Article Text

Abstract
Objective To compare the outcomes of manual small incision cataract surgery (MSICS) and phacoemulsification performed by ophthalmology trainees.
Design Retrospective cohort design.
Setting Tertiary eye care centre.
Participants A total of 1029 subjects underwent cataract surgeries with MSICS technique or phacoemulsification by trainees during one quarter (July–September 2007). Only 484 (47%) subjects were males. Surgeries which were primarily large incision extracapsular or intracapsular cataract extraction and performed on patients less than 20 years of age were excluded.
Outcome measures The postoperative best corrected visual acuity (BCVA) along with the rates and types of complications were compared between both the groups.
Results A total of 1029 surgeries were performed by 22 resident surgeons. In all, 522 (50.7%) were done using MSICS technique and 507 (49.2%) were done by phacoemulsification. Those in the MSICS group were significantly older (age >70 years; 5.7% vs 3.4%; p<0.001) and had worse preoperative visual acuity (visual acuity <6/60; 69.3% vs 40.4%; p<0.001). Postoperatively, the number of patients having BCVA≥6/12 was similar in both the groups (84.3% vs 88%; p=0.09). The complication rates were higher in MSICS group (15.1% vs 7.1%, p<0.001). Most common risk factor for poor outcome (postoperative BCVA<6/60) in both the groups was presence of associated ocular pathologies (OR 7.4 95% CI 3.4 to 16.4) and having a complications (OR 5.7 95% CI 3.0 to 10.8).
Conclusions Although the complication rate was higher in the MSICS group, there was no difference in BCVA in both the groups.
- Audit
- Education & Training (see Medical Education & Training)
- Ophthalmology
This is an open-access article distributed under the terms of the Creative Commons Attribution Non-commercial License, which permits use, distribution, and reproduction in any medium, provided the original work is properly cited, the use is non commercial and is otherwise in compliance with the license. See: http://creativecommons.org/licenses/by-nc/2.0/ and http://creativecommons.org/licenses/by-nc/2.0/legalcode.
Statistics from Altmetric.com
Article summary
Article focus
-
Manual small incision cataract surgery (MSICS) is the most common surgery performed in developing countries, followed by phacoemulsification.
-
Many reports have compared the efficacy, safety and cost-effectiveness of these two techniques, when performed by expert surgeons.
-
However, there are no data on comparison of the outcomes of MSICS and phacoemulsification performed by ophthalmology trainees.
Key messages
-
Despite higher complications in the MSICS group, there was no significant difference in best corrected visual outcomes in the two groups.
-
Most common risk factor for poor outcome in both the groups was the presence of associated ocular pathologies and having complications.
-
Having uniform standards of training can result in improvement in outcomes irrespective of the technique performed.
Strengths and limitations of this study
-
Strength includes large sample size, first study comparing outcomes of MSICS and phacoemulsification in ophthalmology trainees and generalisability of the results to other training programmes in the country.
-
Limitations include that the data are retrospective and non-randomised.
Introduction
With the advent of intraocular lens, large incision extra capsular cataract extraction with non-foldable, posterior chamber intraocular implantation was the initial surgical technique taught to the trainee ophthalmologist.1 In recent years, the trend has changed towards using smaller incisions and performing sutureless surgeries. Majority of the trainees, especially in developing countries, learn the sutureless manual small incision cataract surgery (MSICS) technique initially followed by phacoemulsification.2 ,3 Some training programmes, in developed countries, start by teaching phacoemulsification as the first technique of cataract removal.4–6 Many reports have compared the efficacy, safety and cost-effectiveness of these two techniques, when performed by expert surgeons.7–9 In prior reports related to cataract surgery training, only the success rate of phacoemulsification done by trainees has been evaluated.3–6 10–20 To the best of our knowledge, this is the first study to compare the results of MSICS and phacoemulsification done by trainees.
