSE declined over the 5-year follow-up period and was −0.88 for the whole sample; −0.95 for ASA non-users and −0.05 for those using ASA in 2000 and 2005 (N=66). Women on low-dose ASA at baseline declined less on MMSE than those not on ASA even after adjusting for baseline MMSE, age at baseline, APOE ɛ4 carriership, other NSAIDs and cardiovascular risk score (table 2). Other NSAIDs did not influence MMSE change.
Multiple linear regression results of selected factors affecting change in MMSE in women followed from 2000 to 2005
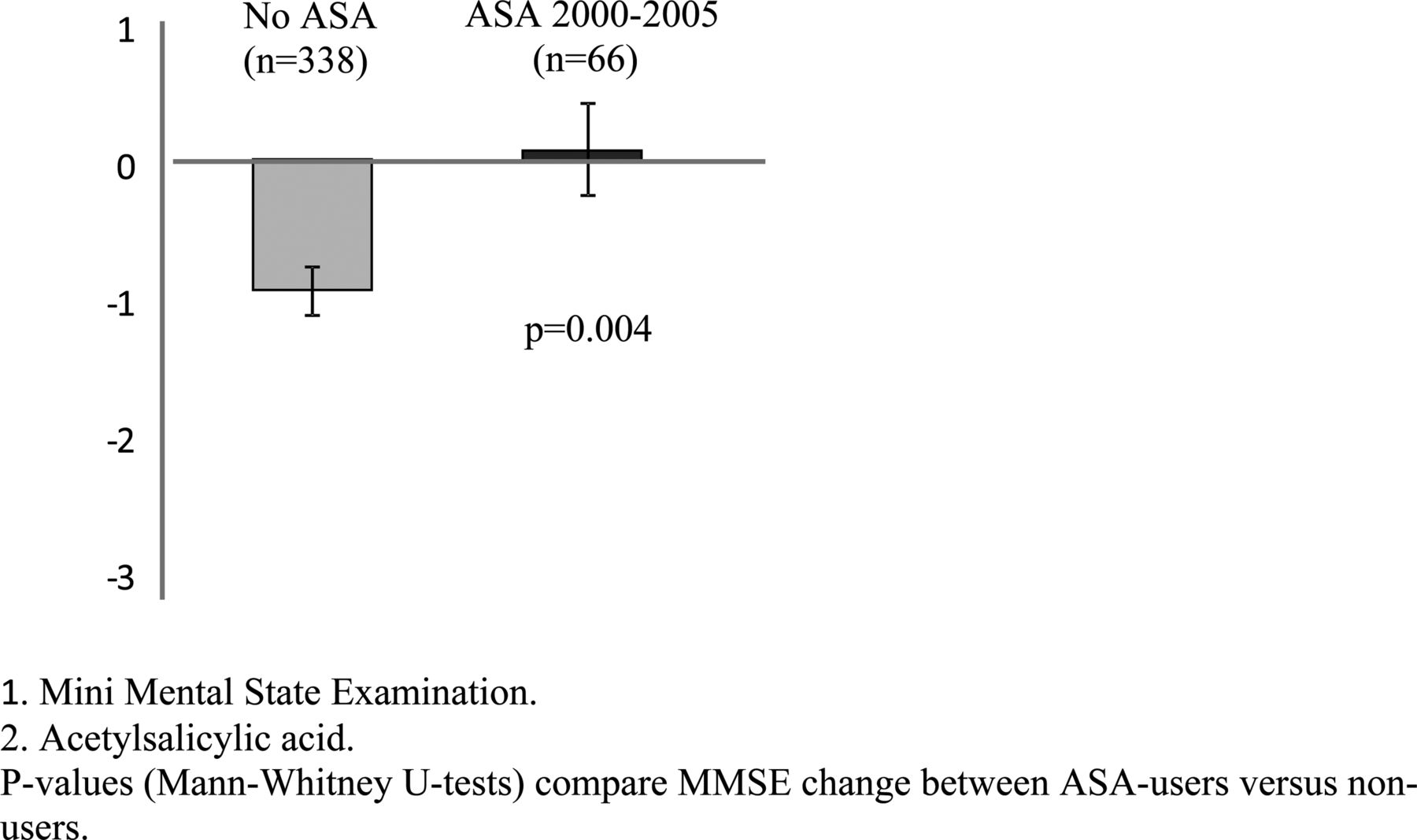
The sample was then stratified into those using ASA in 2000 and 2005 (N=66), those using ASA in 2000 but not in 2005 (N=18), those not using ASA in 2000 but using it in 2005 (N=67) and those not using ASA at either examination (N=338). Women using ASA at both examinations increased in MMSE score (p=0.004 compared to never users; figure 1). Non-significant declines were found for women using ASA at one of the two measure points (baseline users p=0.191; follow-up users p=0.346). The results did not change when those who developed dementia in 2005 were excluded.