Materials and methods
L V Prasad Eye Institute, Andhra Pradesh, India is a tertiary care eye hospital and a WHO collaborating centre in prevention of blindness. Data pertaining to all cataract surgeries performed by trainees during one quarter (1 July 2007 to 30 September 2007) were analysed. A trainee is defined as someone who has completed his/her ophthalmology residency and has joined for fellowship programme at the institute. All cataract surgeries performed by 22 trainees using either MSICS or phacoemulsification were included in the study. Surgeries which were primarily large incision extracapsular or intracapsular cataract extraction and performed on patients less than 20 years of age were excluded. Approval of the Ethics Committee of the Institute was obtained for the data collection.
All the trainees had completed their basic residency in ophthalmology from different centres across India and as a part of training; they are supposed to be trained in microsurgery. However, unlike the developed West, the training standards are quiet variable across the country.21 Hence, to have a uniform standard for these trainees, all of them performed surgeries under supervision, for their first 25–30 cases at our institute. After this, they were allowed to perform surgeries independently.
Preoperative data collection for each eye included the patient age and gender, preoperative visual acuity (uncorrected and best corrected visual acuity; UCVA and BCVA, respectively), details of slit lamp examination of the anterior segment and preexisting ocular conditions likely to influence either the operative course or the final visual acuity.The intraocular pressure was recorded by applanation tonometry in all cases. The posterior pole was examined with slit-lamp biomicroscopy using +90 D or +78 D lens. Indirect ophthalmoscopy was done to evaluate the retinal periphery. The status of the other eye was similarly documented. In the case of non-visibility of posterior segment, B-scan was performed for the eye.
Axial length measurements and keratometry recordings were done and SRK-II formula22 was used to calculate the intraocular lens (IOL) power required. The systemic status of the patient was evaluated to ensure fitness for surgery under local anaesthesia.
Operative data included the name of the resident, consultant in-charge, date of the surgery, technique of surgery employed—including the details of each step and details of the IOL implanted. The occurrence of any intraoperative complication was documented along with the details of the subsequent management.
All surgeries were performed under local (peribulbar) anaesthesia. MSICS was performed by a modified Blumenthal technique.2 After cleaning and draping the eye, a barraquer speculum was applied. A superior rectus bridle suture was applied with 4'0 silk. A paracentesis was made at 10 o'clock position with a micro vitreoretinal (MVR) blade. In cases of total/dense cataracts where the fundal glow was not visible, trypan blue dye was used to stain the anterior capsule. Viscoelastic was injected into the anterior chamber. A capsulorrhexis was performed with the help of a cystitome through the paracentesis. Whenever the capsulorrhexis threatened to extend to the periphery, it was converted to a can-opener capsulotomy. If the size of the rhexis was deemed insufficient for prolapsing of the nucleus into the anterior chamber, two relaxing incisions were made on the rhexis margin. A fornix-based conjunctival flap was made from 10 to 2 o’clock position. A 5.5–6 mm-long scleral incision was made with a No. 15 blade about 1–2 mm posterior to the limbus. Two back cuts (1–2 mm long) were made at the ends, at approximately 45° angulations. A sclero-corneal tunnel was dissected with a crescent, with 1–2 mm dissection into the cornea (and always cutting backwards with the sides of the crescent). An anterior chamber maintainer (ACM) was inserted into the anterior chamber through a slightly longer paracentesis at the infero-lateral aspect of the cornea (7 o’clock for right eye and 5 o'clock for left eye). With the ACM switched on, the anterior chamber was entered with a keratome, and the internal opening was extended up to 7–8 mm, taking care to cut inwards. Hydrodissection and hydrodelineation were performed as deemed appropriate for the case. The nucleus was prolapsed into the anterior chamber either during hydrodissection or by using a sinsky hook and the nucleus was delivered out. Cortical matter was aspirated using the single-port Blumenthal canula with the ACM on. A 6.5 mm polymethyl methacrylate (PMMA) posterior chamber IOL was implanted into the bag, under viscoelastic. Viscoelastic was removed and paracenteses were hydrated. Wound was checked for the absence of leak and if present, it was sutured. Conjunctival flap reposited over the incision. Speculum was removed and the eye was patched after instilling a drop of 2.5% betadine in the conjunctival cul-de-sac.
Phacoemulsification was performed using a peristaltic, Universal-II machine of Alcon Pharmaceuticals (Alcon Laboratories, Fort Worth, Texas, USA), with standard ‘divide and conquer’ technique. A capsulorrhexis was performed from the paracentesis as described earlier. A 5 mm scleral straight incision was made superiorly and a sclera tunnel created. A second paracentesis was made at 2 o'clock position. Hydrodissection and hydrodelineation were performed. After ensuring the free rotation of the nucleus, a four-quadrant technique was used during trenching. Each quadrant was then emulsified and aspirated. Cortical matter was cleaned using automated irrigation and aspiration. A non-foldable PMMA posterior chamber IOL with a 5.25 mm optic was implanted into the capsular bag under viscoelastic. Viscoelastic was removed using automated irrigation and aspiration. Wound was checked for the absence of leak, and if present, was sutured. Conjunctival flap reposited over the incision. Speculum was removed and the eye was patched, after instilling a drop of 2.5% betadine.
In the event of complications or impending complications, the consultants guided the trainees and helped in averting the complication or in managing the problem.
Postoperative data were documented on the first day, between 1 and 3 weeks and finally at 4–11 weeks visit. Prednisolone acetate 1% eye drops six times per day and ofloxacin 0.3% eye drops four times per day were given for the first week. From the second week onwards, antibiotic drops were discontinued and topical steroids were tapered over the next 5 weeks. On each of the visits, uncorrected visual acuity and pin-hole improvement was noted along with detailed slit lamp examination of the anterior segment along with fundus examination, when needed. On the last follow-up (4–11 week visit), in addition to above, refraction was performed and BCVA was noted, and glasses were prescribed.
Statistical analysis
Statistical analysis was performed using Stata 11.23 For categorical variables, χ2 or Fischer's exact test were used and for continuous variables, Independent sample t test was used. Normality of continuous variable was checked using Shapiro-Wilk test. Logistic regression was used for univariate and multivariate analysis to look for risk factors for poor outcomes (defined as BCVA<6/60 in final follow-up visit). Multicollinearity between variables was assessed looking at the variance inflation factor and fitness of the model was assessed using the Hosmer Lemeshow test for goodness of fit.24
Results
A total of 1067 surgeries were performed by 22 residents during the study period. Of these, 38 surgeries were either large incision extracapsular or intracapsular cataract extraction and hence, excluded from the study. Table 1 shows the preoperative comparison of two groups (MSICS and phacoemulsification). Out of the total 1029 surgeries analysed, 522 (50.7%) were done with MSICS technique and 507 (49.2%) with phacoemulsification. Patients in MSICS group were significantly older than patients in phacoemulsification group (t-test; p<0.001). The number of elderly patients (age >70 years) were more in MSICS group (5.7%), than in phacoemulsification group (3.4%) and this difference was statistically significant (p<0.001). There was no statistically significant difference in the gender distributions (p=0.1). Both groups had 28 patients each, who had risk factors (ocular comorbidities) which may have adversely affected the intraoperative or the postoperative course, (p=0.9). For example, corneal scar/degeneration, uveitis, glaucoma or retinal pathology.