{kind=link}
Change in Mini Mental State Examination (MMSE) by acetylsalicylic acid (ASA) use in women followed from 2000 to 2005 p Values (Mann-Whitney U tests) compare MMSE change between ASA-users versus non-users.
Other cognitive tests (word fluency, naming test and word memory) showed the same trends but the differences between the groups were not statistically significant (data not shown).
At follow-up in 2005, 41 participants had developed dementia. There was no significant difference between the ASA and non-ASA treatment group regarding the development of dementia (table 3). In the ASA treatment group, 7.1% (N=6) had a stroke during follow-up compared with 5.2% (N=21) in the non-ASA treatment group (p=0.438; table 3). Three women had haemorrhages between 2000 and 2005. None of these had ASA treatment. There were no significant differences between the ASA and non-ASA treatment groups regarding the development of gastric ulcer (table 3).
Acetylsalicylic acid (ASA) use at baseline in relation to development of gastric ulcer, stroke and dementia during follow-up in women
Among the 94 on other NSAIDs than ASA, 80 participated in 2005 and 25 were still using other NSAIDs. Those on other NSAIDs than ASA did not differ from those not on NSAIDs regarding change in MMSE scores and other cognitive tests.
High-risk group
We then analysed only those with a Framingham risk score of more than 10%. Information on risk factors was insufficient for calculation of the risk score in 51 participants, leaving 630 women. In 2000, 601 of 630 (95.4%) women had a CVD risk higher than 10%. The mean Framingham score in the ASA treatment group was higher than in the non-treatment group (23.7 SD 6.4 vs 22.2 SD 6.5; p=0.019, MWU). Within the high-risk group, those on ASA treatment decreased less in MMSE scores than those without ASA (−0.33 SD 3.3 vs −0.95 SD 2.9; p=0.028, MWU). The other cognitive tests (word fluency, naming test and word list memory) showed similar trends but the differences between the groups were not statistically significant. Those on NSAIDs other than ASA did not differ from those not on NSAIDs regarding change in MMSE scores and other cognitive tests.
Discussion
Statement of principal findings
Despite ASA being widely prescribed to prevent CVD, as recommended by the American Heart Association,13 there are only few studies examining the influence on cognitive function.8 ,16–19 In a longitudinal population-based study, we found that low-dose ASA treatment was related to less global cognitive decline in women at high risk for cardiovascular disease.
Strengths and limitations of the study
Among the strengths of this study are the population-based sample, the comprehensive examinations and the longitudinal design. In addition, we were able to create homogenous groups regarding high cardiovascular risk.
Some methodological considerations need to be addressed. First, it must be emphasised that this is an observational study. We can therefore not exclude the possibility that the results are influenced by confounding by indication. However, randomised controlled trials may be difficult to conduct due to ethical reasons in individuals with high cardiovascular risk. Second, the primary outcome in this analysis is the MMSE. Despite this being the most commonly used cognitive test, the MMSE is not sensitive to detect small changes in cognitive function. However, a low sensitivity would decrease the possibility to find differences between the groups. Third, MMSE score measures global cognitive function and mainly test cognitive domains that are related to language. Thus, the MMSE does not detect executive dysfunction, which has been hypothesised to be especially influenced by ASA use.19 We might therefore have underestimated the effect of ASA by using the MMSE. Fourth, we cannot exclude a selection bias so that individuals with incipient cognitive decline are less likely to take ASA. However, the lower MMSE score at baseline in the ASA treatment group does not support this suggestion. Fifth, our study may be too small to detect very small differences between the groups. However, small differences may not be clinically relevant. Finally, we cannot exclude the possibility of that the reduced cognitive decline among ASA-users might represent regression to the mean, or, as always possible, the results may be due to chance. For a definite conclusion more studies are needed.
Our findings in relation to others
Despite the large literature on NSAIDs and cognitive change in the elderly, few studies have examined the role of ASA. The Women's Health Study (WHS) showed no general effect of ASA on primary cognitive outcomes, but reported a slightly positive effect on category fluency without beneficial effect on global cognitive function.19 We found no effect on category fluency, but an effect on global function using MMSE. One reason for the effect on category fluency in WHS may be that this study included very healthy women, while our study included mostly individuals with high cardiovascular risk. Category fluency is considered to reflect executive functions, which may be disturbed in patients with subcortical cerebrovascular disease. It may be that our high-risk group already had developed subcortical cerebrovascular disease, which could no longer be influenced by ASA use, while in the low-risk group in WHS it was still possible to prevent these changes. Another reason may be that WHS used telephone interviews to assess cognitive function, while we used personal examinations.