Baseline characteristics of patients
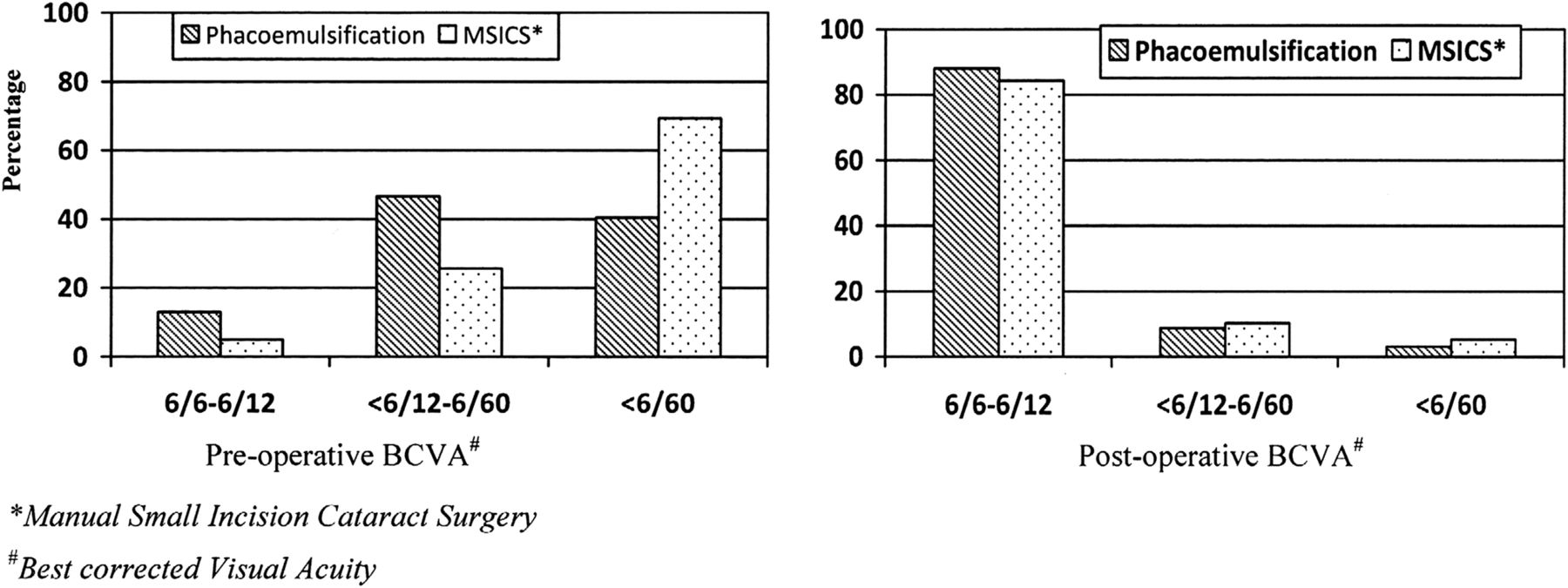
Figure 1 illustrates the mean preoperative and postoperative BCVAs. The preoperative visual acuity was worse in the MSICS group than the phacoemulsification group (visual acuity <6/60: 69.3% vs 40.4%; p<0.001). Postoperatively, BCVA was ≥6/12 in 84.3% patients in MSICS group as compared with 88% in phacoemulsification group (p=0.09). Visual acuity of 6/60 or worse was seen in 5.4% patients of MSICS group and 3.2% patients of the phacoemulsification group (p=0.18). Intraocular lens was implanted successfully in 509 cases (97.5%) of MSICS group and 503 cases (99.6%) in the Phacoemulsification group (p=0.005).
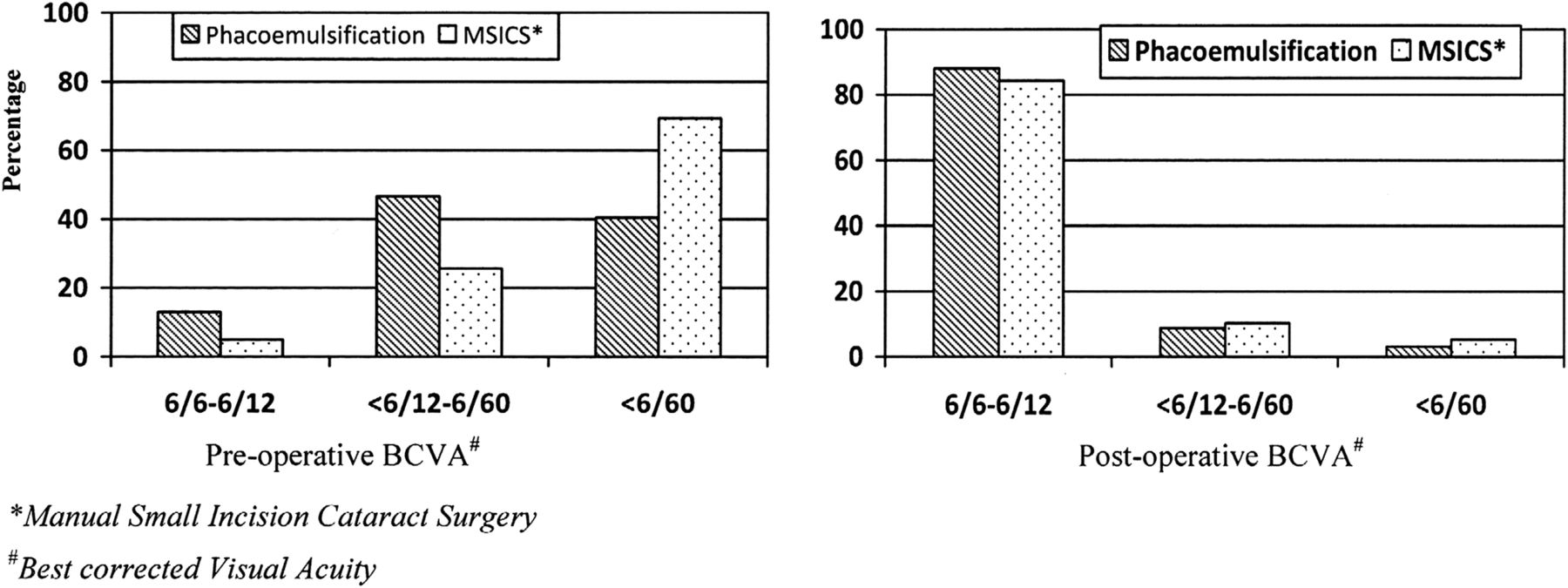
Comparison of preoperative and postoperative best corrected visual acuity (BCVA) in both the groups. MSICS, manual small incision cataract surgery.
Figure 2 shows the detailed distribution of the complications in both the groups. It reveals that the overall complications were seen more in the MSICS group as compared with the phacoemulsification group (15.1% vs 7.1%, p<0.001). The most common complication in both the groups was a posterior capsular rent (PCR) followed by zonular dialysis (ZD). PCR was seen in 36 eyes (6.9%) in MSICS group and 22 eyes (4.3%) in the phacoemulsification group (including one eye with a nucleus drop). Similarly, ZD was seen in 20 eyes (3.8%) in MSICS group and 7 eyes (1.4%) in the phacoemulsification group. Overall, PCR and ZD were higher in MSICS group as compared with the phacoemulsification group (p<0.001). Endophthalmitis was noted in three cases (one in MSICS and two in the phacoemulsification group) postoperatively. The causative organisms were identified as Staphylococcus epidermidis (this patient was lost to follow-up); non-fermenting Gram-negative bacillus (patient regained final BCVA of 6/24 after retinal intervention); no organism was isolated in the third patient, who had a final BCVA of 6/48 after intervention. All seven cases of Descemet's membrane detachment (DM detachment) occurred only in the MSICS group (1.3%). Three cases were managed by air bubble injection into the anterior chamber at the end of surgery and had an uneventful postoperative course. Final visual acuity of these patients were 6/6, 6/12 and 6/18. Two cases had C3F8 injection at the end of surgery and had final visual acuity of 6/12 and 6/18 postoperatively. One patient underwent C3F8 descemetopexy 3 days postoperatively and the corneal oedema subsided subsequently. His visual acuity was 6/18. One patient was advised descemetopexy, but he refused and was lost to follow-up. His visual acuity at the final follow-up was 6/60.

{kind=link}
{kind=link}
Detailed distribution of the complications in both the groups.
Other complications include broken haptic (6), continuous curvilinear capsulorhexis (CCC) extension (2), iridodialysis (3), nucleus piece in the anterior chamber (1) and wound leak (10).