We found that ASA, but not other NSAIDs, had a beneficial effect on change in cognitive function. The Baltimore Longitudinal Study on Aging (BLSA) reported that ASA use was related to better concurrent result on some tests, including the MMSE, and an interaction effect with age on memory tests, interpreted as more prospective decline in these tests.27 Our results are in contrast to this, that is, we found lower baseline MMSE and less decline in the ASA group. These differences may be due to the considerably lower age (mean of 51 years) and lower CVD risk in BLSA compared to our population.
Several studies examined the effect of ASA on the incidence of Alzheimer's disease, and not on general cognitive function. The results of these studies are contradictive, some suggest a protective effect on Alzheimer's disease9 ,11 ,12 while others do not.5 ,6 ,28 In our study, ASA did not influence the incidence of dementia at follow-up. This may be due to a very short time of follow-up. Our finding that ASA use influenced cognitive function may reflect an effect on preclinical dementia, indicating that treatment must start early to have a sufficient neuroprotective effect.
Meaning of the study
The mechanism for the protective effect of ASA is not fully understood. Low-dose ASA irreversibly blocks the formation of thromboxane A2 in platelets producing an inhibitory effect on platelet aggregation,15 whereas other NSAIDs (such as ibuprofen or diclofenac) are reversible inhibitors.29 In low doses, ASA thus mainly confers an antiplatelet effect and a limited anti-inflammatory effect.30 It is therefore possible that ASA might influence cognitive decline by enhancing the cerebral blood flow by reducing platelet aggregation. In addition, a recent review suggested that some of the beneficial actions ascribed to ASA are due to ASA's ability to act through cyclooxygenase-2 to generate new neuroprotective docosanoids from docosahexaenoic acid (DHA) and arachidonic acid (AA). AA and DHA are converted to new families of lipid mediators that are pivotal in promoting resolution.31
Only less than one-fourth with a high-risk score for CVD was on ASA. Some European countries and the American Heart Association recommend ASA treatment in patients at high CVD risk.32–34 However, these guidelines are debated14 and in Sweden there are no such recommendations. ASA treatment is therefore mainly used in patients with manifest artherosclerotic disease. This is partly due to concerns for adverse side effects. However, there were no haemorrhages and no increased risk of peptic ulcers during follow-up in the ASA treatment group. We can however not exclude the possibility of an increased risk for microbleeds.35 ,36
Unanswered questions and future research
Our study suggests a neuroprotective effect of ASA, at least for elderly women at high cardiovascular risk. Longer follow-ups are needed to evaluate the long-term effect of ASA on cognitive function and dementia. Randomised controlled studies are important to finally evaluate the effect of ASA on cognitive function. However, this may be difficult to conduct in individuals with high CVD risk due to ethical reasons. Basic science studies are necessary to fully understand the mechanisms behind the possible neuroprotective effect of ASA treatment.
Acknowledgments
We thank the participants and their families, study nurses and staff at the neuropsychiatric unit.
References
Footnotes
-
Contributors SK analysed and interpreted the data and wrote the paper. IS conceived and designed the study, refined study methods, was involved in analysis and interpretation of the data and revised the article critically for important intellectual content. JK contributed with important aspects of the study design and revised the article. SÖ was involved in analysis and interpretation of the data and revised the article critically for important intellectual content. ABH was involved in study design, analysis and interpretation of the data, writing, revising and editing. The corresponding author has the right to grant on the behalf of all authors, and all authors gave final approval to the version to be submitted.
-
Funding This study was supported by grants from the Swedish Council for Working Life and Social Research (no 2001–2835, 2001–2646, 2003–0234, 2004–0150, 2004–0145, 2006–0596, 2006–0020, 2008–1111, 2008–1229 and 2010–0870), the Alzheimer's Association Stephanie B. Overstreet Scholars (IIRG-00-2159), the Swedish Research Council (no. 11267, 2005–8460, 825–2007–7462), The Bank of Sweden Tercentenary Foundation, Stiftelsen för Gamla Tjänarinnor and Handlanden Hjalmar Svenssons Forskningsfond. The funding sources had no involvement in study design; the collection, analysis and interpretation of data; in the writing of the paper and in the decision to submit the paper for publication.
-
Competing interests None.
-
Ethics approval The study was approved by the Ethics Committee for Medical Research at the University of Gothenburg.
-
Provenance and peer review Not commissioned; externally peer reviewed.
-
Data sharing statement As this is a longitudinal exploratory, non-interventional, observational study of a systematic sample of the general elderly population, we have no data to share.