The surgical technique per se was not a risk factor for poor outcome (table 2). In univariate analysis and multivariate analysis, the risk factors for poor outcome were: having associated ocular co-morbidity and having a complication during surgery.
Risk factors for poor outcome (postoperative uncorrected visual acuity <6/60)
Discussion
The surgical results obtained in our study compare favourably with those mentioned in the literature for phacoemulsification done by trainees.4 ,6 ,10–12 ,19 However, to the best of our knowledge; there are no prior reports of the visual outcomes and complications in MSICS being performed by trainees who are still in their initial stages of surgical training. Overall, the outcomes reported were less than reported in clinical trials and this could be possible due to difference in the inclusion and exclusion criteria for a given clinical trials.7–9 ,25 The study shows good success for either procedure. Despite the MSICS group having worse visual acuity preoperatively; postoperatively visual acuity achieved after both types of surgery was similar, with most reaching a level of 6/12, which is functional vision.
There were few complications, the most serious being three cases of endophthalmitis. Other problems were PCR and DM detachment which were adequately managed. However, the relatively limited follow-up precludes evaluation of long-term problems like posterior capsular opacification and retinal detachment and the ultimate success rate of the procedure. The rate of PCR in phacoemulsification group was comparable to some of those reported in the literature.10 ,17 ,19 ,20 However, the rate of complications is higher in MSICS group as compared with the phacoemulsification group. This could possibly be because of the reason that fellows undergoing long-term training in this institute are taught the MSICS technique initially followed by phacoemulsification. This could translate into a better surgical hand and improved tissue handling intraoperatively by the time they start doing phacoemulsification. The DM detachments occurring in the MSICS group are a new phenomenon. Previous reports describe results of MSICS done by expert surgeons and in addition, most surgeons performed the viscodissection technique rather than the Blumenthal technique used here. As is already known, the chances of DM detachments are higher during the use of an anterior chamber maintainer (due to faulty insertion techniques) especially in the hands of trainees.
Among the risk factors for poor outcomes, having ocular co-morbidity and a complication were independent risk factors and the technique of surgery was per se not a risk factor.
Overall, the study was not immune to limitations and it lies in the inherent nature of the study, that is, being retrospective and non-randomised. We could not look at the fact that the outcomes differed by the grade of the nucleus as the retrospective nature of the study limited our ability to standardise this grading. Similarly, the surgeon factor could not be taken into account. A prospective randomised controlled trial would be more robust and would take care of the above-mentioned limitations. However, despite the above-mentioned limitations, the result of study becomes more generalisable and the results can be extrapolated to other residency/training programmes done in India.
In conclusion, it needs to be emphasised, despite the subjects in MSICS group being older and having worse preoperative visual acuity and a higher rate of complications as compared with the phacoemulsification group, it did not translate into a poorer visual outcome in this study. The overall visual outcome is similar in both the groups and compares favourably with that reported from other training programmes.
Acknowledgments
The authors wish to thank Professor William M Bourne, MD, Emeritus Professor of Ophthalmology, Mayo Clinic for doing a critical review of data and providing insights into the possible aspects of improvement and emphasis in the initial drafts of the manuscript. The authors also kindly acknowledge Professor Robert Biggar for extending his expertise in scientific writing. We are thankful not only for his patient review of this manuscript line by line, but also for setting right even the smallest of nuances which he could come across when viewing through his scientific magnifying glass.
References
Footnotes
-
Contributors RCK contributed in the concept and design of the study, data analysis and interpretation and drafting and revision of the article. SK contributed in design of the study, acquisition of the data and drafting and revision of the article. GPSS contributed in data analysis and interpretation and revision of the article. VSS contributed in the concept and design of the study, data interpretation and revision of the article. All the authors approved the final version of the manuscript.
-
Competing interests None.
-
Provenance and peer review Not commissioned; externally peer reviewed.
-
Data Sharing Statement Extra data can be accessed via the Dryad data repository at http://datadryad.org/ with the doi:10.5061/dryad.kt8tf.